Article Text

Abstract
The objective of this systematic review was to determine the effectiveness of lifestyle interventions to improve the management of type 2 diabetes mellitus (T2DM) among migrants and ethnic minorities. Major searched databases included MEDLINE (via PubMed), EMBASE (via Ovid) and CINAHL. The selection of studies and data extraction followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. In the meta-analysis, significant heterogeneity was detected among the studies (I2 >50%), and hence a random effects model was used. Subgroup analyses were performed to compare the effect of lifestyle interventions according to intervention approaches (peer-led vs community health workers (CHWs)-led). A total of 17 studies were included in this review which used interventions delivered by CHWs or peer supporters or combination of both. The majority of the studies assessed effectiveness of key primary (hemoglobin (HbA1c), lipids, fasting plasma glucose) and secondary outcomes (weight, body mass index, blood pressure, physical activity, alcohol consumption, tobacco smoking, food habits and healthcare utilization). Meta-analyses showed lifestyle interventions were associated with a small but statistically significant reduction in HbA1c level (−0.18%; 95% CI −0.32% to −0.04%, p=0.031). In subgroup analyses, the peer-led interventions showed relatively better HbA1c improvement than CHW-led interventions, but the difference was not statistically significant (p=0.379). Seven studies presented intervention costs, which ranged from US$131 to US$461 per participant per year. We conclude that lifestyle interventions using either CHWs or peer supporters or a combination of both have shown modest effectiveness for T2DM management among migrants of different background and origin and ethnic minorities. The evidence base is promising in terms of developing culturally appropriate, clinically sound and cost-effective intervention approaches to respond to the growing and diverse migrants and ethnic minorities affected by diabetes worldwide.
- diabetes mellitus
- type 2
- self-management
Data availability statement
Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as supplemental information. Data are available in a public, open access repository.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The number of international migrants reached 272 million in 2019, up from 221 million in 2010.1 The proportion international migrants worldwide increased from 2.8% in 2000 to 3.5% in 2019,2 with >50% of them living in just 10 countries.2 The reasons for the rising numbers of people migrating from low-income and middle-income countries (LMICs) to high-income or industrialized countries (according to the World Bank classification)3 are multidimensional but can be classified into push (eg, poverty, crimes, wars, etc) and pull (eg, better employment and educational opportunities, access to services, political stability, etc) factors.2 4–7 On arriving in their host countries, international migrants experience lifestyle changes, which over time predispose them to an increased risk of non-communicable diseases (NCDs) such as type 2 diabetes mellitus (T2DM).4
While T2DM has emerged to become one of the leading causes of mortality worldwide,5 6 it remains unequally distributed between and within nations. Migrants from LMICs residing in high-income countries are disproportionately affected by T2DM, but the risk varies among ethnic groups.4 7–9 A meta-analyses by Meeks et al8 found that the risk of developing T2DM among migrants living in Europe (first-generation migrants) was higher than Europeans. Migrants from South Asia had the highest odds of T2DM, followed by those from the Middle East and North Africa, sub-Saharan Africa, the Western Pacific and South and Central America.8 Similarly, past studies have reported that the prevalence of diabetes was higher among migrants compared with the host population.9–11
It has been reported that migrants and ethnic minorities suffer disproportionately from diabetes-related complications12 including higher rates of avoidable hospital admissions.13 In the Southall and Brent Revisited study, undertaken in the UK, those originating from South Asia were found to have increased prevalence of both diabetes13 and cardiovascular diseases compared with white Europeans.14 Evidence shows that T2DM does not impact all population groups equally as there exists important differences relating to age, sex, ethnicity and family background.15 Socially disadvantaged groups, including migrants and ethnic minorities, are more likely to be exposed to obesogenic environments and experience more vulnerable lifestyle such as unhealthy eating, physical inactivity, tobacco smoking and excessive alcohol consumption.16–18
Despite migration-related and ethnic minorities-related inequalities and inequities in the burden of T2DM,8 9 there is limited evidence of what works in these subpopulations in terms of T2DM prevention and management. Furthermore, migrants and ethnic minority populations remain under-represented in these interventions.12 Most of T2DM interventions in high-income countries focus on highly accessible subpopulations and tend to include migrants and ethnic minorities with high levels of English proficiency or the host country’s official language.4 These studies show that lifestyle interventions which focuses on improving healthy eating habits, physical activity, smoking cessation, reducing harmful use of alcohol, social and cultural support and tailored in local language can be effective in preventing the development of T2DM and associated complications.19 20 Given the global call in the Sustainable Development Goals (SDGs)21 to curb the problem of NCDs and enhance healthy quality of life, there is a critical need for interventions that engage migrants and ethnic minorities to bridge migration-related inequalities in T2DM, and to address their elevated risk of the complications associated with this chronic disease.22 This systematic review addresses this gap by addressing following questions: (1) What types of interventions have been used to improve diabetes health outcomes among migrants and ethnic minorities living in industrialized countries? (2) What is the effectiveness of such interventions in improving clinically important primary outcomes such as hemoglobin (HbA1c), blood glucose levels, lipids and secondary outcomes such as weight, body mass index (BMI), diet, physical activity, tobacco smoking, alcohol consumption? and (3) What is the cost of such diabetes interventions?
Methods
The selection of studies and data extraction followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.23 The protocol of this review was registered in the Prospective Register of Systematic Reviews (PROSPERO, registration #CRD42020114770).
Search strategy and study selection
Articles were identified through a systematic literature search from the MEDLINE (via PubMed), EMBASE (via Ovid), CINAHL and PsychINFO databases between January 2000 and August 2019. The search terms were developed by a study team member (LR) in close consultation with an experienced medical librarian based on Medical Subject Headings (MeSH) terms with input from the author/s (AMNR). Subsequently, the PubMed search terms were adapted to EMBASE and CINAHL criteria. Further manual searching for additional articles was done using relevant databases including the Cochrane Central Register of Controlled Trials Register, Proquest dissertation, Agency for Health Care Research and Quality and Google Scholar. The search terms were mapped to MeSH terms/subject headings and used with keyword searches. The key terms for searching migrants and those with low socioeconomic status included: (“migrant population” OR “migrants”) (“low socio-economic status” OR “ethnic minorities” OR “poor” OR “poverty” OR “disadvantaged” OR “underprivileged” OR “vulnerable”) with filters to “Clinical Trial”, “Randomized controlled trials”; Publication date from January 1, 2000 to August 31, 2019 and the studies conducted among humans). For diabetes, the MeSH term included: “Diabetes Mellitus Type 2” OR “Glucose Intolerance” OR “Diabetes prevention” OR “Diabetes Complications”. The search strategy employed for Medline is attached as online supplemental appendix 1.
Supplemental material
The titles and abstracts of the articles retrieved were screened by LR to exclude articles that did not meet our inclusion criteria. LR further reviewed the full text of the remaining articles and selected eligible full-text articles, which was checked by BWS. Discrepancies were resolved by consensus with BJS and AMNR. References for each of the studies were screened for potential studies missed out in the search.
Inclusion and exclusion criteria
Studies were included if: (1) they were lifestyle or behavioural intervention studies undertaken to improve management of T2DM among migrants and ethnic minorities residing in host industrialized countries; (2) management of T2DM was undertaken using non-pharmacological interventions and (3) they reported diabetes primary outcome HbA1c. The international migrants were defined according to the United Nations2 24 25 and WHO26 classifications as those individuals who have crossed their state boundaries and have been staying in the host countries for various reasons.2 24 25 This includes temporary labour migrants; irregular, illegal or undocumented migrants; highly skilled and business migrants; refugees; asylum seekers; those experiencing forced migration; migrants uniting with their families; return migrants and long-term, low-skilled migrants.
All forms of intervention studies were included regardless of the setting (community or health facility based). Studies were excluded if: (1) published in languages other than English or (2) were reported in reviews, qualitative studies, editorials, abstracts, theses, books, case reports and letters to the editor. If publications presented data from the same study, only the publication with the largest sample size, which measured the T2DM or its components, was included.
Quality assessment of the studies
The quality of the studies included in the review was assessed using the ‘quality assessment tools for intervention studies’ as recommended by the National Collaborating Centre for Methods and Tools.27 28 The assessment covered selection bias, study design, confounders, blinding, data collection methods, intervention integrity, method of analysis, withdrawals and dropouts. For each section, a methodological rating of strong, moderate or weak was given, which led to an overall study rating. The results of the quality assessment were used as part of the criteria in rating the quality of evidence. LR reviewed the full-text articles for quality assessment, which was checked by BWS. Discrepancies in terms of quality assessment were resolved by consensus with BWS and AMNR.
Data extraction and synthesis
Relevant data from each of the selected studies were extracted using an Excel spreadsheet for this review. These data included: first author; study title; country of study; sample size; sociodemographic characteristics of participants; study design; random allocation; follow-up; intervention methodology and persons involved in implementing the intervention; an assessment of the quality of evidence and intervention outcomes (primary and secondary outcomes). Where more than one paper was published reporting outcomes from the same study, these were cross-checked to determine the presence of additional relevant information.
Data analyses and heterogeneity of studies
We undertook meta-analyses of those studies providing the data on mean changes of HbA1c levels among both intervention and control groups and both at baseline and at follow-up. Seven studies provided these data and were included in the meta-regression analyses. Data were analyzed to measure the pooled mean difference of HbA1c levels among the migrants and ethnic minorities who received lifestyle interventions compared with the usual care groups. Subgroup analyses were performed to compare the effect of lifestyle interventions according to intervention approaches (peer-led vs CHW-led). We assessed heterogeneity using the I2 statistic and a random effects model was used due to the heterogeneity of the studies (I2 >50%)29 that may have resulted because of the differences in sample size, study design, intervention design and outcome measures. Publication bias was assessed using Begg’s adjusted rank correlation test, Egger’s regression asymmetry test, and visual inspection of funnel plots.30
Results
Identification of studies
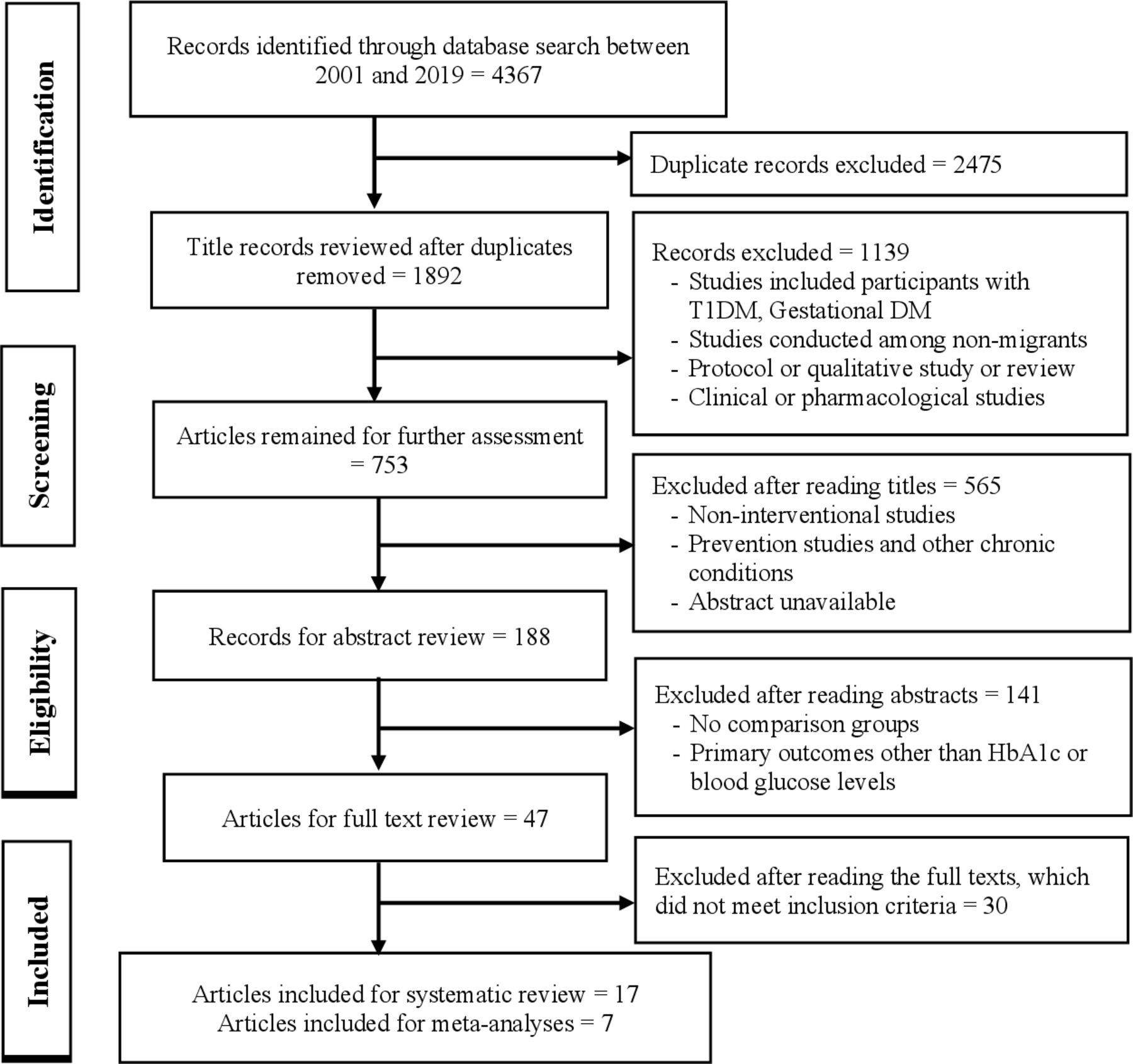
The search of different databases yielded 4367 studies. A total of 1892 non‐duplicated publications were screened. The titles and abstracts were screened for 188 studies and after removing reviews, duplicate studies, non-interventional lifestyle studies and studies in native rather than migrant and ethnic minority populations, 47 studies met full-text review criteria. The full-text manuscripts were reviewed and further assessed for eligibility and finally, 17 studies met inclusion criteria and were included in this review. Seven studies which provided required data were included in the meta-analyses (figure 1).

Systematic review flow diagram. DM, diabetes mellitus; HbA1c, hemoglobin A1c; T1DM, type 1 diabetes mellitus.
Participants characteristics and study designs
The characteristics of the studies included in this review are summarised in online supplemental table 1. The studies were conducted in the USA (n=13, 76.5%),31–43 the UK (n=2),44 45 Spain (n=1)46 and the Netherlands (n=1).47 Eight studies were conducted among migrants of European, Caucasian, American, Mexican or Middle East background,31–35 40 41 46 five among those of black and African backgrounds36–39 42 and four43–45 47 among South Asian migrants. Altogether, there were 5018 total participants with T2DM included in these studies. The total participants in each intervention ranged from 7742 to 868,45 with mean age of the participants ranged from 49.641 to 60 years.42 The majority of the studies were randomized controlled trials (14/17), while three used prospective randomized, repeated measures40 and experimental pre-test-post-test designs.35 41
Supplemental material
Intervention characteristics and outcome measures
The majority of the interventions were delivered by either trained community health workers (CHWs)34–38 40 41 43–47 or by peer supporters/leaders.31–33 39 42 The World Health Organization Study Group in 1989 defined CHWs as members of communities who are supported by the health system but not necessarily a part of its organization, and have shorter training than professional workers.48 Dennis defined peer supporters as ‘a person who has experiential knowledge of a specific behaviour or stressor and similar characteristics as the target population’.49 The intervention duration ranged from 3 weeks (one study) to 6 months (five studies) and 10–12 months (nine studies). All studies assessed primary outcomes, such as HbA1c or fasting plasma glucose, as well as the secondary outcomes such as weight, BMI, physical activity level, tobacco smoking, alcohol consumption, food habit and healthcare utilization. Altogether, 11 studies reported use of insulin medication for T2DM treatment at baseline, which ranged from 5.8% in study by Brown et al41 to 71.5% by Long et al.42
Peer support interventions
Most interventions were based on the chronic disease self-management approach. Lorig et al implemented a 6-week diabetes self-management program delivered by peer leaders, where participants received a 2.5-hour weekly program, followed by an automated telephone call.31 Participants were given the option of listening to 90 min vignettes about various aspects of diabetes, and each of 15 vignettes was offered twice over 15 months.31 Safford et al paired the participants with peer coaches and were provided with diabetes self-management education, followed by telephone calls by coaches on a weekly basis for the first 8 weeks, then monthly for a total of 10 months. Thom et al33 tested a 6-month intervention in which peer coaches helped patients to design action plans and provided regular support (via phone calls and face-to-face meeting). Similarly, Lujan et al34 and Long et al42 also used peer coaches using both face-to-face and telephone calls.
CHWs-led interventions
Philis-Tsimikas et al32 tested an intervention delivered by a combination of CHWs and peer educators over 6 months. The intervention participants attended 8-weekly 2-hour diabetes self-management classes run by the CHWs along with subsequent monthly support groups led by a trained peer educator. In a study by Islam et al,43 trained CHWs provided five 2-hour monthly group educational sessions and two one-on-one visits lasting ~90 min each. The intervention contents were culturally and linguistically adapted for Bangladeshi community members. Middelkoop et al implemented CHW-led (nursing staff and a dietician) education sessions over a period of 3 months (three visits at least), followed by subsequent monthly support.47 In an intervention by Culica et al,35 patients were provided with three 60 min individual education sessions, followed by 60 min quarterly assessment and case management visits by bilingual CHWs, over a 12-month period. Frosch et al37 implemented 6-month intervention package consisting of a short video on lifestyle change, a workbook and five sessions of telephone coaching by a trained diabetes nurse. Lima et al46 engaged general practitioners (GPs) to undertake diabetes management assessment, and to provide advice, counseling and clinical care to participants over 12 months.46 Studies by Kangovi et al36 and Brown et al40 also used CHWs to facilitate discussion and lifestyle interventions over 6 and 12 months, respectively.
Combination of CHWs and peer support
Keyserling et al38 used both the CHWs and peer leaders and the intervention lasted for 12 months. In a study by Brown et al,41 the participants in the ‘compressed’ group received 8 weekly 2-hour educational sessions followed by support sessions held at 3, 6 and 12 months, whereas the participants in the extended group received a series of 12 weekly 2-hour sessions on diabetes self-management, followed by 14 2-hour support group sessions.41 The studies by O’Hare et al44 and Bellary et al45 used trained multilingual workers and diabetes specialist nurse.
Risk of bias of the included studies
The overall quality of the studies was determined as moderate for 14 studies and weak for 3 (online supplemental table 2). The quality of the recruitment of participants in ensuring representative samples of the target populations was determined as moderate in seven studies and weak in the remaining studies. Two studies specified a sampling frame for recruitment of participants,33 37 with another 15 studies relying on referrals from GPs, engagement with community health clinics or by advertisement. The study design was assessed strong for one RCT,39 moderate for 14 RCTs31–34 36–38 40 41 43–47 and weak for two studies.35 42 Because of the nature of the studies, which require lifestyle interventions for patients with T2DM, the intervention was not blinded in any of the studies, but three studies mentioned that the persons involved in assessing outcomes were blinded.31 32 39
Supplemental material
The quality of data collection methods was determined as strong in one study,31 weak in three studies32 42 46 and moderate in the remainder. All studies described the procedures for collecting both the primary and secondary outcomes and mentioned that they used validated measurement tools. All studies used accredited laboratories for measuring HbA1c and lipids. Four studies were classified as strong which provided details for withdrawal and dropout of participants,31 32 37 38 10 as moderate33 35 39–45 47 and 2 as weak.34 36
In terms of intervention integrity, two studies were considered as strong31 38 and the remainder as moderate. The studies rated as strong provided details including intervention development, the theoretical basis, intervention frequency, compliance and the methods of providing follow-up contacts for participants.31 38 Those studies rated as moderate described what was delivered for both the interventions and the control arms and the duration of the intervention and follow-up.32–37 39–41 43–47 No studies provided information about the fidelity and consistency of the lifestyle interventions delivered to participants or reported on possible contamination by lifestyle interventions which were not related to the study.
Assessment of quality in terms of analysis and adjustment of confounders was determined as strong in four studies,33 37 39 41 44 45 weak in four studies32 34 38 42 and as moderate in the remainder.31 35 36 40 43 46 47 Three studies used intention-to-treat (ITT) analyses and adhered to the Consolidated Standards of Reporting Trials guidelines.33 37 41 Two studies used complete cases only with no imputed data for those lost to follow-up.33 37 The studies rated as moderate on this criteria provided basic information about assessment of relative effect sizes, but no further details such as adjustment for confounding, use of ITT and other steps in analyses.32 34 38 40 43 47 The quality of data analyses was determined as strong in 6 studies31 33 36 38 39 41 moderate in 10 studies32 34 35 37 40 43–47 and weak in 1 study.42 Studies used one-way analysis of covariance (ANCOVA) and two-way ANCOVA to examine differences between the groups at follow-up.31 36 38 40 41 Studies used generalized additive mixed models,39 and a linear mixed model and logistic regression.33 Other studies used paired t-tests, whereas one study provided no details about the statistical tests used.34 See online supplemental table 2 file for details.
Meta-analyses findings
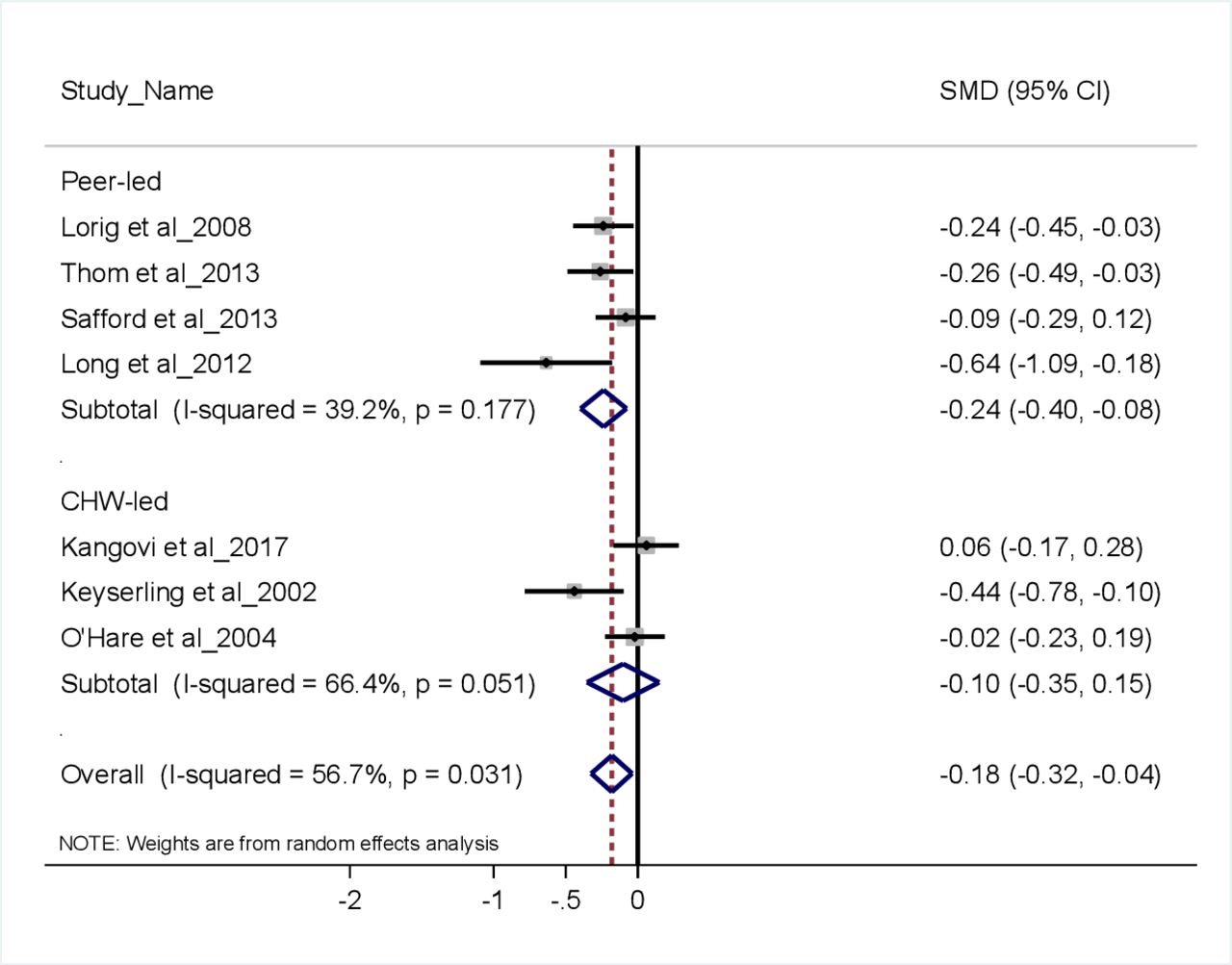
Seven studies that provided data on mean change in HbA1c levels were included in the meta-regression analyses. Findings show lifestyle interventions delivered among the migrant and ethnic minorities adults with diabetes are associated with a small but statistically significant reduction in HbA1c level of −0.18% (95% CI −0.32% to −0.04%, p=0.031) (figure 2). In subgroup analyses (figure 3), the peer-led interventions showed relatively better outcomes in terms of HbA1c reduction compared with CHW-led interventions (−0.24%, 95% CI −0.40% to −0.08%, p=0.177 vs −0.18%, 95% CI −0.32% to −0.04%, p=0.031), but the difference was not statistically significant (p=0.379). Because of a small number of studies included in meta-analyses (seven studies), we were unable to perform analyses for secondary outcome measures such as BMI. In the efforts of obtaining necessary data (mean and SD of HbA1c changes at follow-up) required for meta-analyses, we communicated personally with the corresponding authors of the studies, however we were unable to obtain such data.

Effect of lifestyle interventions on improving hemoglobin A1c (HbA1c) levels.

{kind=link}
{kind=link}
{kind=link}
Subgroup analyses accessing the effect of lifestyle interventions by peer support and community health workers (CHW)-led interventions.
Intervention effectiveness
The findings concerning the effectiveness of different intervention approaches are described below.
Peer support interventions
Most of the peer support interventions showed modest levels of effectiveness on clinical and behavioural outcomes including HbA1c, lipids level, BMI, health distress level, self-reported health outcomes, etc. Lorig et al31 reported intervention participants improved HbA1c levels by 0.41% vs 0.05% in control participants, after 6 months. Furthermore, the intervention participants improved HbA1c levels of 0.32% at 18 months and the changes were statistically significant (p=0.030).31 The intervention also improved secondary health outcomes including health distress levels, self-reported health status and symptoms of hypoglycemia and hyperglycemia.31 Thom et al reported that participants who received peer coaching reduced mean levels of HbA1c from 10.14% at baseline to 8.98% at 6 months follow-up, compared with the usual care participants (baseline 9.84%, follow-up 9.55%).33 Safford et al39 reported that there was almost no reduction of HbA1c levels from baseline (HbA1c levels 8.0% vs 7.9%) to the 10 months follow-up in both the intervention (changes HbA1 −0.004) and control participants (HbA1c 0.070), however, the intervention was promising in improving secondary outcomes such as diabetes distress scores.39 A study in the USA which used bilingual peer leaders (known as ‘Promotoras’) found significant improvement in HbA1c levels from 8.21% at baseline to 7.76% at 6-month follow-up in the intervention arm compared with increment in HbA1c levels from 7.71% to 8.01% among the usual care participants.34
CHWs and primary care interventions
The interventions that used either CHWs or nurse practitioners also showed overall improvement in both primary and secondary outcomes. For example, Culica et al35 reported that patients who made all recommended health clinic visits in their study had HbA1c levels reduced from 8.14% at baseline to 7.00% at 12 months follow-up, compared with those patients who had partial health clinic visits. Two studies conducted among mostly African-American samples using CHWs found improvements in HbA1c levels.36 37 Intervention participants improved HbA1c level from 8.7% at baseline to 8.3% at 6-month follow-up compared with almost no changes in the usual care arm.36 Frosch et al37 reported that the intervention participants reduced HbA1c levels from 9.4% at baseline to 8.9% at 6-month follow-up and the usual care participants from 9.8% to 9.2%. Two studies which used multilingual link workers and diabetes nurse in the UK among South Asian migrants achieved moderate improvement in clinical and behavioral outcomes among the intervention patients compared with the controls.44 45 Islam et al43 using trained CHWs found intervention effectiveness in improving patient-centered outcomes (knowledge, physical activity and diet, etc) among Bangladeshi migrants with T2DM living in the USA. Lima et al,46 using general practices to provide diabetes self-management education found improvement of HbA1c levels from 8.89% at baseline to 8.19% at follow-up in intervention participants and usual care participants from 8.93% to 8.28%.
Combined peer support, CHW and telephone support interventions
Overall, the lifestyle interventions that used a combination of CHWs and peer supporters showed effectiveness in terms of improving both clinical and behavioural outcomes. Tsimikas et al32 reported significant improvement in HbA1c levels in the intervention arm at both 4-month and 10-month follow-ups compared with the usual care participants. At 4 months, the intervention participants reduced HbA1c levels from 10.5% at baseline to 9.0% and the reductions remained almost unchanged at the 10 months follow-up. The usual care participants also improved HbA1c levels from 10.3%, at baseline to 9.1%, at 4 months, however this increased to 9.7%, at 10 months. This intervention also improved other secondary outcomes including BP, BMI and body weight. Brown et al41 reported that HbA1c levels among the intervention participants reduced by 1.4% below the mean of the usual care participants; however, the mean level of HbA1c was still >10.0%.40 Another study by Brown et al41 found that extended interventions were equally effective in improving both primary and secondary outcomes among Mexican American adults with T2DM. These include HbA1c, fasting plasma glucose and knowledge about diabetes. However, Keyserling et al38 found almost no changes in HbA1c levels in both the intervention and control participants. See online supplemental table 3 file for details.
Supplemental material
Cost-effectiveness of the interventions
Most of the studies included in this review did not assess cost-effectiveness of the interventions or undertake cost-benefit analyses. Only five studies reported cost-related information. Lorig et al31 reported that the direct costs of the Spanish diabetes self-management program implemented over a 18-month period were approximately US$250 per participant over 18 months. The community-based diabetes education program by Culica et al35 50 reported that the cost per patient was US$461, which included the CHW salary, glucose monitors and testing strips, but excluded medication expenses. The glucose monitors and testing strips were the largest items of expenditure. A study by Brown et al41 estimated the general cost of an intervention that included health personnel and foods necessary for meal preparation.40 The cost of per person was estimated at US$384 for 12 months. In another study, Brown et al41 estimated the cost for compressed and extended versions of lifestyle interventions, reporting that the total cost per person for the former was US$131, whereas for the latter it was US$384 per person. These figures include cost of educational sessions, support group sessions and foods provided during the sessions. A study O’Hare et al44 conducted among South Asian migrants reported the cost of intervention per patient as GB£264 per year and staff cost GB£365 per patient with diabetes per year. Another study by Bellary et al45 implemented for a long term reported a cost of intervention per patient of GB£434 (GB£406 net service and GB£28 net prescribing costs) for the duration of 2 years. This study also reported the incremental cost-effectiveness ratio to GB£28 933 per quality-adjusted life year gained.
Discussion
In this review, we have presented a synthesis of evidence concerning interventions to support the management of diabetes using non-pharmacological, lifestyle change approaches among migrants and ethnic minorities residing in industrialized countries. The migrants and ethnic minorities were part of the interventions in this review included Hispanic population, African-Americans, Latinos-Americans, South Asians and Caucasians and Romanies. This systematic review found that lifestyle interventions delivered by CHWs or peer supporters (or a combination of these) can improve diabetes self-management among these priority subgroups, shown by modest effects on clinical and behavioural outcomes. We did not observe comparable difference in terms of intervention effectiveness among and between the subgroups who received either peer support or CHW-led or combination of these interventions. The evidence examined in this review suggests that lifestyle intervention programs delivered by CHWs or local volunteer or peer supporters or those with a bilingual background were effective.
The meta-analyses findings showed lifestyle interventions were moderately effective in reducing HbA1c levels among the migrants and ethnic minorities. These findings are comparable with recent systematic reviews and meta-analyses, which have found that lifestyle interventions using peer support have positive impacts on clinical outcomes such HbA1c levels, as well as diabetes self-management knowledge and practices. Patil et al included 17 studies published between 2000 and 2015 and reported that peer support interventions using lifestyle management approaches were effective in reducing HbA1c levels by 0.24% (95% CI 0.05% to 0.43%).51 52 Gatlin et al52 included seven studies in their review conducted between 2006 and 2016, and found that peer support intervention were effective in reducing HbA1c levels among peer education support groups compared with controls.51 Heterogeneity in terms of sample sizes, study design, intervention design and outcome measures were reported in both reviews. A systematic review by Rawal et al also reported that the lifestyle interventions implemented in low -resource settings were effective in improving glycemic control and behavioral outcomes.20 Conversely, a recent systematic review by Navodia et al, which included four studies conducted among South Asian migrants residing in industrialized countries reported that the culturally appropriate diabetes self-management programs did not show statistically significant outcomes in reducing HbA1c levels.53
Our review also showed that lifestyle interventions using CHWs were effective in improving both primary and secondary outcomes.34 35 37 46 Previous reviews have shown similar findings.19 54–57 Palmas et al57 in their systematic review showed that the CHW interventions were effective in bringing modest reduction in HbA1c (of 0.21%, 95 % CI 0.11 to 0.32) compared with the usual care patients. The reduction in HbA1c was found to be larger in studies in which participants had higher mean baseline HbA1c levels. Evidence suggests that because CHWs have in-depth knowledge of their community they are able to provide culturally appropriate services to communities that are medically underserved.56 However, the roles of CHWs and outcomes achieved can vary greatly, making it difficult to draw conclusions about their overall effectiveness in T2DM interventions. Studies that involved CHWs providing regular telephone support to patients with T2DM have shown positive changes in clinical and behavioral outcomes.58 59 These programs have included CHW coaching, peer support as well as the regular telephone calls, implemented in different low-resource settings and reported positive impacts on T2DM self-management. Furthermore, a systematic review by Vas et al54 found that lifestyle interventions were effective in improving diabetes self‐management, resulting in reductions in HbA1c, improved diabetes knowledge and self‐care practices. A systematic review by Henderson et al,55 which included 16 studies suggested that use of bilingual CHWs in culturally and linguistically diverse communities may promote greater uptake of NCD prevention and management programs.
In our review, we endeavoured to systematically assess the cost-effectiveness of the lifestyle interventions implemented among migrants and ethnic minorities. No study reported cost-effectiveness data. While only a few studies reported cost-related information in their interventions,31 35 40 41 50 the evidence suggests that lowering blood sugar levels among those people with diabetes has significant benefits in reducing the healthcare cost.60 61
Limitation
This review focused on assessing the effectiveness of lifestyle interventions for management of T2DM with HbA1c and other biochemical measures as key outcomes but did not include primary prevention interventions. Some primary as well as secondary outcomes to T2DM management such as duration of diabetes, number of patients on oral antidiabetic agents, history of smoking or alcohol, etc are not reported in this review. Another limitation may be bias related to inclusion of studies that were only published in English. While the language, cultural values, background of the participants and access to services/resources, etc may have significant influence on intervention utilisation and impact, where available, we have therefore reported this information narratively. However, the level of detail provided varies across the included studies and we were unable to quantitatively stratify the findings according to these factors. The generalizability of the findings is also limited as the significant heterogeneity of the study population included in these studies was observed in addition to implementation occurring in a limited number of industrialised countries.
Conclusions
The global estimates show that the rate of migration, particularly from the LMICs to high-income countries, is increasing substantially. The majority of those from migrant and ethnic minorities backgrounds are likely to develop NCDs in their lifetime. Furthermore, there is substantial evidence that migrants and ethnic minorities suffer additional barriers to optimal care, putting them at even greater risk for costly diseases and associated complications. The evidence presented in this review is encouraging as most of the studies using either CHW, peer supporters or a combination of the both have shown improvements in the management of T2DM. There is great potential for developing culturally and linguistically appropriate, clinically sound and cost-effective interventions to respond to the growing and diverse migrant and ethnic minority populations affected by diabetes worldwide.
Data availability statement
Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as supplemental information. Data are available in a public, open access repository.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors LR, BWS, BJS, KK and AMNR contributed conceptualizing the study, drafting the manuscript and finalization. LR, BWS and AMNR contributed in data search, assessment, analyses and results write up. BJS, KK, EO-A and AMNR thoroughly reviewed the manuscript and contributed substantially for necessary revision. LR, BWS, BJS, KK, EO-A and AMNR finally reviewed the manuscript and prepared for submission.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.