Article Text

Abstract
Introduction Antares is a pulse wave analysis (PWA) algorithm designed to allow a non-invasive estimation of central (aortic) blood pressure (cBP) using automated oscillometric blood pressure (BP) devices. Diabetes may affect elastic and muscular arteries differently, resulting in disparate pulse wave characteristics in central and peripheral arteries, which may limit the accuracy of PWA devices. The aim of our study was to evaluate the accuracy of Antares for estimating cBP as compared with invasively measured cBP in patients with type 2 diabetes.
Research design and methods In this study, consecutive patients undergoing elective coronary angiography were recruited between November 2017 and September 2020. In 119 patients with type 2 diabetes, cBP was measured invasively and simultaneously determined non-invasively using the custo screen 400 device with the integrated Antares algorithm.
Results The mean difference between the estimated and invasively measured cBP was 1.2±6.3 mmHg for central systolic BP (cSBP), 1.0±4.3 mmHg for central mean arterial pressure (cMAP) and 3.6±5.7 mmHg for central diastolic BP (cDBP). High correlations were found between estimated cBP and invasively measured cBP (cSBP: r=0.916; cMAP: r=0.882; cDBP: r=0.791; all p<0.001).
Conclusions The present study suggests that the Antares algorithm incorporated into the custo screen 400 device can estimate cBP with high accuracy turning a conventional oscillometric BP device into a type II device for the non-invasive estimation of cBP, which is applicable in patients with type 2 diabetes. Integration of Antares into commercially available BP devices could facilitate the introduction of cBP into routine clinical practice as a part of disease and risk management.
- blood pressure
- diabetes mellitus, type 2
- hypertension
- algorithms
Data availability statement
Data are available on reasonable request. The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Hypertension and type 2 diabetes are known to be common comorbidities, and hypertension is an important risk factor for atherosclerotic cardiovascular disease, heart failure and microvascular complications.
Brachial blood pressure, as a standard parameter for risk stratification, does not fully reflect the central (aortic) blood pressure to which the heart, brain and kidneys are exposed due to the phenomenon of pulse pressure amplification, and several studies have shown that central blood pressure has a stronger association with target organ damage and increased risk of cardiovascular disease compared with brachial blood pressure.
WHAT THIS STUDY ADDS
Our data show the accuracy of the Antares algorithm for the non-invasive estimation of central blood pressure based on a standard oscillometric brachial blood pressure measurement in patients with type 2 diabetes.
The Antares algorithm can transform a conventional automated oscillometric blood pressure device into a type II medical device for an easy-to-use non-invasive assessment of central blood pressure in patients with type 2 diabetes.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The results presented could help stimulate innovative scientific research in the context of central blood pressure in patients with type 2 diabetes (eg, association of central blood pressure compared with peripheral (brachial) blood pressure with prognosis of cardiovascular events; effects of therapeutic strategies on central blood pressure).
Introduction
Patients with type 2 diabetes have significantly higher cardiovascular morbidity and mortality than non-diabetics.1 2 Hypertension is common in patients with type 1 and type 2 diabetes and is an important risk factor for both atherosclerotic cardiovascular disease, heart failure and microvascular complications.3 4 Antihypertensive treatment significantly reduces cardiovascular morbidity and mortality in patients with diabetes.3 For these reasons, regular blood pressure (BP) determination is recommended as important part of disease and risk management.4 However, brachial BP, as a standard parameter for risk stratification, does not fully reflect the central (aortic) BP to which the heart, brain and kidneys are exposed due to the phenomenon of pulse pressure (PP) amplification.5 As pulse waves propagate from the conducting arteries to the brachial artery, physiologically, changes in arterial properties (eg, elasticity/stiffness gradient, vasomotor tone), architecture of the arterial tree (eg, branching points), decreasing vessel radius and overlap with pulse wave reflections peripherally result in a steeper systolic upstroke and peak pressure waves, increasing peripheral systolic blood pressure (SBP) and PP, while diastolic blood pressure (DBP) and mean arterial pressure (MAP) remain relatively constant.6 However, the degree of PP amplification between the aorta and brachial artery depends on several factors including age, gender, height and heart rate as well as traditional cardiovascular (CV) risk factors such as hypertension, diabetes, hypercholesterolaemia, smoking or established CV disease.6 7
From a physiological perspective, it is reasonable to hypothesize that central BP (cBP) may provide prognostic information for clinicians beyond brachial BP. In this context, several studies have shown that cBP has a stronger association with target organ damage and increased risk of cardiovascular disease compared with brachial BP.8–13 Another interesting aspect of central hemodynamics is the differential effect of antihypertensive drugs on central and brachial BP.14–17
There are several methods for determining cBP using non-invasive techniques.18 With Antares, an algorithm exists for calculating cBP based on pulse waveform characteristics that can be integrated into a conventional oscillometric BP device to function as a type II pulse wave analysis (PWA) device. Antares has already been invasively validated in a patient population with various conditions, including 43 patients with type 2 diabetes.19 In patients suffering from both diabetes and hypertension, aortic stiffness is higher than in patients suffering from only one of the two diseases.20 21 The process of arterial stiffening is influenced by hemodynamic and mechanical factors, where the latter are caused by the remodeling of matrix proteins in the arterial wall, in which advanced glycation end products are formed by non-enzymatic cross-linking between glucose and amino groups.20 Diabetes may affect elastic (eg, aorta, carotid) and muscular (eg, radial, brachial) arteries differently,22 23 resulting in different pulse wave characteristics in central and peripheral arteries. Therefore, it is still unclear whether these potential differences affect the accuracy of Antares in patients with diabetes. The availability of additional invasive BP data collected as part of the ongoing invasive validation study allows for a more sophisticated validation of the Antares algorithm in this specific population.
Hence, the aim of our study was to evaluate the accuracy of Antares for calculating cBP as compared with invasively measured aortic BP in patients with type 2 diabetes.
Research design and methods
Following the 2017 ARTERY Society Task Force consensus statement on protocol standardization for validation of non-invasive central blood pressure devices,24 the ANSI/AAMI/ISO 81060-2:201925 and the 2018 AAMI/ESH/ISO validation standard protocols26 between November 2017 and September 2020, a total of 389 patients were enrolled in a multicenter invasive validation study undergoing cardiac catheterization for clinical reasons. An overview of ARTERY and ANSI/AAMI/ISO protocol components and requirements are presented in the online supplemental table S1.
Supplemental material
For acquisition of central systolic BP, central diastolic BP and central mean arterial pressure (cMAP) simultaneous invasive (ascending aorta) and non-invasive measurements were performed in cardiac catheterization laboratories of three German study centers: Greifswald, Bad Oeynhausen and Bad Berka. The invasive reference BP monitoring device used complies with the requirements of ISO 81060-2:2019.25 Data collection was performed in an undisturbed resting phase, free from acute hemodynamic interventions, free from acute medication changes and without conversation. All invasive measurements were performed with fluid-filled catheters with radial or femoral catheter access. For the determination of the invasive systolic BP, the peak of every recorded valid pulse wave; for invasive diastolic, the lowest signal point; and for invasive MAP, the area under the curve was taken for the calculation.
The simultaneous cuff-based non-invasive measurements were performed at the left upper arm with the oscillometric custo screen 400 device (custo med GmbH, Ottobrunn, Germany), which has integrated the Antares algorithm (Redwave Medical GmbH, Jena, Germany) for calculating cBP. Redwave Medical is patent holder for PWA) in oscillometric pulse waves that are recorded during inflation and deflation of a cuff (patent no DE 10 2017 117 337 B4). The Antares algorithm receives a cuff pressure signal in the deflation phase as input and separates the pulsatile signal component from the inherent cuff pressure. The individual pulse waves are identified. The weighted, multiple transforms of each pulse wave is based on several analytical steps, which could be called an adaptive transfer function. Grid points are then identified to calculate hemodynamic parameters such as cBP. The residual, or the margin between the actual and expected pressure of the deflated cuff, is calculated. Arrhythmias and other confounding artifacts are identified based on the residual and the shape of the pulse wave. By integrating Antares into the software of a BP device, a brachial cuff BP device is expected to become a type II PWA device with relatively accurate absolute cBP values independent of peripheral BP measurement. Also, Antares algorithm does not use any other patient information except the recorded pulse wave shapes and sex. For a more detailed description of the invasive and non-invasive measurement methodological approach, see Dörr et al.19
The invasively measured aortic reference BP including the experimentally determined SD reflects the instantaneous BP variation during the estimation of the calculated cBP by Antares. Information on the data distribution of invasive aortic BP and the corresponding beat-to-beat variation is presented in the online supplemental table S2 and S3. According to ISO 81060-2:2019,25 the measurement error by Antares was considered to be 0 mmHg when the estimation was within this range. When the calculated cBP was outside the range of the invasive aortic reference BP, the value of the adjacent range limit of the invasive reference BP was subtracted from the value of the calculated cBP.25 This difference represents the measurement error of this determination and was used to calculate the mean difference between the invasive reference and non-invasive recording within the study population.
Based on the information in the physician’s letter, 140 of the 389 patients (36%) had type 2 diabetes. Following ISO 81060-2:2019,25 15 cases had to be excluded due to high variation in invasive BP recordings (eight cases with SD in invasive systolic BP >20 mmHg, seven cases with SD of invasive diastolic BP >12 mm Hg). In addition, six cases were identified as extreme outliers (>3-fold IQR of mean difference between invasive reference and non-invasive recording) and excluded from statistical analysis because of implausible data and their confounding influence. This resulted in 119 patients with type 2 diabetes being included in the final analysis. Table 1 gives an overview of the patient characteristics.
Characteristics of the study population with type 2 diabetes
All 119 included patients were Caucasian, of whom cardiac catheter access was radial in 91 cases (76.5%) and femoral in 28 cases (23.5%). Three patients (2.5%) were younger than 50 years, 57 patients (47.9%) were between 50 and 70 years and 59 patients (49.6%) were older than 70 years. Ninety-four patients were within a heart rate of 60–100/min (78.9%).
All patient and measurement data were saved in a database (Excel 2019, Microsoft Corp, Redmond, Washington, USA) and analyzed with IBM SPSS Statistics V.22 software (IBM Corp). The data are reported as the mean±SD. Distribution of data was analyzed with Shapiro-Wilk test. In accordance with distribution of data, the Pearson product–moment correlation coefficient was used to assess the strength of linear association between invasive and non-invasive central BP. In addition, scatter plots were created for a graphical overview. Agreement between the invasive and non-invasive central BP was evaluated using Bland-Altman plots with limits of agreement (±1.96 SD). Significance level was set at p<0.05.
Results
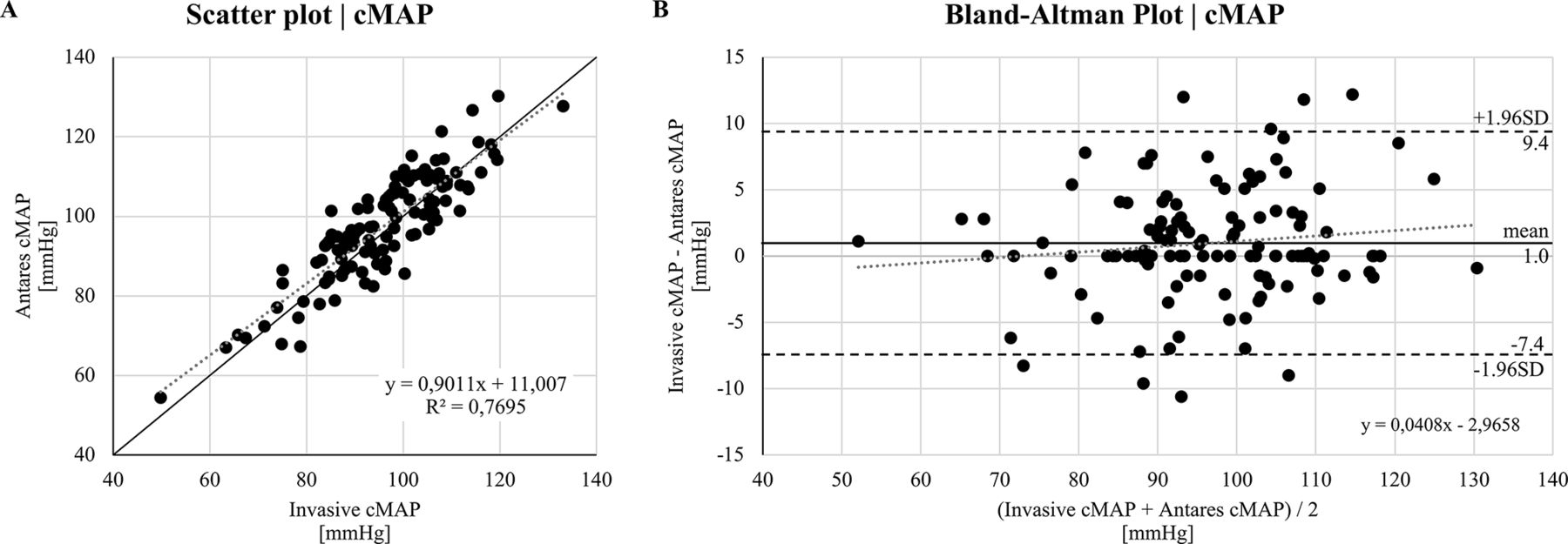
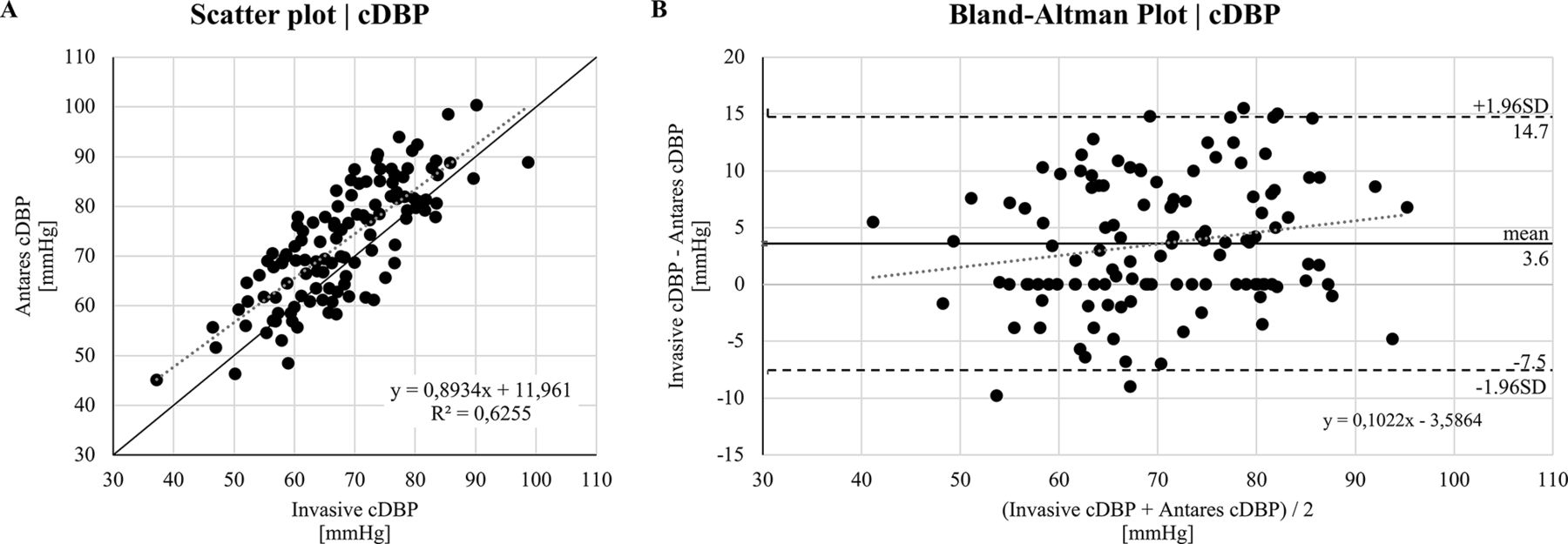
The statistical analysis for all 119 patients with type 2 diabetes revealed strong correlations between Antares non-invasively calculated cBP with invasively measured aortic BP for central systolic BP (cSBP; r=0.916, p<0.001), cMAP (r=0.882, p<0.001) and central diastolic BP (cDBP; r=0.791, p<0.001). The mean differences and SD for cSBP, cMAP and cDBP can be found in the corresponding Bland-Altman plots shown in figures 1–3 demonstrating good limits of agreement. The trend lines illustrate no significant overestimations or underestimations for cSBP, cMAP or cDBP.
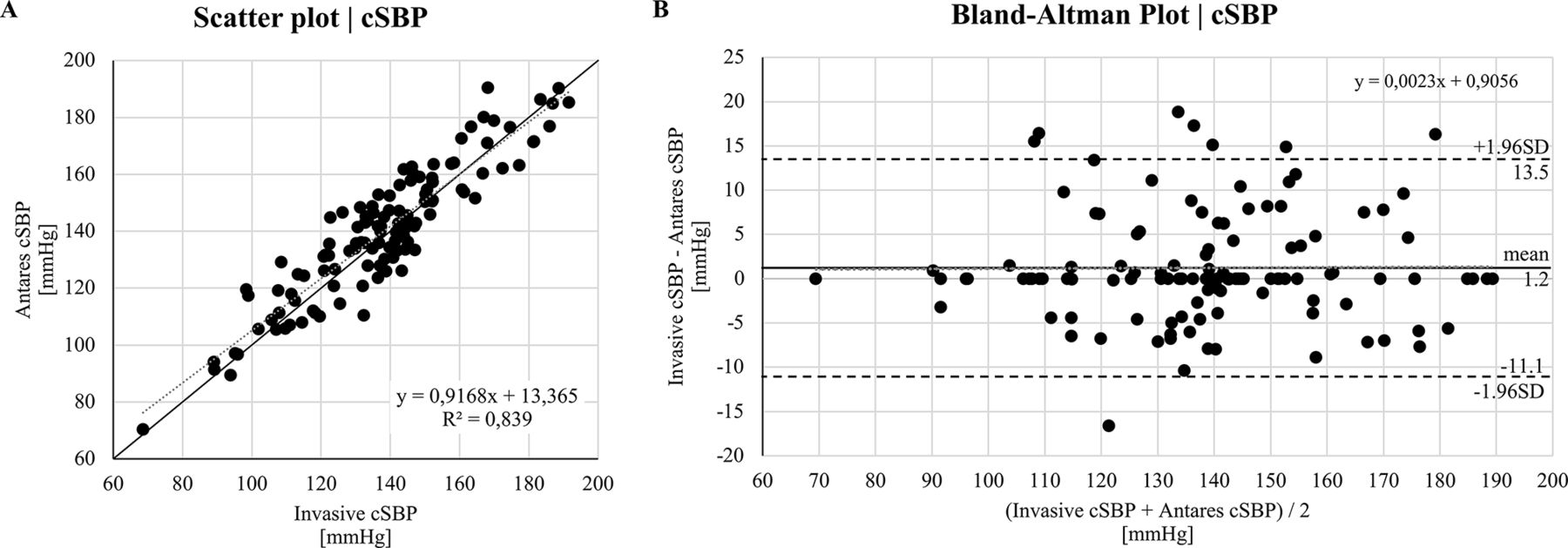
Relationship between invasive central systolic blood pressure (cSBP) and non-invasive cSBP (calculated with Antares) in patients with type 2 diabetes (n=119). (A) Scatter plot for invasive cSBP and Antares cSBP. Grey dotted line: linear regression line. Black line: identity line. R2, coefficient of determination. (B) Bland-Altman plot for invasive cSBP and Antares cSBP with the representation of mean difference (black line) and limits of agreement (black dashed line), from ±1.96 SD. Mean difference±SD: 1.2±6.3 mm Hg. Grey dotted line: linear regression line.

Relationship between invasive central mean arterial pressure (cMAP) and non-invasive cMAP (calculated with Antares) in patients with type 2 diabetes (n=119). (A) Scatter plot for invasive cMAP and Antares cMAP. Grey dotted line: linear regression line. Black line: identity line. R2, coefficient of determination. (B) Bland-Altman plot for invasive cMAP and Antares cMAP with the representation of mean difference (black line) and limits of agreement (black dashed line), from±1.96 SD. Mean difference±SD: 1.0±4.3 mm Hg. Grey dotted line: linear regression line.

{kind=link}
{kind=link}
{kind=link}
Relationship between invasive central diastolic blood pressure (cDBP) and non-invasive cDBP (calculated with Antares) in patients with type 2 diabetes (n=119). (A) Scatter plot for invasive cDBP and Antares cDBP. Grey dotted line: linear regression line. Black line: identity line. R2, coefficient of determination. (B) Bland-Altman plot for invasive cDBP and Antares cDBP with the representation of mean difference (black line) and limits of agreement (black dashed line), from±1.96 SD. Mean difference±SD: 3.6±5.7 mm Hg. Grey dotted line: linear regression line.
Discussion
The results presented in this study suggest that the Antares algorithm can qualify the custo screen 400 oscillometric BP monitor as a type II device for non-invasive estimation of cBP in patients with type 2 diabetes. Type II in this context means that the device can estimate the intra-arterial ‘true’ cBP (ie, relatively accurate absolute cBP value despite inaccuracy at the peripheral site).24 In contrast, a type I device provides an estimate of cBP relative to measured brachial BP (ie, a relatively accurate pressure difference between central and peripheral sites). This validation study, comparing invasively measured cBP with non-invasively estimated cBP based on oscillometric BP measurement, demonstrates that Antares meets validation requirements defined as a mean difference of ≤5.0 mmHg with an experimental SD of ≤8.0 mmHg.24 25 Furthermore, the study results show that they are in accordance with the AAMI/ESH/ISO statement (the probability of a tolerable error of ≤10 mmHg is at least 85%).26 In this context, a measurement error of Antares ≤10 mmHg was found in 117 subjects (98.3%) for cSBP, in 118 subjects (99.2%) for cMAP and in 119 subjects (100.0%) for cDBP. In addition, Antares was found to meet the British Hypertension Society criteria for grade A rated BP devices.
According to the 2017 ARTERY consensus statement,24 which includes most but not all the recommendations of ANSI/AAMI/ISO 81060-2:2019,25 a sample size of at least 85 patients is suggested, which was met in this validation study. However, ANSI/AAMI/ISO 81060-2:2019 claims that a clinical trial using invasive reference BP measurement should include at least 15 patients with no more than 10 valid BP measurements per patient, resulting in at least 150 valid BP measurements for validation. Thus, the present study did not fully comply with ANSI/AAMI/ISO requirements. We acknowledge that ANSI/AAMI/ISO 81060-2 was not developed to validate devices for noninvasive estimation of cBP against invasive pressures. Since Antares, analogous to the principle of the oscillometric waveform envelope (OMWE), provides only one value for cSBP, cDBP and cMAP, the comparison of these individual values with exclusively the mean value of the corresponding invasive reference would not sufficiently take into account the invasive physiological BP range to be considered (eg, due to respiration and other influencing factors). Therefore, we found it reasonable to follow the ANSI/AAMI/ISO protocol as well, in addition to the ARTERY consensus statement, because they include rules for considering this physiological pressure range within the aortic reference BP (calculation method of measurement error) and criteria for hemodynamic stability of invasive measurements. According to this, the invasively measured beat-to-beat variation of cBP in our study population was <10 mmHg for cSBP and <6 mmHg for cSBP (online supplemental table S3). In this way, hemodynamic stability can be assumed.
Several physiological factors influence cBP. In patients with type 2 diabetes, vascular irregularities such as endothelial dysfunction,27 central20 28–30 and peripheral31 arterial stiffness and risk factors for cardiovascular disease such as hyperlipidemia32 and smoking33 34 may have a greater impact on central than brachial BP, resulting in a higher central systolic burden. In this regard, a meta-analysis by Climie et al35 indicates that patients with type 2 diabetes have elevated central and brachial BP compared with healthy controls, as well as increased central systolic load, which cannot be identified by conventional measurement of brachial BP alone. There is evidence for the superiority of invasively measured cBP over brachial BP in the prediction of cardiovascular events,8–13 although this aspect has not yet been fully elucidated36 and needs to be subject of further research.
Cuff-based brachial BP measurement is currently the cornerstone of hypertension management. However, Picone et al37 demonstrated the inaccuracy of cuff BP compared with intra-arterial brachial and central BP. Based on the discrepancies identified (cuff overestimates DBP at brachial and aortic level; cuff underestimates SBP at brachial level) and their impact on the classification of BP according to clinical guideline criteria, there is an explicit call from a clinical perspective to develop more accurate non-invasive cuff BP methods for estimating brachial and/or central BP. Thus, as was done in the present study, these new methods must undergo robust validation according to appropriate protocol specifications to ensure their accuracy before they are used in patient care or population health studies. To be independent of the described potential error (underestimation of SBP, overestimation of DBP) of brachial oscillometric BP measurement, Antares internally performs recalibration of oscillometric waveforms to obtain mean arterial pressure and diastolic pressure, which are used as an internal preprocessing step for calibration. For recalibration, the shape of every oscillometrically recorded pulse wave is used by Antares.
To date, there is no comparable validation study for cuff-based oscillometric BP devices in patients with type 2 diabetes that would meet the requirements of the validation guidelines mentioned. Rossen et al38 compared the non-invasive determined cBP by Arteriograph, a brachial cuff-based, oscillometric device, with the invasively measured cBP in 22 patients with type 2 diabetes. They found a mean difference of 4.4±8.7 mmHg, with Arteriograph cBP systematically underestimated. Laugesen et al39 compared cSBP and cDBP data using the SphygmoCor device with invasively recorded data in 34 patients with type 2 diabetes. They found a difference of −2.3±5.6 mmHg for cSBP and 1.0±0.9 mmHg for cDBP when calibrating the SphygmoCor transfer function with invasively measured cSBP and cDBP in the ascending aorta. However, clinically, it would not make any sense to calibrate invasively a non-invasive oscillometric measurement for estimation of cBP. When calibrated non-invasively using oscillometric brachial BP measurements, DBP and mean BP appeared to provide the most accurate group-level estimate (1.9±12.2 mmHg, cSBP; 14.1±6.2 mmHg, cDBP),39 but also would not meet validation requirements of the aforementioned protocols. In addition, the authors noted that the large limits of agreement indicated limited accuracy in individual patients. However, comparison of the present study results with the studies of Rossen et al and Laugesen et al is limited because of the apparently different error determination methods used to determine the differences between invasively measured and non-invasively estimated cBP.
There are some limitations of this study. We only examined patients with type 2 diabetes who had a clinical indication for cardiac catheterization (eg, diagnosis of coronary heart disease and valve disease, heart failure and coronary intervention). Therefore, the results are not clearly applicable to patients with type 2 diabetes without suspected coronary disease. Because the multicenter invasive validation study was not explicitly planned for a diabetic population but was an inclusion criterion for study participation, no disease-specific data such as hemoglobin A1C (HbA1c) or information on diabetes treatment are available from the medical records. However, this is not a major limitation because it was intended to verify whether Antares was still accurate in estimating cBP in a clinical population with a substantial burden of central and peripheral vascular calcification and corresponding pulse wave characteristics. The case of calcification is underlined by the fact that 68% had coronary heart disease, 60% of patients underwent PCI and the mean body mass index was 30.1 kg/m2, all situations that potentially challenge the accuracy in performing PWA. Thus, the potential limitation of diabetes diagnosis being less informative is likely outweighed by the multiple other cardiovascular risk factors and status after cardiovascular events. Another limiting factor is the age distribution of the patients (only three patients were younger than 50 years). The low number in this age group is because younger people rarely have a clinical indication for cardiac catheterization. Another limitation is the small number of female study participants, who made up only 24% of the study population. Thus, the sample characteristics claimed in both validation protocols regarding gender distribution were not fully met. One more limitation is that although we invasively measured a total of 119 diabetic patients, we were only able to include eight patients with an invasive cSBP less than or equal to 100 mmHg and five patients with an invasive cDBP greater than or equal to 85 mmHg in the extreme BP ranges. Even though the Bland-Altman plots showed good agreement, further invasive comparisons must be carried out to determine whether Antares works as robustly in these extreme BP ranges as it does in the other ranges. As a further limitation, the sample size of at least 150 comparable BP measurements claimed in the ANSI/AAMI/ISO protocol was not achieved, as already indicated. From the authors’ point of view, however, the aspect of considering different BP ranges based on data from the much larger sample size (n=119) offers a significant advantage over the rigid validation requirement of a minimum of 15 patients with a maximum of 10 pairs of BP measurements each.
Conclusion
In conclusion, this study suggests that the Antares algorithm is able to transform the oscillometric custo screen 400 device into a type II device for estimating ‘true’ central BP in patients with type 2 diabetes. Whether Antares can also be integrated into other oscillometric BP devices with similarly robust results remains to be proven. However, our study has shown that Antares appears to be applicable in a clinical setting in patients with type 2 diabetes and several other cardiovascular risk factors and cardiovascular diseases.
Data availability statement
Data are available on reasonable request. The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by: (1) Landesärztekammer Thüringen (Reg.-Nr.: 36950/2018/76); (2) Ethics Committee University Medicine Greifswald (Reg.-Nr.: BB032/17); and (3) Ethics Committee Ruhr University Bochum (Reg.-Nr.: 2017-219). Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors AS and JB performed data management and analysis, manuscript writing and edition; MD, M-AO, SR and SE performed data collection and data management; SE helped in manuscript editing; CP, MK, SE and MD provided editorial assistance and scientific oversight for the manuscript. All authors have read and approved the final manuscript. AS is the guarantor of this work and as such had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Funding The University Medicine Greifswald and Zentralklinik Bad Berka have received non-targeted financial support by Redwave Medical GmbH for carrying out the study. The main parts of the study were financed by own funds of the participating centers. Redwave Medical GmbH did not have any influence on the design and conduct of the study as well as on data analyses and writing of the manuscript, except providing detailed information about the algorithm requested by the authors. The publication of this article was funded by the Open Access Publishing Fund of Leipzig University supported by the German Research Foundation within the program Open Access Publication Funding.
Competing interests AS has part‐time obligations in Redwave Medical GmbH. SE has received equipment for research projects from custo med. MD has received equipment for research projects from custo med and funding for research projects from Redwave Medical GmbH. JB has interest in Redwave Medical GmbH and has received equipment and lecture fees from IEM GmbH, BPLab, SMT medical GmbH & Co, SOT Medical Systems and Tensiomed. Redwave Medical GmbH had no role in the design, execution or interpretation of the study. Redwave Medical GmbH provided information about the algorithm requested by the authors.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.