Article Text

Abstract
Introduction Various studies have shown a number of glycemic parameters to improve over several weeks in people with type 1 diabetes during the first surge of the COVID-19 pandemic. Whether and to what extent such improvement is sustained during following COVID-19 surges remains unknown. Therefore, the aim of this study was to investigate glycemic parameters during the first year of the COVID-19 pandemic in people with type 1 diabetes and to determine factors associated with glycemic improvement.
Research design and methods This was an observational cohort study in people with type 1 diabetes, aged ≥16 years. We compared glycated hemoglobin (HbA1c) and flash glucose monitoring (FGM) downloads between the prelockdown period and approximately 1 year thereafter. Using logistic regression analysis, we assessed associations between an HbA1c reduction of at least 0.5% (~5.5 mmol/mol) with baseline clinical characteristics and self-reported changes in psychological well-being and lifestyle behavior related to COVID-19.
Results A total of 437 participants were included. As compared with prepandemic data, 1 year after the start of the COVID-19 pandemic and associated lockdowns, HbA1c had decreased from 7.9%±1.1% (63±12 mmol/mol) to 7.5%±1.0% (59±11 mmol/mol) (p<0.001), whereas time in range increased from 55.8%±16.7% to 58.6%±16.7% (p=0.004) and time below (<3.9 mmol/L) and above (>13.9 mmol/L) range and glucose variability all decreased (all p<0.05). FGM use, higher HbA1c at baseline and current smoking were independently associated with an HbA1c decrease of at least 0.5%, whereas self-reported changes in psychological well-being and lifestyle behavior related to the first surge of the COVID-19 pandemic and associated lockdowns were not.
Conclusions The COVID-19 pandemic and related lockdown measures were associated with improvement in glucometrics, including HbA1c and FGM data, in individuals with type 1 diabetes, particularly in FGM users, those with higher HbA1c at baseline or current smokers.
- COVID-19
- HbA1c
- diabetes mellitus, type 1
- blood glucose self-monitoring
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Short-term improvement in several glycemic parameters has been shown in people with type 1 diabetes during the first surge of the COVID-19 pandemic.
WHAT THIS STUDY ADDS
Glycated hemoglobin (HbA1c) and flash glucose monitoring (FGM) data improve, over 1 year of follow-up after the start of the COVID-19 pandemic and implementation of various lockdown measures.
The improvement in glycemic parameters is largely consistent across subgroups.
Use of FGM, higher HbA1c at baseline and current smoking are independently associated with an HbA1c decrease of at least 0.5% (~5.5 mmol/mol).
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
Pandemics and the associated lockdown measures are associated with improvement rather than with worsening of glycemic control in individuals with type 1 diabetes.
Introduction
As of January 1, 2022, worldwide >312 million people have been diagnosed with infection caused by SARS-CoV-2 and >5.5 million have died.1 People with both type 1 and type 2 diabetes mellitus have a twofold increased risk for severe COVID-19 infection and mortality compared with people without diabetes.2–4 Both hyperglycemia at presentation and elevated glycated hemoglobin (HbA1c) are independently associated with severity of COVID-19 infections and increased mortality.5–7
To control the COVID-19 outbreak, many countries implemented several (lockdown) measures over the past 1.5 years. In the Netherlands, such lockdown measures, first implemented in March 2020 and changed throughout the year based on rates of infection, included stay-at-home orders for people working in non-vital areas of society, social distancing, a curfew and closures of schools, restaurants, theatres and other public spaces. There were also changes in the healthcare system with downscaling of outpatient clinic visits, partly replaced by virtual meetings and postponement of certain (surgical) procedures.8 9 Unique and widespread impact of these lockdown measures have been described on (societal) behavior, including those related to lifestyle and self-care, which may have directly or indirectly affected glucose (self) management and glycemic parameters.10
Several studies have reported various glycemic parameters to improve over several weeks in people with type 1 diabetes during the first surge of the COVID-19 pandemic.11–16 Whether and to what extent such improvement is sustained during following COVID-19 surges remains unknown, as studies with longer follow-up are lacking. Furthermore, few studies have investigated factors that contribute to this glycemic improvement. Therefore, the aim of the present study was to investigate, in a contemporary cohort of people with type 1 diabetes, glycemic parameters prestart and 1 year after the start of the COVID-19 pandemic and associated lockdown measures and factors associated with HbA1c improvement.
Research design and methods
Study design and population
This study was an observational cohort study. People with type 1 diabetes who attend the diabetes outpatient clinic of the Radboud University Medical Center were invited to participate in the study. Inclusion criteria for the study were type 1 diabetes, age ≥16 years, sufficient comprehension of the Dutch language and ability to provide informed consent. Type 1 diabetes diagnosis was based on clinical criteria. Participants were excluded when the medical history mentioned severe psychiatric comorbidity or other comorbidity interfering with completing the questionnaires. After providing consent, participants were either invited to the outpatient clinic of our hospital or a virtual appointment was made for data collection.
We assessed 702 people with type 1 diabetes for eligibility in the study, 184 of whom did not want to participate and 81 persons were excluded for various reasons. As such, a total of 437 people with type 1 diabetes agreed to participate in the study (online supplemental figure 1). Individuals who declined to participate or were excluded did not differ from those who were included with respect to age and sex. For 427 participants (97.7%), HbA1c data were available for both time periods (ie, period before and 1 year after the start of the COVID-19 pandemic and associated lockdown measures), whereas 200 participants (45.8%) gave consent to access their flash glucose monitoring (FGM) data. A total of 190 (43.5%) participants had both HbA1c and FGM data for these periods.
Supplemental material
Demographics and clinical characteristics
Data collection took place from February 2020 to April 2021. Demographics and clinical characteristics, including age, sex, presence of microvascular and macrovascular diabetes complications, smoking, alcohol use, data on insulin treatment (mode and dose), mode of glucose monitoring, diabetes duration, number of (severe17) hypoglycemic events, hypoglycemia awareness status assessed with the Clarke questionnaire18 and frequency of hospitalizations in the past year, were obtained by questionnaires and verified from clinical records, wherever possible. Body mass index was measured at the outpatient clinic or retrieved from the clinical record if the appointment for data collection was virtual.
At the end of the first COVID-19 surge, we administered the Problem Areas in Diabetes (PAID-5) questionnaire, where a score ≥8 indicates possible diabetes-related emotional distress,19 and a questionnaire, containing questions about whether there was any emotional distress, worries and changes in diabetes self-management or behavior due to the COVID-19 pandemic and the associated lockdown during the first COVID-19 surge (online supplemental table 1). Emotional distress due to the COVID-19 pandemic could include any of the following: having little interest or pleasure in activities, feeling nervous, anxious or tense, unable to stop worrying, feeling lonely or isolated, feeling little control over life or feeling insecure about the future.
Glycemic parameters
HbA1c levels were derived from the electronic medical record, whereas online data sharing platforms were used to gain access to FGM data. Both HbA1c and FGM data before the onset of the COVID-19 pandemic and associated lockdown measures (ie, prelockdown data) were collected between September 2019 and March 2020, whereas 1-year follow-up data were collected between January and March 2021. The primary outcome in this study was the change in HbA1c between these defined periods. Data from FGM were collected for the participants who were using FGM and had data for both defined periods. FGM data (representation of 28 days) used for the analysis were: time sensor is active (% of time), average number of scans per day (n), average glucose (mmol/L), glucose variability (%), time below target range (% of time glucose ≤3.9 mmol/L), time in target range (% of time glucose 3.9–10.0 mmol/L), time above target range (% of time glucose >10.0 mmol/L), number of low glucose events (glucose ≤3.9 mmol/L) and duration of low glucose events.
Statistical analyses
Continuous data are expressed as mean (±SD) if normally distributed or median (IQR) if not normally distributed. Categorical data are presented as number (percentage, %). Demographics and clinical characteristics were compared using one-way analysis of variance followed by post hoc analysis with least significant difference or Kruskal-Wallis followed by post hoc analysis Mann-Whitney U test for continuous variables, depending on their distribution, and χ2 test was used for categorical data. Glycemic data from the prelockdown and the 1-year follow-up period were compared using the paired samples t-test or the Wilcoxon signed rank test or McNemar test, as appropriate. We performed subgroup analysis for the primary outcome (ie, change in HbA1c) for subgroups defined by sex, age, baseline HbA1c, diabetes duration, insulin administration strategy, hypoglycemia awareness status, mode of glucose monitoring, FGM start year, PAID-5 score ≥8 and any change in psychological well-being and lifestyle behavior due to the first surge of COVID-19 pandemic and associated lockdown. Mixed models were used to investigate differences between these subgroups.
We investigated demographics, clinical characteristics and COVID-19-related changes associated with an HbA1c reduction of ≥0.5% (~5.5 mmol/mol), using univariable and multivariable logistic regression analysis. For the multivariable regression analysis, we used different models to adjust for potential confounders. In model 1 of the analysis, we adjusted for age and sex; model 2 was additionally adjusted for impaired awareness of hypoglycemia (IAH) and hospitalization in the past year and model 3 was additionally adjusted for continuous subcutaneous insulin infusion (CSII) use and insulin dose. Self-monitoring of blood glucose (SMBG) was used as reference category for mode of glucose monitoring.
All statistical analyses were performed with IBM SPSS V.25 software (Armonk, New York, USA). Graphs were made with GraphPad Prism V.8.0 (La Jolla, California, USA). Data are shown as mean±SD, median (IQR) or number (%), as appropriate. ORs with 95% CIs are reported for the logistic regression analysis and for mixed models. P values <0.05 were considered statistically significant.
Results
Characteristics of the study sample
Demographic, clinical and behavioral characteristics stratified according to mode of glucose monitoring are shown in table 1. In the total study population there was an equal sex balance (50.3% male) and HbA1c on average was 7.9%±1.1% (63±12 mmol/mol). At the time of inclusion, 330 (75.5%) participants used the FGM sensor for a median duration of 1.0 year (IQR 0.0–2.0), 35 (8.0%) used real-time continuous glucose monitoring (rt-CGM) and 72 (16.5%) used SMBG. Eight individuals used a hybrid closed-loop system and one individual used a do-it-yourself closed-loop system. There were no differences between FGM, rt-CGM and SMBG users with respect to age, sex, diabetes duration, HbA1c and most other clinical parameters (table 1). The prevalence of IAH, the rate of hypoglycemia and the rate of CSII use was higher in the rt-CGM users as compared with FGM users. The rate of CSII use and the number of hypoglycemic events was lower in people using SMBG as compared with those on FGM.
Characteristics of the study populations (n=437) stratified according to mode of glucose monitoring
A PAID-5 score of at least 8 was present in 22.3% (n=86) of the individuals. Any emotional distress due to the COVID-19 pandemic was reported by 45.3% (n=177) of the participants and 8.9% (n=39) had worries about their diabetes and/or COVID-19 in this period. About 17% (n=63) of the individuals reported to aim for another (ie, higher or lower) blood glucose level and 22.7% (n=86) of participants expressed to be more involved in their diabetes care during the COVID-19 pandemic period compared with the period before. Changes in physical activity, diet and sleep duration after the first surge of the COVID-19 pandemic and associated lockdown measures were reported by 58.2% (n=221), 28.7% (n=109) and 23.2% (n=88) of the individuals, respectively. Any self-reported change in psychological well-being and lifestyle behavior due to the first surge of COVID-19 pandemic and associated lockdown was present in 75.3% (n=329) of the individuals.
Glycemic parameters
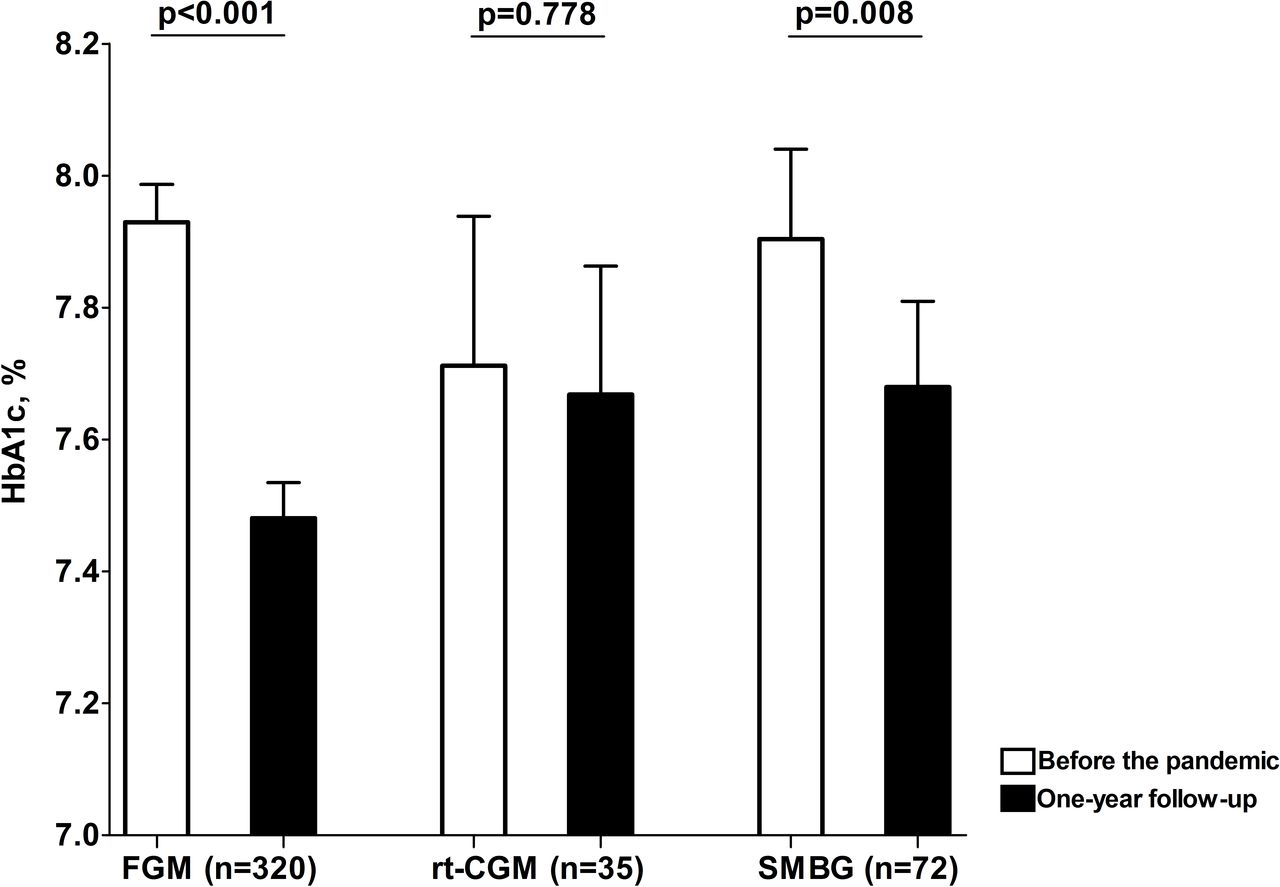
The average follow-up between the two periods of data collection was 376±94 days. HbA1c decreased from 7.9%±1.1% (63±12 mmol/mol) before the lockdown to 7.5%±1.0% (59±11 mmol/mol) 1 year later (mean difference (95% CI): 0.4% (0.3 to 0.4) (4 mmol/mol (3 to 5)); p<0.001)). The fall in HbA1c between the defined time periods occurred in all participants independent of the mode of glucose monitoring, but was slightly greater for participants using FGM compared with participants not using FGM, that is, rt-CGM users and SMBG (0.2% (0.1 to 0.4) vs 0.4% (0.3 to 0.5); p=0.044). There was no significant difference in HbA1c change between participants using rt-CGM or SMBG (figure 1 and online supplemental figure 2). There was also no difference in HbA1c decrease between participants using FGM with or without available FGM data (0.5% (0.3 to 0.6) vs 0.4% (0.3 to 0.6); p=0.923). The number of participants with HbA1c <7% (53 mmol/mol) increased from 80 (18.4%) before the lockdown to 126 (29.5%) 1 year later (p<0.001).

HbA1c change in participants with available HbA1c for both time periods (n=427), stratified according to mode of glucose monitoring. FGM, flash glucose monitoring; HbA1c, glycated hemoglobin; rt-CGM, real-time continuous glucose monitoring; SMBG, self-monitoring of blood glucose.
With respect to FGM parameters, time in range increased over the 1 year of follow-up, whereas times below 3.9 and above 13.9 mmol/L and glucose variability all decreased (table 2). The number of low glucose events and the duration of these events did not change. Mean percentage of time during the day that FGM was active increased from 70%±31% in the prelockdown period to 87%±22% after 1-year follow-up (18% (95% CI 12.8 to 22.5); p<0.001)) and the median scan frequency per day (IQR) increased from 6 (4–10) to 10 (6–14)6–14 (median difference (IQR): 4 (2–4); p<0.001).
Flash glucose monitoring data before and 1 year after start of the pandemic (n=200)
HbA1c change in subgroups
Figure 2 shows the subgroup analysis for the primary outcome. The decrease in HbA1c that we observed over the 1-year follow-up period was consistent in subgroups defined by sex, age, baseline HbA1c, diabetes duration, insulin administration strategy, hypoglycemia awareness status, mode of glucose monitoring, FGM start year, PAID-5 score and any self-reported change in psychological well-being and lifestyle behavior due to the first surge of COVID-19 pandemic and associated lockdown. Although HbA1c improved in both males and females, the fall in HbA1c was greater in men compared with women (p=0.049). Furthermore, HbA1c decrease was greater in the participants with baseline HbA1c ≥7.5% compared with those with lower HbA1c (p<0.001), in the participants using FGM compared with those using SMBG or rt-CGM (p=0.001) and in the individuals who started using FGM after January 1, 2020 compared with individuals who already used FGM before that date (p=0.001). A PAID-5 score ≥8 or self-reported change in psychological well-being or lifestyle behavior during the first surge of the pandemic were not associated with a greater improvement in HbA1c.

{kind=link}
{kind=link}
Subgroup analysis for change in HbA1c. CSII, continuous subcutaneous insulin infusion; FGM, flash glucose monitoring; HbA1c, glycated hemoglobin; IAH, impaired awareness of hypoglycemia; MDI, multiple daily injection; NAH, normal awareness of hypoglycemia; PAID-5, Problem Areas in Diabetes-5 questionnaire; rt-CGM, real-time continuous glucose monitoring; SMBG, self-monitoring of blood glucose.
Factors associated with improved HbA1c
Univariable logistic regression analysis showed that use of FGM (OR (95% CI): 2.1 (1.2 to 3.6), higher HbA1c level at baseline (2.4 (1.9 to 3.0) and current smoking (2.4 (1.3 to 4.3) were significantly associated with an HbA1c decrease of at least 0.5% (online supplemental table 2). After correction for potential confounders, all these associations remained significant in all three models in the multivariable logistic regression analysis (table 3). No COVID-19-related change in psychological well-being or behavior were found to be related to an HbA1c reduction of at least 0.5%.
Multivariable logistic regression analysis relating demographic and clinical factors to HbA1c decrease of ≥0.5% (~5.5 mmol/mol) (n=427) in different models
Discussion
This study shows a clinically significant improvement in a number of glycemic parameters in individuals with type 1 diabetes over 1 year follow-up after the start of the COVID-19 pandemic and implementation (and temporary lifting) of various lockdown measures. HbA1c fell by 0.4%, which was mirrored by increases in time in range and decreases in times below and substantially above target range and in glucose variability. Although we found no relation between changes in psychological well-being or behavior and the change in HbA1c, it is likely that the COVID-19 pandemic has played an important role in the improvement in glucometrics in people with type 1 diabetes 1 year after the onset of the pandemic.
Our data are in line with previous studies that examined the effect of the first COVID-19 wave on glucose outcomes11–16 and extend these to a longer period. Previous studies that examined FGM parameters over several weeks of the first COVID-19 wave reported improvements in time in range11–16 and time above range11–15 that were of about similar magnitude as what we observed. Only one study reported a decrease in time below range16 similar to our results, while other studies found no difference12–14 or even an increase in this outcome.15 An increase in the time that the sensor was active and number of daily scans was also reported by one study,11 but not by other studies,12 14–16 whereas some,13 16 but not all studies11 12 14 15 reported a decrease in glucose variability. However, due to the much shorter follow-up periods, most of these studies were unable to observe an improvement in HbA1c, at least not to the extent observed here.11–16
Our data contrast with a study from India showing deterioration of glycemic parameters, including an increase in HbA1c, in people with type 1 diabetes during a lockdown period in the first COVID-19 wave.20 However, since this change was mainly due to non-availability of insulin or glucose strips during this period, the disparity between this study and our study are probably explained by the major differences between the Netherlands and India in healthcare system and resources. A study conducted in the UK described an ~80% fall in HbA1c tests for diabetes diagnosis and management during the COVID-19 pandemic, which was associated with a rise in HbA1c among individuals with diabetes with pre-existing suboptimal glycemic outcomes.21 Also, the few studies that investigated glucose parameters during the lockdown period in people with type 2 diabetes have reported no improvement in HbA1c or even an increase of HbA1c in older people.11 22 Explanations for the discrepancy with people with type 1 diabetes include the usually much less frequent use of continuous or flash glucose monitoring and the potential educational gap with respect to handling of insulin therapy in the small proportion of people with type 2 diabetes using insulin.
In our study, we found that the use of FGM and higher HbA1c at baseline were independent predictors of a larger HbA1c decrease. This is in line with a meta-analysis supporting greater fall in HbA1c in people using FGM and with higher initial HbA1c values.23 FGM enables people with diabetes to monitor glucose levels more closely, when compared with SMBG, and it has been shown that more daily scans are associated with a lower HbA1c.24 Our finding that scan frequency under FGM users increased during follow-up may support this notion. People using rt-CGM did not show a large increase, however, this was a relatively small group with a lower start HbA1c, as well as avoiding (severe) hypoglycemia rather than lowering HbA1c being the main indication for its use.
Surprisingly, our analysis also showed that current smoking was independently associated with greater HbA1c improvement. This association remained significant after correction for multiple confounders. It could be argued that people who smoke are more inclined to improve glucose management since smoking is a risk factor for more severe COVID-19 infections. Whether there are other, (patho-) physiological, mechanisms underlying this association would require further study, yet this finding should not be regarded as a beneficial effect of smoking.
There could be several reasons for the improvement of glycemic parameters that we observed. First, fear of contracting the virus and the potential role of suboptimal glycemic control in becoming ill may have been incentives for people to increase efforts to improve glucose levels to lower the risk of COVID-19 infection.25 26 However, diabetes-related distress, emotional distress due to the first surge of the COVID-19 pandemic, worries about diabetes or COVID-19, more involvement in diabetes care and aiming for other blood glucose levels in the COVID-19 pandemic period, were not associated with improvement in glucose control. It should we acknowledged, however that the COVID-19 questionnaires were completed within the first months after the start of the pandemic and associated lockdown, of which most of the participants reported no detrimental effects. We cannot exclude an effect of changes in psychological well-being later during the pandemic on the change in HbA1c.
The improvement in glycemic parameters could also have been due to changes in lifestyle or daily activities in the lockdown period with less fluctuation in glucose profiles and insulin needs. Indeed, a recent study showed that time in range increased from 54.4% to 65.2% (p=0.010) in people with type 1 diabetes who stopped working and stayed at home during the pandemic compared with those who continued working.12 It could also be speculated that these conditions made it easier for people with diabetes to count carbohydrates, administer insulin in time, have more time to monitor their glucose profiles (eg, from sensors) and pay more attention to diet and exercise.
The improvement in glucometrics could also be independent of the pandemic, for example, with more people becoming increasingly familiar with FGM. HbA1c decreased to a greater extent in people using FGM as compared with people not (yet) using FGM and the decrease was more pronounced in participants who recently started FGM. However, glycemic parameters also improved in people who used FGM longer, which argues against this option being the only explanation. In the Netherlands, the introduction of FGM had largely taken place before the COVID-19 pandemic, and this study shows paired data of those already on FGM. The magnitude of the improvement that we show is larger than the HbA1c drop of 0.2% associated with flash monitor initiation, reported by a nationwide Scottish observational study.27
A key strength of our study is the 1-year follow-up, with data on HbA1c and FGM parameters enabling us to study the long-term impact of the COVID-19 pandemic on glucose management in people with type 1 diabetes. Our study also has limitations. First, we only included people with type 1 diabetes with HbA1c and/or FGM data that could be evaluated after 1 year, which may introduce selection bias. Not everyone consented in providing us access to their FGM data, which resulted in missing FGM data. However, the fall in HbA1c for participants with FGM data was comparable to that among participants without FGM data. Another limitation is that we did not investigate glycemic parameters from rt-CGM in the participants using rt-CGM. However, although such data would have helped to explain the apparent smaller change in HbA1c in participants using rt-CGM, the number of people using rt-CGM was small. Due to data protection regulation, we could only make a group comparison between the participants and those who declined to participate or were excluded, with respect to age and sex. We can therefore not fully rule out selection bias. Furthermore, several aspects around changes in behavior because of the COVID-19 pandemic and associated lockdown measures (eg, change in work habit, change in insulin dose, etc) were not addressed in our questionnaire and the questionnaire was administered only once. Finally, this was a monocentre study, potentially limiting extrapolation to the wider diabetes population, and since the study was observational, we were unable to attribute causation to the results.
In conclusion, our study shows an association between COVID-19 pandemic and related lockdown measures with a clinically relevant improvement of various glycemic parameters in individuals with type 1 diabetes during 1-year follow-up. We found a greater fall in HbA1c in participants who used FGM, had higher HbA1c at baseline or were current smokers. The glycemic improvements were substantial and seemingly sustainable, but further studies are needed to see whether and to what extent these improvements can be sustained after the COVID-19 pandemic-associated lockdown measures are lifted.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
Ethical approval for the study was obtained from the Institutional Review Board of the Radboud University Medical Center (NL-71207.091.19) and the study was conducted in accordance with the Declaration of Helsinki. All participants gave written informed consent before participation.
Acknowledgments
The authors thank the participants of the study and the contributing physicians.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors NA and BEDG designed the study. NA and SEH recruited the participants and collected the clinical data. NA analyzed the data and wrote the first draft of the manuscript. NA, BEDG, GN, CJT discussed the results and provided input for and commented on the manuscript at all stages. NA, BEDG and SEH had full access to the data and all authors approved the final version, and accept the responsibility to submit the study for publication. The guarantors of the study are NA and BEDG.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.