Article Text

Abstract
Objective In patients with diabetes mellitus, metformin treatment is associated with reduced mortality and attenuation of cardiovascular risk. As a subanalysis of the Glycometabolic Intervention as adjunct to Primary Coronary Intervention in ST Elevation Myocardial Infarction (GIPS-III) study, we evaluated whether metformin treatment in patients with ST-segment elevation myocardial infarction (STEMI) without diabetes improves the cardiovascular risk profile.
Methods A total of 379 patients, without known diabetes, presenting with STEMI were randomly allocated to receive metformin 500 mg twice daily or placebo for 4 months.
Results After 4 months, the cardiovascular risk profile of patients receiving metformin (n=172) was improved compared with placebo (n=174); glycated hemoglobin (5.83% (95% CI 5.79% to 5.87%) vs 5.89% (95% CI 5.85% to 5.92%); 40.2 mmol/mol (95% CI 39.8 to 40.6) vs 40.9 mmol/mol (40.4 to 41.2), p=0.049); total cholesterol (3.85 mmol/L (95% CI 3.73 to 3.97) vs 4.02 mmol/L (95% CI 3.90 to 4.14), p=0.045); low-density lipoprotein cholesterol (2.10 mmol/L (95% CI 1.99 to 2.20) vs 2.3 mmol/L (95% CI 2.20 to 2.40), p=0.007); body weight (83.8 kg (95% CI 83.0 to 84.7) vs 85.2 kg (95% CI 84.4 to 86.1), p=0.024); body mass index (26.8 kg/m2 (95% CI 26.5 to 27.0) vs 27.2 kg/m2 (95% CI 27.0 to 27.5), p=0.014). Levels of fasting glucose, postchallenge glucose, insulin, high-density lipoprotein cholesterol, and blood pressure were similar in both groups.
Conclusions Among patients with STEMI without diabetes, treatment with metformin for 4 months resulted in a modest improvement of the cardiovascular risk profile compared with placebo.
Trial register number NCT01217307.
- Cardiac Function
- Cardiovascular Disease Risk
- Cardiovascular Risk Factors
- Metformin
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
In patients with acute myocardial infarction at risk for diabetes, 4 months of treatment with metformin on top of optimal treatment resulted in a modestly more favorable cardiovascular risk profile compared with placebo.
Perhaps the most important and clinically the most relevant observation was the reduction in weight gain associated with metformin use. Weight loss may be the key factor responsible for metformin's alleged cardioprotective effects.
Metformin resulted in an improvement of cholesterol levels on top of optimal statin therapy.
Introduction
After ST-segment elevation myocardial infarction (STEMI), secondary prevention therapies as recommended by current guidelines such as β-blockers, ACE inhibitors, platelet aggregation inhibitors (acetylsalicylic acid and others), and lipid-lowering drugs all have been proven to reduce mortality and attenuate cardiovascular risk profile.1 In addition to the targeted substrates by current therapies, such as blood pressure, neuroendocrine activation, and increased thrombogenicity, glycometabolic dysregulation is strongly associated with adverse outcome after STEMI.2 Impaired fasting glucose and insulin resistance is associated with impaired prognosis, even at levels of dysglycemia not yet diagnostic of diabetes mellitus.3–5 Dysglycemia is common in patients with STEMI—as much as one in every four patients have undiagnosed diabetes and up to one in every two patients has prediabetes.6 Although glycometabolic dysregulation is both common and strongly associated with adverse outcomes after STEMI, it nonetheless is not a target of current pharmacotherapy.
Metformin is an effective glucose-lowering biguanide and currently the most widely used oral antihyperglycemic agent.7 Metformin has been shown to improve cardiovascular outcome, with a benefit that exceeds the benefit that may be expected solely by blood glucose lowering.8–18 In patients with diabetes mellitus and cardiovascular disease, metformin was associated with reduced all-cause mortality compared with other antihyperglycemic strategies.8–11 Long-term metformin treatment in patients at risk for or with diabetes improved cardiovascular risk profile mediated by weight loss, improved insulin resistance, reduction of the metabolic syndrome, and by lowering total and low-density lipoprotein (LDL) cholesterol.13–21 Further, in patients at risk for diabetes, but without cardiovascular disease, metformin reduced diabetes development with 30–40%.13–16
We aimed to evaluate if metformin treatment, on top of standard care, would improve cardiovascular risk in patients without diabetes. We therefore conducted this prespecified subanalysis in the ‘Metabolic Modulation With Metformin to Reduce Heart Failure After Acute Myocardial Infarction: Glycometabolic Intervention as adjunct to Primary Coronary Intervention in ST Elevation Myocardial Infarction (GIPS-III)’ study, that enrolled patients without diabetes who underwent primary percutaneous coronary intervention (PCI) for STEMI.
Methods
The study design and baseline characteristics of the single-center, randomized, double-blind, placebo-controlled GIPS-III trial have been reported previously.22 ,23 In brief, patients presenting at the University Medical Center Groningen between January 1, 2011 and May 26, 2013 who underwent acute catheterization for suspicion of STEMI were considered for this trial. Patients older than 18 years who underwent a successful primary PCI with implantation of at least one stent were eligible. Exclusion criteria were known diabetes (defined as documented history of diabetes, current use of antihyperglycemic medication or verbal confirmation by the patient, or glycated hemoglobin (HbA1c) of ≥6.5% (48 mmol/mol) prior to admission),24 previous myocardial infarction, severe renal dysfunction, need for coronary artery bypass grafting, conditions resulting in inability to provide informed consent, and conditions that interfered with the ability to comply with the protocol.
The study protocol was in accordance with the Declaration of Helsinki (Fortaleza, 2013), Dutch laws, and was approved by the local ethics committee (Groningen, the Netherlands) and national regulatory authorities. The study received financial support from the Netherlands Organization for Medical Research (ZonMw; grant nr. 95103007); the funding source had no role in the study.
Procedures
The study procedures and main outcomes have been described in detail.22 ,23 In short, immediately after coronary angiography and subsequent coronary intervention, 379 patients were randomly allocated to metformin 500 mg or visually matching placebo, both administered twice daily. Patients provided verbal informed consent during the PCI procedure and the first dose was administered immediately after arrival at the coronary care unit (CCU).
At admission, body weight, height, blood pressure, and heart rate were measured, and body mass index (BMI) was calculated. Blood was drawn during primary PCI, and blood glucose, HbA1c, insulin, creatinine, and cholesterol levels were assessed. A detailed history including cardiovascular risk profile was assessed during hospitalization. Patients arriving at the CCU between 00:00 and 20:59 were subjected to a standardized oral glucose tolerance test (OGTT) with 75 g of glucose (dissolved in 200 mL water) the following morning.24 In patients arriving at the CCU between 21:00 and 23:59, the OGTT was performed the second morning after admission. During the OGTT in the CCU all patients had already taken at least one to maximally four tablets of study medication. All patients received standard medication according to current guidelines, received counseling on diet, smoking, and lifestyle and were offered a cardiac rehabilitation programme.1 ,25 Patients who were diagnosed with new-onset diabetes were seen by an endocrinologist.
Patients visited the outpatient clinic 2 weeks, 7 weeks, and 4 months after discharge. At 4 months, a standardized OGTT was performed after an overnight fast of at least 8 h. In order to assess whether the study medication actually affected underlying dysglycemia rather than masking its presence, the OGTT was scheduled at least 3 days after stopping the study medication.
End points and definitions
Primary outcomes in this prespecified analysis from the GIPS-III trial were levels of, and change in HbA1c, fasting glucose, postchallenge glucose, insulin levels, cholesterol levels, body weight, BMI, and blood pressure at 4 months, adjusting for baseline levels.
Analysis of glucose, hemoglobin, creatinine, and total cholesterol, LDL-cholesterol, high-density lipoprotein (HDL) cholesterol was performed as part of standard care on standard laboratory assays (Roche Modular, Roche Mannheim, Germany). HbA1c was measured using an immunochemical assay (Tosoh G8, Tosoh Bioscience Inc, South San Francisco, USA). Insulin levels were determined post hoc from blood samples stored at −80°C on a chemoluminescence immunoassay (Architect i2000 SR Immunoassay analyzer, Abbott Diagnostics, Abbott Park Illinois, USA). Blood samples, other than specific glucose samples for assessment of fasting glucose, were non-fasting samples.
An independent end point adjudication committee, blinded to treatment allocation, using data on HbA1c levels, OGTT, and use of medication assessed diabetic state. Diabetes was defined as an HbA1c of ≥6.5% (48 mmol/mol), and/or a fasting blood glucose of ≥7.0 mmol/L and/or a 2 h postchallenge blood glucose concentration of ≥11.1 mmol/L; prediabetes as an HbA1c between 5.7% (39 mmol/mol) and 6.4% (47 mmol/mol), and/or a fasting blood glucose of 5.6–6.9 mmol/L, and/or a 120 min postchallenge blood glucose 7.8–11.0 mmol/L; patients not meeting any of these criteria were classified as normoglycemic.24
Statistical analyses
Continuous variables are reported as means±SD or medians (IQR) for normally and non-normally distributed data, respectively. Differences between groups were tested using Student t test or analysis of variance for normally distributed data, and Wilcoxon or Kruskall-Wallis tests for non-normally distributed data. Differences in proportions were assessed using χ2 tests. Analysis of covariance was used to evaluate differences in continuous variables at 4 months, adjusting for baseline values, reported as mean with 95% CIs. Multivariable linear regression was used to investigate associations between continuous variables and treatment, and to adjust for potential confounders.
Linear mixed-effects models were used to evaluate the trajectories of variables over time. These models included time and an interaction with study treatment as fixed effects (population-level estimates) and allowed for participant-specific variation in baseline levels and changes (a so-called random slope, random intercept model). Linear, cubic, and quadratic time transformations were considered; best fit for the fixed effects structure was selected based on akaike criterion information (AIC) and bayesian criterion information (BIC) (measures for model fit; lower is better), while the best random effects structure was evaluated via likelihood ratio tests in nested models. The interaction between treatment and time indicates whether a different trajectory (slope) exists between the two treatment groups. All reported p values are two-sided, and a p value of <0.05 was considered significant. All analyses were performed using R: A Language and Environment for Statistical Computing, V.3.02 (R Foundation for Statistical Computing, Vienna, Austria).
Results
At baseline, HbA1c measurements were available in all but 6 (1.6%) patients. Of these 373 patients, 27 (7.2%) had an HbA1c of ≥6.5% (48 mmol/mol; 12 in the placebo group and 15 in the metformin group) and excluded for the current analysis, resulting in 346 patients without diabetes.
The baseline characteristics of the patients for both groups (metformin group, n=172; placebo group, n=174) are presented in table 1. Both groups were comparable at baseline regarding age, sex, cardiovascular risk profile, cardiovascular history, physical diagnostic measurements, and baseline markers reflective of renal function, glycometabolism, and cholesterol profile.
Baseline characteristics
HbA1c concentration
At 4 months, HbA1c levels in the metformin group were slightly lower than in the placebo group, adjusting for baseline values (table 2). The mean absolute change in HbA1c concentration from baseline to 4 months was 0.06 (95% CI 0.03 to 0.10%); 0.66 mmol/mol (95% CI 0.33 to 1.09) in the metformin group and 0.12% (95% CI 0.08% to 0.15%); 1.31 mmol/mol (95% CI 0.87 to 1.64) in the placebo group (p=0.049; figure 1A). Figure 2 shows the change in HbA1c levels over time in both groups, fitted using a smoothed spline. A linear mixed-effects model evaluating change in HbA1c over time showed a significant interaction between time and study treatment (p=0.031), indicating different trajectories between the metformin and placebo group (figure 2).
Measurements of glycometabolic state and cardiovascular risk profile at 4 months

Change in markers of glycometabolism and cardiovascular risk profile. Absolute changes in (95% CI) the metformin and placebo groups in glycated hemoglobin (HbA1c) concentration (A), insulin levels (B), body weight (C), total cholesterol (D), low-density lipoprotein (LDL)-cholesterol (E), and high-density lipoprotein (HDL)-cholesterol (F) were analyzed using analysis of covariance.
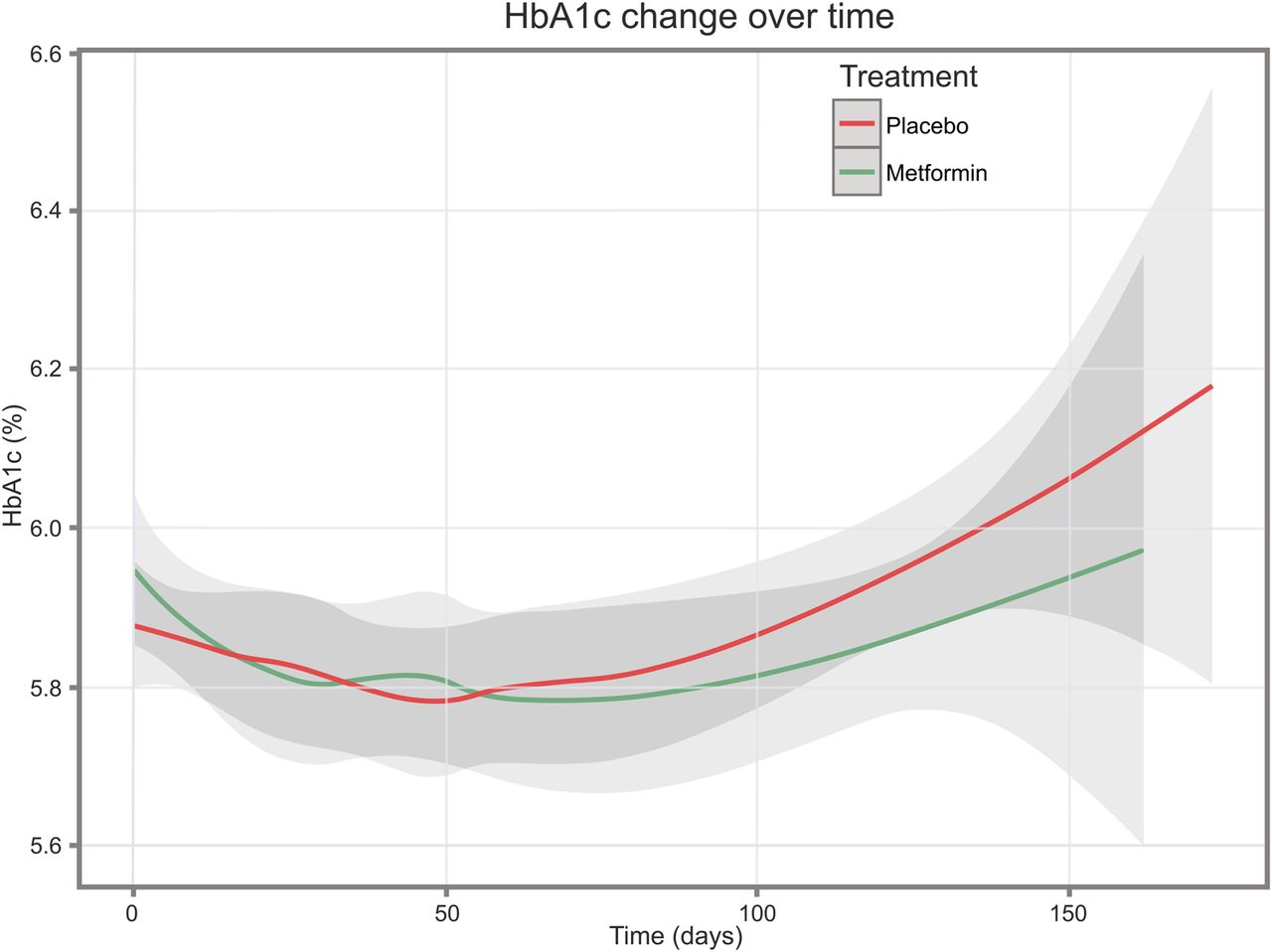
Change in glycated hemoglobin (HbA1c) over time. Trajectories of change in HbA1c over time (95% CI) were analyzed using linear mixed-effects model, showing different trajectories between the two treatment groups (p=0.031).
Fasting glucose and postchallenge glucose
All patients underwent an OGTT during hospitalization whereas 28 patients (7.5%) refused an OGTT at 4 months (10 patients (5.7%) in the metformin group and 18 patients (10.5%) in the placebo group).
During hospitalization for STEMI, the metformin and placebo group had similar fasting glucose levels (6.4±1.0 vs 6.4±0.9 mmol/L, p=0.75), whereas the 120 min postchallenge glucose levels were lower in the metformin group compared with placebo (10.0±2.7 vs 10.6±2.5 mmol/L; p=0.03; figure 3A). Four months after STEMI and after stopping the study medication for at least 5 days, there were no differences between the metformin and placebo group concerning the fasting glucose levels (5.6±0.6 vs 5.6±0.7 mmol/L, p=0.76) and the 120 min postchallenge glucose levels (7.7±2.2 vs 7.8±2.2 mmol/L, p=0.83; figure 3B).

{kind=link}
{kind=link}
{kind=link}
Oral glucose tolerance testing during hospitalization and at 4 months after infarction. Bar and whisker plots demonstrating blood glucose concentrations during hospitalization (A) and at 4 months (B). Each plot shows fasting blood glucose concentration left of the dotted line, and 120 min postchallenge glucose concentration right of the dotted line. The bars represent median (p50) and IQR (p25 and p75) and the whiskers p5 and p95.
Insulin levels
Twenty-four hours after PCI, the non-fasting insulin level in the metformin group was 34.5 mU/L (95% CI 29.3 to 39.6) and 33.2 mU/L (28.4 to 38.1) in the placebo group (p=0.274). The mean absolute change in insulin levels from baseline to 24 h was 9.2 mU/L (95% CI 4.0 to 14.3) in the metformin group and 7.9 mU/L (95% CI 3.1 to 12.8) in the placebo group (p=0.914). Also at 4 months, insulin levels in the metformin group did not differ from the placebo group, adjusting for baseline values (table 2). The mean absolute change in insulin levels from baseline to 4 months was −3.3 mU/L (95% CI −8.64 to 2.0) in the metformin group and −7.5 mU/L (95% CI −12.6 to −2.4) in the placebo group (p=0.979; figure 1B).
Incidence of diabetes and prediabetes
New-onset diabetes, diagnosed at 4 months, was diagnosed in 20 patients (12%) in the metformin group and 18 patients (10%) in the placebo group (p=0.70). Prediabetes was diagnosed in the metformin group in 108 patients (63%) and in 123 patients (71%) in the placebo group (p=0.40) after 4 months.
Body weight and BMI
Four months after STEMI, body weight and subsequently BMI were lower in the metformin group compared with placebo (table 2). The patients in the metformin group did not gain weight (0.0 kg (95% CI −0.84 to 0.90), whereas the weight gain in the control group was 1.4 kg (95% CI 0.56 to 2.3; p=0.024; figure 1C). As a consequence, the BMI at 4 months was lower in the metformin group than in the placebo group (table 2). Another important factor possibly influencing body weight is cessation of smoking. The number of smokers at baseline did not differ between groups (table 1). At 4 months, there was no between-group difference in cessation of smoking: 52 patients in the metformin group had quit smoking versus 63 patients in the placebo group (p=0.39).
Total, LDL, and HDL cholesterol
The adjusted total cholesterol levels and LDL cholesterol levels in the metformin group were lower than the placebo group after 4 months (table 2). The mean reduction from baseline to 4 months in total cholesterol in the metformin group was 1.58 mmol/L (95% CI 1.45 to 1.70) and in the placebo group 1.40 mmol/L (95% CI 1.29 to 1.52; p=0.045; figure 1D), whereas the mean reduction in LDL-cholesterol was 1.74 mmol/L (95% CI 1.64 to 1.84) in the metformin group and 1.54 mmol/L (95% CI 1.44 to 1.64) in the placebo group (p=0.007; figure 1E). The adjusted HDL-cholesterol level did not differ among groups. The mean increase in HDL-cholesterol from baseline to 4 months was 0.04 mmol/L (95% CI 0.01 to 0.07) in the metformin group and 0.07 mmol/L/L (95% CI 0.04 to 0.10) in the placebo group (p=0.153; figure 1F). At baseline, only two patients in the metformin group and three patients in the placebo group had a LDL-cholesterol level of <1.9 mmol/L/L, which is the targeted level for cholesterol-lowering therapy.1 Despite overall lowering LDL values, 49 patients in the metformin versus 46 patients in the placebo group reached the LDL-cholesterol target level of <1.9 mmol/L (p=0.397) at 4 months. The statins used, and the equipotency of these statins did not differ between groups, since at baseline 12 patients in the metformin group versus 13 patients in the placebo group used statins, and at 4 months 153 vs 157 patients used statins (p=not significant for both time points). At hospital discharge, the statins used and equipotency did not differ (see online supplementary appendix, tables S1 and S2).
Blood pressure
The systolic and diastolic blood pressure at 4 months was similar in both treatment groups: 123 mm Hg (95% CI 120 to 125) and 74 mm Hg (95% CI 72 to 75) in the metformin group, and 125 mm Hg (95% CI 122 to 127) and 74 mm Hg (95% CI 72 to 75) in the placebo group (p=0.241 and p=0.649, respectively). The mean decrease in either systolic or diastolic blood pressure from baseline to 4 months did not differ between groups (data not shown).
Discussion
The main observation of this prespecified analysis from the GIPS-III trial is that metformin treatment in patients with STEMI for 4 months on top of standard care leads to a modestly improved cardiovascular risk profile compared with placebo in a subselection of patients without diabetes. HbA1c levels, weight gain, total cholesterol, and LDL-cholesterol levels were all lower in patients receiving metformin. A reduction in the incidence of new-onset diabetes was not observed. Furthermore, systolic and diastolic blood pressure, insulin levels, and HDL cholesterol levels remained unchanged by metformin treatment. These results imply that metformin might be able to modestly reduce the cardiovascular risk in patients without diabetes on top of standard care (including statin therapy). Whether these findings are substantial and can lead to a reduction in cardiovascular events remains to be determined.
Our results concerning HbA1c levels are comparable with results from the recent Carotid Atherosclerosis: MEtformin for insulin ResistAnce (CAMERA) study, that demonstrated that 18 months of treatment with metformin in patients with coronary artery disease without diabetes also resulted in a reduction of HbA1c levels.19 The Diabetes Prevention Program (DPP) demonstrated that 3 years of treatment with metformin 850 mg twice daily significantly lowered HbA1c in comparison to placebo.13 The DPP study demonstrated that metformin treatment at long-term follow-up resulted in a reduction in the development of diabetes.14 In all three studies (DPP, CAMERA, and the GIPS-III), the observed effect of metformin treatment on HbA1c was significant yet small. The use of markers of HbA1c as a prognostic marker is not unequivocal.25 However, the incremental prognostic value of HbA1c on top of standard risk factors has been established.26 Therefore, it is generally accepted that lowering HbA1c likely is associated with improved prognosis. Still, the clinical relevance of metformin-induced lowering of HbA1c on the incidence and risk of future major cardiac events remains to be determined.
During hospitalization, one to maximally four dosages of metformin treatment already resulted in a lower postchallenge blood glucose concentrations compared with placebo. Since we did not measure fasting insulin levels 24 h after PCI, this effect could be due to directly lowering insulin resistance, but also due to other glucose-lowering effects of metformin, such as reduction of hepatic gluconeogenesis may be of effect. Hyperglycemia is often present during and the days following myocardial infarction, and is associated with impaired myocardial reperfusion, larger myocardial infarct size, and impaired outcome.3 Therefore, many studies using insulin-based strategies have aimed at lowering glucose levels during myocardial infarction.27–29 However, none of those trials showed improved outcome, yet all of those trials concluded that lowering insulin resistance was achieved and associated with improved outcome. Regrettably, the insulin-based therapies instituted increased risk of hypoglycemia and mortality, resulting in an overall adverse effect. Our analysis suggests that metformin can lower glucose levels during STEMI, without the adverse effects of insulin-based lowering strategies. Whether administration of metformin prior to reperfusion, with adequate blood levels of metformin, in patients with STEMI (for instance in the ambulance) will result in improved outcome, cannot be deducted from this trial.
Another very interesting and important observation in our study was that metformin prevented weight gain. The overall weight gain after STEMI (in GIPS-III this was 1.4 kg in the placebo group) is likely due to inactivity after myocardial infarction. There was no difference in the number of patients who stopped smoking after STEMI between both groups, suggesting that cessation of smoking did not affect these results. The DPP study group calculated that 64% of the effect of metformin treatment on cardiovascular risk reduction was caused by weight reduction.30 Fontbonne et al20 demonstrated in The BIGuanides and Prevention of Risks in Obesity (BIGPRO1) study that metformin treatment (850 mg twice daily) for 1 year resulted a weight reduction of 1.2 kg compared with placebo. In support of this, Preiss et al19 demonstrated in the CAMERA study that metformin treatment for 18 months resulted in a mean weight loss of 3.2 kg compared with placebo. So, if weight reduction is one of the targets for improvement of cardiovascular risk, metformin should be considered as an addendum to achieve this.
Our study demonstrated that metformin effectively lowers LDL cholesterol and total cholesterol levels on top of initiation of statin therapy. The BIGPRO1 study showed that metformin treatment for 1 year resulted in a reduction of 0.16 mmol/L in total cholesterol and 0.12 mmol/L in LDL-cholesterol.20 However, these patients were not treated with statins or other lipid-lowering drugs. In contrast, Preiss et al19 did not report an effect of 18 months of metformin treatment on cholesterol levels in patients without diabetes with coronary artery disease in the CAMERA study. One of the eligibility criteria in the CAMERA study was statin therapy, which all patients received already for 6.5 years on average. In our study, only 25 of 346 (7.2%) of patients used statins since the STEMI mostly was their first presentation with cardiovascular disease, but at hospital discharge 99.5% of patients in our study received statins.22 Second, the total cholesterol levels at baseline in the CAMERA were much lower than in our trial (4.3 vs 5.3 mmol/L). Third, the average reduction in cholesterol level at 6 months was 0.03 mmol/L in the CAMERA trial, whereas in our trial on average a reduction of 1.4 mmol/L was observed, with a larger reduction in the metformin group compared with the placebo group. Since the effect of metformin lowering total cholesterol and LDL on top of statin therapy was clearly visible in our study, metformin may exert cholesterol-lowering qualities during initiation of treatment.
This prespecified substudy of the GIPS-III trial had several strengths. The GIPS-III had a double-blind, placebo-controlled trial, and included patients at the same time point in their illness, namely directly after PCI for STEMI. All end points were adjudicated by an independent end point committee. The dosages of metformin used (500 mg bid) are commonly used to treat type 2 diabetes mellitus. A potential weakness of the GIPS-III trial was that it was not designed for mortality reduction trough secondary prevention of the cardiovascular risk profile. However, several clinically relevant and targeted markers were lowered by metformin therapy, suggesting the sample size is sufficient to address cardiovascular risk profile. The study medication was only administered for 4 months, which in terms of secondary prevention is short.
Altogether, we observed that metformin treatment in patients without diabetes presenting with STEMI, resulted in prevention of gain in body weight, improved levels of HbA1c, and improved levels of LDL and total cholesterol. Estimating the total effect size on cardiovascular risk of these combined effects is difficult. A risk calculator for outcome after STEMI, integrating all important known variables, has yet to be developed. However, quantification of the effect sizes on outcome is necessary in order to establish the usefulness and benefit of metformin in secondary prevention. Therefore, further study on the effects of metformin on cardiovascular risk profile and prognosis in patients with STEMI are warranted. Currently, the Glucose Lowering in Non-diabetic hyperglycemia Trial (GLINT, ISRCTN34875079) is an ongoing double-blind, randomized controlled trial set to include over 12 000 patients designed to assess the effect of metformin in non-diabetic hyperglycemia on cardiovascular risk.
Conclusion
In patients with acute myocardial infarction at risk for diabetes, 4 months of treatment with metformin on top of optimal treatment resulted in a modestly more favorable cardiovascular risk profile compared with placebo. Metformin treatment improved glycemic control and cholesterol levels, and prevented gain in body weight. Whether these favorable effects on risk factors can be translated to improved long-term outcomes requires further study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Collaborators GIPS-III Investigators: Wouter G Wieringa, Ad FM van den Heuvel, Hendrik W van der Werf, Remco AJ Schurer, Gabija Pundziute, Eng S Tan, Hendrik M Willemsen, Bruce HR Wolffenbuttel, Bernard Dorhout, Hans L Hillege, Wybe Nieuwland, Peter van der Meer, René A Tio, Jenifer Coster, Yoran M Hummel, Barbara HW Molmans, Gert J ter Horst, Remco Renken, Anita J Sibeijn-Kuiper, Bart JGL de Smet, Albert C van Rossum, Robin Nijveldt, Jan GP Tijssen.
Contributors CPHL, ANAvdH-S, and ICCvdH researched data and wrote manuscript. EL, ACMK, RAdB, and DJvV contributed to discussion, reviewed/edited manuscript. MAEV and PvdH researched data, reviewed/edited manuscript.
Funding The GIPS-III study was supported by grant number 95103007 from ZonMw, the Netherlands Organization for Health Research and Development, The Hague, The Netherlands.
Competing interests RAdB reported receiving research grants from Abbott and BG Medicine Inc; serving as a consultant to Abbott, BG Medicine Inc, Novartis, and Medcon; receiving speakers’ fees from Abbott, BG Medicine Inc, Novartis, Pfizer, AstraZeneca, Baxter, and Biomerieaux; and holding ownership interest in Pectacea.com and scPharmaceuticals. DJvV reported receiving board membership fees and/or travel expenses from Amgen, Johnson & Johnson, Novartis, Sorbent, Vifor, BG Medicine, and BioControl..
Patient consent Obtained.
Ethics approval Medical Ethics Trial Committee, University Medical Center Groningen.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.