Article Text

Abstract
Introduction Recent studies have shown that insulin resistance (IR) is correlated to atherosclerosis development. However, few studies have investigated the association between IR and asymptomatic intracranial arterial stenosis (aICAS).
Research design and methods This cross-sectional study enrolled 2007 rural residents in China who were aged ≥40 years without a clinical history of stroke and transient ischaemic attack. We used transcranial Doppler ultrasonography in combination with magnetic resonance angiography to diagnose aICAS (stenosis ≥50%). IR was defined as a homeostasis model assessment of insulin resistance ≥3.0 based on the 75th percentile for all the participants. Multivariate logistic regression models were employed to assess the relationship of diabetic parameters with aICAS in all participants, as well as with aICAS in non-diabetic participants, and further stratified by sex.
Results After adjusting for age, gender, smoking habit, drinking habit, low-density lipoprotein cholesterol, raised blood pressure, triglycerides, high-density lipoprotein cholesterol and waist circumference, diabetes mellitus (DM) (OR=2.09, 95% CI 1.31 to 3.32), fasting plasma glucose (FPG) (OR=1.34, 95% CI 1.14 to 1.57), and IR (OR=1.75, 95% CI 1.11 to 2.75) were associated with aICAS in the total study population; however, these relationships remained significant only in men after the analyses were stratified by sex (DM: OR=3.40, 95% CI 1.62 to 7.13; FPG: OR=1.64, 95% CI 1.26 to 2.13; IR: OR=3.04, 95% CI 1.44 to 6.42). When further excluding the diabetic participants from the total study population, positive associations between IR and aICAS were similarly observed only in men (OR=4.65, 95% CI 1.69 to 12.82).
Conclusions IR might predict the prevalence of aICAS independently of major cardiovascular risk factors and metabolic syndrome components among men living in rural China.
- atherosclerosis
- insulin resistance
- metabolic syndrome
- asymptomatic diseases
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Insulin resistance (IR) is correlated to atherosclerosis process. IR may increase the risk of coronary calcification and higher carotid intima-media thickness, independently of conventional cardiovascular risk factors (CRFs).
What are the new findings?
In apparently healthy Chinese men, IR is associated with higher odds of asymptomatic intracranial arterial stenosis (aICAS), even after adjustments for major CRFs and metabolic syndrome components.
After excluding the participants with diabetes from analysis, IR remains independently related to a higher probability of having aICAS in non-diabetic men.
The established CRFs do not fully explain the association between IR and aICAS.
How might these results change the focus of research or clinical practice?
Our findings suggest that IR could be explored as a potential marker to identify rural Chinese men at risk of aICAS.
Introduction
Intracranial arterial stenosis (ICAS) is a leading cause of ischemic stroke worldwide and remains a significant target for stroke prevention, particularly among Asian populations.1 The identification of the modifiable risk factors associated with asymptomatic ICAS (aICAS) may facilitate the primary prevention of clinical stroke.2 However, one large-scale study reported that cardiovascular risk factors (CRFs), such as hypertension, diabetes mellitus (DM), dyslipidemia and obesity, could only explain <40% of the carotid intima-media thickness variance.3 Therefore, there is increasing interest in the investigation of new CRFs.
Type 2 DM is characterized by insulin resistance (IR), with elevated fasting plasma glucose (FPG) and insulin concentration. The association of aICAS with FPG was well established in previous studies.4 5 However, the association between IR and aICAS was unknown. As we all know, IR is associated with several CRFs and metabolic syndrome (MetS) components,6 while other studies have shown that IR may increase the atherosclerosis-related risks directly by mediating proinflammatory activity, influencing the endothelial function and macrophage recruitment.7 8 A Spanish study concluded that IR was an independent predictor for moderate to severe ICAS after adjustment of the rest of MetS components in a white population.9 However, studies that focus on this association among Asian population were scarce, and the association between IR and aICAS was unknown after adjustment for MetS components and conventional CRFs.
Due to the biological differences between men and women, including sex hormones levels, they share different risk factor profiles of intracranial atherosclerosis.10 Previous studies have shown that higher IR measured with homeostatic model assessment of insulin resistance (HOMA-IR) increased the risk of coronary calcification, independently of the presence of MetS components in Japanese men,11 and lower insulin sensitivity, measured using the euglycemic hyperinsulinemic clamp test, was associated with higher carotid intima-media thickness after the adjustment of the established risk factors in apparently healthy European men.12 Both of the two studies were analyzed among male population; therefore, the sex-based differences on the association of aICAS and IR in a general population remain unclear.
IR can be diagnosed using the euglycemic hyperinsulinemic clamp test that is considered the gold standard method for accurate assessment of insulin sensitivity. However, the use of this method is not feasible in large-scale or epidemiological studies owing to the expensive and time-consuming procedures involved. HOMA-IR derived from the mathematical modeling of FPG and insulin concentrations is a simple and inexpensive alternative for the evaluation of insulin sensitivity and has been widely accepted in large-scale studies because of its cost-effectiveness, convenience, and good correlation with the results of the gold standard method.13
Thus, the present study aimed to evaluate whether IR or DM is associated with aICAS prevalence independently of MetS components and conventional CRFs and to explore if the sex-based differences on the association between aICAS and IR or DM exist or not in a rural Chinese population.
Methods
Study design and study population
Participants in this study were enrolled in the Kongcun Town Study, which has been described in detail previously.14 15 The Kongcun Town Study is an ongoing population-based study that aimed to investigate the prevalence of aICAS and major CRFs or biomarkers related to the development and prognosis of aICAS. Briefly, 2311 rural residents have been enrolled who are aged ≥40 years without a clinical history of stroke or transient ischaemic attack and living in Kongcun Town, Shandong Province, China. From October 2017 to October 2018, information on demographics, socioeconomics, personal and family medical history, and lifestyle factors was collected through face-to-face interviews, physical examination and blood tests, and all the participants underwent transcranial Doppler (TCD) ultrasonography in phase I. Finally, 204 participants who were positive for aICAS on TCD ultrasonography were invited to undergo brain magnetic resonance imaging (MRI) and magnetic resonance angiography (MRA) examinations in phase II.
Participants were excluded from this study if they had missing information about demographics, anthropometrics measurements, TCD ultrasonography and blood test results, or with outlier of any continuous variables. Participants who were contraindicated for brain MRI and MRA, such as those with pacemakers and metal denture implantations were also excluded.
All the participants provided written informed consent for study participation. This study was conducted as per the principles for medical research involving human participants expressed in the Helsinki Declaration.
Data collection and assessment
Data on demographic characteristics, CRFs, anthropometric measurements, and blood biochemical markers were collected, as described previously.14 15 The fasting insulin level was measured using the electrochemiluminescence immunoassay (Roche Diagnostics, Mannheim, Germany). In this study, we defined hypertension as blood pressure level ≥140/90 mm Hg, use of antihypertensive drugs, or a previous diagnosis of hypertension. DM was defined as a FPG level ≥7.00 mmol/L, use of hypoglycemic drugs, insulin injection, or self-reported history of DM. Smoking was defined as smoking at least one cigarette per day for >1 year; current and previous smokers with a history of quitting for <6 months were included. Drinking was defined as alcohol consumption at least once a week for at least 6 months; current and previous drinkers with a history of quitting for <6 months were included.
Assessment of aICAS
The aICAS evaluation protocol has been described in detail previously.14 15 In brief, aICAS was initially screened using TCD examination and then diagnosed using MRA. At phase I, two experienced physicians with expertise in sonography performed TCD examination for all participants. The bilateral middle cerebral artery, anterior cerebral artery, posterior cerebral artery, vertebral artery and basilar artery were examined through a temporal window, occipital window and eye window, respectively. The diagnosis of ≥50% intracranial stenosis of various arteries followed the criteria described in the Stroke Outcomes and Neuroimaging of Intracranial Atherosclerosis trial.16 At phase II, participants who were screened positive by TCD underwent structural brain MRI and MRA scans. The severity of stenotic lesion in the examined arteries was classified into five grades as normal, mild (signal reduction <50%), moderate (signal reduction ≥50% and <70%), severe (signal reduction ≥70%) or occlusion, which were completed by a neurologist who specialized in stroke treatment (QS) and a clinical neuroradiologist (GW) together by consensus, according to the criteria in the Warfarin-Aspirin Symptomatic Intracranial Disease Study.17 All TCD and MRA findings were made blinded to clinical information. A previous study showed that aICAS with stenosis degree >50% could increase the risk of stroke.18 In addition, signal reduction ≥50% is a more explicit and severe outcome of atherosclerosis; it is more reliable to taking signal reduction ≥50% as the definition of aICAS, adding credibility to our findings. Therefore, in this study, aICAS was defined as having at least one lesion (signal reduction ≥50%) in any of the examined arteries.
Diagnosis of IR and MetS
Insulin sensitivity was measured using HOMA-IR, calculated with the following formula: HOMA-IR=FPG (mmol/L)×fasting insulin (mUI/L)/22.5.19 IR was defined as a HOMA-IR value ≥3.0 based on the 75th percentile for all the study participants.
As per the 2009 Joint Interim Statement, MetS was diagnosed if at least three of the following conditions were present: waist circumference (≥90 cm for men and ≥80 cm for women), high triglyceride level (≥1.7 mmol/L) or medication, decreased high-density lipoprotein cholesterol (HDL-C) level (<1.0 mmol/L for men and <1.3 mmol/L for women) or medication, increased blood pressure (systolic blood pressure (SBP) ≥130 mm Hg and/or diastolic blood pressure (DBP) ≥85 mm Hg) or medication, and elevated FPG level (≥5.6 mmol/L) or medication.20
Statistical analysis
All the analyses were performed with the Statistical Package for the Social Sciences software V.22.0 for Windows. The characteristics of the study participants are presented as mean and SD values for continuous variables with a normal distribution and as median and IQRs for continuous variables with a non-normal distribution. Categorical variables are presented as frequencies and percentages. Variables were compared as per sex or the presence of aICAS using t-test, Mann-Whitney U test, or χ2 test, as applicable.
We used multivariate logistic regression models to analyze the association between diabetic parameters (DM, FPG level, HOMA-IR, and IR) and aICAS in the total study population to obtain the adjusted ORs and 95% CIs, and considering the multicollinearity between DM and IR, we also investigated the association between diabetic parameters and aICAS in the non-diabetic participants in order to reduce the impact of the increased glucose concentration on the association between IR and aICAS. We further designed post hoc models stratified by sex. We reported the results from two models: model 1 was adjusted for age, sex, smoking habit, alcohol consumption, and low-density lipoprotein cholesterol (LDL-C); model 2 was adjusted for variables in model 1 plus additional MetS components (raised blood pressure, triglycerides, HDL-C, and waist circumference). Continuous variables that had a non-normal distribution were analyzed after logarithmic conversion. ORs were for 1-SD increase in continuous parameters. A p value <0.05 was considered to indicate statistical significance.
Results
Study participants
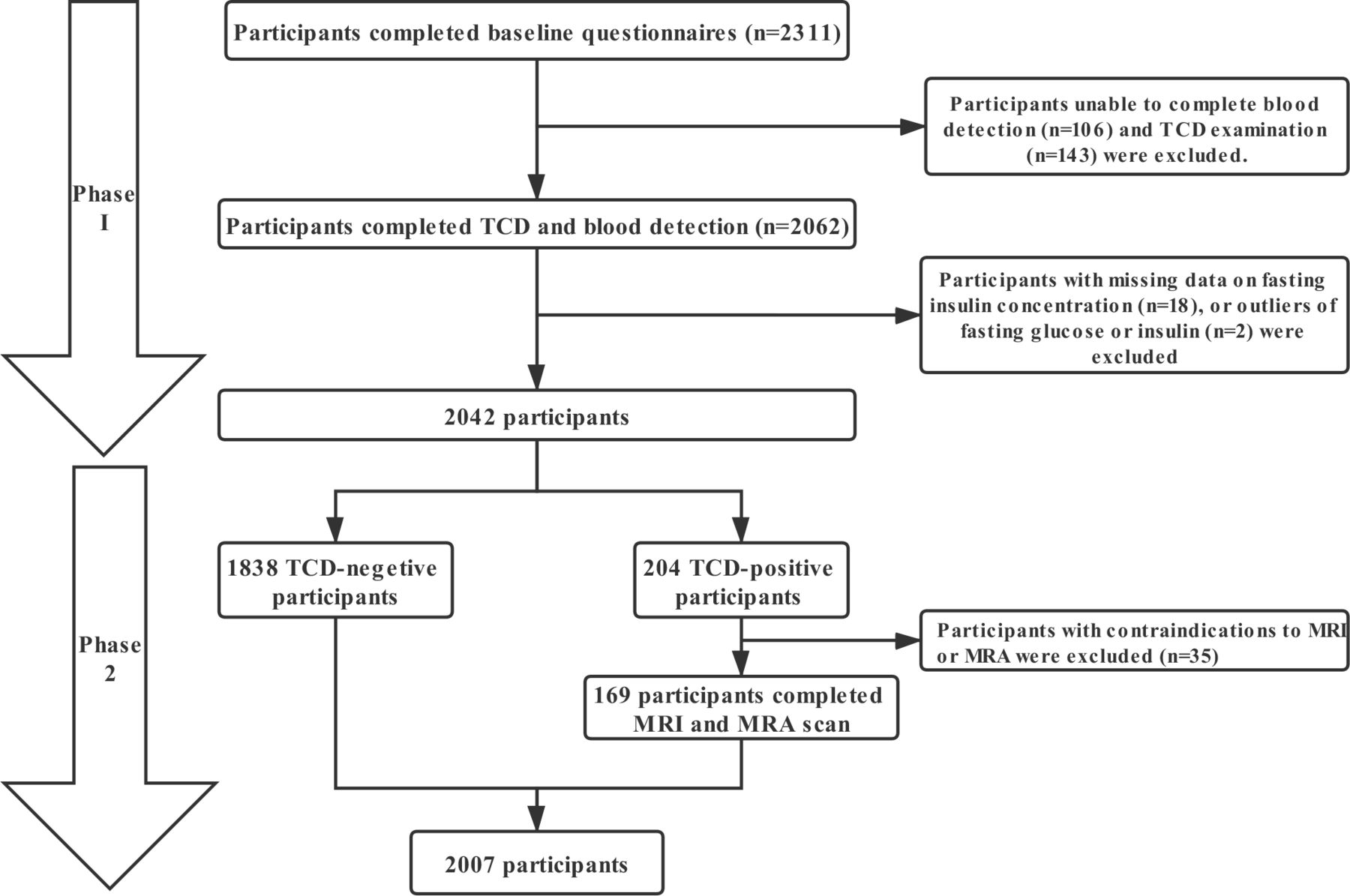
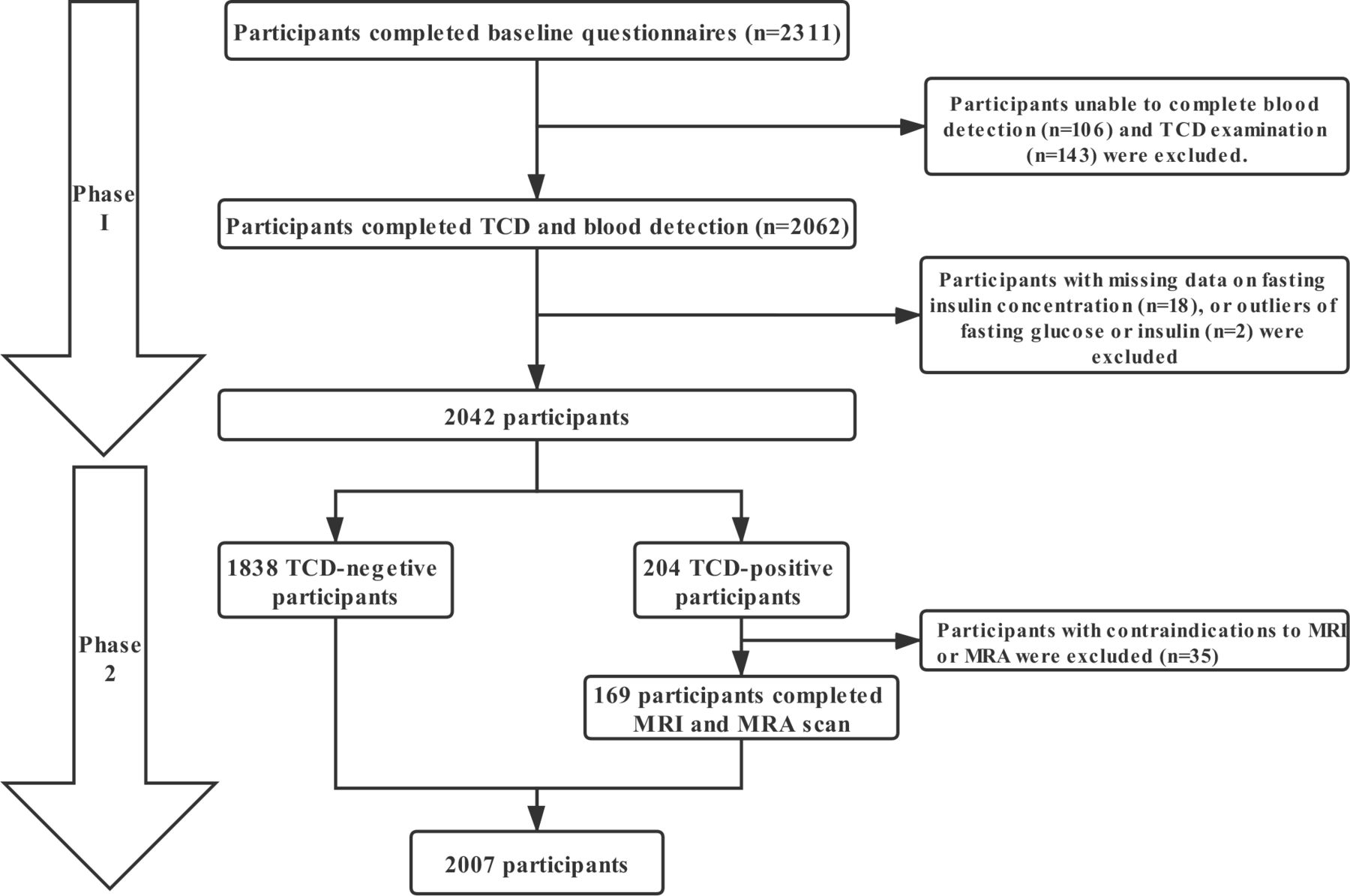
As shown in figure 1, we excluded 269 participants in phase I, who had missing information about TCD ultrasonography (n=143), fasting insulin level (n=18), and other blood test results (n=106); or with outlier of fasting insulin and glucose concentration (n=2). In phase II, we excluded 35 participants who were contraindicated for brain MRI and MRA, such as those with pacemakers or metal denture implantations. Therefore, of the total 2311 participants who were eligible for study inclusion, 2007 (86.8%) were enrolled.
{kind=link}
Flow chart of the study participants. MRA, magnetic resonance angiography; TCD, transcranial Doppler.
Participants characteristics
Table 1 presents participants characteristics, stratified as per sex. The prevalence of aICAS was 4.9% (n=99) in the total population, 4.1% (n=39) in men, and 5.7% (n=60) in women. There were sex-based differences in the HOMA-IR value and the prevalence of most CRFs and metabolic risk factors, except SBP, HDL-C level, and hypertension.
Demographic and clinical characteristics of total participants stratified by gender
Participants characteristics according to the presence of aICAS are shown in table 2. As compared with those without aICAS, participants with aICAS were older, had lower HDL-C levels, and had higher waist circumference, SBP, DBP, triglyceride level and LDL-C level. Moreover, hypertension, DM, MetS, IR, and use of medications for hypertension and DM were more commonly observed in those with aICAS. With respect to diabetic parameters, there were significant differences in the FPG level, fasting insulin level, and HOMA-IR value of participants with and without aICAS. In terms of lifestyle habits, the participants with aICAS were less likely to be current smokers or alcohol consumer than those without aICAS.
Demographic and clinical characteristics of study participants by aICAS
Association between diabetic parameters and aICAS in the total study population
After adjusting age, gender, smoking habit, drinking habit, and LDL-C (model 1), all the diabetic parameters were associated with aICAS in the total population (table 3). After further adjusting the MetS components, including raised blood pressure, triglycerides, HDL-C, waist circumference (model 2), DM (OR=2.09, 95% CI 1.31 to 3.32), FPG level (OR=1.34, 95% CI 1.14 to 1.57), and IR (OR=1.75, 95% CI 1.11 to 2.75) remained independently associated with aICAS (table 3).
Multivariate-adjusted ORs and 95% CIs between asymptomatic intracranial arterial stenosis and diabetic parameters of the total participants and as per sex
The sex-specific analyses showed that all the diabetic parameters were significantly correlated with aICAS in both male and female participants in model 1. Male participants had higher ORs than female participants. However, after further adjusting the MetS components (in model 2), DM (OR=3.40, 95% CI 1.62 to 7.13), FPG level (OR=1.64, 95% CI 1.26 to 2.13), and IR (OR=3.04, 95% CI 1.44 to 6.42) remained associated with aICAS only in the male participants (table 3).
Association between diabetic parameters and aICAS in the non-diabetic participants
The logistic regression analyses in the non-diabetic participants shows that both FPG (OR=1.91, 95% CI 1.09 to 3.35) and IR (OR=1.79, 95% CI 1.03 to 3.14) were associated with a higher risk of aICAS in model 1. After further adjusting the MetS components (in model 2), these relationships were not statistically significant (table 4).
Multivariate-adjusted ORs and 95% CIs between asymptomatic intracranial arterial stenosis and diabetic parameters of the non-diabetic participants and as per sex
In the male participants, FPG (OR=2.66, 95% CI 1.01 to 7.01) and IR (OR=4.29, 95% CI 1.1.70 to 10.84) were associated with having aICAS in model 1; however, only IR (OR=4.65, 95% CI 1.69 to 12.82) was related to a higher probability of having aICAS in model 2. No significant association was found between these diabetic parameters and aICAS in the female participants (table 4).
Discussion
In this population-based study, an independent association was found between IR or DM and aICAS after the adjustment of major CRFs and MetS components in apparently healthy Chinese men. The association between IR and aICAS remained significant in further analysis among non-diabetic male participants, suggesting that IR may have additive value for predicting aICAS prevalence via mechanisms other than glucose homeostasis.
In the present study, DM and FPG were the independent predictor of the presence of aICAS among the total participants, which is consistent with previous studies.4 5 The highlight of this study is that IR was also associated with aICAS, independently of the presence of major CRFs and MetS components in Chinese men, even in non-diabetic male participants. To our knowledge, the Barcelona-Asymptomatic Intracranial Atherosclerosis (AsIA) study among Caucasians (≥50 years of age) is the only study that has assessed the relationship between IR and aICAS.9 Consistent with our findings, the AsIA study concluded that IR is a risk factor for moderate to severe aICAS, independent of the presence of MetS components, including waist circumference, blood pressure, triglyceride, and low HDL level.9 These data indicate that IR may have additional predictive value in detecting aICAS that was not mediated by glucose homeostasis and lipid metabolism.
Insulin is a key hormone in the maintenance of metabolic homeostasis of cells in many tissues in the human body. Hyperglycemia and hypertriglyceridemia are the main metabolic alterations induced by IR. Under IR, the target cells fail to respond to normal levels of circulating insulin, leading to increased gluconeogenesis in the liver and impaired glucose uptake in the skeletal muscles.21 The long-term hyperglycemia induced by IR can cause cell damage by triggering oxidative stress and inflammatory response. Moreover, impaired hormone function results in limited degradation of apolipoprotein B induced by impaired PI3K activation and increased synthesis of very low-density lipoprotein,22 leading to the formation of atherosclerotic plaque.
The independent association between IR and aICAS may be partially explained by its vascular effect.21 Increasing evidence has shown that in addition to causing metabolic changes, insulin signaling defects under IR also play an important role in the development of atherosclerotic lesions.23 Under physiological conditions, insulin exerts a protective effect by activating endothelial nitric oxide synthase via the PI3K/Akt pathway. Furthermore, it exerts a detrimental effect because it induces vascular smooth muscle cell proliferation and vasoconstriction via the mitogen-activated protein kinase (MAPK) pathway. Under IR, the PI3K pathway is impaired, while the MAPK pathway remains intact. Thus, the detrimental effects of insulin are more than its protective effects on the vascular beds, leading to the formation of atherosclerosis. Based on the above data, we speculated that physicians may underestimate the possibility of having aICAS when the HOMA-IR value or insulin sensitivity of patients is not available. For the primary prevention of stroke, we need to grade the effects of IR and its related metabolic changes on aICAS in the future.
As we all know, significant differences exist between men and women in sex hormones. A previous have reported the sexual difference on the conventional risk factor profiles of intracranial atherosclerotic disease.10 However, few studies have focused on the sex-based differences in the new risk factors. In this study, IR was independently associated with aICAS only in male participants. Similarly, sex-based differences were found in some studies on other vessel territories, such as carotid12 and coronary arteries.24 The mechanism underlying this difference remains unknown. Some studies have indicated that women have higher endogenous antioxidant capacity than men, which may partially explain the female advantage in eliminating increased IR-related risks.25 26 Moreover, in this study, the higher prevalence of unhealthy lifestyle habits and poor management of CRFs in men may partly contribute to this sex-based difference.
In this study, we found only 1.2% of women with smoking habits in rural China, which was not exactly similar to that of two other Chinese studies (2.0% and 2.6%),27 28 and 4% of women drink alcohol, which was slightly higher than that in another Chinese study (2%).29 The reasons for the different prevalence rates across studies are not entirely clear, but differences in demographic features of the study populations (eg, region and age) and methodological issues (eg, definition of smoking habits) may partly contribute to the difference.
To our knowledge, this is the first study to investigate the association between IR and aICAS in rural Chinese population. However, this study has certain limitations that should be considered. First, the cause and effect cannot be explained in this cross-sectional study. The participants with IR in this study should be assessed in longitudinal studies in the future. Second, insulin sensitivity was measured using HOMA-IR rather than the gold standard euglycemic hyperinsulinemic clamp technique. Third, TCD as a tool for screening aICAS might have missed some cases and underestimated the prevalence of aICAS, which may have an impact on the association between IR and aICAS. Fourth, the cut-off value of HOMA-IR (75th percentile) for IR diagnosis in this study cannot be used in other studies because the 75th percentile of HOMA-IR may vary with different populations or different insulin assays. Finally, this study is a single-center study, and generation to the other population should be done with caution, and further large-scale multi-center studies are needed to verify this association and sex-based difference.
Conclusions
In this study, IR (HOMA-IR ≥3.0) or DM might be associated with the aICAS prevalence, independently of major CRFs and MetS components in Chinese men living in rural communities. Moreover, the association between IR and aICAS remained significant after excluding the diabetic participants, suggesting that IR may be associated with aICAS via mechanisms other than glucose homeostasis. This sex-based difference may facilitate improvement in risk stratification and primary prevention of ischemic stroke.
Acknowledgments
We would like to thank the study participants for their contribution to the project.
References
Footnotes
Contributors QS, YD, and FX conceived the study, participated in its design and coordination, and helped in the drafting of the manuscript. QW, XW, XJ, and FX performed the statistical analyses. QW, XW, ShS, ML, YZ, SS, GW, and QS enrolled the patients and performed the ultrasonography and MRI scan. QW, XW, XM, and QS contributed to the discussion and were involved in drafting and revising the manuscript. All authors read and approved the final manuscript.
Funding This study was supported by the Jinan Science and Technology Bureau (201704101), Key Technology Research and Development Program of Shandong (2014GSF118106, 2016GSF201062), Natural Science Foundation of Shandong Province (ZR2017MH114), the National Natural Science Foundation of China (8171101298, 81971128), and the Ministry of Sciences and Technology of the People's Republic of China (2017YFC1310100 and 2017YFC0907003), the International Science and Technology Cooperation Programme (2014DFA32830).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This study was approved by the ethical standards committee on human experimentation of Shandong Provincial Hospital, Cheeloo College of Medicine, Shandong University and conducted in accordance with the principles for medical research involving human participants expressed in the Helsinki Declaration. All the participants provided written informed consent for study participation.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request. The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.