Article Text

Abstract
Objective We compared the cost-effectiveness of two inpatient diabetes care models: one offered by a specialized diabetes team (SDT) versus a primary service team (PST).
Research design and methods We retrospectively evaluated 756 hospital admissions of patients with diabetes to non-critical care units over 6 months. Out of 392 patients who met the eligibility criteria, 262 were matched 1:1 based on the mean of the initial four blood glucose (BG) values after admission. Primary outcomes were 30-day readmission rate and frequency, hospital length of stay (LOS) and estimated hospital cost. Secondary outcomes included glycemic control and BG variability.
Results Diabetes complexity and in-hospital complications were significantly higher among patients treated by SDT versus PST. Thirty-day readmission rate to medical services was lower by 30.5% in the SDT group versus the PST group (P<0.001), while 30-day readmission rate to surgical services was 5% higher in the SDT group versus the PST group (P<0.05), but frequency of 30-day readmissions was lower (1.1 vs 1.6 times, P<0.05). LOS in medical services was not different between the two groups, but it was significantly longer in surgical services in SDT (P<0.05). However, LOS was significantly lower in patients who were seen by SDT during the first 24 hours of admission compared with those who were seen after that (4.7 vs 6.1 days, P<0.001). Compliance to follow-up was higher in the SDT group. These changes were translated into considerable cost saving.
Conclusions Inpatient diabetes management by an SDT significantly reduces 30-day readmission rate to medical services, reduces inpatient diabetes cost, and improves transition of care and adherence to follow-up. SDT consultation during the first 24 hours of admission was associated with a significantly shorter hospital LOS.
- inpatient diabetes management
- cost effectiveness
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Hospital admissions for patients with diabetes are more likely to originate from emergency departments; they account for 20.3% of all US hospital readmissions and their hospital length of stay (LOS) is frequently longer. Having a higher hemoglobin A1c was shown to be associated with higher hospitalization cost.
What are the new findings?
30-Day readmission rate to non-critical medical units is reduced by around 30% when a specialized diabetes team (SDT) is involved in inpatient diabetes care in comparison with standard diabetes care by primary service team.
SDT consultation within the first 24 hours of admission is associated with a significantly shorter LOS.
Diabetes management by SDT reduces hospital cost and improves postdischarge follow-up adherence.
How might these results change the focus of research or clinical practice?
This study suggests that more medical centers should consider using SDTs as part of their inpatient care for patients with diabetes. Benefits of SDT utilization warrant further investigation in prospective, long-term studies.
Introduction
In 2014, about 9.3% (29.1 million) of the US population were presumed to have diabetes mellitus (DM).1 The American Diabetes Association reported that the total cost of diabetes in 2012 was around $245 billion ($176 billion in direct medical costs).2 About 43% ($105.35 billion) were attributed to hospital admissions.2 An estimated 43.1 million hospital days (25.7% of the 168 million total hospital days) were incurred by patients with diabetes. Out of which, 26.4 million days were attributed to diabetes as primary diagnosis.2
Hospital admissions for patients with diabetes are more likely to originate from emergency departments (ED) and their hospital length of stay (LOS) is frequently longer.3 4 Higher glycated hemoglobin A1c (HbA1C), particularly >10%, was shown to be associated with higher hospitalization cost.5 Meanwhile, both hyperglycemia and hypoglycemia were shown to independently predict longer LOS.6 Improved glycemic control results in lower rates of in-hospital secondary complications.7 Reducing blood glucose (BG) variability was shown to be associated with reduced inpatient mortality,8 LOS, secondary complications9 and 30-day readmission rate.10 11 Prolonged exposure to hyperglycemia was also shown to be associated with higher risk of 30-day and 90-day readmission rates in patients with congestive heart failure (CHF).12
In most US hospitals, a primary service team (PST) is responsible for diabetes management in both medical and surgical non-critical care units and only few hospitals use specialized diabetes teams (SDT). Diabetes management by SDT usually includes diabetes evaluation and management by an endocrinologist or a diabetes nurse practitioner, general diabetes education by a dietitian and/or a certified diabetes educator followed by providing a diabetes discharge/transition plan and follow-up. This comprehensive diabetes care may be particularly valuable for patients with poorly controlled diabetes. However, it is unclear if comprehensive diabetes management by SDT is a better resource utilization when compared with diabetes management by PST. The main objective of this study is to compare the impact of the two different models of diabetes care on 30-day readmission rate and overall hospital cost in both medical and surgical non-critical care units.
Methods
We conducted a comprehensive retrospective chart review of 756 consecutive patients with DM diagnosis admitted to the non-critical care units at a tertiary referral medical center in Boston, Massachusetts, USA, between July 2012 and January 2013. All non-pregnant patients aged 18 years and older with established diagnosis of DM were included in the study regardless of their primary admitting diagnosis(es). HbA1C of >6.5% or treatment with any antihyperglycemic medications was considered an additional confirmation of DM diagnosis. Newly diagnosed patients during hospital admission or patients with DM diagnosis of <3 months were excluded. We also excluded patients whose LOS is <2 days to ensure our ability to collect enough BG readings for this analysis. We presumed that within such short admission period, neither teams were to considerably impact study outcomes. We also excluded patients with long LOS of more than 10 days, as the average LOS in non-critical units in US hospitals is less than half of that duration (4.8 days).13 This strategy would mirror typical admissions and exclude outliers. All eligible patients who were readmitted within 30 days of their first admission or readmitted during the study period were only evaluated at their first admission.
During the 6-month study period, we identified 756 hospital admissions to non-critical care units with DM mentioned as primary, secondary or tertiary diagnosis on admission. Out of them, 392 patients were older than 18 years of age, non-pregnant and had an established DM diagnosis for >3 months. Out of these 392 patients, 262 were matched in 1:1 ratio (131 in each group) based on the mean value of their first four BG readings after admission. We used this criterion to ensure a common starting point for fair comparison between the two groups. We included in our analysis an equal number of patients managed in medical and surgical services for each group. The matching process was conducted by a biostatistician blinded to all study data except those values needed for matching as outlined.
Secondary medical complications specified for this study include new infections such as pneumonia or urinary tract infection, preoperative or postoperative infections, acute kidney injury (AKI), acute liver injury, myocardial infarction, CHF, acute cerebrovascular accident, gastrointestinal bleeding and transfer to intensive care unit (ICU). Diabetes complexity was defined as presence of type 1 diabetes diagnosis, HbA1C >8.5% or presence of secondary medical complications during hospital admission.
Models of care
The PST group included patients managed by hospitalists, general internal/family medicine or general surgery physicians with or without involvement of house staff. The comparative group included patients managed by an SDT from Joslin Diabetes Center (JDC) who were consulted to manage DM. This team included an endocrinologist (with or without house staff or endocrinology fellow), a diabetes nurse practitioner, a certified diabetes nurse educator and discharge/transition coordinators. Comprehensive discharge pathway based on risk category was only offered in medical units, while routine discharge process was used in surgical units according to the hospital policy. This pathway indicates that patients with DM discharged on insulin are considered high-risk. A coordinated transition of DM care is synchronized between the medical center and JDC’s outpatient clinic, where high-risk patients are scheduled to see their primary care physicians (PCPs), endocrinologists or diabetes nurse practitioners within 1–4 days of discharge and other patients are scheduled to see them within 2 weeks of discharge. General diabetes education and education assessments were provided for 30–60 min by a certified diabetes educator during hospital admission. Endocrinologists followed specified diabetes management protocols based on JDC guidelines for hospitalized patients. PST did not use any specific protocols in diabetes management.
Time of consultation
To further evaluate the impact of SDT on DM management, we subdivided this group according to the time of initial consultation: (1) early SDT consultation: if requested SDT consults were initiated within the first 24 hours of admission; and (2) late SDT consultation: if requested consults were initiated after 24 hours of admission. This allowed us to properly evaluate the impact of SDT on hospital outcomes based on their time of involvement in DM management.
Follow-up
Patients’ follow-up plans were obtained from discharge summaries. We were able to track if patients kept their follow-up appointments by reviewing providers’ notes in the medical center’s electronic health records (EHRs). However, we were only able to review this information for patients whose PCPs or endocrinologists are within the medical center’s network of hospitals and clinics. Around 18% were outside this network. Due to this limitation, accurate assessment of follow-up adherence was deficient for some patients.
Data collection
During this study period, all capillary BG values during admission were captured to evaluate glycemic control, BG variability and episodes of documented hypoglycemia or hyperglycemia. For the SDT group, BG values were subdivided to before and after consultations. We defined hypoglycemia as BG <70 mg/dL and hyperglycemia as BG >180 mg/dL. BG variability was expressed as the SD of mean BG. All other clinical variables such as in-hospital secondary complications, mortality, LOS, 30-day readmission and primary diagnosis of first readmission were collected from the hospital EHR and scanned paper charts.
Study outcomes
The three primary outcomes of this study are 30-day readmission rate and frequency, LOS, and estimated hospital admission cost. Secondary outcomes include glycemic control, BG variability and incidence of hypoglycemia and hyperglycemia.
Statistical methods
Demographic and baseline characteristics were evaluated using descriptive statistics. All continuous variables were presented as means and SDs, and non-normally distributed variables were presented as medians and IQRs. All nominal/categorical variables were presented as frequencies and percentages. For comparisons between the two study groups, independent samples t-test was used for continuous variables. χ2 or Fisher’s exact tests were used to compare categorical variables. Multivariate linear regression analysis was used to find predictors of the following numerical end-points: LOS and the total number of 30-day readmissions. Multivariate logistic regression analysis was used to define predictors of the following binary end-points: occurrence of any complications during inpatient admission, provided follow-up referrals at time of discharge and readmitted within 30 days of discharge. For all methods mentioned above, 95% CIs were used and P values <0.05 were considered statistically significant. Stata V.12 software was used for data analysis.
Results
There were no differences in gender between the two study groups, but patients in the PST group were significantly older (P<0.001) (table 1). Degree of diabetes complexity was significantly higher among patients treated by SDT versus PST (HbA1C 8.7±2.1% vs 7.4±1.3%, respectively, P<0.001 for both). In-hospital secondary complications were significantly higher among patients treated by SDT versus PST (60.6% vs 20.6%, respectively, P<0.001). These complications include new infections, AKI, acute liver injury, myocardial infarction, CHF, acute cerebrovascular accident, gastrointestinal bleeding and transfer to ICU. Additionally, the SDT group had eight times the number of patients with type 1 diabetes (34.1% vs 4.6%, respectively, P<0.001). All patients on insulin pump in this cohort were managed by SDT as dictated by the medical center’s internal policy. Baseline demographic data are outlined in table 1.
Baseline characteristics of patients managed by the primary service team (PST) and by the specialized diabetes team (SDT)
Rates of hyperglycemia and hypoglycemia were significantly higher in the SDT group (P<0.001) (table 2). Diabetes consultation with SDT was initiated within the first 24 hours of admission in more than half of patients evaluated in this cohort. Surgical services were slightly more inclined to consider late consultations to SDT than medical services. There was significant improvement in average BG values pre-SDT versus post-SDT consults (215±58 vs 192±44 mg/dL, P<0.001). However, there was no difference in average BG values after early versus after late consults in the SDT group. We also did not find any difference in average BG values between PST and SDT for either early or late consults. Patients with type 2 DM followed by SDT had significantly lower BG variability (72 vs 87 mg/dL, P<0.01) than patients with type 1 DM followed by the same team.
Metabolic control during hospitalization and discharge disposition in patients managed by the primary service team (PST) and by the specialized diabetes team (SDT)
There was no difference in discharge disposition to home or home care with visiting nurse services between the two groups. However, PST had significantly higher rate of discharge to rehabilitation and skilled nursing facilities (P<0.001 for both) (table 2). More patients in the SDT group were referred to their PCPs and endocrinologists (P<0.001 for both). For patients with in-network trackable hospital follow-up visits, we found that patients seen by SDT were more likely to keep their appointments with their PCPs or endocrinologists after discharge (P<0.001 for both) (table 3).
Transition of care in patients managed by primary service team (PST) and by specialized diabetes team (SDT)
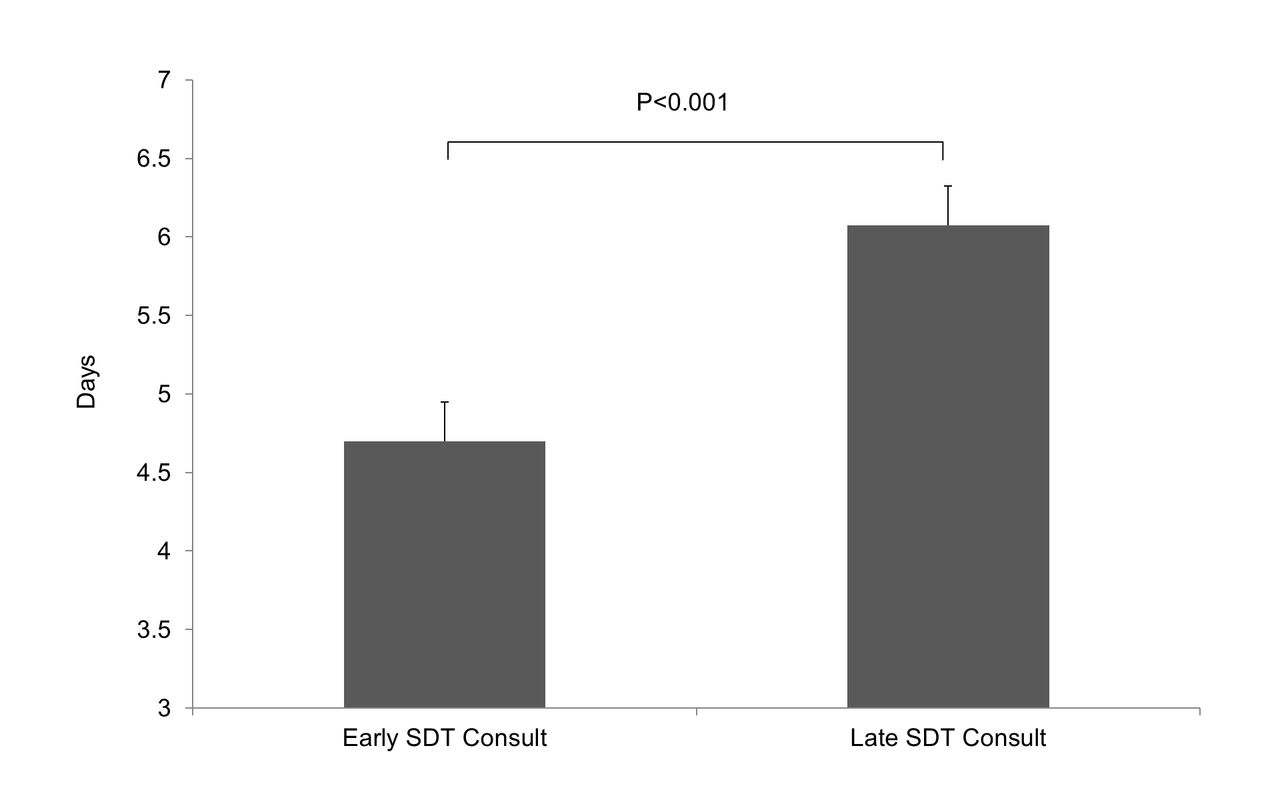
The 30-day readmission rate to medical services in the SDT group was 30.5% lower than the PST group (22.5 vs 32.4%, respectively, P<0.001), with non-significant difference in frequency of admission during 30 days (1.1 vs 1.2 times, respectively, P>0.05). The 30-day readmission rate to surgical services in the SDT group was higher than the PST group (26.7% vs 21.7%, respectively, P>0.05), but the frequency of 30-day readmission was significantly lower (1.1 vs 1.6 times, P=0.015) (table 4). The most common reasons for readmission are CHF, pneumonia and acute cardiovascular events. LOS was not different between the two groups (table 4). Patients who received SDT consultations within 24 hours of admission had a significantly lower LOS compared with patients who received SDT consultations after 24 hours (4.7 vs 6.1 days, P<0.001) (figure 1).

{kind=link}
Hospital length of stay depending on the time of specialized diabetes team (SDT) consult after admission. Values are mean±SEM. Early: within 24 hours of admission; late: >24 hours of admission. n=131, 58% in the early SDT consult group and 42% in the late SDT consult group.
30-Day readmission rate and length of stay in patients managed by primary service team (PST) and by specialized diabetes team (SDT)
Considering hospital cost, historical hospital data showed that 30-day readmission rates for all patients to non-critical medical and surgical services irrespective of diabetes diagnosis were 16.6% and 13.9%, respectively, in 2011, and 15.1% and 9.7%, respectively, in 2012. Based on a constructed cost model for a total of 6695 admissions with diabetes in 2011 and the 5567 admissions in 2012, we estimate that the full utilization of SDT for all patients with DM was to prevent 500 readmissions to medical services in 2011 and 416 readmissions in 2012 while increasing readmissions to surgical services by 36 in 2011 and 44 in 2012. Since the national average of hospital cost for patients with diabetes was $7830 per admission in 2010,14 we estimate that full utilization of SDT for all patients with DM in non-critical care units of the medical center would save $2.9 million in hospital cost in 2011 and $3.5 million in 2012 (table 5).14
Postulated model of cost saving if specialized diabetes team (SDT) were to manage all patients with diabetes admitted in 2011 and 2012 in comparison with primary service team (PST) (model is calculated based on the actual admissions with diabetes diagnosis in 2011 and 2012)
Discussion
Healthcare spending is progressively increasing and accounts for one-fifth of the US economy.15 In 2012, the Centers for Medicare and Medicaid Services started to apply hospital penalties by reducing payments to hospitals for readmissions in an attempt to reduce national healthcare expenditure on diseases like heart failure, pneumonia and acute myocardial infarction.16 Uncontrolled hyperglycemia was shown to worsen outcomes and increase readmission rates in some of these comorbid conditions.12
SDT utilization was previously evaluated in several studies, which reported different outcomes.17–19 Results from one pilot study showed that SDT utilization resulted in reducing patients’ 30-day hospital readmission rate.17 However, another pilot study showed that patients managed by an SDT had reduced visits to ED, but with no change in readmission rates owing to patients’ disease complexity as evident by their longer LOS.18 On the other hand, a recent study showed that SDT utilization for preoperative diabetes management improved glycemic control and reduced LOS.19
Observed reduction in readmission rate among patients managed by SDT in this study, particularly in medical units, could be multifactorial. This may include better glycemic control, inpatient diabetes education (IDE), comprehensive discharge plan and appropriate transition of care. This notion is further supported by recent logistic regression models that elucidate formal IDE to be independently associated with lower frequency of all cause 30-day readmission rates.20 One may argue that PST in this study cared for older patients who are more likely to have poorer outcome in general. However, the PST group represented a relatively healthier cohort with better baseline HbA1C and a lower percentage of in-hospital secondary complications. On the other hand, patients with type 1 DM were largely managed by the SDT group. Those patients tend to be younger, usually on insulin pumps, treated with complex insulin regimens and have higher BG variability. Therefore, higher frequencies of hypoglycemia and hyperglycemia in the SDT group were not surprising. It is known that readmission is traditionally higher among patients with higher HbA1C on admission, patients with type 1 DM, and patients with multiple acute and chronic comorbid conditions.21 22
In contrast to medical units, the readmission rate to surgical units was not improved in the SDT group. Diabetes education was provided to all patients in the SDT group in both medical and surgical units, so it is unlikely to contribute to any difference in outcomes between the two units. However, coordinated and comprehensive diabetes discharge plan with mandatory recommendations of PCPs or endocrinologists follow-up was only offered in medical units and might contribute to the observed difference in readmission between medical and surgical units. Involvement of SDT in DM management occurred after 24 hours of admission in over 50% of patients evaluated in this study. Trend of late consultations was higher in surgical units and might contribute to the observed differences in readmission rate between the two units. We rationally expect that earlier consultations to SDT during the hospital course may lead to better glycemic outcomes.
In this study, consulting SDT was appropriate for managing complex diabetes cases irrespective of the BG readings on admission. It was noticed that patients managed by the SDT were more likely to be referred to their PCPs and/or endocrinologists on discharge and were more likely to comply with their transition of care. This is an important step in preventing medication errors since medication reconciliation is required at various stages of patient care and may reduce frequency of unnecessary utilization of urgent or emergent care resources. In most if not all the hospitals across the USA, discharge instructions, follow-up plans and transition policies are handled by the PST, guided by hospital policy, patients’ health insurance and availability of hospital services that handle transition of care. In this study, involvement of SDT increased the likelihood of appropriate transition of care and improved adherence to follow-up plans. Outpatient care following proper diabetes discharge plan by SDT in medical wards might prevent readmission since reduction in readmission was not seen in surgical wards for the same group, where there is no diabetes discharge plan or proper follow-up.
In this study, involvement of SDT in DM management had no impact on LOS, which is typically longer by 1 day for patients with DM compared with patients without DM.21 We found that hospital LOS was shorter in the PST group in comparison with the SDT group. This may be explained by the higher observed frequency of in-hospital secondary complications, larger number of patients with type 1 DM and higher HbA1c in the SDT group. Additionally, patients who were managed by SDT early in their hospital admissions had a significantly shorter LOS. It was long-debated which strategy has better positive impact on hospital cost: reducing 30-day readmission rate or reducing LOS. In the last few years, the Centers for Medicare and Medicaid Services, the largest insurer/payer in the USA, and many other insurance plans shifted toward reducing 30-day readmission rate rather than reducing LOS.23 It has been shown that single readmission usually costs more than an additional 1–2 days of hospital stay during first admission.24
This study suggests a considerable cost saving if SDT were to care for all patients admitted with DM diagnosis. Cost saving was slightly offset by increased readmissions to surgical units. Providing comprehensive discharge plans and transitions of care for surgical patients similar to those implemented for medical patients might contribute to additional cost saving.
This study has several limitations. First, it is a retrospective study conducted at a single, academic, tertiary care center and included a relatively small number of patients over a limited time period. The retrospective study design has the advantage of reporting accurate, real-life, hospital scenarios without any intention to change DM management behavior. However, this study design still has its own limitations, which include inability to properly match the comparative groups and inability to control timing of SDT consultation. Other clinical centers may have different protocols for diabetes care and different transition plans, so it is difficult to assume that these results are valid or reproducible in other hospitals. This study was not designed to evaluate newly diagnosed patients with DM during first admission, a patient population which may have different metabolic and hospital outcomes. It is assumed that this category of patients may benefit from basic diabetes education during admission and from structured diabetes discharge and transition plans.20 Although all readmissions were individually verified, it may be possible that readmissions to other hospitals occurred and were not reported in patients’ EHR. For these reasons and to confirm our findings, we suggest a prospective randomized multicenter clinical study that neutralizes baseline variables for comparative groups, calculates actual costs and includes newly diagnosed patients and patients admitted to the ICU. Since patients with DM diagnosis account for 20.3% of all US hospital readmissions,14 this proposed study may be of great importance in our quest to reduce hospital cost of patients with DM.
In conclusion, this study suggests that using an SDT to manage diabetes in non-critical medical units may result in significant reduction in 30-day readmission rate in comparison with managing DM by a PST. Consultations of SDT should be initiated early after admission and preferably within the first 24 hours of admission in order to reduce LOS. Transition of DM care after discharge to PCPs and/or endocrinologists should be encouraged for all patients with DM discharged from either medical or surgical units to improve follow-up adherence and reduce 30-day readmission rate.
Acknowledgments
The authors would like to acknowledge the support of the Office of Business Conduct and Quality at Beth Israel Deaconess Medical Center and the billing department of Joslin Diabetes Center for providing access to patients’ data.
References
Footnotes
Contributors VB supervised study conduct and drafted its manuscript. AM contributed to statistical analysis, and reviewed and edited the manuscript. TKP did statistical analysis. NA, EC and AC collected patient data. MS shared in manuscript writing. RAG reviewed and edited the manuscript. OH supervised study conduct, shared in data analysis and edited the manuscript.
Funding The study was internally funded.
Competing interests OH receives research support from Abbott Nutrition, Novo Nordisk, Intarcia and the National Dairy Council; consults for Merck; and is on the advisory board of AstraZeneca. RAG consults for Onduo.
Patient consent Detail has been removed from this case description/these case descriptions to ensure anonymity. The editors and reviewers have seen the detailed information available and are satisfied that the information backs up the case the authors are making.
Ethics approval The study protocol was approved by the medical center’s internal review board (Committee on Clinical Investigations, Beth Israel Deaconess Medical Center).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.