Article Text

Abstract
Introduction The treatment of diabetes has a significant impact on the pathogenesis of non-alcoholic fatty liver disease (NAFLD). We compared the effectiveness of tofogliflozin, a selective sodium-glucose cotransporter 2 inhibitor, and pioglitazone for the treatment of NAFLD patients with type 2 diabetes mellitus.
Research design and methods This open-label, prospective, single-center, randomized clinical trial recruited NAFLD patients with type 2 diabetes mellitus and a hepatic fat fraction of at least 10% as assessed based on the MRI-proton density fat fraction (MRI-PDFF). Eligible patients were stratified according to hemoglobin A1c (HbA1c), alanine transaminase, and MRI-PDFF levels and randomly assigned (1:1) to receive either 20 mg tofogliflozin or 15–30 mg pioglitazone, orally, once daily for 24 weeks. The primary endpoint was an absolute change in MRI-PDFF at 24 weeks. Efficacy and safety was assessed in all treated patients. This trial was registered in the Japan Registry of Clinical Trials.
Results Overall, 40 eligible patients were randomly assigned to receive tofogliflozin (n=21) or pioglitazone (n=19). Changes in hepatic steatosis after 24 weeks of treatment were evaluated by MRI-PDFF, which showed a significant decrease in both groups (−7.54% (p<0.0001) and −4.12% (p=0.0042) in the pioglitazone and tofogliflozin groups, respectively). Compared with baseline, the body weight decreased by 2.83±2.86 kg (−3.6%, p=0.0443) in the tofogliflozin group and increased by 1.39±2.62 kg (1.7%, p=0.0002) in the pioglitazone group after 24 weeks. No life-threatening events or treatment-related deaths occurred.
Conclusions Tofogliflozin was well tolerated, and it reduced the MRI-PDFF levels in NAFLD patients with type 2 diabetes mellitus.
Trial registration number jRCTs031180159.
- diabetes mellitus
- type 2
- non-alcoholic fatty liver disease
- pharmacology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Pioglitazone is the gold-standard pharmacotherapy for non-alcoholic steatohepatitis patients with type 2 diabetes mellitus (T2DM) based on current guidelines.
Sodium-glucose cotransporter 2 (SGLT2) inhibitors have become candidate therapeutic agents for non-alcoholic fatty liver disease (NAFLD) patients with diabetes mellitus.
What are the new findings?
This randomized prospective open-label controlled trial is the first report to investigate the efficacy of tofogliflozin in NAFLD patients with T2DM.
Treatment with tofogliflozin for 24 weeks was effective in improving hepatic steatosis to low-dose pioglitazone without statistical significance.
Pioglitazone significantly improved MR elastography-liver stiffness measurement (MRE-LSM), whereas tofogliflozin did not decrease MRE-LSM during the 24-week treatment.
How might these results change the focus of research or clinical practice?
SGLT2 inhibitors including tofogliflozin can be potential candidates for treatment of patients with NAFLD with T2DM as they can simultaneously improve hyperglycemia and decrease body weight efficiently.
Introduction
Non-alcoholic fatty liver disease (NAFLD) is the most common liver disease, with a prevalence rate of 25.2% globally and 29.6% in Asia.1 2 NAFLD is a reflection of adipose tissue dysfunction and insulin resistance and is associated with other risk factors for metabolic syndrome.1 3–6 NAFLD is associated with worse insulin resistance and worse glucose tolerance.7 NAFLD is both a liver-specific disease and an early mediator of several diseases. The prevalence of comorbidities associated with NAFLD has been reported to be 51%, 23%, 69%, 39%, and 43% for obesity, type 2 diabetes mellitus, hyperlipidemia, hypertension, and metabolic syndrome, respectively.1 It is also an independent risk factor for cardiovascular events closely associated with the life expectancy of patients with diabetes.8 Metabolic disorders such as lipid accumulation, insulin resistance, and inflammation have been implicated in the pathogenesis of NAFLD, but the underlying mechanisms, including those that drive disease progression, are not fully understood.9 10
There are several types of antidiabetic drugs: insulin sensitizers (metformin and pioglitazone), insulin secretagogues (sulfonylureas, dipeotidyl peptidase-4 inhibitors, and glucagon-like peptide-1 (GLP-1) receptor agonists), and glucose absorption and secretion modulators (alpha-glucosidase inhibitors and sodium-glucose cotransporter 2 (SGLT2) inhibitors). Insulin therapy and sulfonylureas are not considered effective in NAFLD activity or fibrosis; therefore, they have not been carefully studied.11 In the USA, metformin is recommended as a first-line drug for diabetes,12 but metformin-induced histological improvement of NAFLD has not been demonstrated.10 Pioglitazone is the gold-standard pharmacotherapy for patients with type 2 diabetes mellitus and non-alcoholic steatohepatitis (NASH) based on current guidelines (eg, Japanese Society of Gastroenterology 201513; EASL-EASO-EASD 20169; and AASLD 201810). Several large-scale randomized controlled trials have reported the effectiveness of pioglitazone in treating NASH14–17; it has also been shown to improve markers of hepatic steatosis and fibrosis on liver histology.10 17 However, pioglitazone should be used with caution in patients with severe obesity, diastolic dysfunction, congestive heat failure, edema, or history of osteoporosis or bladder cancer.18
SGLT2 inhibitors prevent glucose reabsorption in the proximal tubule, thereby leading to glucosuria and plasma glucose reduction. SGLT2 inhibitors also have cardio-protective or renal-protective effects19 and are being actively investigated for their therapeutic effects in NAFLD with type 2 diabetes mellitus. Several randomized, double-blind, placebo-controlled trials have investigated the effects of SGLT2 inhibitors such as empaglifozin,20 dapaglifozin,21 22 and canagliflozin23 in NAFLD patients with type 2 diabetes mellitus. For ipragliflozin and luseogliflozin, effectiveness has also been reported in a small number of open-label studies.24 25 To the best of our knowledge, however, no retrospective study or prospective trial has investigated the efficacy of tofogliflozin in NAFLD patients with type 2 diabetes mellitus.
In the present study, we compared the effectiveness of tofogliflozin and pioglitazone for the treatment of NAFLD patients with type 2 diabetes mellitus (ToPiND study). The efficacy of these drugs in improving hepatic steatosis was assessed by biochemical tests and MRI for estimating the proton density of the fat fraction (PDFF) of the liver, as this is the most reliable technique for steatosis quantification.20–22 26 We additionally evaluated liver fibrosis by assessing the expression of hepatic fibrosis markers and measuring liver stiffness by MR elastography-liver stiffness measurement (MRE-LSM). We also evaluated other metabolic and oxidative stress factors and compared the safety of tofogliflozin with that of pioglitazone for treating NAFLD patients with diabetes.
Research design and methods
Study design and patients
This open-label, prospective, single-center, randomized study compared the effectiveness of tofogliflozin and pioglitazone in treating hepatic steatosis in patients with NAFLD and type 2 diabetes mellitus, over 24 weeks.27 The study protocol complied with the principles of the Declaration of Helsinki and the Ethics Guidelines for Clinical Research published by the Ministry of Health, Labour, and Welfare of Japan. This trial was registered in the Japan Registry of Clinical Trials. The trial results have been reported in accordance with the Consolidated Standards of Reporting Trials 2010 guidelines.
Adult patients with NAFLD and type 2 diabetes mellitus (age range: 20–74 years) with hemoglobin A1c (HbA1c) ≥6.5% (48 mmol/mol) and alanine transaminase (ALT) levels beyond the institutional standard level (42 IU/L for men and 23 IU/L for women), who had undergone diet and exercise therapies for ≥12 weeks, were enrolled. Details of the inclusion and exclusion criteria are shown in online supplemental table S1. The use of other SGLT2 inhibitors, thiazolidinedione, insulin, and GLP-1 receptor agonists was prohibited during the observation period. Use of vitamin E was also prohibited during the randomization period, as it is an antioxidant, and has been recommended by several guidelines for treating nondiabetic adults with NASH.9 10 13 In principle, changes in the medication for diabetes mellitus, including adding, discontinuing, or changing the dosage, were not allowed throughout the study period. Patients were treated with either tofogliflozin 20 mg or pioglitazone 15–30 mg once a day for 24 weeks.
Supplemental material
The flow chart of the study is shown in online supplemental figure S1. The study recruited 40 adult patients from the Yokohama City University Hospital. All patients provided written informed consent before participation in the study.
Randomization
The patients underwent screening to ensure that they fulfilled the inclusion criteria and did not meet any of the exclusion criteria (online supplemental table S1). The principal investigator or coinvestigator completed the patient enrollment form for eligible patients (primary registration), following which, patients with ≥10% liver fat content on MRI-PDFF were randomly assigned to the tofogliflozin or pioglitazone group, stratified by HbA1c levels (<7% and ≥7.0%), ALT levels (<50 IU/L and ≥50 IU/L), and MRI-PDFF values (<20% and ≥20%) (definitive registration). Eligible patients were randomly assigned equally (1:1) to receive 20 mg tofogliflozin or 15–30 mg pioglitazone orally once daily. Randomization was performed using a computer-generated, centrally administered procedure and a minimization method. Patients were allocated to each treatment group through the central registration system; both the physician and patient were aware of the allocated treatment. To confirm adherence to the treatment regimen, the investigator or coinvestigator questioned patients at each visit on medication adherence.
Procedures
After randomization, patients were examined at weeks 0 (the day before the first drug dose), 12, and 24, after having fasted for at least 8 hours. The diet was standardized according to the comprehensive lifestyle approach per guidelines.9 MRI-PDFF and MRE-LSM were performed at baseline and 24 weeks after treatment, and MRI-PDFF results were interpreted by an independent blinded liver specialist (KI) according to the method reported previously.28 MRI was performed using standardized instruments at high field strength (Discovery MR750 3.0T, GE Healthcare, Japan), without oral or intravenous contrast. Physical examination and blood tests were performed before and at 12 and 24 weeks after drug administration.
Outcomes
The primary endpoint was change in hepatic steatosis evaluated using MRI-PDFF at 24 weeks; this was compared between patients treated with tofogliflozin and pioglitazone. The key secondary endpoint was change in ALT levels at 24 weeks after drug administration. Other secondary endpoints included adverse events (AEs), results of standard laboratory analysis, physical examination, and vital signs. Patients were examined at weeks 0, 12, and 24 during the treatment. Body weight and body mass index (BMI) were measured at screening and at weeks 0, 12, and 24. Fasting liver enzymes, the lipid panel (ie, total cholesterol, low-density lipoprotein cholesterol, triglycerides, and high-density lipoprotein (HDL) cholesterol), diabetes markers (ie, fasting blood sugar, HbA1c), and uric acid levels were measured at the Yokohama City University Hospital laboratory at weeks 0 and 24. Fibrosis markers (type IV collagen 7S and Wisteria floribunda agglutinin-positive Mac-2 binding protein (WFA-M2BP) glycosylation isomer), high sensitivity C reactive protein, and Uric 8-OHdG, which is one of the major forms of DNA damage induced by reactive oxygen species, adiponectin, and ketone body fraction (acetoacetic acid and 3-hydroxybutyric acid), were measured by a local laboratory (SRL, Tokyo, Japan) at weeks 0 and 24. The scoring system (Fibrosis-4 (FIB-4)) for fibrosis markers was calculated in post hoc analyses (online supplemental table S2).
Adverse events
All AEs that occurred during the study were recorded in a case report form, which included information regarding the symptom/disease, its onset and end date, severity and seriousness, investigator’s opinion of the association with tofogliflozin/pioglitazone treatment, action taken regarding tofogliflozin/pioglitazone usage and AE treatment, cause of the event, and resolution/outcome. AEs were followed-up until they were normalized or achieving normalization. In cases where the AE was irreversible, it was followed-up until the symptoms were stable. If the investigator or co-investigator judged the AE as recovered or considered it to have no association with the study outcomes, it was not followed-up similarly, and the reasons were mentioned in the medical records.
Criteria for discontinuation of treatment
Treatment was discontinued if the HbA1c level increased by >1.0% after initiation of medication, aspartate transaminase (AST) or ALT increased by >3 fold of that before medication, the patient became ineligible for the trial, medication compliance was <75%, continuous medical examination became challenging due to severe AEs, and in case of pregnancy. Treatment was also discontinued if the participant requested discontinuation, use of medication had to be combined with prohibited medicine because of deterioration of the primary disease or its complications, or if the doctor decided that discontinuation was appropriate for other reasons.
Gene test
The investigators collected the blood samples at any time from definitive registration to 48 weeks after the treatment regimen to confirm genetic polymorphisms of PNPLA3 and TM6SF29 by real-time PCR.
Statistical analyses
Sample size calculation was performed to ensure satisfactory power for the analysis of variance F-test. Assuming the mean change in MRI-PDFF in the tofogliflozin and pioglitazone groups to be −4.9% and −6.7%, respectively,29 with a common SD of 2.0, the required minimum number of patients per group with a power of 80% and a two-sided significance level of 5% was calculated to be 20. Per protocol set (PPS) analyses were performed to evaluate the primary and secondary endpoints. The full analysis set (FAS) used the intention-to-treat population; the analysis included patients who had been registered in this study and assigned to the drug group. Those with serious violations of the research plan (eg, not obtaining consent and registration date beyond the registration period) were excluded. During PPS analysis, we excluded patients with serious violations of inclusion and exclusion criteria, patients using prohibited drugs, and those with a compliance rate of >120% or<75% from the FAS population. The data of the remaining patients were analyzed.
The patients who had registered in the study, started treatment as assigned, and undergone part of or all treatment comprised the target population for safety analysis. The statistical significance of the change between the groups was evaluated for the endpoints. The null hypothesis was an equal change in liver fat content in both groups. This was tested using analysis of covariance by defining the groups as fixed effects and stratified factors (HbA1c, ALT, and MRI-PDFF) as covariates. Additionally, descriptive statistics (number of cases, average value, SD, minimum value, median value, and maximum value) of changes at 24 weeks of medication were calculated. The two-sided level of significance was set at 5%.
Medical statisticians developed a statistical analysis plan and specified the details of statistical methods to be used for data handling. The plan was prepared before data collection.
Furthermore, the frequencies of the genotypes and alleles were compared between the groups in three different modes using the χ2 test. In the genotype mode, the differences in genotype were compared between cases and controls using a 3×2 contingency table. In the allele frequency mode, allele frequencies were compared between cases and controls using a 2×2 contingency table. JMP Pro version 15.0 was used for performing all analyses.
Results
Patient baseline characteristics
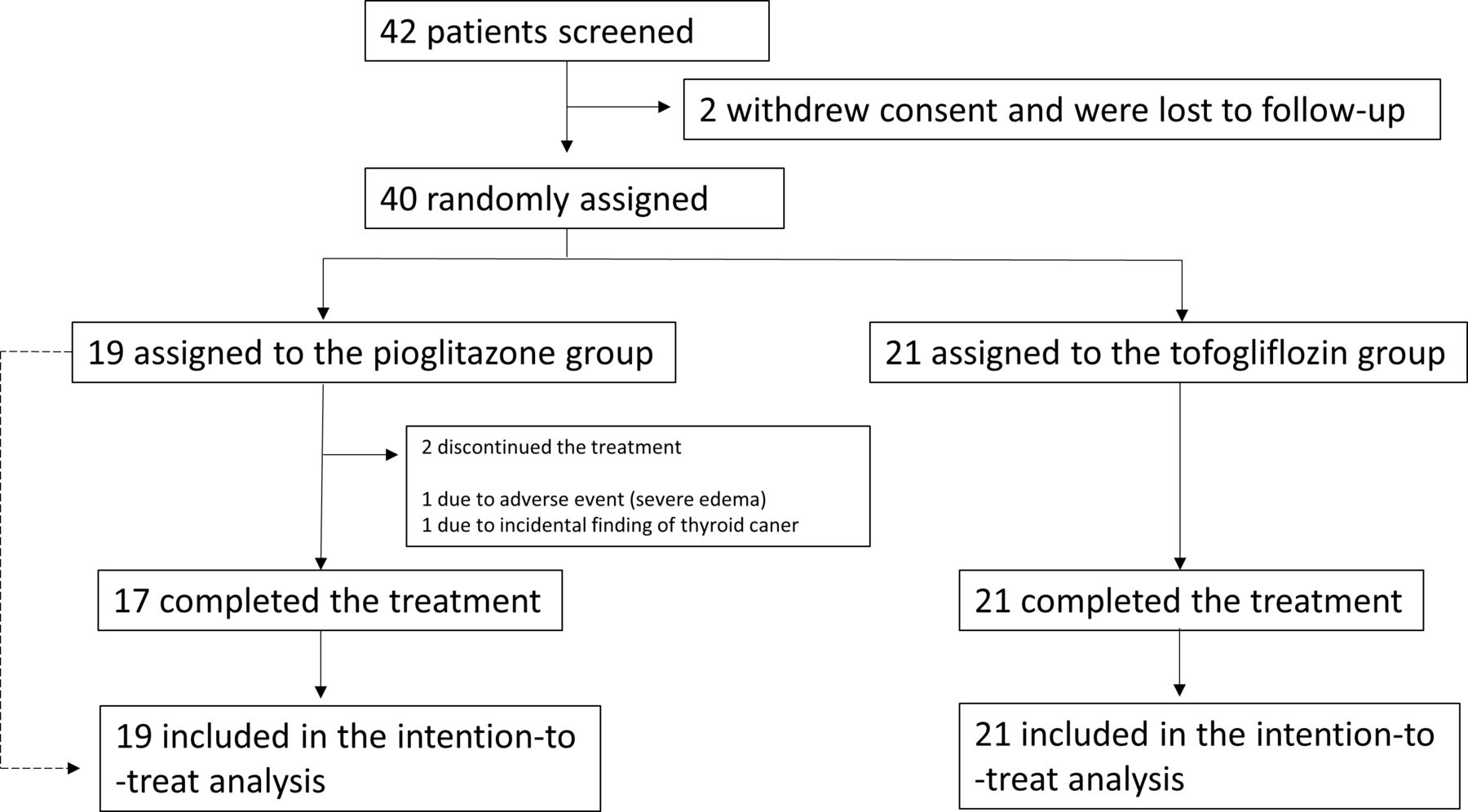
Between 30 March 2018 and 13 December 2019, 42 patients were screened, and 40 eligible patients were randomly assigned to receive tofogliflozin 20 mg (n=21) or pioglitazone 15–30 mg (n=19). Figure 1 shows the outline of the trial; 38 patients completed the trial (tofogliflozin group: n=21; pioglitazone group: n=17). In pioglitazone group, 15 out of 17 received pioglitazone 15 mg and the other two received pioglitazone 30 mg. The mean dose of pioglitazone at 24 weeks was 16.8 mg/day. Adherence in those who completed the trial was 100% in both the pioglitazone and tofogliflozin groups. Table 1 shows the demographic and baseline characteristics of the participants. The mean age was 58.6±10.3 years, mean HbA1c was 7.1%±0.77%, and mean BMI was 30.0±4.76 kg/m2.
Baseline characteristics of the intention-to-treat population
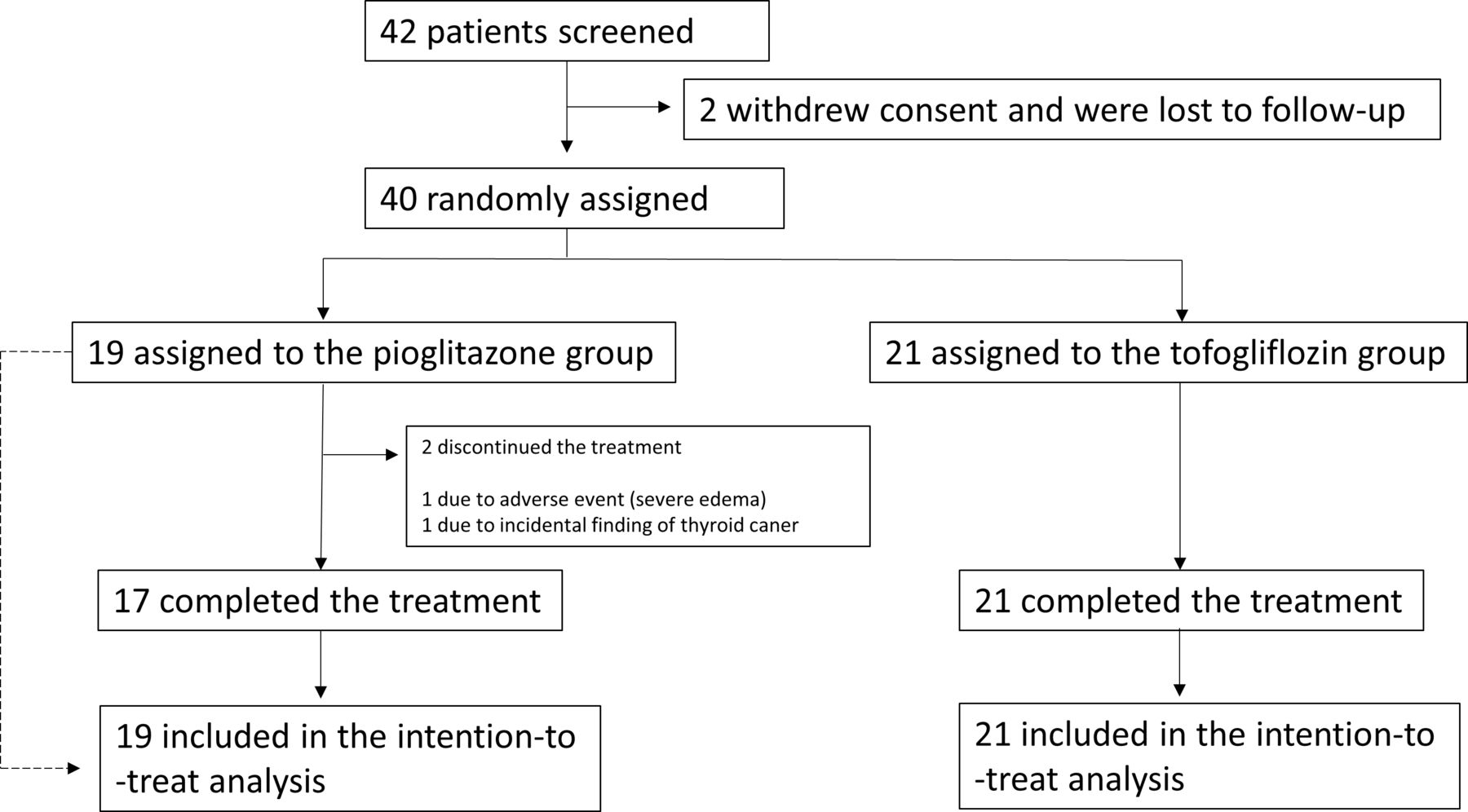
Outline of the trial.
Changes in MRI-PDFF and liver tests
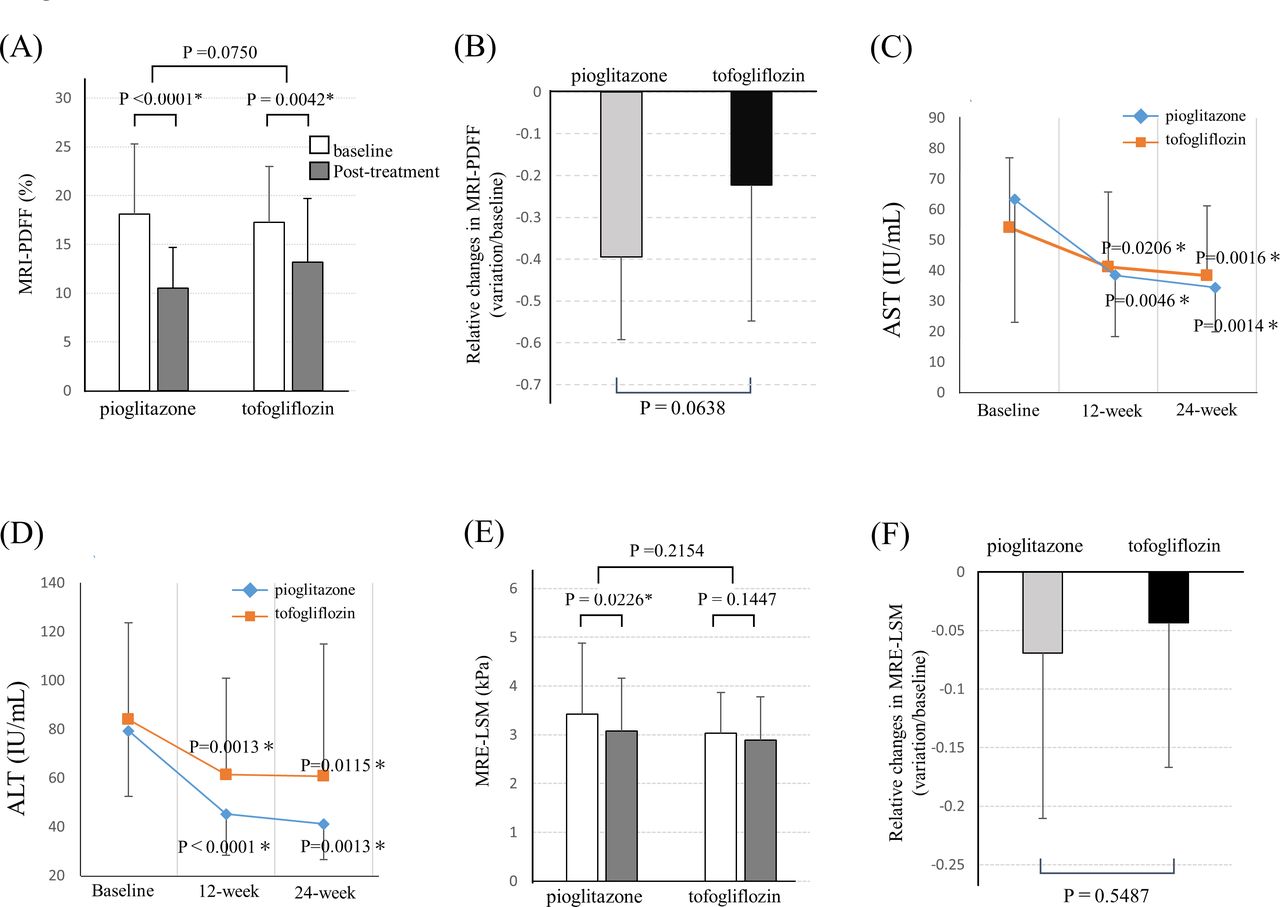
Changes in hepatic steatosis after 24 weeks of pioglitazone and tofogliflozin treatment were evaluated using MRI-PDFF, which decreased significantly by 7.54% (p<0.0001) and 4.12% (p=0.0042) in the pioglitazone and tofogliflozin groups, respectively (figure 2A). No significant differences were observed between the groups with respect to relative change (variation/baseline) (p=0.0638) (figure 2B). Additionally, the level of ALT showed a significant reduction at 24 weeks compared with that at baseline by −33.8 IU/mL (p<0.0001) and −23.3 IU/mL (p=0.0115) in the pioglitazone and tofogliflozin groups, respectively (figure 2C). The level of AST also showed a significant reduction at 24 weeks compared with that at baseline by −27.9 IU/mL (p=0.0014) and −15.7 IU/mL (p=0.0016) in the pioglitazone and tofogliflozin groups, respectively (figure 2D). No significant differences of AST and ALT were observed between the groups. Similarly, γ-glutamyl transpeptidase (GGT) levels improved significantly in both groups, and the difference was not significant between the groups (p=0.1244). Alkaline phosphatase levels decreased significantly in the pioglitazone group but not in the tofogliflozin group (p=0.0389, table 2).
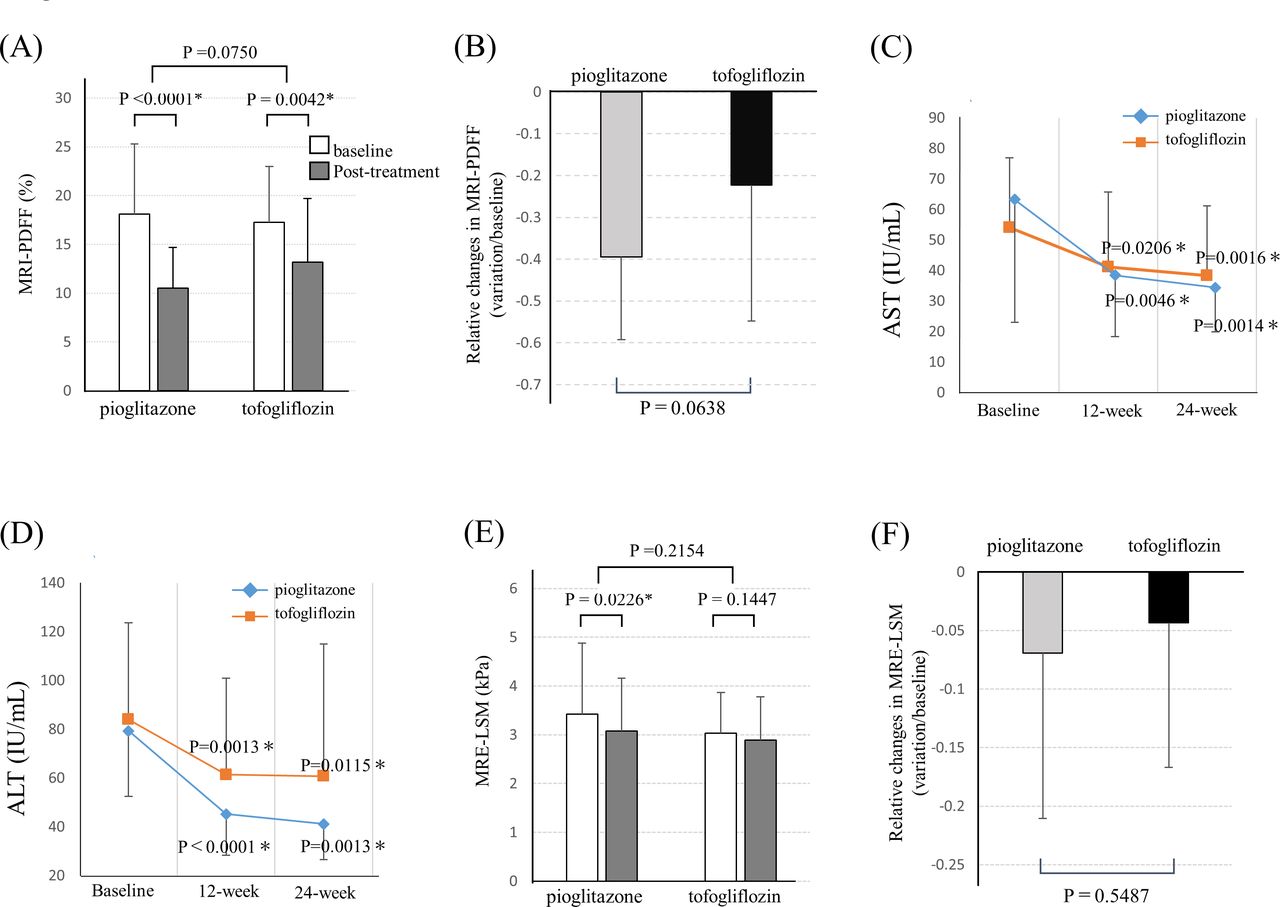
(A) Baseline and post-treatment changes in liver fat at 24 weeks in the pioglitazone and tofogliflozin groups assessed by MRI-PDFF. (B) Relative changes in MRI-PDFF (variation/baseline) in the pioglitazone and tofogliflozin groups. (C) Changes in aspartate aminotransferase (AST) over time in the pioglitazone and tofogliflozin groups. (D) Changes in alanine transaminase (ALT) over time in the pioglitazone and tofogliflozin groups. (E) Baseline and post-treatment changes in liver fat at 24 weeks in the pioglitazone and tofogliflozin groups assessed by MRE-LSM. (F) Relative changes in MRE-LSM (variation/baseline) in the pioglitazone and tofogliflozin groups. LSM, liver stiffness measurement; MRE, magnetic resonance elastography; MRI-PDFF, MRI for estimating the proton density of the fat fraction of the liver.
Changes in factors from baseline to 24 weeks in the pioglitazone and tofogliflozin groups
Changes in liver fibrosis indicators
Changes in liver stiffness after 24 weeks of pioglitazone and tofogliflozin treatment were evaluated using MRE-LSM, which showed a reduction of 0.34 kPa (p=0.0443) and 0.14 kPa (p=0.1447) in the pioglitazone and tofogliflozin groups, respectively. Although MRE-LSM decreased in both groups, the change was significant only in the pioglitazone group. No significant difference was observed at 24 weeks of treatment between the groups (p=0.2154) (figure 2E,F). Furthermore, there were no significant differences in the FIB-4 index and type IV collagen 7S between baseline and post-treatment in both groups (FIB-4 index: p=0.1595 and p=0.1483 in the pioglitazone and tofogliflozin groups, respectively; type IV collagen 7S: p=0.8480 and p=0.2577 in the pioglitazone and tofogliflozin groups, respectively). A significant decrease in WFA+-M2BP was observed at 24 weeks compared with that at baseline in both treatment groups (p=0.0092 and p=0.0130 in the pioglitazone and tofogliflozin groups, respectively, table 2).
Changes in glycemic and metabolic parameters
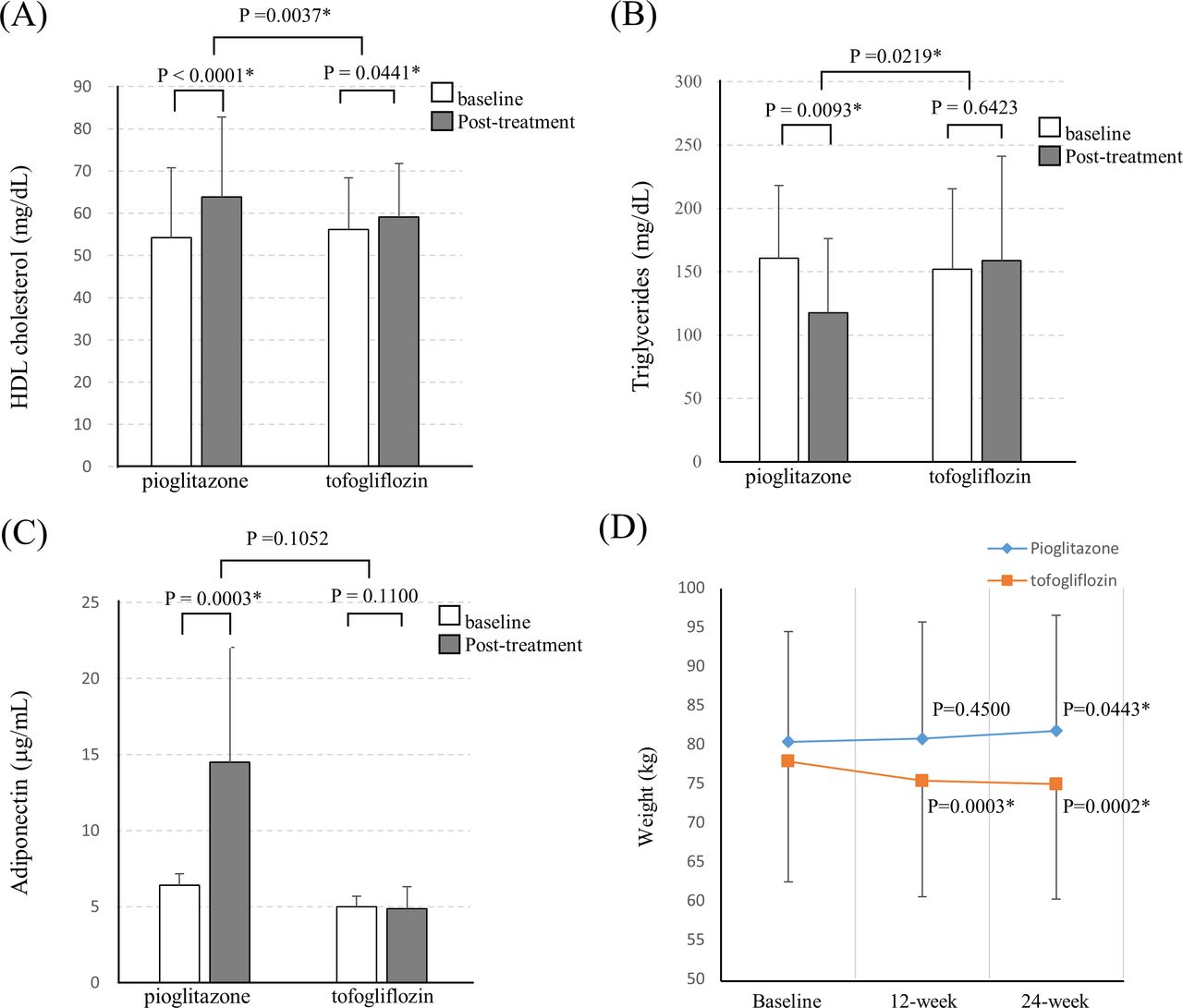
HbA1c improved significantly in both groups (p=0.0003 and p=0.0013 in the pioglitazone and tofogliflozin groups, respectively), and the difference was not significant between the groups (p=0.1052) (table 2). Additionally, HDL increased significantly by 9.7 mg/dL (p<0.0001) and 2.9 mg/dL (p=0.0441) in the pioglitazone and tofogliflozin groups, respectively, at the end of 24 weeks. Significant elevation was observed in the pioglitazone group compared with the tofogliflozin group (p=0.0037) (table 2, figure 3A). Triglyceride levels decreased significantly in the pioglitazone group (p=0.0093) but not in the tofogliflozin group (p=0.6423). There was a significant difference in treatment effect between the groups at 24 weeks (p=0.0219) (table 2, figure 3B). Uric acid levels decreased significantly in the tofogliflozin group (p=0.0004) but not in the pioglitazone group (p=0.2459). The difference was significant between the groups (p=0.0336) (table 2).
{kind=link}
{kind=link}
{kind=link}
(A) Baseline and post-treatment changes in HDL cholesterol at 24 weeks in the pioglitazone and tofogliflozin groups. (B) Baseline and post-treatment changes in triglycerides at 24 weeks in the pioglitazone and tofogliflozin groups. (C) Baseline and post-treatment changes in adiponectin at 24 weeks in the pioglitazone and tofogliflozin groups. (D) Changes in weight over time (baseline, 12 weeks and post-treatment (24 weeks)) in the pioglitazone and tofogliflozin groups. HDL, high-density lipoprotein.
Changes in oxidative stress, adiponectin, CK-18 fragment, and pro-ketogenic markers
The urine 8-OHdG level decreased significantly in the tofogliflozin group (p=0.0005) but not in the pioglitazone group (p=0.1138). The difference between the groups was not significant at 24 weeks (p=0.2058) (table 2). Adiponectin, a key adipocytokine in metabolic syndrome, increased significantly in the pioglitazone group (p=0.0003) but not in the tofogliflozin group (p=0.1100), and the change was significant between the groups (p<0.0001) (table 2, figure 3D). The CK-18 fragment M30 antigen, which correlates with the magnitude of hepatocyte apoptosis and independently predicts the presence of NASH, decreased significantly in both groups (p=0.0007 and p=0.0048 for the tofogliflozin and pioglitazone groups, respectively), but the difference was not significant between the groups (p=0.2345) (table 2).
The ketone bodies, acetoacetate, and 3-hydroxybutyrate increased significantly in the tofogliflozin group (acetoacetic acid: p=0.0363; 3-hydroxybutyrate: p=0.0308) but did not change in the pioglitazone group, and the difference between the groups was not significant (table 2).
Adverse events
There was a case of severe edema and an unexpected discovery of thyroid cancer (12 and 8 weeks after starting pioglitazone, respectively) in the pioglitazone group. AEs such as edema and/or weight gain of ≥3% occurred in 31.6% (6/19) of patients in the pioglitazone group, whereas only one case of urinary tract infection (4.8%) was observed in the tofogliflozin group (online supplemental table S3). One patient in the pioglitazone group discontinued treatment because of severe edema. No life-threatening events or treatment-related deaths occurred during the study in either group.
Compared with the baseline, the body weight decreased significantly by 2.83±2.86 kg (−3.6% from baseline) in the tofogliflozin group (p=0.0002) and increased significantly by 1.39±2.62 kg (1.7%) in the pioglitazone group after 24 weeks of treatment (p=0.0443) (figure 3D); the change was significant between the groups (p<0.0001)
PNPLA3 and TM6SF2 analysis
PNPLA3 genotyping was performed in the pioglitazone group (CC (n=2), CG (n=8), and GG (n=7)) and tofogliflozin group (CC (n=5), CG (n=8), and GG (n=8)). There was no difference in both, the genotype and allele frequency of PNPLA3 between the groups.
TM6SF2 genotyping was performed in the pioglitazone (CC (n=14), CT (n=3), and TT (n=0)) and tofogliflozin groups (CC (n=17), CG (n=3), and GG (n=1)). There was no difference in the genotype of TM6SF2 between the groups. Furthermore, no significant differences in the efficacy of treatment were observed in both groups after stratification based on PNPLA3 and TM6SF2 genotypes (data not shown).
Discussion
To our knowledge, this is the first study to investigate the effect of tofogliflozin on hepatic steatosis in NAFLD patients with type 2 diabetes mellitus. We found that both tofogliflozin and pioglitazone improved the primary endpoint (absolute change in MRI-PDFF), key secondary endpoint (absolute change in ALT level) and several other parameters after 24 weeks of treatment. This is an open-label design that involves an implicit bias by investigators as the focus of the study was on tofogliflozin. Open-label design could have contributed, for example, for the weight loss observed in that group which appears somewhat larger than with others of the class.18
Whereas pioglitazone is the only established diabetic medicine incorporated into treatment guidelines for NASH.9 10 13 SGLT2 inhibitors are a relatively new class of antidiabetic drugs that could play a potential role in the treatment of NASH.18 30 We used the SGLT2 inhibitor tofogliflozin; its half-life of 5.4 hours is much shorter than that of other SGLT2 inhibitors, such as ipragliflozin (14.97 hours), luseogliflozin (11.2 hours), empaglifozin (9.88 hours), dapaglifozin (12.1 hours), and canagliflozin (10.2 hours). The shorter half-life leads to quicker effects and less nocturnal side effects, such as hypoglycemia.31
The primary endpoint analysis demonstrated that both, tofogliflozin and pioglitazone, treatments improved hepatic steatosis in NAFLD patients, based on MRI-PDFF. PDFF, which is the fraction of MRI-visible protons bound to fat divided by all protons in the liver (bound to fat and water), is now considered to be the highest quality imaging technique for evaluating hepatic steatosis,28 32 and MRI-PDFF changes have been associated with changes in histological steatosis.33 In previous studies, which investigated the effect of SGLT2 inhibitors in NAFLD patients, the liver to spleen ratio on CT was used for evaluating hepatic steatosis in the open-label trial,24 and several recent placebo-controlled RCTs used MRI-PDFF for evaluating the effect of SGLT2 inhibitors on hepatic steatosis.20–22 The ALT level, the key secondary endpoint decreased in both treatment groups at a comparable level. In previous reports, the reduction in liver fat with pioglitazone 45 mg/day is about 60%,14 17 while that of SGLT2 inhibitors is 15%–20%.18 In this study, there was no statistically significant difference between low-dose pioglitazone and tofogliflozin group in the PDFF and ALT studies, but pioglitazone group tended to be more effective in hepatic steatosis. It must also be considered that the lack of statistically significant differences may be due to the small sample size. Furthermore, we evaluated the effects of tofogliflozin and pioglitazone on liver stiffness using MRE, which is currently considered the most accurate non-invasive imaging method for the diagnosis of liver fibrosis.28 34 35 To our knowledge, this is the first study to evaluate the therapeutic effect of SGLT2 inhibitors on hepatic stiffness using MRE. Pioglitazone significantly improved MRE-LSM, whereas tofogliflozin did not decrease MRE-LSM during the 24-week treatment. Previous reports and the results of this study suggest that pioglitazone may be more effective in improving fibrosis. Due to the short duration of this study, the variation in MRE values may have been influenced by the changes fibrosis as well as steatosis and inflammation. CK-18 fragments, which are involved in the inflammatory response and apoptosis in NAFLD patients,36 also showed a comparable ameliorative effect in both groups. Hepatic fibrosis was also evaluated by estimating fibrosis markers, including type IV collagen 7S and WFA+-M2BP. Both markers are clinically used for assessing the degree of liver fibrosis in NAFLD patients.37 38 No significant difference was observed in the level of type IV collagen 7S in both groups, whereas a significant decrease in WFA+-M2BP was observed in both groups. It is possible that WFA+-M2BP, rather than type IV collagen 7S, reflected minor changes in fibrosis. Long-term testing is necessary when evaluating improvements in liver fibrosis.
Furthermore, both drugs showed a diabetes-ameliorating effect, and there was no change between the groups. Pioglitazone treatment elevated the levels of adiponectin and HDL and lowered the level of triglycerides significantly compared with the tofogliflozin group; this may have been due to changes in adiponectin levels.39 This study reconfirmed that pioglitazone-treated patients clearly had a lowering of triglycerides, an increase in HDL, and an increase in adiponectin. These are important factors in the previously reported cardiovascular disease (CVD)-preventive effect of pioglitazone.40 Uric acid levels were reduced only in the tofogliflozin group; SGLT2 inhibitors have a uric acid lowering effect and have been reported to cause gout less frequently than other antidiabetic drugs.41
Furthermore, tofogliflozin treatment caused an increase in acetoacetic acid and 3-hydroxybutyric acid levels that were not observed with pioglitazone treatment. SGLT2 inhibitors have been reported to cause a high degree of glucosuria and calorie loss, releasing glucagon from the alpha cells of the pancreas; this exerts a positive alterative effect on the myocardium, thereby effectively improving heart failure.42 The production of 3-hydroxybutyric acid, a type of ketone body from the liver, increases with an increase in glucagon and a decrease in the insulin/glucagon ratio. Under conditions of mild persistent hyperketonemia, such as during treatment with SGLT2 inhibitors, 3-hydroxybutyric acid is freely taken up by the heart (among other organs) and oxidized in preference to fatty acids.43 Given the suboptimal glycemic and cardiovascular risk control in type 2 diabetes, novel therapies such as SGLT2 inhibitors seem to offer an important clinical advantage in improving glycemic control and cardiovascular44 and renal outcomes.45
The noteworthy aspect of this clinical study is the frequency of AEs and adverse drug reactions in particular. The most common AEs of pioglitazone are pedal edema and weight gain.18 One person in the pioglitazone group discontinued treatment after 3 months due to severe edema, which improved promptly after stopping the treatment. Inverse changes in body weight were observed in the pioglitazone and tofogliflozin groups. It should be noted however that weight gain with pioglitazone has opposite metabolic effects compared with weight gain by excess caloric intake, being associated with a reduction in visceral fat46 and improvement in insulin sensitivity, atherogenic dyslipidemia, NASH, and risk of type 2 diabetes mellitus and CVD.6 SGLT2 inhibitors are known to exert blood glucose lowering and body weight lowering effects. They have also been reported to demonstrate pleiotropic effects on various complications and regulatory effects on macrovascular events47 in addition to beneficial effects on hepatic dysfunction in both clinical trials and animal models.48 Combination therapy of pioglitazone and SGLT2 may therefore have an offsetting effect on weight gain, an additive effect on hepatic steatosis improvement and prevention of CVD.
This study has a few limitations. First, it had a single-center design, small sample size, short duration of treatment, absence of liver biopsy, open-label design, and selection bias as the use of several antidiabetic medicines and vitamin E were prohibited. Second, the dose of pioglitazone was set to 15–30 mg/day with the intention of minimizing the risk of AEs. Only 2 of 17 patients were administered 30 mg pioglitazone. Finally, treatment group was randomly assigned to the tofogliflozin or pioglitazone group, stratified by HbA1c levels, ALT levels, and MRI-PDFF values. While not statistically different in table 1 given the small sample size, AST, GGT, ALP, systolic and diastolic blood pressure trended to higher in the pioglitazone group. The small sample size might prevent trends favoring pioglitazone versus tofogliflozin to be significant.
Future long-term studies including larger cohorts of patients with NAFLD and type 2 diabetes mellitus implementing a comparative histological assessment based on liver biopsy across multiple centers are needed to validate our findings.
In conclusion, both the treatment of pioglitazone and tofogliflozin 24 weeks improved hepatic steatosis; there were differences between the groups, including changes in weight, fibrosis and other metabolic factors. Although the antifibrotic effect of tofogliflozin in NAFLD patients with type 2 diabetes mellitus is uncertain, SGLT2 inhibitors including tofogliflozin can be potential candidates for treatment of patients with NAFLD with type 2 diabetes mellitus, as they can simultaneously improve hyperglycemia and decrease body weight efficiently.
Acknowledgments
We would like to thank the patients, their families, the study coordinators, and investigators. The technical assistance from Kyoko Kato and Machiko Hiraga, and the administrative assistance from Yoshiko Yamasaki, Ayako Ujiie, and Naho Kobayashi (Yokohama City University) are gratefully acknowledged.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors MY and AtN contributed to study design. MY, YH, YO, TakaoK, TakasK, KI, AO, AsN, HK, TI, TakeK and SS were responsible for data collection. MRI interpretation was done by KI. MT and TY participated in the data analysis. MY and AtN participated in the data interpretation. MY and AtN were responsible for the preparation of the tables and figures. All authors participated in the manuscript review and writing.
Funding The present clinical trial was conducted at the Yokohama City University (as the sponsor) and funded by Kowa Co Ltd (Tokyo, Japan).
Disclaimer The funders of this study had no role in the study design, data collection, data analysis, data interpretation, or writing of the report.
Competing interests MY received research support from Kowa Company, Ltd; the other authors report no other relationships or activities that could have influenced the submitted work.
Patient consent for publication Not required.
Ethics approval The study protocol was approved by the Yokohama City University Certified Institutional Review board (approval number: CRB318007). This trial was registered in the Japan Registry of Clinical Trials (jRCTs031180159).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Due to privacy and ethical concerns, neither the data nor the source of the data can be made available.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.