Article Text

Abstract
Background Maintaining glucose in the target range, while avoiding hypoglycemia, is challenging in critically ill patients. We investigated the performance and safety of Medtronic Sentrino, a newly developed continuous glucose management (CGM) system for critically ill adults.
Methods This was a prospective, single-center, single-arm, open-label study in adult patients with cardiac ICU admission. Sentrino subcutaneous glucose sensors were inserted into patients’ thigh with planned study participation of 72 h. Sensor glucose results were displayed, and the system's alerts and alarms fully enabled. Reference blood glucose was collected from central venous catheter and analyzed with a blood gas analyzer. Treatment decisions were made independently of sensor glucose values, according to the existing standard of care.
Results A total of 21 patients were enrolled; all successfully completed the study. Sensor glucose values were displayed 96% of the time, and 870 paired blood glucose–sensor glucose points were analyzed. Overall mean absolute relative difference (MARD) was 12.8% (95% CI 11.9% to 13.6%). No clinically significant differences in accuracy were seen within subgroups of hemodynamic status (MARD 12.3% and 13.1% for compromised vs stable hemodynamics). Consensus grid analysis showed >99% of sensor glucose values within A/B zones. No device or study-related adverse events were reported. 100% of clinicians found Sentrino easy to use after two patients.
Conclusions In our single-center experience, Sentrino CGM system demonstrated good accuracy and reliability, with no device-related adverse events in critically ill cardiac patients, and was easy to use and integrate in the cardiac ICU.
Trial registration number NCT01763567.
- Cardiac
- Glucose Sensor(s)
- Glucose Monitoring Technologies
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
-
Maintaining glucose in the target range, while avoiding hypoglycemia, is challenging in cardiac intensive care unit (ICU) patients. Continuous glucose monitoring (CGM) is a promising technology that may help address these challenges, but its accuracy and safety have not been well established.
-
We conducted a prospective, open-label single-arm trial of Sentrino CGM, a new CGM system developed for critical care, in 21 cardiac ICU patients (20 postcardiac surgery, of which 3 had cardiac transplant).
-
We found that Sentrino CGM demonstrated good accuracy and reliability, with no device-related adverse events, and was easy to integrate in the flow of care.
Introduction
Elevated blood glucose (BG) is common in cardiac intensive care unit (ICU) patients, including those undergoing cardiac surgery, and is associated with adverse outcomes regardless of diabetes status.1 Previous studies have demonstrated that improved BG control may reduce morbidity and length of stay in cardiac surgery patients, and it is now a standard practice in this patient population.2 In fact, patients undergoing cardiac surgery represent the only group in which improved postoperative glucose control is currently a metric of quality care and a performance measure.3
While the use of standardized protocols and order sets has helped with achieving better glucose control in critically ill patients, significant challenges remain. One key challenge is maintaining glucose levels within the target range while avoiding hypoglycemic and hyperglycemic excursions. More specifically, hyperglycemia is strongly associated with increased risk of mortality1 ,2 ,4; similarly, hypoglycemia is a frequent occurrence in this patient population, and is also independently associated with increased risk of mortality,5–8 even when the degree of hypoglycemia is mild (BG <70 mg/dL).9 ,10 Continuous glucose monitoring is a promising technology that may help address these challenges.4 While the current standard of care is obtaining BG measurements intermittently (typically every 2–4 h), continuous glucose monitoring provides a more complete picture by revealing hyperglycemia and hypoglycemia that intermittent BG measurements might miss, thus potentially allowing for more timely intervention(s).
The feasibility of integrating continuous glucose monitoring technology into the flow of care in the cardiac ICU, as well as its performance in this patient population have not been established. Accordingly, we investigated the performance and safety of Sentrino, a newly developed continuous glucose management (CGM) system for critically ill adults, in the cardiac ICU patients who required intravenous insulin infusion for glucose control.
Materials and methods
Patient selection
This was a prospective, single-center, single-arm, open-label feasibility (pilot) study. Consecutive adult patients with actual or planned admission to either the cardiothoracic or cardiac ICU at Saint Luke's Mid America Heart Institute (Kansas City, Missouri, USA) were screened for participation in the study. Patients were considered eligible if they were aged >18 years, had anticipated life expectancy >96 h, were either initiated on or were likely to require intravenous insulin infusion for glucose control (with target glucose <140 mg/dL) following ICU admission, and did not have any of the following exclusion criteria: participation in another clinical study, current pregnancy, current treatment with hydroxyurea, and any medical condition that in the opinion of the principal investigator warranted exclusion from the study. Eligible patients were approached for study participation and completion of informed consent. Patients who signed informed consent, were admitted to one of the cardiac ICUs, and required intravenous insulin infusion for glucose control with anticipated treatment duration of at least 24 h were considered eligible for sensor insertion and study enrollment. Patients were considered as enrolled in the study following the glucose sensor insertion. The first two participants were considered ‘run-in’ patients (phase 1); phase 2 included the 19 patients enrolled after the run-in period was completed (participants #003-021.) Saint Luke's Hospital institutional review board reviewed and approved the informed consent document prior to the initiation of patient recruitment.
Study device
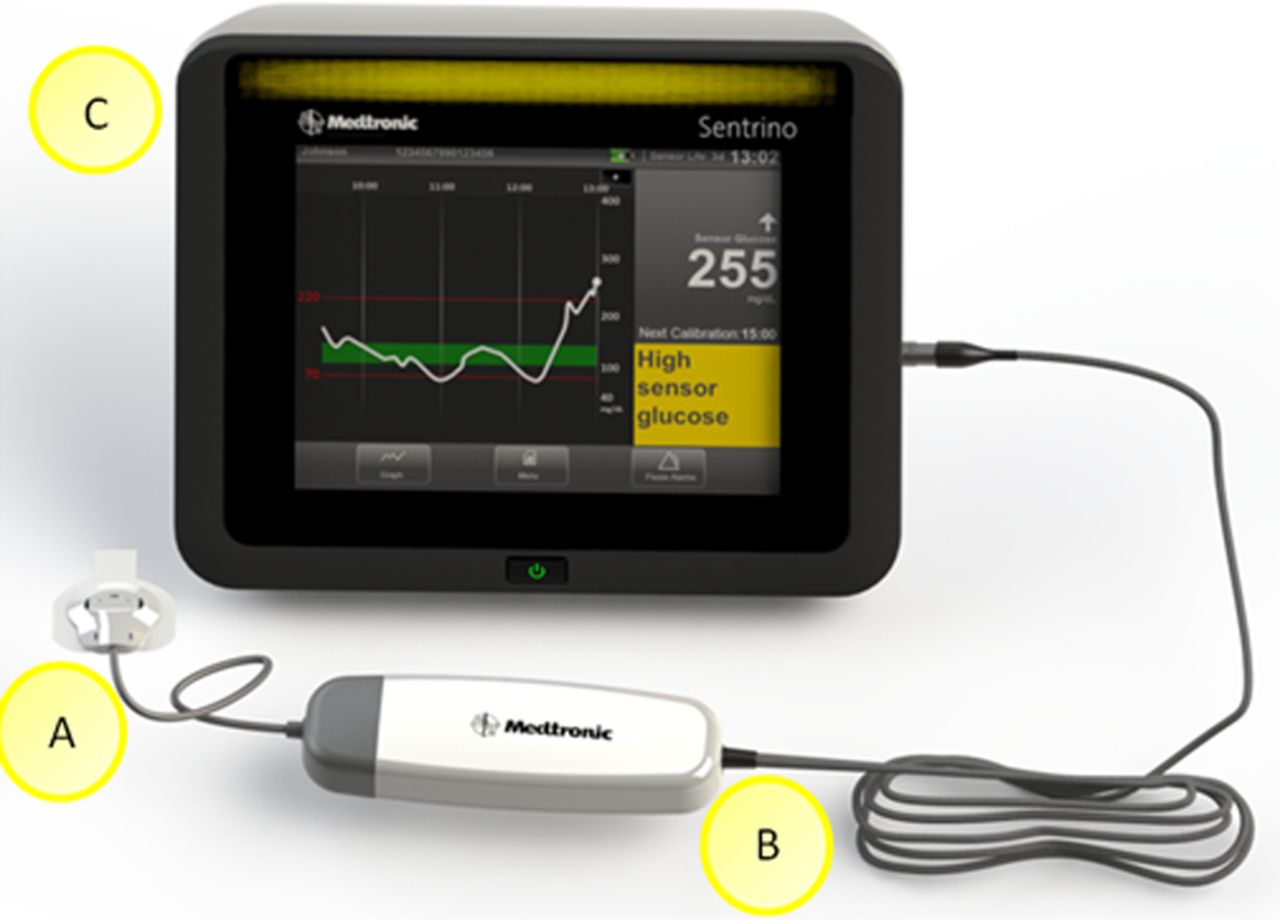
Sentrino CGM system (Medtronic Minimed, Northridge, USA) consists of three components: a subcutaneous continuous glucose sensor, the processor cable, and the monitor. The sensor is placed in the subcutaneous layer of a patient and generates an electrochemical signal representing the glucose level of the interstitial fluid via the glucose oxidase reaction. The sensor is connected to the processor cable, which captures and digitizes the electrochemical sensor signal it receives from the sensor, and subsequently sends it to the monitor (figure 1).

Components of the Sentrino continuous glucose management system: sensor (A), processor cable (B), and monitor (C).
The monitor is an interactive and portable display and data storage device that provides real-time sensor glucose (SG) values every minute, as well as alarm notification, and is used for configurable and operational control of the system.
Study procedure
After initiation of the intravenous insulin infusion (modified Yale protocol in the cardiac ICU, and Portland protocol4 ,5 in the cardiothoracic ICU, target glucose <140 mg/dL in both units), subcutaneous glucose sensors were inserted into patients’ anterior thigh by the study personnel, with planned study participation of 72 h. A maximum of two attempts were allowed for the initial sensor insertion. Each sensor could be replaced once following the initial insertion, if needed. Following sensor insertion and initial calibration, the clinical nursing staff carried out all of the sensor maintenance functions, including all subsequent calibrations, alarm management, and troubleshooting. Research staff were continuously available for study support when needed.
SG values were continuously displayed on the monitor during the study period, with the system's predictive alerts and alarms fully enabled. Reference BG values were obtained with frequency dictated by each unit's protocol, with blood samples drawn from the central venous catheter and analyzed with either an advanced, handheld blood analyzer (i-STAT, Abbott, USA) or the hospital Central Laboratory (Vitros 600 Ortho Clinical, Johnson & Johnson). In addition to the reference BG values obtained for clinical purposes, additional samples were drawn for monitor calibration and when hypoglycemia and hyperglycemia alarms were triggered.
For this study, CGM hypoglycemia alarm threshold was set at <80 mg/dL, and hyperglycemia alarm threshold was set at >180 mg/dL. In case either a hypoglycemia or hyperglycemia alarm was activated, clinical staff were instructed to acknowledge each alarm on the monitor, obtain a confirmatory reference BG value using the i-STAT blood gas analyzer (BGA) or central laboratory value, and provide treatment (if indicated) based on their respective ICU's standard of care protocol. Clinical staff were instructed to only use BGA or central laboratory results, and not SG data, for glucose management (ie, insulin dose adjustments, hypoglycemia management, etc).
Study end points and statistical analysis
The primary purpose of the study was to assess the following domains of Sentrino CGM system performance: accuracy, reliability, alarm performance, safety and ‘usability’. In the primary analysis, all 21 patients (phase 1 and phase 2) were included. SG values that were in the system's operating range (40–400 mg/dL) were compared with the reference i-STAT BG values and central laboratory results for accuracy and alarm performance assessments. Mean absolute relative difference (MARD) was used as the primary metric of analytic accuracy, calculated for each patient individually and computed separately for prespecified patient subgroups: low (≤8%) vs high (> 8%) Society of Thoracic Surgeons (STS) scores; and compromised vs stable hemodynamics during postoperative period (defined using invasive hemodynamic assessment with cardiac index ≤2 L/min/m2 or documentation of hypotension in the medical record). Consensus Error Grid analysis was used to evaluate clinically relevant accuracy and perform analysis of the outlier SG values. Bland-Altman plot was used to evaluate for fixed bias. The proportions of true, missed, and false alarms were calculated to evaluate alarm performance.
In order to assess Sentrino CGM system reliability, the ‘on-time’, that is, the ratio of total time of displayed SG data (in minutes) versus duration of sensor implantation (from the first calibration until end of sensor life, in minutes), was calculated for each patient, and averaged across the patient population. In addition, gaps in continuous sensing were categorized as either due to accidental or intentional disconnections, and/or due to performance issues. Overall ‘on-time’ was defined as the time SG was actually displayed (numerator, in minutes) divided by the total intended time of monitoring (denominator, in minutes); this total ‘on-time’ value accounts for all data gaps, regardless of cause. Additionally, sensor-cause ‘on-time’ was intended to account for device-related data gaps only, ignoring the environmental data gaps such as disconnections; it was thus calculated as the time SG was displayed after accounting for device-related data gaps (numerator, in minutes) divided by the total intended time of monitoring (denominator, in minutes).
All patients were monitored for device-related and study-related adverse events to evaluate safety.
Finally, the research personnel and clinical staff completed surveys regarding their experience with Sentrino CGM system to assess ease of use, as well as feasibility of incorporating it into the cardiac ICU flow of care (SurveyMonkey.com, LLC, Palo Alto, California, USA). The surveys were collected based on overall experiences and observations.
A secondary analysis was conducted in which data from the first two (run-in) patients were excluded, and only i-STAT BGA (and not hospital central laboratory) BG values were used as reference.
Descriptive statistical analysis, using real-time data, was performed with SAS software, V.9.3, 2013 (SAS Institute, Cary, North Calorina, USA).
Results
Baseline characteristics
A total of 21 patients were enrolled in the study between March 27 and August 23 of 2012, and all patients successfully completed the study. Demographics, baseline characteristics and admitting diagnoses of study participants are presented in table 1. The mean age was 65 years, 38% were women, 90% were Caucasian, and 67% had diabetes; 20 were admitted to the cardiothoracic ICU following cardiac surgery, and one was admitted to the cardiac ICU with the diagnosis of acute myocardial infarction. Types of surgery included coronary artery bypass graft (CABG, 33%), valve replacement (29%), combined CABG and valve replacement (19%), and cardiac transplantation (14%). Two patients (10%) had high STS score, 11 (52%) had low STS score, and in the remaining 8 patients STS score could not be calculated due to the nature of their surgery (eg, cardiac transplantation, etc). Nine patients (43%) exhibited compromised perfusion within 24 h after ICU admission.
Baseline patient characteristics
Accuracy
A total of 870 SG-BG paired values were available which combined the i-STAT and central laboratory reference values; the overall MARD was 12.8% (95% CI 11.9% to 13.6%). Analysis of 854 SG-BG paired points above 75 mg/dL demonstrated a MARD of 12.5%. No clinically significant difference in MARD was observed across the prespecified subgroups of low versus high STS score (MARD 12.6% and 10.7% with STS >8% vs ≤8%, respectively). No clinically significant difference in MARD was noted across the subgroups of perfusion status (MARD 12.3% and 13.1% with compromised vs stable hemodynamics, respectively). For the three participants who underwent heart transplantation, MARD was 12.9%.
An overwhelming majority of the SG values were within the acceptable clinical accuracy zones. Consensus Error Grid analysis showed 99.2% of SG values to be within the A and B zones; 7 SG values (0.8%) were within the C zone, and 0 SG values (0%) were in the D and E zones (figure 2). No significant fixed bias was identified using Bland-Altman plot (figure 3).
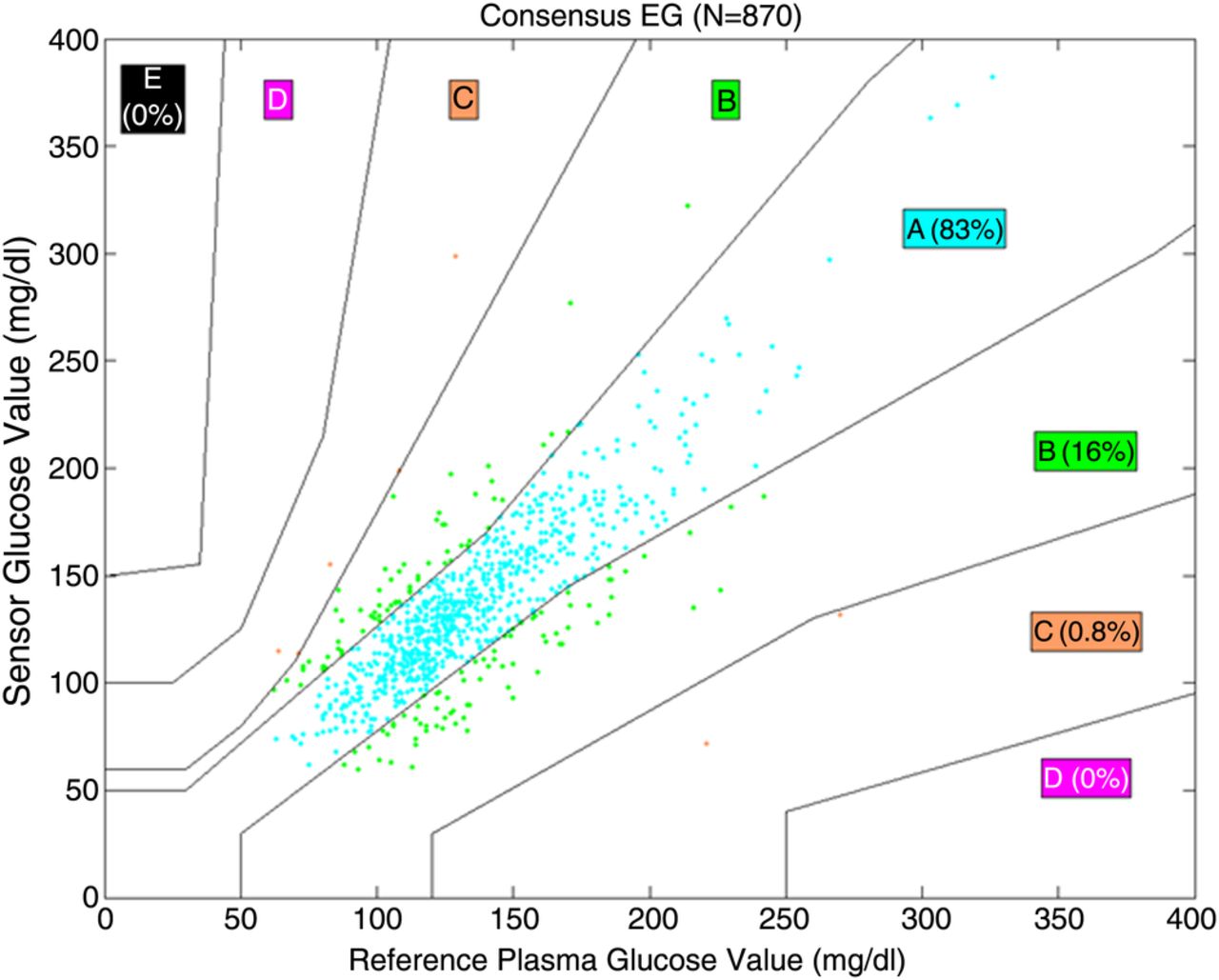
Consensus Error Grid (EG): 870 paired points, n=21 participants.

{kind=link}
{kind=link}
{kind=link}
Bland-Altman: 870 paired points, n=21 participants. iSTAT and laboratory Bland-Altman. Mean 2.5, upper limits 48.7, lower limits −43.7.
Secondary analysis of 19 phase 2 participants (total of 747 paired points using only i-STAT BG as reference) produced similar results: overall MARD was 12.8%, with no clinically significant differences across the subgroups; Consensus Error Grid analysis showed 99.1% of SG values to be within A and B zones, 7 SG values (0.9%) were within the C zone, and 0 SG values were within the D and E zones. No significant bias was identified using Bland-Altman plot.
Reliability
A total of 29 sensors were inserted in 21 patients during the study course. Of these, five sensors had to be replaced immediately due to suboptimal initial deployment; three additional sensors required replacement in order to complete the 72 h study period for issues unrelated to sensor performance (two due to the use of electrocautery, and one due to patient-inflicted damage to the processor cable).
‘On-time’ results are displayed in table 2. Overall median ‘on-time’ was 96.1% (IQR 95.3–97.2%). Median sensor-cause ‘on-time’ was 98.9% (IQR 98.2–99.7%). In the secondary analysis of phase 2 participants only, the reliability results were unchanged.
Reliability (on-time) of Sentrino continuous glucose management
Alarm performance
Alarm performance is summarised in table 3. Primary analysis calculated hyperglycemia and hypoglycemia threshold alarm performance using both reference values (i-STAT and central laboratory) in all participants (n=21). A total of 24 hypoglycemia events (defined as BG <80 mg/dL) were observed, of which Sentrino CGM system correctly identified 18 (true alarm rate of 75%, missed alarm rate of 25%). There were a total of 47 SG hypoglycemia alarms, of which 33 (70.2%) were false alarms. A total of 108 hyperglycemia events (as defined by BG >180 mg/dL) were observed, of which Sentrino CGM system correctly identified 98 (true alarm rate of 90.7%, missed alarm rate of 9.3%); there were 101 SG hyperglycemia alarms, 54 (53.5%) of which were false alarms.
Hypoglycemia/hyperglycemia alert and alarm using both reference values, n=21 participants
Safety
No anticipated or unanticipated device-related or study-related adverse events were reported.
Usability
When evaluating sensor insertion, 70% of research personnel found it ‘very easy’ to insert the sensor, while 30% found the experience ‘neutral’. Thirty-three of the 40 survey responders interacted with system; of these, 80% found the system easy to use after one patient, and 100% found it easy to use after two patients.
Discussion
In this single-center study of 21 patients hospitalized in the cardiac ICU, we found that when deployed in the intended-use environment and operated primarily by clinical nurses, the Sentrino CGM system exhibited good accuracy; good reliability that was in the ‘desirable performance’ range as suggested by the recent consensus recommendations,6 and was easily integrated into the flow of ICU care. Alarm performance was mixed: while missed alarm rate was low in the hyperglycemia range, it was higher for hypoglycemia; and the false alarm rates were high for both alarm types. The reliability of the estimate for hypoglycemia alarm performance was likely affected by the very low number of hypoglycemic events, and it is yet unclear what thresholds of alarm performance are optimal to result in clinical benefit (ie, improve time in the glucose target range and reduce hypoglycemia); this will need to be defined in future clinical trials. Finally, there were no device-related or study-related adverse events.
Several prior studies reported the use of subcutaneous continuous glucose monitoring technology in the ICU environment with variable results.8–11 While some previous investigations showed good accuracy and safety of several subcutaneous continuous glucose monitoring technologies (FreeStyle Navigator, Abbott Diabetes Care and Guardian, Medtronic Minimed) in the cardiac surgery patients,8 ,9 and one randomized clinical trial of continuous glucose monitoring versus usual care among general ICU patients even suggested a clinical benefit with hypoglycemia reduction in the continuous glucose monitoring group,4 results from other studies showed less optimal performance.10 ,11 However, these investigations used continuous glucose monitoring technology that was developed for the outpatient use, with limited applicability to the ICU environment. By evaluating the first minimally invasive continuous glucose monitoring device specifically designed for the ICU, allowing the clinical nurses to interact with the fully enabled system in the intended use setting, and collecting a broader range of outcomes (including reliability and usability), our study adds valuable and clinically relevant information to this field. Moreover, to the best of our knowledge, this is the first report of continuous glucose monitoring use in patients undergoing cardiac transplantation—a group that commonly experiences significant hyperglycemia.
With rapid evolution of continuous glucose monitoring technology, multiple devices are currently in development, including blood-based and minimally invasive products.7 While each technology has its advantages and limitations, one of the potential concerns with regard to subcutaneous CGM (given potential lag between BG and the interstitial fluid glucose) has been its accuracy among hemodynamically compromised patients with impaired tissue perfusion. Although the number of patients in our study was small, we found no clinically significant difference in Sentrino CGM system performance across the subgroups of surgical risk or hemodynamic stability. Ultimately, a broad array of continuous glucose monitoring devices with various accuracy, safety, and range of features would allow the most flexibility for clinicians to tailor the appropriate technology to the appropriate patient. Our data with regard to Sentrino CGM system's performance and safety profile, although preliminary and in need of confirmation, suggest that subcutaneous CGM technology may have a role in the monitoring of critically ill ICU patients, and should be further evaluated in appropriately designed and larger clinical trials.
The specific thresholds for treatment initiation and goals for glycemic management remain the subjects of intense debate, with clinical guidelines liberalizing glucose targets to a moderate range (ie, 140–180 mg/dL) and highlighting the importance of hypoglycemia avoidance in recent years,12 and many institutions adjusting their ICU glucose control protocols accordingly. Nevertheless, professional societies continue to recommend target-driven glucose control in the ICU environment when significant hyperglycemia is present.12 This is particularly important in the cardiac surgery patients, a group in which glucose control may improve patient outcomes and is strongly recommended by the professional guidelines.2 ,13 Since continuous glucose monitoring offers a promise of improved glucose control and less hypoglycemia, the development of this technology may be especially relevant to cardiac surgery patients. However, the potential clinical benefits of continuous glucose monitoring as compared with the current standard of care remain undefined, and need to be rigorously assessed in future studies. In addition to clinical outcomes, these studies should also evaluate the incremental cost-effectiveness of CGM technology as compared with the current standard of intermittent glucose monitoring. Ultimately, it is the combination of incremental clinical effectiveness and cost-effectiveness that will likely influence the clinical adoption of this novel technology in the ICU setting.
Our results should be considered in the context of several potential limitations. First, it was performed in a single tertiary care center with highly skilled and experienced ICU nursing staff, and limited predominantly to cardiac surgery patients. Therefore, its findings may not be generalizable to other hospitals or different patient populations. Second, the number of patients was relatively small, and our findings will need to be confirmed in larger patient groups. Third, hypoglycemic events were rare, making the accurate assessment of hypoglycemia detection by Sentrino CGM system difficult. Finally, we focused on the performance, safety, and usability of Sentrino CGM system and did not evaluate its impact on clinical outcomes.
Conclusion
In our single-center experience, Sentrino CGM system demonstrated good accuracy and reliability, with no device-related adverse events in critically ill cardiac patients; and was easy to use and integrate in the cardiac ICU. Future studies are needed to determine if the use of Sentrino can improve BG control and reduce hypoglycemia in this patient group.
Acknowledgments
The authors want to acknowledge and thank John Shin and Suiying Huang who provided the statistical analysis on behalf of Medtronic Diabetes.
References
Footnotes
-
Contributors MK, RKG, JAS and DP conceived the study and participated in its design and coordination. MK, JAS, DP, PK and MB provided administrative support. MK, DP, AG and PK participated in screening, enrollment and examination of patients. MK, RKG, JAS and DP analyzed and interpreted the data. MK, RKG and JAS drafted the manuscript. All authors participated in acquiring the data and in critical revisions of the manuscript for important intellectual content.
-
Funding This study was sponsored by Medtronic Minimed, Northridge, California, USA.
-
Competing interests MK has received research support from, and was previously a consultant for Medtronic Minimed. RKG and JAS are currently employees of Medtronic Minimed.
-
Ethics approval Saint Luke's Hospital of Kansas City Institutional Review Board.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement Additional data analyses can be provided at editors’ and reviewers’ request.