Article Text

Abstract
Objective Stair climbing–descending exercise (ST-EX) is a convenient method to increase exercise intensity. We compared the acute effect of ST-EX on lowering postprandial hyperglycemia with that of constant bicycle exercise (BI-EX) performed at the same heart rate (HR).
Research design and methods Seven people with type 2 diabetes and seven with impaired glucose tolerance volunteered for this study. The step rate for ST-EX and work rate for BI-EX were individually determined to correspond to high-moderate to low-vigorous intensity (HR ~130 beats per minute). For the ST-EX trial, the subjects performed 16 repetitions of walking down one flight of stairs followed by climbing up to the starting point (~8 min in duration) 90 min after consuming a test meal. For the BI-EX trial, the subjects performed a constant pedaling exercise for the same duration at the same time after the meal.
Results The reduction in blood glucose (BG) level between 90 and 105 min after a meal was significantly greater for ST-EX (–4.0±0.7mmol/L) than for BI-EX (–2.7±0.9mmol/L). The net reduction in BG between 90 and 105 min was also significantly greater for ST-EX (–3.2±0.7mmol/L) than for BI-EX (–2.0±0.6mmol/L). Serum insulin levels did not differ between the groups. Oxygen consumption for ST-EX was higher than that for BI-EX, but the blood lactate level and respiratory exchange ratio (RER) for ST-EX were lower than those for BI-EX.
Conclusions Compared with BI-EX performed at the same HR, ST-EX more rapidly decreased postprandial BG level with lower blood lactate and RER responses. A short bout of ST-EX may be clinically useful to acutely ameliorate BG levels after meals.
- exercise prescription
- oxygen consumption
- postprandial blood glucose
- muscle glucose uptake
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Stair climbing–descending exercise (ST-EX) is an easy-to perform method to increase exercise intensity in daily life.
What are the new findings?
ST-EX performed after a meal more rapidly decreased postprandial blood glucose level than bicycle exercise performed at the same heart rate.
How might these results change the focus of research or clinical practice?
ST-EX might be a clinically useful modality for efficient amelioration of postprandial hyperglycemia.
Introduction
Acute aerobic exercise (AE) is an important modality to control blood glucose (BG) level in people with type 2 diabetes . AE should be initiated at a moderate intensity corresponding to 40%–60% of maximal aerobic capacity, but people with type 2 diabetes already exercising at a moderate intensity have been recommended to undertake AE at a higher intensity to obtain additional BG benefits.1
Postprandial hyperglycemia is an important risk factor for cardiovascular disease.2-4 The American Diabetes Association5 recommends that postprandial BG should be controlled to <10.0 mmol/L, particularly when hemoglobin A1c (HbA1c) remains >7.0% despite preprandial BG being well controlled to 4.4–7.2 mmol/L. However, postprandial hyperglycemia is prevalent in people with type 2 diabetes, including those with apparently good HbA1c levels.6
It has been shown that high-intensity AE effectively reduces postprandial BG level.7-10 However, it is notable that the reported protocols of high-intensity AE (eg, 6 bouts of 1 min high-intensity incline walking,9 10 bouts of 60 s high-intensity cycling,8 repeated cycles of 3 min of slow and fast walking for 1 hour,10 and 4 bouts of high-intensity cycling for a total of 46 min7) are often too strenuous and/or too long to perform regularly in daily life.
We have been conducting a series of studies to demonstrate that a short period of stair climbing–descending exercise (ST-EX), a convenient method for increasing exercise intensity, is sufficient to reduce postprandial BG levels.11-15 ST-EX is easy to perform regardless of weather conditions and without the need for any special exercise facility or changing into training clothes. Typically, one set of ST-EX comprises 3‒6 min of repetitions of climbing briskly to the second floor followed by walking slowly down to the first floor. The exercise intensity is high during the ascending phase, but it is reduced during the descending phase, thereby increasing the overall intensity without excessive effort.11-14 In our recent report, we showed that a single bout of as little as 3 min of ST-EX performed 60 and 120 min after a meal decreased BG level in people with type 2 diabetes more rapidly than a fully sedentary condition.14
We also demonstrated that in people with impaired glucose tolerance (IGT), a 6 min bout of ST-EX starting 90 min after a meal decreased BG level more rapidly than a bout of level walking of the same duration.11 However, it is reasonable that ST-EX had a greater hypoglycemic effect than level walking, because the heart rate (HR) during ST-EX was significantly higher than during level walking (128±8 beats per minute (bpm) vs 113±9 bpm, p<0.01), and the estimated average oxygen consumption (VO2) of ST-EX was twice that of level walking (24.8±2.5 vs 12.3±0.7 mL/kg/min, p<0.01).11
Therefore, the primary purpose of the present study was to confirm the superiority of the acute hypoglycemic effect of ST-EX on postprandial hyperglycemia by comparing it with another type of exercise performed at the same HR as ST-EX. For this comparison, we used constant bicycle exercise (BI-EX) because BI-EX is a popular indoor exercise and its exercise intensity can be manipulated easily and quantitatively. We found that ST-EX ameliorated postprandial BG level more rapidly than BI-EX in people with type 2 diabetes or IGT.
Research design and methods
Subjects
Seven people with type 2 diabetes (male/female=4/3) and seven people with IGT (male/female=5/2) but no macrovascular and microvascular complications, whose physical characteristics and metabolic profiles are shown in (table 1), volunteered for this study. None of the subjects were engaged in any regular endurance or resistance training program at the time of the experiments, had uncontrolled hypertension (>160/100 mm Hg) or an orthopedic disorder that caused physical inactivity, or were taking drugs such as beta-blockers that affect the HR responses to exercise. The subjects were able to ascend and descend stairs without difficulties in their daily life. Five of the subjects with type 2 diabetes were being treated with oral hypoglycemic agents (glimepiride and pioglitazone (n=1); gliclazide (n=1); metformin, pioglitazone and alogliptin (n=1); metformin, pioglitazone, vildagliptin and acarbose (n=1); or metformin (n=1)). The subjects took their medications in the usual way on the experimental days. Written informed consent was obtained from all the participants before the study. The study was approved by the Institutional Review Board of Nagoya City University.
Physical characteristics and metabolic profiles of study subjects
Study design
The experiments were conducted on four separate days over 3 weeks. Intervals of more than 3 days were maintained between the experiments to avoid the metabolic effects of the exercise performed during the previous experiment. It has been shown that a single bout of exercise session increases insulin action and glucose tolerance for more than 24 hours but less than 72 hours.1 The subjects were instructed to have a Japanese-style breakfast (rice or bread, and side dishes including broiled fish, rolled omelet and vegetables; ~400 kcal) at home before 07:30 and to come to the laboratory by 11:30 on each experimental day.
On experimental day 1, the subjects performed the control (REST) trial. The subjects ate a test meal (lunch; 106.5 g carbohydrate, 18 g protein, 18 g fat, 660 kcal) between 12:00 and 12:15 and then rested quietly on a chair for 150 min. At –5, 90, 105, 120 and 150 min relative to the start time of lunch, blood samples were collected from a fingertip to determine BG level. At –5 min relative to the start time of lunch, blood samples were drawn from the antecubital vein to determine serum HbA1c level.
After completion of the REST trial, preliminary experiments were conducted to determine the step rate for ST-EX and the work rate for BI-EX that would correspond to an intensity of high-moderate to low-vigorous intensity (60%‒65% of age-predicted HR reserve (HRR)),16 and that the subjects were able to perform without a feeling of excessive effort (Borg rating of perceived exertion score of 13‒14).17 For ST-EX, a straight flight of stairs with 21 steps each 18 cm high was used. At the stairs, the subjects performed 8‒10 repetitions of ST-EX (walking down one flight of stairs followed by climbing up to the starting point) without rest. At the top and bottom of the stairs, they made a U-turn in 2‒3 s. For BI-EX, the subjects performed a pedaling exercise on an isopower-controlled cycle ergometer (232C, Combi, Tokyo, Japan) at their preferred pedaling rate (50‒65 cycles/min) for 5‒7 min. To avoid excessive fatigue because of delayed cardiac and circulatory responses, the work rate was initially set at 50% of the individually predetermined work rate for 1 min and thereafter increased to the predetermined work rate. HR was recorded every 5 s during exercise using an HR monitor (Polar Accurex Plus; Polar Electro, Kempele, Finland).
On experimental day 2 and day 3, the subjects performed either the ST-EX or BI-EX trials in random order (figure 1). We chose the timing for exercise based on previous findings that ST-EX starting at 90 min after a meal resulted in a rapid and substantial decrease in BG, and did not induce a rebound of BG after exercise.11 13 For the ST-EX trial, the subjects had lunch between 12:00 and 12:15, rested on a chair for 90 min and then performed 16 repetitions of ST-EX (walking down one flight of stairs followed by climbing up to the starting point) without rest or, if they requested it, a short rest (<30 s) in standing position at the top of the stairs. They climbed the stairs at an individually predetermined step rate of 80–115 steps/min to the beat of a metronome, and descended at a free step rate, which was lower than the ascending rate for each individual. For the BI-EX trial, the subjects had lunch between 12:00 and 12:15, rested on a chair for 90 min and then performed the pedaling exercise at an individually predetermined work rate. The duration of BI-EX was the same as that of ST-EX for each subject. We determined the timing for blood sampling based on previous findings that the hypoglycemic effect of ST-EX starting at 90 min was significant at 105 min11 13 and 120 min11 after a meal. At –5, 90, 105, 120 and 150 min relative to the start time of lunch, blood samples were collected from a fingertip to determine the BG level. At 90, 120 and 150 min relative to the start time of lunch, blood samples were drawn from the antecubital vein to determine serum insulin level. At 1 min after the end of ST-EX or BI-EX, blood samples were collected from a fingertip to determine plasma lactate levels. HR was monitored every 5 s during exercise using Polar Accurex Plus. After the experiment on day 3, the subjects answered the question ‘Which exercise (ST-EX or BI-EX) did you feel required less effort?’
On experimental day 4, the subjects performed the ST-EX and BI-EX trials, accompanied by expired gas analysis using the Douglas bag method (figure 1). Three older women with type 2 diabetes were excluded from this investigation to avoid the risk of their falling on the stairs because of interference with their vision by the gas sampling mask. The subjects performed both ST-EX and BI-EX in random order as described above, with a rest interval of at least 50 min between the exercises. VO2 and respiratory exchange ratio (RER) were determined during the steady state of ST-EX (last 8 repetitions, ~4 min) and of BI-EX (last 4 min) by a gas analyzer (AR-1, Arco System, Chiba, Japan). HR was monitored every 5 s during exercise. One minute after the end of ST-EX or BI-EX, a blood sample was collected from a fingertip to determine plasma lactate level.
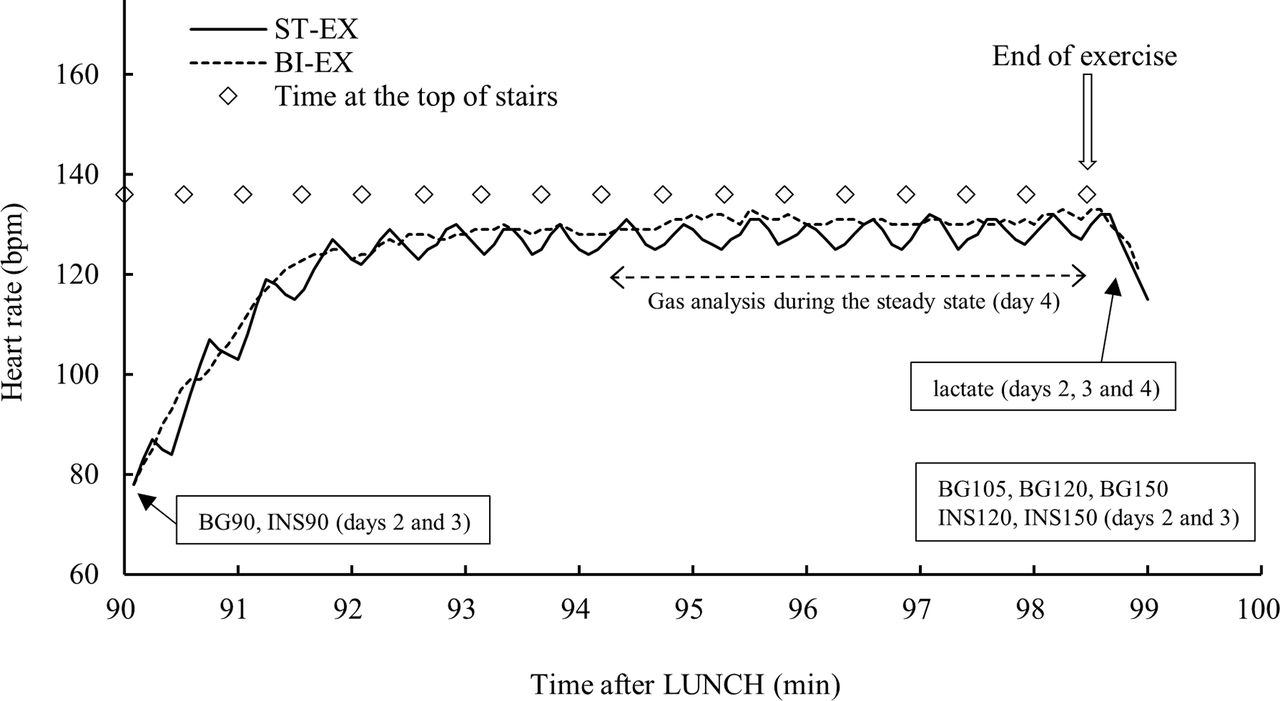
Experimental protocol for days 2, 3 and 4. On days 2 and 3, subjects performed either ST-EX (16 repetitions) or BI-EX for the same duration starting 90 min after lunch. Blood glucose and insulin levels were measured at 90 min (immediately before starting exercise), 105, 120 and 150 min, and 90, 120 and 150 min after lunch, respectively. On day 4, subjects performed ST-EX and BI-EX in random order with a rest interval of >50 min. Gas analysis was conducted during the steady state of ST-EX (last 8 repetitions, ~4 min) and BI-EX (last 4 min). Blood lactate was measured 1 min after exercise on days 2, 3 and 4. Heart rate was monitored every 5 s during exercise on days 2, 3 and 4. BI-EX, bicycle exercise; bpm, beats per minute; ST-EX, stair climbing–descending exercise.
Blood sample analysis
BG was simultaneously measured in singlicate or duplicate using three different sets of automatic glucose analyzers (Glutest Ace; Arkray, Kyoto, Japan). The average value was calculated. BG0, BG90, BG105, BG120 and BG150 represent BG at –5, 90, 105, 120 and 150 min from the beginning of lunch, respectively. ΔBG90–105, ΔBG90–120 and ΔBG90–150 represent the differences in BG between BG90 and BG105, BG90 and BG120, and BG90 and BG150, respectively. Serum insulin level was measured using an immunoassay kit (Architect Insulin, Abbott Japan, Tokyo, Japan). INS90, INS120 and INS150 represent the serum insulin levels 90, 120 and 150 min from the beginning of lunch, respectively. ΔINS90–120 and ΔINS90–150 represent the difference in serum insulin level between INS90 and INS 120, and between INS90 and INS150, respectively. Plasma lactate level was determined in singlicate using an automated analyzer (Lactate Pro; Arkray). HbA1c level was assayed at Nagoya Clinical Center (Nagoya, Japan) using a latex-agglutination assay.
Statistical analysis
Data are shown as mean±SD except for those in figure 2B. Mann-Whitney U test was performed to determine whether there were significant differences between type 2 diabetes and IGT (tables 1, 2 and 3). Differences between ST-EX and BI-EX were analyzed by paired analysis using the Wilcoxon signed-rank test (table 2). Comparisons of data between the three trials were performed using the Friedman test (table 3, figure 1). Post-hoc testing of significance between corresponding mean values was performed using the Scheffe method. Significance was set at p<0.05. All statistics were analyzed using SPSS V.18.0 for Windows.
{kind=link}
{kind=link}
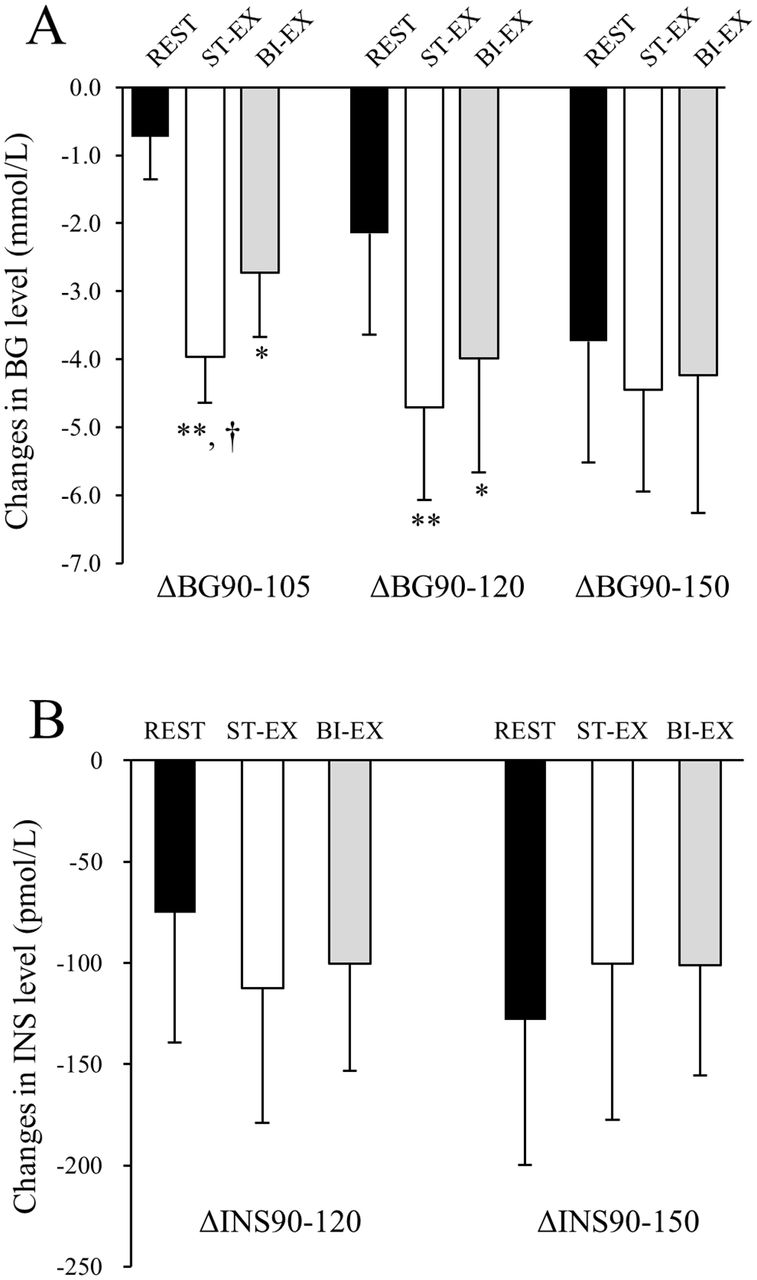
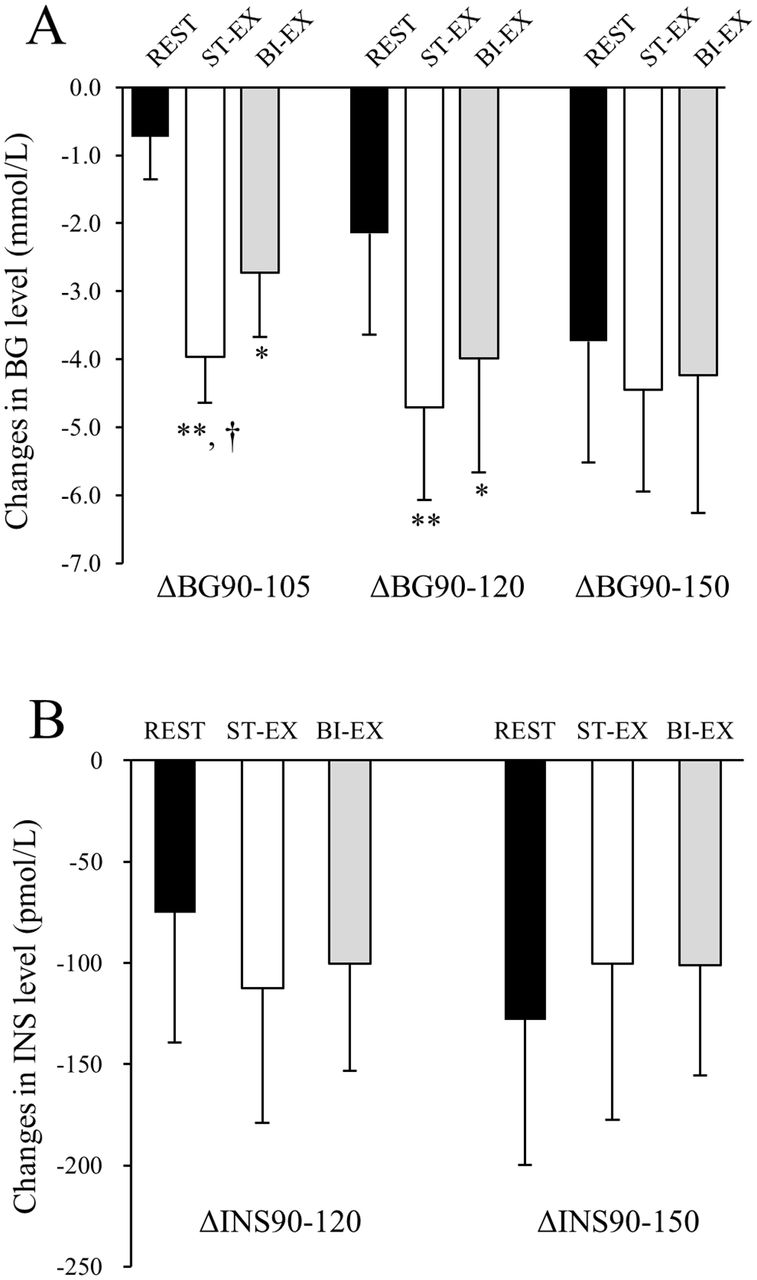
(A) Changes in BG level during REST, ST-EX and BI-EX trials in the combined (ALL) group. * and ** indicate the presence of significant differences (p<0.05 and p<0.01, respectively) from REST. † indicates the presence of a significant difference (p< 0.05) from BI-EX. Values are expressed as mean±SD. n=14. (B) Changes in serum insulin (INS) level during REST, ST-EX and BI-EX trials in the combined group. Values are expressed as mean±SE. n=14. BG, blood glucose; BI-EX, bicycle exercise; INS, serun insulin; ST-EX, stair climbing–descending exercise.
Physiologic responses to ST-EX and BI-EX (experimental days 2 and 3)
Changes in blood glucose (BG) level during REST, ST-EX and BI-EX trials
Results
Physiologic responses to ST-EX and BI-EX
Table 2 shows the physiologic responses to ST-EX and BI-EX in the type 2 diabetes, IGT and combined (ALL) groups measured on experimental day 2 and day 3. HR, %HRR and exercise duration did not differ significantly between the groups or trials. By contrast, the blood lactate level for ST-EX was significantly lower than that for BI-EX in each group (p<0.05). Five subjects with type 2 diabetes and four with IGT responded that ST-EX required less effort than BI-EX, and one subject with type 2 diabetes and 2 with IGT answered that both ST-EX and BI-EX required equal effort.
VO2 and RER during the steady state of ST-EX and BI-EX were measured on experimental day 4. There were no differences in the steady-state HR (ST-EX 130.6±5.9 bpm vs BI-EX 131.1±6.7 bpm, NS) and %HRR (ST-EX 63.3±8.3% vs BI-EX 63.7±8.0%, NS). VO2 for ST-EX was significantly higher (by 9%) than that for BI-EX (ST-EX 18.7±1.4 mL/kg/min vs 17.2±1.3 mL/kg/min, p<0.01), but RER and blood lactate level for ST-EX were significantly lower than those for BI-EX (RER: ST-EX 0.91±0.05 vs BI-EX 0.97±0.04, p<0.01; lactate: ST-EX 3.4±1.2 mmol/L vs BI-EX 4.4±1.0 mmol/L, p<0.01).
Changes in BG level after ST-EX and BI-EX
Table 3 shows the changes in BG level during the REST, ST-EX and BI-EX trials. BG90, that is, BG level immediately before starting ST-EX or BI-EX, for the type 2 diabetes group was higher than that for the IGT group (p<0.05), and there were no differences in BG90 between the trials for each subject group. However, ΔBG90–105 for ST-EX was much greater than that for REST in the type 2 diabetes group (7.5× higher, p<0.05), the IGT group (4.3×, p<0.01) and the combined group (5.5×, p<0.01). ΔBG90–105 for ST-EX was also 1.5× greater than that for BI-EX for the combined group (p<0.05). The net decrease in BG between BG90 and BG105 (net ΔBG90–105) for ST-EX was significantly greater (by 77%) than that for BI-EX in the type 2 diabetes group (p<0.05), by 48% in the IGT group (p<0.05) and by 62% in the combined group (p<0.01). There was no difference in net ΔBG90–105 between type 2 diabetes and IGT groups.
Figure 2A shows the time-course changes in ΔBG during the REST, ST-EX and BI-EX trials for the combined group. ΔBG90–105 for ST-EX was greater than that for either REST (p<0.01) or BI-EX (p<0.05), and ΔBG90–120 for ST-EX was greater than that for REST (p<0.01). However, ΔBG90–120 for ST-EX did not differ from that for BI-EX, and ΔBG90–150 for ST-EX did not differ from those for BI-EX or REST.
Changes in insulin level after ST-EX and BI-EX
Figure 2B shows ΔINS90–120 and ΔINS90–150 for the combined group. There were no differences in ΔINS between the trials for either time period. INS90 also did not differ between the trials (420±320, 310±306 and 322±259 mmol/L for REST, ST-EX and BI-EX trials, respectively).
Discussion
The novel finding of the present study is that an approximately 8 min bout of ST-EX starting 90 min after a meal decreased postprandial BG level more rapidly than REST and BI-EX performed at the same HR in subjects with IGT and type 2 diabetes, although the serum insulin levels did not differ between the three groups. It has been shown that changes in insulin level during exercise are related to the intensity and duration of the exercise. For example, Larsen et al7 18 showed that moderate-intensity to high-intensity BI-EX for 45 min during the ascending phase of BG after a meal blunted the postprandial increase in insulin level in people with type 2 diabetes. Insulin secretion was decreased in response to the reduction in BG level induced by exercise and by the induction of a counter-regulatory response during exercise, including increased sympathetic nervous activity.19 Our data suggest that neither ST-EX nor BI-EX elicited a strong counter-regulatory effect, and that insulin secretion was reduced as a secondary response to the decreased BG levels.
It is well established that contraction rapidly activates glucose uptake in skeletal muscle by inducing translocation of glucose transporter 4 (GLUT4) to the cell surface (contraction-stimulated glucose uptake).20 21 It has been shown in humans that glucose uptake is increased within 5 min,22 23 and reaches a near-maximum within 10 min after the start of exercise.24 In rat skeletal muscle incubated in vitro a single 10 s contraction by electrical stimulation (ES) was sufficient to initiate increased glucose uptake, and maximal glucose uptake was achieved after 10 contractions (once per minute).25 This increase was maintained for at least 10 min after stimulation and had decreased by only 50% after 60 min.25 In another study of rat skeletal muscle, 34% of the initial level of glucose uptake was maintained 3 hours after exercise.26 Importantly, contraction-stimulated glucose uptake and GLUT4 translocation in humans remain at normal levels in insulin-resistant conditions such as type 2 diabetes and obesity.27-29 These exercise-evoked mechanisms have been widely applied for acute amelioration of high BG, particularly postprandial hyperglycemia.
Our results appeared to show a discrepancy between VO2 and blood lactate/RER values (see ‘Physiologic responses to ST-EX and BI-EX’). Although the results for VO2 indicate that the exercise intensity for ST-EX was higher than that for BI-EX, blood lactate/RER results suggest that the exercise intensity was lower for ST-EX than for BI-EX. Moreover, 9 of 14 (64%) subjects responded that ST-EX required less effort than BI-EX did. The rate of carbohydrate utilization for both aerobic and anaerobic energy production increases as the work intensity increases.23 30 In the present study, the average power during the ascending phase of ST-EX for the combined group was estimated to be ~180 W (62.5 (kg) × 9.8 (m/s2) × 0.18 (m) × 96.9/60 (steps/s)). When an individual ascends stairs continuously at this work rate, their estimated rate of VO2 is ~39 mL/kg/min (2.03 × 0.18 (m/step) × 96.9 (steps/min) + 3.7).12 We did not determine the aerobic capacity of the study subjects, but considering their age and their lack of current participation in exercise programs, it is highly likely that a large part of their energy production during the ascending phase of ST-EX was dependent on anaerobic glycolysis. However, our ST-EX protocol consisted of a short ascending phase (~13 s) followed by a long descending phase with U-turns on a flat floor (~18 s). We consider that for most of the study subjects, this alternative exercise regimen of ST-EX decreased the blood lactate/RER values below the levels generated by BI-EX and alleviated the perceived exertion while maintaining VO2 at higher levels than with BI-EX. In this regard, it should be noted that a light-intensity or moderate-intensity exercise subsequent to a high-intensity exercise has an ‘active recovery’ effect, which clears blood lactate faster than ‘passive recovery’.31 32
Because the rate of glucose uptake is closely correlated with exercise intensity represented by VO2 during exercise,22-24 to some extent, the small (9%) but significant difference in VO2 between ST-EX and BI-EX may contribute to the significant difference in the reduction in BG produced by ST-EX and BI-EX. However, different modes of exercise often induce different physiologic and metabolic responses even at the same VO2. We previously compared the effect of ES of lower limb muscles with that of voluntary contractions (VC) at the same VO2 using a glucose clamp procedure.33 In healthy subjects lying in the supine position, both lower limb muscles were stimulated through surface electrodes to contract for 20 min (20 Hz stimulation frequency with 1 s on–off duty cycle). On a different day, the subjects also performed supine VC for 20 min using a cycle ergometer. Despite the identical elevation of VO2 from baseline (ES 7.3±0.3 mL/kg/min vs VC 7.5±0.3 mL/kg/min, NS), ES increased the blood lactate concentration from 1.2±0.1 to 3.2±0.3 mmol/L (p<0.01) after the initiation of ES, whereas VC caused no such increase. ES also elevated RER more strongly than did VC (ES 0.99±0.03 vs VC 0.83±0.03, p<0.01). Furthermore, the increase in glucose disposal rate disappeared within 50 min after the cessation of VC, while it was maintained for at least 90 min after the cessation of ES. These observations clearly indicate that VO2 is not the ‘gold standard’ for adjusting the exercise intensity of different exercise types, particularly when examining glucose uptake and glycolysis in contracting skeletal muscles. In the present study, we used HR, instead of VO2, to adjust the exercise intensity of ST-EX and BI-EX, because it is one of the most widely used modalities for monitoring exercise intensity in clinical practice.16
We note that the body mass index (BMI) of Japanese people with type 2 diabetes is lower than that of Westerners. For instance, the average BMI of participants in the UK Prospective Diabetes Study was 29.4 kg/m2 (n=2015), while that of the participants in the Japan Diabetes Complication Study was only 23.1 kg/m2 (n=2205).34 The BMI of the subjects of this study was comparable with the Japanese value (table 1). Because the maximal cardiorespiratory fitness of obese individuals with type 2 diabetes is often as low as 7–9 metabolic equivalents (METs)35 36 there may be concern that ST-EX is too strenuous for obese patients and is not practically applicable to such subjects. In this regard, we previously measured VO2 in Japanese adults who performed ST-EX with or without a weight jacket to adjust each subject’s BMI to 25, 30 and 35.12 These experiments clearly demonstrated that VO2 values were almost equal regardless of the change in BMI (18.8‒20.2 mL/kg/min (5.4‒5.8 METs at 90 steps/min). We consider that the exercise intensity of ST-EX per se is within a well-tolerated level not only in normal-weight patients but in most obese patients.
The clinical significance of the differences in the decrease in postprandial BG after ST-EX and after BI-EX needs to be clarified in a future study. Continuous glucose monitoring may be helpful to analyze precisely the BG responses after both types of exercises. We recently conducted a pilot study to explore the practical relevance of the differences in the decrease in postprandial BG in people with type 2 diabetes with and without ST-EX.15 Seven men with type 2 diabetes who took oral hypoglycemic agents (age 68.0±3.7 years) performed two sets of ST-EX 60 and 120 min after each meal for the first 2 weeks, but not for the following 2 weeks. Each set of exercises, which were performed at home, comprised 3 min of continuous repetition of climbing briskly to the second floor at a rate of 80–110 steps/min followed by slow walking down to the first floor at a free step rate. A rest period of 1–2 min was allowed between each set. We found that the serum 1,5-anhydroglucitol level significantly increased by 11.5% from baseline at the end of the 2-week exercise period (p<0.05), and returned to the baseline value at the end of the following 2-week period. These results indicate that a home-based postprandial ST-EX program may improve the overall glycemic control in sedentary people with type 2 diabetes.
In summary, an 8 min bout of ST-EX starting 90 min after a meal and comprising 16 repetitions of walking down one flight of stairs followed by brisk climbing up to the starting point has an acute hypoglycemic effect in people with IGT and type 2 diabetes. Compared with BI-EX performed at the same HR, ST-EX more rapidly ameliorated postprandial hyperglycemia, although the blood lactate level and RER were significantly lower and VO2 was higher for ST-EX than BI-EX. Based on these observations and our previous reports,11-15 we propose that a short bout of ST-EX is a potentially useful method to improve glucose excursion after meals. The exercise regimen of ST-EX (eg, step rate, number of repetitions, duration of rest between the repetitions and so on) should be individually adjusted according to clinical condition.
Acknowledgments
The authors gratefully acknowledge the helpful advice of Dr. Sung Chul Lee. The authors also express their sincere gratitude to the study participants for their time and effort.
References
Footnotes
Contributors TT conceived, designed and performed the experiments. TT and TH analyzed the data and wrote the manuscript. Both authors approved the final version of the manuscript. Both authors are the guarantors of this work.
Funding This work was supported by Grants-in-Aid for Research from Nagoya City University; JSPS KAKENHI (15K01711) and research grants from the Japanese Council for Science, Technology and Innovation, SIP (project ID: 14533567) (funding agency: Bio-oriented Technology Research Advancement Institution, NARO); Ministry of Agriculture, Forestry and Fisheries, Integration Research for Agriculture and Interdisciplinary Fields (project ID: 14532022) (funding agency: Bio-oriented Technology Research Advancement Institution, NARO); and Vascular Disease Research Foundation.
Competing interests None declared.
Ethics approval The Institutional Review Board of Nagoya City University.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement This manuscript includes all the data available.