Article Text

Abstract
Objective To evaluate the impact of an integrated diabetes and kidney disease model of care on health-related quality of life (HRQOL) of patients with comorbid diabetes and chronic kidney disease (CKD).
Research design and methods A longitudinal study of adult patients (over 18 years) with comorbid diabetes and CKD (stage 3a or worse) who attended a new diabetes kidney disease service was conducted at a tertiary hospital. A questionnaire consisting of demographics, clinical data, and the Kidney Disease Quality of Life (KDQOL-36) was administered at baseline and after 12 months. Paired t-tests were used to compare baseline and 12-month scores. A subgroup analysis examined the effects by patient gender. Multiple regression analysis examined the factors associated with changes in scores.
Results 179 patients, 36% of whom were female, with baseline mean±SD age of 65.9±11.3 years, were studied. Across all subscales, HRQOL did not significantly change over time (p value for all mean differences >0.05). However, on subgroup analysis, symptom problem list and physical composite summary scores increased among women (MD=9.0, 95% CI 1.25 to 16.67; p=0.02 and MD=4.5, 95% CI 0.57 to 8.42; p=0.03 respectively) and physical composite scores decreased among men (MD=−3.35, 95% CI −6.26 to −0.44; p=0.03).
Conclusion The HRQOL of patients with comorbid diabetes and CKD attending a new codesigned, integrated diabetes and kidney disease model of care was maintained over 12 months. Given that HRQOL is known to deteriorate over time in this high-risk population, the impact of these findings on clinical outcomes warrants further investigation.
- quality of Life
- chronic kidney disease
- type 2 diabetes
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Among patients with chronic kidney disease (CKD), health-related quality of life (HRQOL) gradually declines as the disease progresses with the worst scores reported by those with advanced renal disease.
When CKD coexists with diabetes, a marked deterioration in HRQOL is expected.
What are the new findings?
HRQOL was preserved over 12 months among those attending a codesigned integrated diabetes and kidney disease model of care.
When women and men were considered separately, the symptom problem list and physical composite scores significantly improved among women while the physical composite score slightly deteriorated among men.
How might these results change the focus of research or clinical practice?
Person-centered integrated clinics for patients with diabetes and renal dysfunction are a promising approach for improving patient outcomes such as HRQOL.
Introduction
Diabetes has become a major challenge to healthcare delivery in the 21st century1 and data from economic modeling suggest a substantial increase in global health expenditure attributable to diabetes care.2 The global prevalence of diabetes is expected to rise to 592 million cases by 2035 up from 415 million cases of diabetes reported in 2015.3 This increase in the number of people with diabetes has led to an upsurge in the number of patients with chronic kidney disease (CKD) and those commencing renal replacement therapy (RRT), in combination with an overall trend of earlier commencement of dialysis.4 The accelerating growth in patients with comorbid diabetes and CKD requiring RRT and the associated health and resource implications highlight the need for new directions in managing this high-risk population.
The management of patients with comorbid diabetes and CKD is complex and requires considerable coordination and facilitation of care during the disease continuum. Integrated person-centered diabetes and kidney disease clinics have emerged as a promising approach to the management of patients with comorbid diabetes and CKD.5 These clinics reduce the unnecessary burden of multiple appointments for patients who already have multiple comorbidities. Patients attending these clinics also have input from a multidisciplinary team including endocrinologists, nephrologists, nurse educators and dietitians.6 7 Additionally, some combined diabetes and kidney disease specialty clinics have reported improvements in metabolic and blood pressure control,5 7 a reduction in progression of renal disease8 and outpatient cost savings.9 However, previous studies have not reported the effects on patient-reported outcomes such as health-related quality of life (HRQOL).
Among patients with CKD, HRQOL gradually declines as the disease progresses10 with the worst scores reported by those with advanced renal disease.11 When CKD coexists with diabetes, a marked deterioration in HRQOL is expected.12 The objective of this study was to evaluate the impact of an integrated diabetes and kidney disease model of care13 on HRQOL of patients with comorbid diabetes and CKD.
Methods
Study design and population
This was a longitudinal study with a follow-up period of 12 months for adult patients (over 18 years) with diabetes and CKD who were referred to the Diabetes Kidney Service (DKS)13 at Monash Health between January 2015 and August 2017. The diagnosis of diabetes was noted in medical records and/or confirmed by laboratory results as per the World Health Organisation (WHO) criteria.14 15 Patients were considered to have CKD if they had a sustained estimated glomerular filtration rate (eGFR) <60 mL/min/1.73 m2 calculated using the Chronic Kidney Disease Epidemiology Collaboration equation16 (ie, two or more eGFR readings) over a 3-month period. Patients were excluded if they had an eGFR ≥60 mL/min/1.73 m2 since this may reflect normal physiologic age-related changes in kidney function. The reporting in this study followed the Strengthening the Reporting of Observational Studies in Epidemiology guidelines.17
The diabetes and kidney disease model of care
The diabetes and kidney disease model of care used by the DKS has been described in detail before.13 In brief, this model of care was codesigned by general practitioners (GP), endocrinologists, nephrologists, nurse practitioners, patients with diabetes and CKD and patient advocacy groups such as Diabetes Australia and Kidney Health Australia in 2015. The design was informed by findings from a large multisite formative evaluation of the barriers and enablers of current health services for diabetes and CKD, and the needs of patients, carers, and their health professionals.18
The diabetes and kidney disease model of care provides patient-centered, coordinated multidisciplinary assessment and management of patients with comorbid diabetes and CKD in partnership with primary care. This service is designed to improve patient self-management and improve communication and coordination of care between endocrinologists, nephrologists and GPs, who remain the coordinator of patient care. As a new initiative, the service also provides a liaison service/GP phone advice hotline to discuss referrals and patient queries during office hours (09:00 to 17:00 hours) and education on managing diabetes and CKD. The team includes a consultant endocrinologist and nephrologist, specialist registrars in endocrinology and nephrology, diabetes and renal nurse practitioners, dietitian, administration and a research officer (for continual service evaluation and improvement). Consistency is maintained by using standard patient assessment templates and minimizing staff attrition. Fidelity assessment is performed monthly to ensure that all aspects of the clinic run as per design. Criteria for referral to the integrated clinic include type 1 or type 2 diabetes with an eGFR <60 mL/min/1.73 m2.
Measures
Demographic and clinical variables
Age, gender, ethnicity, alcohol and smoking history, stage of kidney disease, duration of kidney disease and duration of diabetes were obtained from the first questionnaire (online supplementary appendix 1) which was prospectively completed by site study staff or the clinician, using standardized procedures from the doctor’s notes and laboratory results from the clinic.
Supplemental material
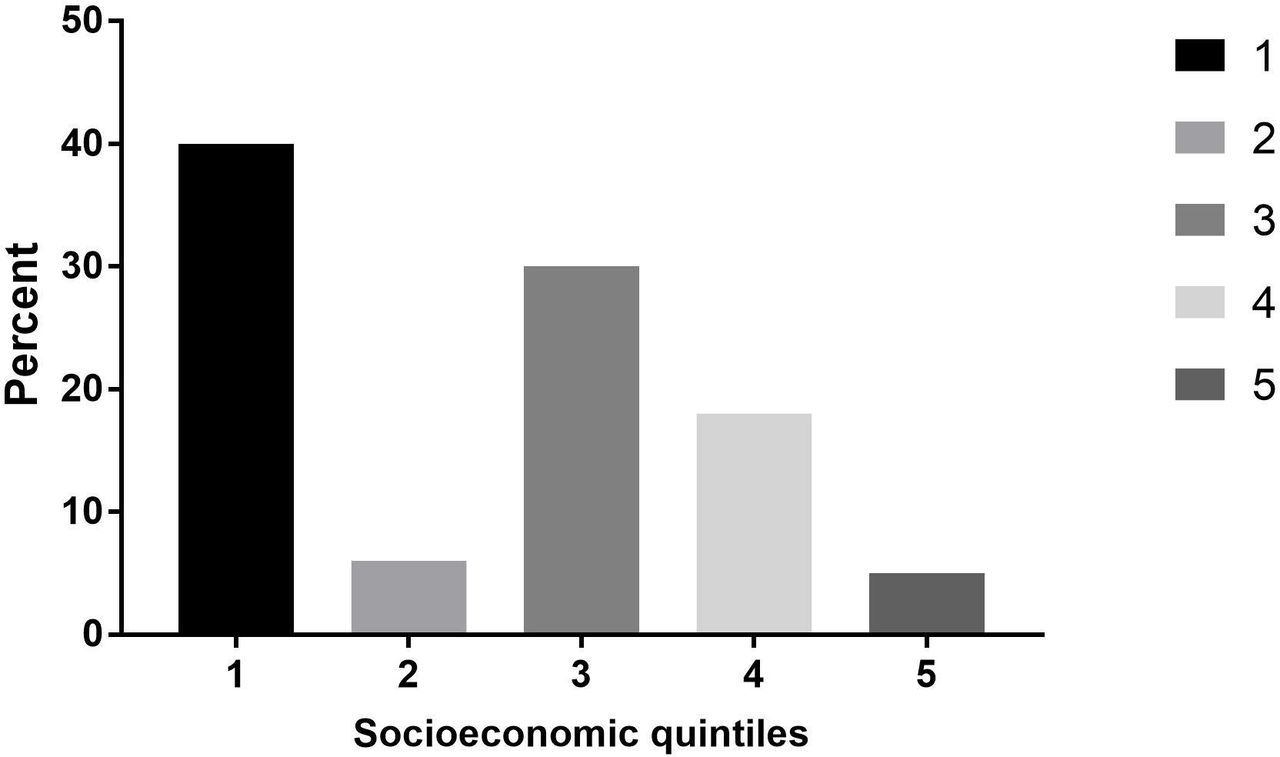
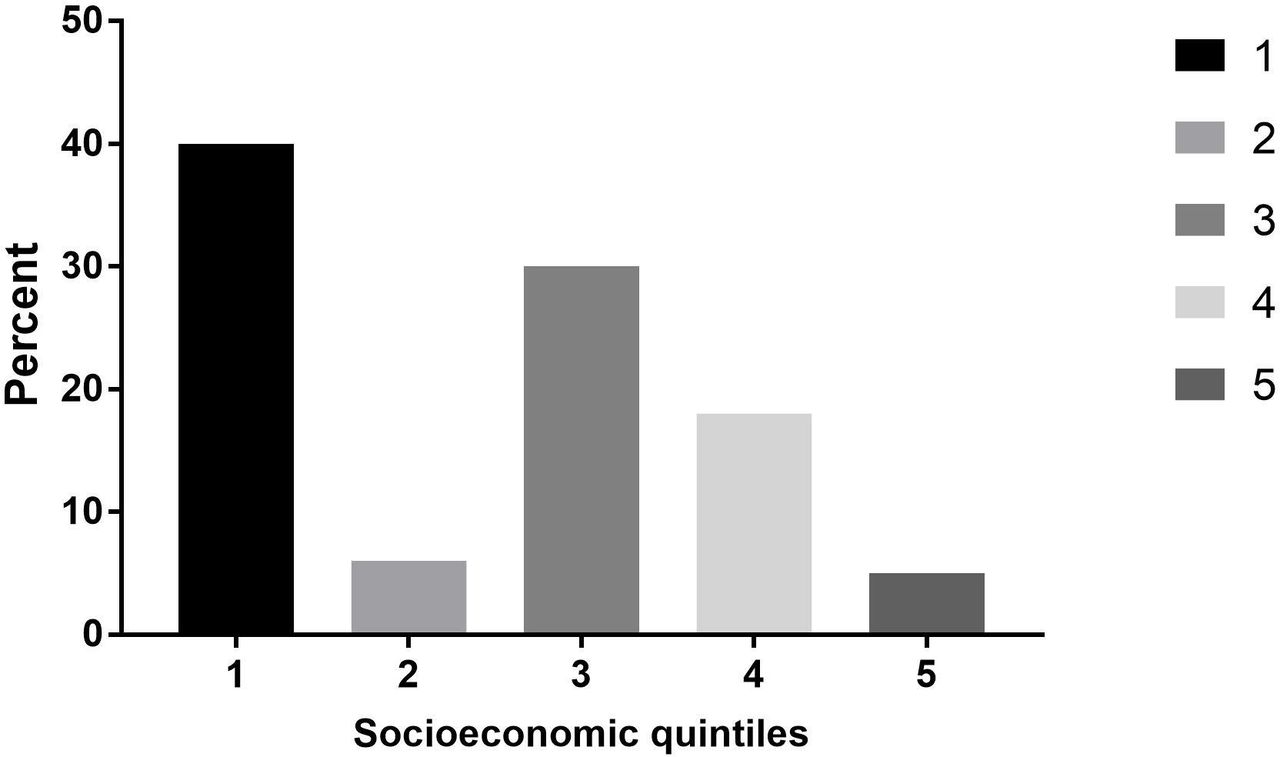
Socioeconomic status (SES) was estimated using the Australian Bureau of Statistics data. Postcodes were coded according to the Index of Relative Social Disadvantage (IRSD), a composite measure based on selected census variables, which include income, educational attainment and employment status. The IRSD scores for each postcode were then grouped into quintiles. The first quintile had individuals from the most disadvantaged areas and the fifth quintile comprised individuals from the least disadvantaged areas.19
Health-related quality of life
HRQOL was assessed using the English version of the Kidney Disease Quality of Life (KDQOL-36) questionnaire. The KDQOL-36 comprises two composite scores for physical and mental health with a population mean of 50 (SD=10) and three kidney disease-specific scales. The three kidney disease-specific scales are the burden of kidney disease, symptom/problems list and the effects of kidney disease subscales20 (online supplementary appendix 2). Item scores were summed for each scale and transformed on a scale of 0–100 with a higher score indicating better HRQOL. The scores of the two summary measures and the total 36-Item Short Form Health Survey (SF-36) are based on the average of the respective scale components.
Supplemental material
Statistical analysis
First, participants with missing values in the KDQOL measure (that did not allow for calculation of the subscales) were excluded following the recommendations of the instrument’s developers.21 Second, means and SDs for all HRQOL subscales were calculated for baseline and follow-up scores. Change scores were calculated as the difference between follow-up and baseline scores. Deteriorations in HRQOL were denoted by a negative value in change scores while a positive value denoted improvements. Third, we compared baseline and follow-up scores of the HRQOL subscales by paired sample t-tests. Lastly, we performed multiple regression analyses using the change scores as dependent variables to determine the factors associated with the change scores. Potential predictor variables for change in HRQOL scores were age, gender, stage of kidney, duration of diabetes and SES which we have described previously.22 To determine whether changes in scores were clinically meaningful, we used the guidelines set by the developers of the SF-36, which suggest that a 5–10 point change along any of the instrument’s subscales is clinically meaningful.23 In our analysis, we defined clinically meaningful results as a 5-point difference in scores from baseline to 12 months. CIs were reported at the 95% level and results were considered significant at conventional p<0.05 level. All analyses were performed with Stata V.15.0 (StataCorp, College Station, TX).
Results
Participants
Of a total of 393 patients screened, 290 entered the study. During follow-up, 11 died (before the 12-month visit) and 179 (64%) completed the 12-month questionnaires (figure 1). The baseline demographic and clinical characteristics of the study population are shown in table 1. Thirty-six percent of the participants were women. At baseline, the mean (SD) age for all participants was 65.9±11.3 years and 64.3±11.8 and 68.6±9.8 years for men and women, respectively. Participants came from various racial and ethnic groups with only 24% having been born in Australia. Forty percent of the participants lived in the most disadvantaged areas (quintile 1) (figure 2). All had diabetes with most having type 2 diabetes (97%) and moderate to advanced CKD (83% stage 3–4 CKD). For all patients, mean subscale scores at baseline were 72.5±20.5, 74.4±23.4, 59.2±30.8, 35.5±10.6 and 48.3±10.5 for the symptom problem list, effect of kidney disease, burden of kidney disease, physical composite summary and mental composite summary scales, respectively (table 2). Patients who did not complete the 12-month follow-up were comparable to patients who did with respect to age, gender, duration of diabetes, type of diabetes and stage of CKD (online supplementary table S1).
Supplemental material
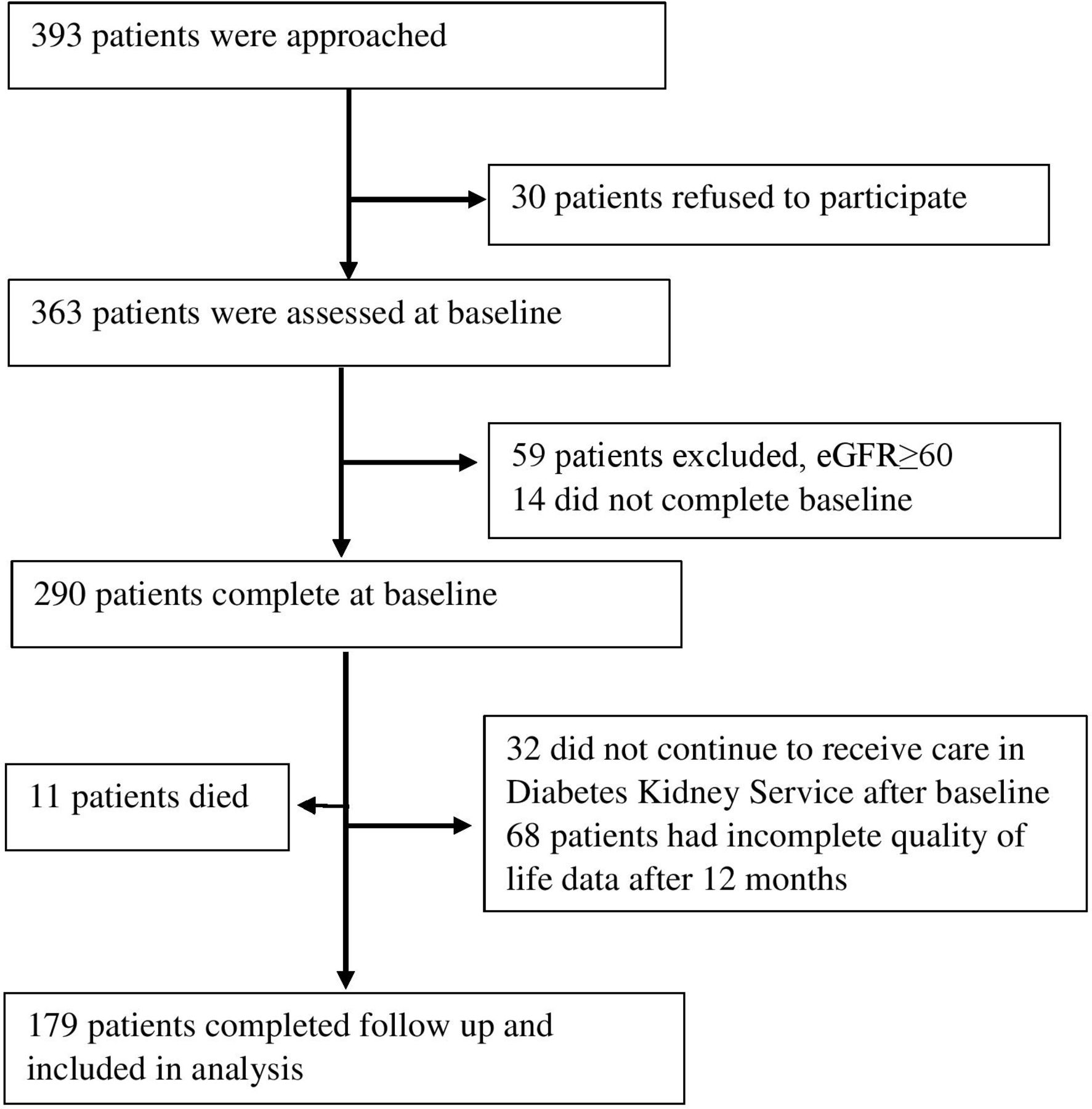
Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) flow diagram of included patients. eGFR, estimated glomerular filtration rate.
{kind=link}
{kind=link}
Socioeconomic status in quintiles. The first quintile had individuals from the most disadvantaged areas and the fifth quintile comprised individuals from the least disadvantaged areas.
Characteristics of patients who completed the study
Change in health-related quality of life scores for all patients (n=179)
Changes of HRQOL scores from baseline to follow-up
Across all subscales, HRQOL did not significantly change over time (p value for all mean differences >0.05 and all change scores less than 5 points) (table 2). However, on subgroup analysis, symptom problem list and physical composite summary scores increased for women (MD=9.0, 95% CI 1.25 to 16.67, p=0.02 and MD=4.5, 95% CI 0.57 to 8.42, p=0.03 respectively) and physical composite scores decreased for men (MD=−3.35, 95% CI −6.26 to −0.44; p=0.03) (table 3).
Change in health-related quality of life scores from baseline to follow-up by gender
Factors associated with change scores
The changes in the symptom problem list and physical composite summary scores were 11 and 8 points (p<0.05) greater in women than in men (table 4). The changes in the effect of kidney disease, burden of kidney disease and mental composite score for patients with stage 5 kidney disease were 21, 38 and 9 points (p<0.05) greater than for patients with mild kidney disease, respectively (table 4).
Multiple linear regression analysis of change scores for all patients
In men, the changes in the symptom problem list and effect of kidney disease scores in those with stage 5 kidney disease were 48 and 44 points (p<0.05) greater than in those with mild kidney disease (online supplementary table S2). In women, the symptom problem list change score for those aged 67 years or older was on average 12 points less (p<0.05) than for those aged less than 67 years. In addition, women with stage 5 kidney disease had greater changes in the burden of kidney disease scores (39 points; p<0.05) than women with mild kidney disease (online supplementary table S3).
Supplemental material
Supplemental material
Discussion
In this longitudinal study of patients with comorbid diabetes and CKD, we have shown that HRQOL was preserved over 12 months among those attending a codesigned integrated diabetes and kidney disease model of care. Scores across all the subscales of the KDQOL instrument were similar at entry into the new service and at 12 months’ follow-up. When women and men were considered separately, the symptom problem list and physical composite scores significantly improved among women while the physical composite score slightly deteriorated among men. Among all patients, those with stage 5 kidney disease experienced a greater improvement in scores for the effect of kidney disease, burden of kidney disease and mental composite summary scores than those with mild kidney disease.
Several studies of patients with CKD have reported that HRQOL significantly deteriorates over time24 25 with the major predictors of the decline being a reduction in eGFR, age and other comorbidities.26 Notably, in studies of patients with comorbid diabetes and CKD, HRQOL deteriorated at a faster rate than in patients with CKD alone.24 Our longitudinal study has found that a codesigned integrated diabetes and kidney disease model of care may prevent deterioration of HRQOL among patients with comorbid diabetes and CKD especially among those with stage 5 CKD. Reasons for this may be that the integrated service provides patient-centered care, higher quality of care, appropriate patient referrals and greater convenience for the patient which when put together, maintain HRQOL. However, the impact of the integrated service on HRQOL may have been influenced by response shift, a phenomenon which occurs when patients change their values and the conceptualization of quality of life over time.27
Cross-sectional studies among patients with comorbid diabetes and CKD22 28 have previously reported that women have lower HRQOL scores compared with men especially in the physical composite score. In our study, we had expected the physical composite scores for both men and women to decline over time as reported previously.29 However, the physical composite scores for women remained stable while those for men declined minimally. This suggests that women may have been more amenable to the interventions embedded within the integrated service than men. To optimize the benefits of the integrated service to men, peer support-based interventions may need to be provided.30
Our data demonstrate that an integrated clinic especially improved HRQOL in patients with advanced kidney disease who are known to have very low quality of life.25 Patients with stage 5 kidney disease experienced a greater change in scores for the effect of kidney disease, burden of kidney disease and mental composite summary scores than those with mild kidney disease. A reason for this is that those with advanced kidney disease may have better accepted their diagnosis31 and been ready to embrace interventions embedded within the integrated clinic to improve their HRQOL. Another reason is that patients with advanced kidney disease may get more attention from clinicians compared with patients with mild kidney disease leading to improved quality of life in particular subscales as seen in this study. This especially applies to those on or commencing dialysis where frequent interactions with nursing and medical staff is the norm. Additionally, an improvement in quality of life may be perceived differently by patients with advanced kidney disease and those with mild kidney disease. A slight improvement in quality of life for patients with stage 5 kidney disease may have a greater influence on how they feel than in patients with mild kidney disease. We did not expect patients with advanced kidney disease to have clinically significant change scores in the physical composite scale compared with those with mild kidney disease due to the physical limitations associated with comorbid diabetes and CKD.
Findings in this longitudinal study have important implications for practice and future research. First, the determinants of HRQOL in patients with comorbid diabetes and CKD are clearer and most importantly, HRQOL may be improved or preserved by interventions codesigned by patients and health professionals. Second, HRQOL should be routinely measured in patients with comorbid diabetes and CKD to enable the provision of tailored interventions. Currently, HRQOL measurement in patients with comorbid diabetes and CKD remains largely a research endeavor, although monitoring HRQOL in routine clinical care has been shown to be feasible.32
Our findings should be interpreted in light of the strengths and limitations of our study design. The strengths include the use of a study design that allowed us to evaluate the impact of codesigned integrated diabetes and kidney disease model of care on HRQOL of patients with comorbid diabetes and CKD over time. Additionally, our participants were drawn from a diverse population allowing for generalizability of study findings. Lastly, there were no differences between patients who completed the study and those who were lost to follow-up. The limitations include that two measurement points may provide less stable results compared with multiple data collection points. However, we chose not to survey patients more frequently to avoid bias associated with repeated testing. Furthermore, patients were followed up for a period of 12 months which may not be enough to realize the full impact of the integrated diabetes and kidney disease model of care on HRQOL. Finally, the interpretation of results from this study was limited by the lack of a control group. A randomized controlled study design although preferable was not feasible due to the complexity of interventions embedded within the integrated diabetes and kidney disease model of care.
In conclusion, this longitudinal study is the first to report on the impact of a codesigned, integrated diabetes and kidney disease model of care on HRQOL among patients with comorbid diabetes and CKD. We have shown that quality of life was maintained, and even improved across some subscales, among patients with comorbid diabetes and CKD. Integrated diabetes and kidney disease care may be particularly important for improving patient experience and clinical outcomes.
Acknowledgments
We acknowledge D Giannopoulos for help in study conduct.
References
Footnotes
Contributors EZ, CL and SZ conceptualized the study. EZ, CL, SR and SZ performed data curation. EZ designed the analysis in consultation with CL, SR, HT, TU, KRP, PGK, GF, MG, SJ, AC, RW, GR, GJ and SZ. EZ drafted the original draft and all authors reviewed and edited the final manuscript.
Funding This work was supported by a National Health and Medical Research Council, Australia (NHMRC) Partnership Grant (ID 1055175) between the following health services, research institutes and national consumer stakeholder groups: Alfred Health; Concord Hospital; Royal North Shore Hospital; Monash Health; Monash Centre for Health Research and Implementation, Monash University; The George Institute for Global Health, University of Sydney; Diabetes Australia; and Kidney Health Australia. An Australian Postgraduate Award Scholarship supported CL. HT was supported by an NHMRC, Practitioner Fellowship. An NHMRC Senior Research Fellowship supported SZ.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Monash University and Monash Health Human Ethics Review Committees.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information. No additional data available.