Article Text

Abstract
Objective Persons with diabetes have accelerated muscle loss. The association of fasting and postchallenge glucose levels per se to grip strength, a clinical marker of poor physical function, and potential sex differences in this relationship has not been previously described.
Design Longitudinal cohort.
Setting USA.
Participants Participants were community-dwelling older adults (mean age 71.3 years) without self-reported diabetes and/or use of diabetes medication with glucose measured at baseline (1992–1996).
Measurements Fasting plasma glucose (FPG) was measured in 1019 women and 636 men. Two-hour glucose (2HG) levels after a 75 g oral glucose tolerance test were also available (women, n=870; men, n=559). Dominant hand grip strength was assessed using a hand-held dynamometer at 3.0±1.6 visits over a median 7.0 years. Mixed linear models examined the association of baseline glucose levels with grip strength, accounting for repeated visits, and adjusting for covariates.
Results Sex-specific FPG quartiles were associated with unadjusted differences in grip strength among women (p=0.03) but not men (p=0.50). However, in men, adjusting for age, education, height, weight, peripheral neuropathy, physical activity, and comorbidities, each SD (SD=17 mg/dL) higher FPG was associated with persistently lower grip strength (−0.44±0.22 kg, p=0.049); 2HG (SD=50 mg/dL) was unrelated to grip strength (−0.39±0.25 kg, p=0.13). In women, neither FPG (SD=16 mg/dL) nor 2HG (SD=45 mg/dL) was associated with grip strength (0.02±0.12 kg, p=0.90; and −0.20±0.14 kg, p=0.14; respectively) after adjustment. The rate of change in grip strength did not differ across FPG or 2HG quartiles in either sex.
Conclusions In age-adjusted analyses, elevated fasting glucose levels are associated with persistently lower grip strength in older men, but not women. Future studies are needed to elucidate reasons for these sex differences and may provide further insight into accelerated loss of muscle function as a complication of diabetes in older adults.
- Elderly
- Sex Difference
- Muscle Weakness
- Epidemiology
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
Diabetes is associated with the accelerated loss of muscle function. However, it remains unclear the degree to which elevated fasting versus postchallenge glucose levels are related to lower grip strength—often considered a clinical marker of physical function—and if there are differences by sex.
In the present study, we found that elevated fasting glucose levels are related to lower grip strength in older men, but not women, and that these differences persisted during follow-up. We did not observe an association of 2 h glucose levels following oral glucose tolerance testing with grip strength in either sex.
These results may have implications for strategies to preserve muscle function and reduce the burden of disability in persons with diabetes. Future studies are needed to elucidate potential mechanisms for the sex differences observed.
Introduction
Diabetes is associated with accelerated loss of muscle mass and strength in the lower extremities.1 However, reports from studies exploring the association of diabetes with loss of muscle function in the upper extremities have been conflicting.1 ,2 In cross-sectional studies, the loss of arm muscle was greatest in those with longest duration of diabetes and highest levels of HbA1c (glycated hemoglobin),2 suggesting a potential role for dysglycemia in this process. It remains unclear whether the relationship between dysglycemia and muscle strength varies by upper versus lower extremity muscle, or whether the association of dysglycemia with muscle strength is confounded by use of therapies for diabetes or comorbidities, particularly the presence of peripheral neuropathy which was not consistently considered in previous cohorts. Inconsistent findings in previous studies exploring grip strength in persons with diabetes may be due to sex differences in the loss of muscle function with aging. Moreover, because grip strength is a reliable and inexpensive measure, and a strong predictor of poor physical functioning and mortality,3–5 grip strength could be used in clinical practice to risk stratify older adults. However, the degree to which dysglycemia per se is related to longitudinal changes in grip strength has not been previously investigated. Yet, exploring the associations between dysglycemia and grip strength may provide insight into possible pathways through which diabetes is related to poor physical functioning.
Sex differences in the loss of muscle function with aging are present in the general population where men have more rapid declines in muscle strength, mass, and quality compared with women.6–12 Because of the wider dynamic change of muscle strength in men than in women, differences due to pathology such as from chronic diseases may be amplified. Indeed, in cross-sectional studies of persons with diabetes, men have lower appendicular muscle strength, both upper and lower, despite having greater appendicular muscle mass compared with men without diabetes.2 This association was not reported in women, who despite greater arm and leg muscle mass in those with diabetes compared with those without diabetes had absolute arm and leg muscle strength at baseline that was not significantly different.2 Since the findings reported above were obtained in a single cohort (the Health, Aging, and Body Composition Study) and among participants followed for a relatively short duration, it is unclear whether the same results would be found in persons followed for a longer time and with repeated measures of grip strength. Of note, elevated fasting glucose levels have been consistently shown to be more common in older men than older women, whereas elevated postchallenge glucose levels are more common in older women than older men.13–17 Consequently, it remains unclear if sex differences in muscle function among persons with diabetes may be due, in part, to dissimilarity in fasting versus postchallenge glucose levels in men compared with women.
The present study tested the following hypotheses: (1) elevated glucose levels (both fasting and 2 h glucose (2HG) levels after a 75 g oral glucose tolerance test (OGTT)) are associated with decreased grip strength among persons without known diabetes at baseline independent of major confounders including demographics, anthropometry, peripheral neuropathy, physical activity, and comorbidities; and (2) sex differences exist in the associations of fasting and postchallenge glucose levels with grip strength during follow-up. We report these associations among a population-based cohort of older men and women from the Rancho Bernardo Study (RBS).
Methods
Study population
The RBS is a population-based cohort study of mostly non-Hispanic Caucasian, middle class residents (who had moved from all over the USA) of a southern California community. Between 1972 and 1974, approximately 82% (n=6629) of adult residents of this new suburb participated in the NIH Lipid Research Clinic Study of cardiovascular disease risk factors. Since then, research clinic visits have been conducted at regular intervals, all funded by the National Institutes of Health.18
The present study reports on 1781 participants in the 1992–1996 (visit 7); 111 of whom were excluded for self-reported diabetes and/or use of diabetes medications. An additional six participants did not have 75 g OGTT results available, leaving 1664 participants. Overall, 1655 participants (1019 women, 636 men) had measurement of baseline fasting plasma glucose (FPG) and 9 participants (7 women, 2 men) did not have fasting glucose available but only 2HG available. A total of 1420 participants (863 women, 557 men) had measurements of both FPG and 2HG levels after OGTT. All participants included in the study had at least one measure of grip strength available at baseline or follow-up (4 participants had a measurement during follow-up only). Subsequent research clinic visits occurred in 1997–1999 (visit 8), 1999–2002 (visit 9), 2003–2006 (visit 10), and 2007–2009 (visit 11). The mean number±SD of visits (including baseline) for participants in this study was 3.0±1.6.
The study was approved by the Institutional Review Board of the University of California San Diego; all participants gave written informed consent prior to participation.
Fasting and postchallenge glucose
A baseline 75 g OGTT was administered between 0730 and 1100 h after a minimum 8 h overnight fast. Blood samples were drawn by venipuncture at 0 and 2 h, and serum and plasma were separated and frozen at −70°C. Plasma glucose was measured by the glucose oxidase method.17
Covariates
Information about demographics (age, race, sex, and education), medical history, and peripheral neuropathy was obtained through standard questionnaires. Height and weight were measured while the participant was wearing light clothing without shoes. Physical activity was reported as physical exercise three or more times per week. Neuropathy was self-reported as numbness or tingling or sensation loss in the hands or feet, similar to other studies.19 The presence of other comorbidities also ascertained by questionnaire included the following: cancer (excluding non-melanoma skin cancer), lung surgery or emphysema, myocardial infarction or angina, hypertension, osteoporosis, arthritis, or stroke.20
Grip strength
Bilateral grip strength was measured using a hand-held dynamometer (Therapeutic Instruments Hand Dynometer, Serial No. 0687083). At the start position, the participant's elbow was flexed at a 90° angle with the forearm parallel to the floor. The dynamometer was maximally squeezed for a 3 s count while simultaneously lowering the arm to full extension. Participants practiced this procedure once per hand, after which measurements were recorded to the nearest 0.5 kg. The instrumental precision error was 1.0%.21 Similar to other authors, grip strength in the dominant hand was analyzed, defined as the hand with the larger grip strength value in kilograms in the present study.5 ,22–24
For 1019 women with FPG levels available, the number of grip strength measures available was: one visit (n=279), two visits (n=158), three visits (n=173), four visits (n=146), and five visits (n=263). For 636 men, the number of grip strength measures available was: one visit (n=178), two visits (n=86), three visits (n=114), four visits (n=88), and five visits (n=170).
Statistical analysis
Differences in baseline characteristics were summarized as means±SD and compared across sex-specific quartiles of FPG separately for men and women using analysis of variance for continuous variables and χ2 tests for categorical variables.
Next, dominant hand grip strength was plotted against age (in years) for participants in each FPG quartile using a local regression (loess) function separately for men and women, including baseline and follow-up data. Similar figures were plotted for participants categorized by sex-specific 2HG quartiles at baseline. Since there were relatively fewer participants aged <50 years (n=47) or >90 years (n=41), results are only shown for participants between the ages 50 and 90 years. We explored the interactions of FPG×age and 2HG×age with grip strength to test the hypothesis that age modified the association of baseline glucose levels with grip strength.
Mixed linear models were utilized to examine the regression of grip strength on baseline FPG (or 2HG) levels with unstructured within-participant covariance matrix. Other structures of the within-participant covariance were also considered (ie, compound symmetry, autoregressive (1), and Toeplitz) but the unstructured covariance matrix had the best model fit based on statistical parameters. Four models were fitted, which sequentially included covariates of interest: model 1 was unadjusted; model 2 was adjusted for age; model 3 was adjusted for model 2+education; model 4 was adjusted for model 3+height+weight; and model 5 was adjusted for model 4+peripheral neuropathy, physical activity, and the presence of individual comorbidities. Height and weight were adjusted for separately in regression models, similar to previous studies, given that higher body mass index as an anthropometric measure can be related to either increased muscle mass or adiposity.25 Peripheral neuropathy and education were only available for the baseline visit. The other covariates, including age, height, weight, physical activity, and other comorbidities, were included as time-varying variables in models. If any of the variables were missing for a particular visit, that visit was not included in the analysis.
In sensitivity analyses, we explored potential non-linear associations by adding a quadratic term in models. We performed sensitivity analyses excluding individuals with undiagnosed diabetes (participants with no known history of diabetes but who had FPG≥126 mg/dL or 2HG≥200 mg/dL) and those with undiagnosed diabetes prescribed glucose-lowering therapies during follow-up. We also performed a sensitivity analysis excluding women on estrogen replacement therapy at baseline. We conducted additional analyses to explore associations of dysglycemia with poor grip strength in the non-dominant (weaker) hand.
All p values presented are two-tailed, with p<0.05 considered statistically significant. Data were analyzed using SAS V.9.0.
Results
The mean baseline age (±SD) of 1656 participants was 71.3±11.4 years. The mean length of follow-up for participants was 7.4±5.7 years and similar for both sexes.
Table 1 shows unadjusted baseline participant characteristics by sex-specific FPG quartile among men. Weight and 2HG increased with increasing FPG quartiles (p<0.001). Higher rates of chronic diseases were reported with increasing FPG quartiles (p=0.004). Grip strength and other participant characteristics did not differ significantly by FPG quartiles. For men, the mean number of grip strength measures available for each participant by quartile of FPG was as follows: quartile 1 (n=3.0), quartile 2 (n=3.0), quartile 3 (n=3.0), and quartile 4 (n=2.8). Table 2 shows that among women, mean age (p<0.001) and education (p=0.02) increased with higher baseline FPG quartile. Weight and 2HG also increased with increasing FPG quartiles (p<0.001 for both). However, in contrast to men, grip strength was significantly different across FPG quartiles at baseline (p=0.03). For women, the mean number of grip strength measures available for each participant by quartile of FPG was as follows: quartile 1 (n=3.0), quartile 2 (n=3.0), quartile 3 (n=2.8), and quartile 4 (n=2.8). Other participant characteristics did not differ by FPG quartiles among women.
Unadjusted baseline participant characteristics by fasting plasma glucose quartile for men (n=636)*
Unadjusted baseline participant characteristics by fasting plasma glucose quartile for women (n=1019)*
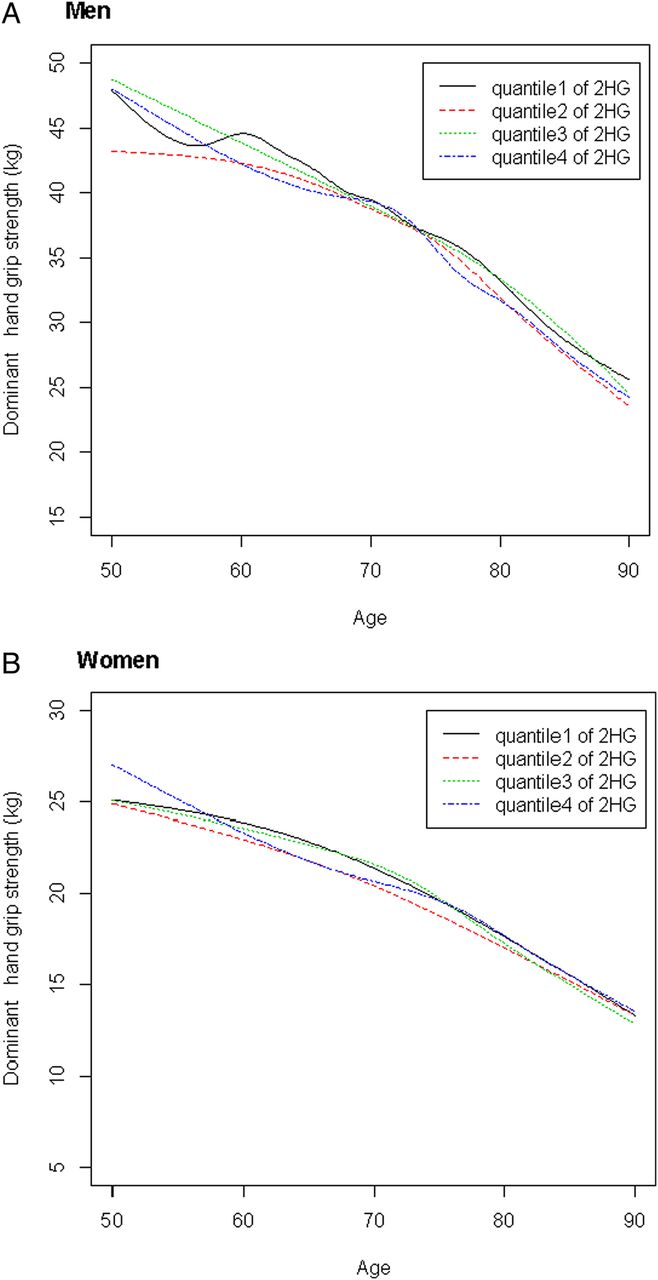
The age trajectory of grip strength, using both baseline and follow-up data were available for men and women categorized by baseline quartile of FPG and 2HG is shown in figure 1A (men) and 1B (women). Grip strength was lower among men in the highest FPG quartile compared with those in lower FPG quartiles after approximately the age of 65 years (figure 1A). Conversely, as shown in figure 1B, grip strength tended to be slightly higher in women in the highest versus lowest FPG quartile until the age of 85 years, but differences narrowed beyond this age. Figure 2A, B shows no consistent differences with aging for the highest versus lowest 2HG quartiles for men or women. However, there was no significant interaction with age by FPG (or 2HG) for either men or women (all p values >0.05).
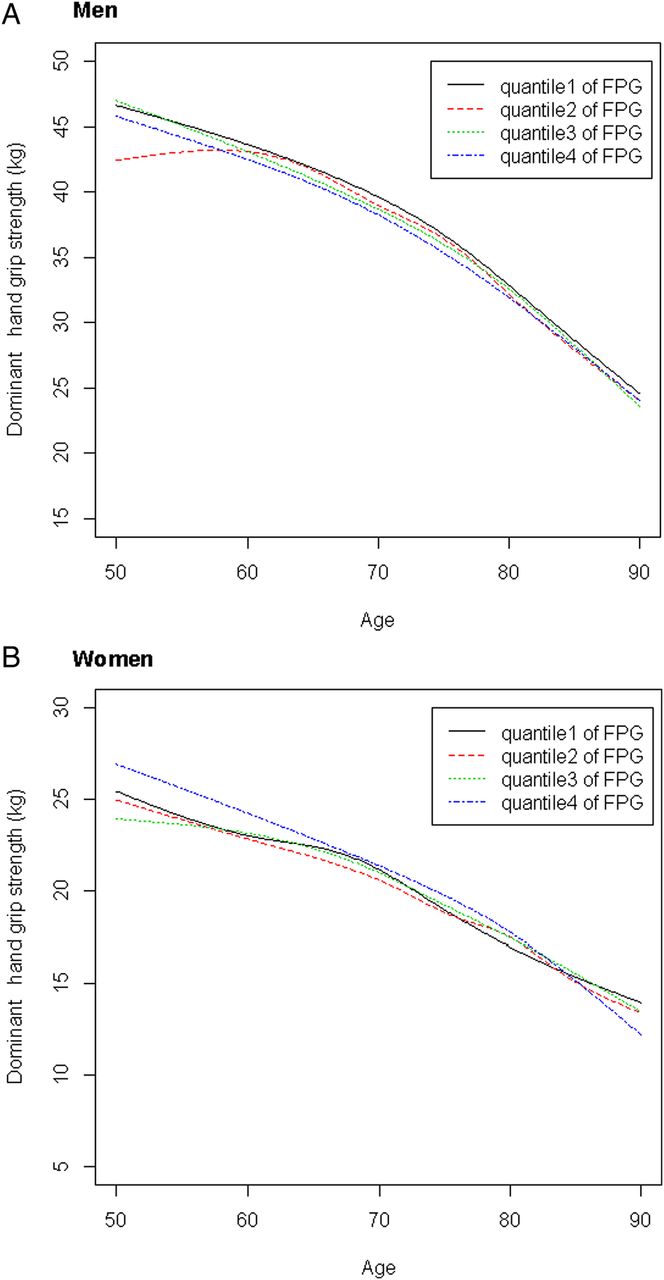
Mean decline in grip strength with aging by baseline quartile of fasting plasma glucose (FPG). For men (A), grip strength was lower among men in the highest FPG quartile compared with those in lower FPG quartiles after approximately the age of 65 years. For women (B), grip strength tended to be slightly higher in women in the highest versus lowest FPG quartile until the age of 85 years, but differences narrowed beyond this age. However, the rate of grip strength decline with age did not significantly differ by FPG quartile for either men or women (both p values >0.05).
{kind=link}
{kind=link}
Mean decline in grip strength with aging is shown for participants categorized by baseline quartile of 2 h glucose (2HG). For men (A) and women (B), there are no consistent findings across 2HG quartiles with aging. The rate of grip strength decline with age did not significantly differ by 2HG quartile for either men or women (both p values >0.05).
Mixed linear models examining mean differences in grip strength for each sex-specific SD increase in FPG (or 2HG) level during follow-up were performed. Among men and adjusting for age and education (table 3), increasing FPG levels (SD=17 mg/dL) were not related to grip strength (−0.20±0.24 kg per SD increase of FPG, p=0.39; model 2), but they were significantly associated with lower mean grip strength after further adjusting for height and weight (−0.43±0.22 kg per SD increase of FPG, p=0.045; model 3). These results remained significant in models adjusting for peripheral neuropathy, physical activity, and the presence of individual comorbidities (−0.44±0.22 kg per SD increase of FPG, p=0.049; model 4). Unadjusted, increasing 2HG levels (SD=50 mg/dL) were associated with significantly lower grip strength measures in men (−1.68±0.33 kg per SD increase of 2HG, p<0.001; model 1), but this association was no longer significant after adjusting for age and education (−0.29±0.28 kg per SD increase of 2HG, p=0.30; model 2), and remained non-significant in fully adjusted models (−0.39±0.25 per SD increase of 2HG, p=0.13; model 4). Among women, neither FPG (SD=16 mg/dL) nor 2HG (SD=45 mg/dL) was associated with grip strength after adjustment for covariates (table 3).
Mixed linear models exploring differences in grip strength among persons without history of diabetes by baseline fasting plasma glucose (FPG) and 2 h glucose (2HG) levels*
Among men, in sensitivity analyses, excluding those with undiagnosed diabetes (n=60), increasing FPG was negatively but non-significantly associated with lower grip strength measures in fully adjusted models (−0.36±0.25 kg per SD increase of FPG, p=0.15; SD=8.6 mg/dL). The relatively lower mean value for grip strength observed in FPG quartile 4 among men may have been related to the presence of persons with undiagnosed diabetes in this category. No significant associations with grip strength were found for 2HG among men in fully adjusted models (−0.12±0.27 kg per SD increase, p=0.66; SD=32.6 mg/dL). Among women, excluding those with undiagnosed diabetes (n=78), increasing FPG was negatively but non-significantly associated with lower grip strength measures in fully adjusted models (−0.23±0.14 kg per SD increase, p=0.09; SD=8.5 mg/dL). No significant associations with grip strength were found for 2HG among women in fully adjusted models (−0.04±0.15 kg per SD increase, p=0.77; SD=32.4 mg/dL). Also, in analyses which included a quadratic term for FPG or 2HG, respectively, non-linear associations were not found among men or women in fully adjusted models.
In sensitivity analysis, excluding persons with undiagnosed diabetes who were initiated on glucose-lowering therapies during follow-up (excluding 15 men and 18 women), we found that the association was more significant for FPG (−0.49±0.19 kg per SD increase, p=0.01; SD=13 mg/dL) and grip strength, with a trend toward significance for 2HG (−0.40±0.21 kg per SD increase, p=0.06; SD=42 mg/dL), among men in fully adjusted models, compared with the primary analysis. The results in sensitivity analysis were overall unchanged for the association of FPG (0.11±0.12 kg per SD increase, p=0.34; SD=14 mg/dL) and 2HG (−0.07±0.14 kg per SD increase, p=0.62; SD=44 mg/dL) with grip strength among women in fully adjusted models.
Among women, excluding those using estrogen replacement therapy (n=460) at baseline, FPG (−0.05±0.16 kg per SD increase, p=0.75; SD=20 mg/dL) and 2HG (−0.26±0.18 kg per SD increase, p=0.16; SD=47 mg/dL) remained non-significantly associated with lower grip strength measures in fully adjusted models.
In additional sensitivity analyses exploring associations of dysglycemia with grip strength in the non-dominant hand, FPG was significantly associated with grip strength in men in models adjusting for age, education, height, weight, and peripheral neuropathy (−0.53±0.24 kg per SD increase of FPG, p=0.03; model 4); results were similar for 2HG (−0.65±0.28 kg per SD increase of 2HG, p=0.02; model 4). However, after excluding those with undiagnosed diabetes, the associations of FPG and 2HG with non-dominant hand grip strength were no longer significant among men. No significant associations were observed for either FPG or 2HG with non-dominant grip strength among women in any of the models.
Discussion
In the present study, we found that among men without history of diabetes followed for an average of 7 years, increasing levels of FPG were associated with persistently lower grip strength. Even after accounting for potential confounders such as age, education, height, weight, physical activity, peripheral neuropathy, and comorbidities among men, the association of higher FPG with persistently lower grip strength remained significant. Such associations were not observed among women in our study, and 2HG was not associated with differences in grip strength among either men or women. Previous cross-sectional studies have reported that diabetes status (diagnosed and undiagnosed) was associated with significantly lower grip strength, in men but not women.2 ,26 However, one longitudinal study demonstrated no differences in grip strength over time in older adults by diabetes status.1 To our knowledge, our study is the first to specifically report the association of dysglycemia (FPG vs 2HG levels) with differences in grip strength among persons without known diabetes. We did not see an association of fasting glucose level with change in grip strength during aging. Rather, men with higher fasting glucose levels had lower grip strength at baseline and that difference persisted over time in those with repeated measurements. The duration of follow-up in our study was much longer than those in previous reports of grip strength in persons with diabetes (∼3 years) which may have contributed to our ability to detect significant differences.1 Sex differences have been previously reported in the cross-sectional association of 2HG levels with grip strength.26 Higher 2HG was associated with reduced grip strength in men without diabetes, but this relationship was not as dramatic in women; however, associations of FPG with grip strength were not explored in the previous cross-sectional study.26 It is possible that we may not have observed a relationship between 2HG and grip strength due to increased variability of 2HG levels compared with FPG levels.27 Alternatively, elevated FPG levels broadly reflect hepatic insulin resistance whereas elevated 2HG levels reflect peripheral insulin resistance, and each biomarker of glucose metabolism may have distinct associations with muscle strength.
Of note, longitudinal studies exploring loss of skeletal muscle mass by diabetes status have demonstrated the greatest loss of appendicular muscle mass (both arms and legs) in persons with undiagnosed diabetes, followed by persons with diagnosed diabetes, and then persons with no diabetes.1 These results may suggest a potential role for dysglycemia in the observed decline of appendicular lean mass. Further, among older men without history of diabetes, increasing quartiles of insulin resistance (assessed by Homeostatic Model Assessment-Insulin Resistance (HOMA-IR)) were associated with greater loss of appendicular and total lean body mass over an average of ∼5 years.28 Although we focused on associations of dysglycemia with grip strength, these prior results together with those of our study suggest that dysglycemia may have a more wide-ranging impact on upper extremity muscle function that should be further explored in future studies. Other authors have described sex differences in the loss of lower extremity strength in the general population with aging,6 and reported a significant interaction effect of diabetes and sex on longitudinal changes in thigh muscle cross-sectional area by CT but no sex differences in grip strength.29 In contrast, our study demonstrated sex differences in the association of fasting glucose levels with persistently lower grip strength over time in persons without known diabetes and who were not on glucose-lowering therapies that may have otherwise impacted observed associations in previous studies.
The potential implications of our study are that dysglycemia may be a risk factor for decreased grip strength, a marker for lower overall muscle strength, particularly in men and ultimately relate to the development of functional limitations and physical disability in older adults. Biological plausibility was suggested by the dose–response relationship of elevated fasting glucose levels with lower grip strength in men. Possible explanations for the sex differences observed in our study may involve differences in body composition between men and women as well as differences in upper body strength related to the fact that women tend to have a lower proportion of lean tissue distributed in the upper body.7 Also, previous studies have found that men have larger muscle fibers in both the upper and lower extremities compared with women.30 Other possible explanations for the observed sex differences include differences related to hormonal etiologies. The greater loss of muscle mass observed in men may be related to declines in growth hormone and androgens with aging.12 The antioxidant properties of estrogen in premenopausal women particularly may be related to an attenuated inflammatory response after exercise and protection from exercise-induced muscle damage compared with men, but findings of previous studies have been inconsistent and require further investigation.31–34 Physical activity level may also differ by sex and impact changes in muscle function with aging; however, we found that associations were independent of activity level in our study.
Several limitations to our study should be considered. Rancho Bernardo was a typical suburb at the time that included mostly white, well-educated, mostly married participants. Results may not be generalizable to other populations. Glucose levels were only assessed at baseline because OGTT was performed only at this time; participants’ glycemic status may have changed over time. Future studies in other cohorts should examine the relationship of changes in glycemic status with grip strength over time, and other glucose biomarkers such as HbA1c. Persons with undiagnosed diabetes may have been prescribed glucose-lowering therapies during follow-up which impacted the significance of our findings. However, in sensitivity analysis excluding these individuals, the association of FPG and grip strength in men was more significant. Thus, the results of our primary analysis represent relatively more conservative estimates. Physical activity and peripheral neuropathy were self-reported rather than objectively assessed; thus, the possibility of residual confounding cannot be excluded. Though repeated measures of grip strength were available in most participants, some individuals had only one measure. However, the mixed linear model is able to appropriately account for individuals with single or multiple measures available. The clinical implications of the differences in grip strength observed remain unclear and should be explored in future studies; however, a decrement of even a few kilograms has been associated with functional limitations and disability in older ages.4 Of note, the average annual decline in grip strength in older women aged 65–79 years has been reported to be approximately 0.5 kg/year in a previous study,35 and in our study which included relatively younger participants, the average annual decline in grip strength was 0.32 kg/year for women and 0.61 kg/year for men (p value for interaction by sex <0.001; data not shown). Thus, these age-related changes are comparable in magnitude to the grip strength differences in the highest versus lowest FPG quartile observed among men in our study. Also, we focused on associations of dysglycemia with upper extremity strength in the present study; the degree to which this correlates with similar changes in lower extremity strength in these participants was not explored in our study but should be explored in the future.
The strengths of our study include the well-defined protocols and characterization of participants in the RBS. We also had relatively long follow-up with repeated measures of grip strength in the majority of our participants. Given the relatively large sample size, we could explore sex differences in observed associations. Because all participants without known diabetes had an OGTT at baseline, we were also able to contrast the associations of both fasting and postchallenge glucose levels with grip strength over time, which has not been previously investigated in other studies. Finally, we were able to assess the relation between dysglycemia and grip strength without concern of potential confounding by therapies for diabetes. In conclusion, our longitudinal study demonstrates sex differences in the association of fasting glucose levels with decreased grip strength in older adults. The role of sex hormones and possible mechanisms underlying the observed differences between men and women warrant further investigation.
References
Footnotes
Contributors RRK, CK, LF, GAL, DK-S, and EB-C contributed to the study concept and design, methods, data analysis and interpretation of data, and preparation of the manuscript. GAL and EB-C contributed to data acquisition. SK and BN also contributed to study methods, data analysis, and interpretation of data.
Funding This work was supported by the National Institute of Diabetes and Digestive and Kidney Diseases (K23-DK093583), the Johns Hopkins Older Americans Independence Center (P30-AG021334), and the intramural research program of the National Institute on Aging. Data collection for the Rancho Bernardo Study was funded by NIDDK (DK31801), and NIA (AG07181; AG028507). Parts of this study were presented in abstract form at the 74th Scientific Sessions of the American Diabetes Association in San Francisco, California, June 13–17, 2014.
Competing interests None declared.
Ethics approval The study was approved by the Institutional Review Board of the University of California San Diego.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.