Article Text

Abstract
Introduction Insulin pumps are able to deliver bolus insulin as a standard, extended or combination bolus. There is minimal research to determine which bolus is preferable in different settings. Anecdotally, many patients utilizes only the standard bolus (SB) due to uncertainty regarding when and how to program the different bolus types. We compared postprandial glycemia when five different extended boluses (EBs) and an SB were used following a test meal. We sought to determine the impact of varying rates of insulin delivery from an EB on early postprandial glycemia.
Methods We conducted a randomized, repeated measures trial of 20 children and adults comparing postprandial glycemic excursions following EBs given at five different rates with SB as a control. All EBs were delivered over 2 h. Rates of EBs were chosen to reflect EBs used in clinical practice: EB1HR=100% of insulin:carbohydrate ratio (ICR) per hour (200% ICR total dose); EB2HR=50% of ICR per hour; EB3HR=33% of ICR per hour; EB4HR=25% of ICR per hour; EB6HR=16% ICR per hour. A standardized breakfast was given and activity was standardized. Continuous glucose monitoring was used to assess glycemia for 2 h after the meal.
Results The mean postprandial glycemic excursions were lower at 30, 60, and 90 min (p<0.05) for SB compared with all EBs. The mean peak postprandial glycemic excursion and the area under the curve was lower for SB compared with all EBs (p<0.05).
Discussion EBs resulted in higher postprandial glycemic excursions than SB for 2 h after the meal. For a moderate glycemic index meal EBs are unable to control glycemia for 2 h after a meal as well as SB. Further studies with different meal types are required to determine the impact of differential delivery of the EB on postprandial glycemia.
Trial registration number ACTRN12612000609853.
- Insulin Delivery
- Insulin Dose Management
- Insulin Pump Therapy
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
-
Extended insulin boluses have been recommended for high fat and protein meals, low glycemic index meals, and in persons with gastroparesis with little research evidence to support such recommendations.
-
In this study of children and adults with well-controlled type 1 diabetes without evidence of complications of diabetes, extended insulin boluses resulted in unacceptable early postprandial hyperglycemia that was not shown with a standard bolus.
-
Further studies of extended boluses across meal types and in different patient groups should be performed to determine whether there is any clinical indication for their use.
Introduction
Modern insulin pumps are capable of delivering meal bolus insulin in three main ways: standard bolus (SB) or rapid bolus, where the insulin is delivered immediately; extended or square wave bolus, where the insulin delivery is spread over a longer time period; and combination or dual wave bolus, where a percentage of the insulin is delivered as a rapid bolus and the remainder is delivered as an extended bolus (EB). Minimal research has been performed to date comparing the different methods of meal bolus insulin delivery.
In our clinical practice, most patients and families exclusively use the SB to deliver the mealtime insulin dose. This is despite current recommendations to use extended and combination boluses for meals high in fat and protein, low glycemic index (GI) meals, and for persons with gastroparesis.1–5 Anecdotally, patients and families report confusion in utilizing the different bolus types due to uncertainty regarding the optimal rate of delivery. To the best of our knowledge, there is no current evidence-based guideline available to assist clinicians, patients and families wishing to program an extended or combination insulin bolus.
Studies of extended insulin boluses are particularly limited. Research to date has suggested that extended insulin boluses are not able to control the postprandial glucose rise for up to 120 min after a meal as well as a standard or combination bolus.6 ,7 This finding limits the utility of ESs, as postprandial hyperglycemia has been associated with complications of diabetes.8–10 However, thus far, multiple rates of extended insulin bolus have not been compared in a clinical research setting. We sought to determine whether increasing the rate of the EB could prevent the postprandial hyperglycemia seen at 60 min following an EB in previous studies.6 ,7 Our aim was to determine the rate of insulin delivery required for an extended insulin bolus to control the early postprandial glucose rise. Our goal was to determine an evidence-based guideline for patients and families wishing to utilize the EB feature of their insulin pump.
Methods
Participants
This study was a randomized, within-person, repeated measures trial conducted at the John Hunter Children's Hospital, Newcastle, Australia. Children and young adults with type 1 diabetes mellitus (T1DM) diagnosed for ≥1 year and treated with insulin pump therapy for ≥6 months were eligible for recruitment. Inclusion criteria were age between 7 and 39 years inclusive, glycated hemoglobin (HbA1c) ≤8% (64 mmol/mol), and body mass index ≤97th centile. Exclusion criteria were coexisting medical problems (including celiac disease), use of medication affecting blood glucose levels (BGLs) other than insulin, complications of diabetes (eg, gastroparesis), inability or unwillingness to take the test meals and inability to take part in the study day due to premeal hyperglycemia (BGL ≥12 mmol/L) or hypoglycemia (BGL ≤3.5 mmol/L).
The study was completed in compliance with the Declaration of Helsinki and the International Conference on Harmonisation Good Clinical Practice Guidelines. Written informed consent and assent was obtained from all participants and their guardians if less than 18 years.
Study procedure
In the week prior to the study, participants and/or their guardians were contacted daily to review the patient's BGLs. Adjustments were made to the insulin pump settings as necessary to meet a prebreakfast BGL target of 4–8 mmol/L and to optimize the breakfast insulin:carbohydrate ratio (ICR) to meet a prelunch BGL target of 4–8 mmol/L. During the study period participants were instructed not to adjust their insulin pump settings.
A standardized, moderate GI meal was provided to each participant for consumption each day for 6 days at breakfast. The test meal consisted of a breakfast cereal, full cream milk, toast, and orange juice and contained 60 g of carbohydrate, 10 g of fat, and 10 g of protein. The meal was based on foods commonly consumed by people with diabetes in our clinic. Meals were individually packaged, with instructions to keep chilled prior to consumption. Food was prepared under controlled conditions and was weighed using Salter kitchen scales (accuracy±1 g; model 323, Salter, Kent, UK). It is clinical practice in some Australian clinics to recommend the use of EBs for all meals (not just high fat or low GI) in an effort to optimize postprandial glycemia.
The insulin dose for each participant was determined for the meal using the participant’s individualized ICR. Five different EB rates and one SB were delivered in random order at breakfast over the 6 days of the study.
The rates chosen for the EBs were based on how these boluses are delivered in clinical practice. In our clinic, the recommended insulin amount for an EB is equal to the ICR. Typically, EBs are delivered over 1–6 h. EB1HR delivered 100% of the ICR per hour for 2 h (total insulin dose 200% ICR) and represents the rate of insulin delivery for an EB given over 1 h, EB2HR delivered 50% of the ICR per hour for 2 h (total insulin dose 100% ICR) and represents the rate of insulin delivery for an EB given over 2 h, EB3HR delivered 33% of the ICR per hour for 2 h (total insulin dose 66% ICR) and represents an EB given over 3 h, EB4HR delivered 25% of the ICR per hour for 2 h (total insulin dose 50% ICR) and represents an EB given over 4 h and EB6HR delivered 16% of the ICR per hour for 2 h (total insulin dose 32% ICR) and represents an EB given over 6 h. Participants were randomized according to computer generated randomization to deliver each bolus once. The EBs were given for 2 h and the glucose level was monitored for 2 h after the test meal with continuous glucose monitoring (CGM). The study period was for the 2 h postprandial period.
The observation period was increased to 3 h for the SB and the EB2HR, where the total insulin dose was identical, to allow interpretation of the glycemic curves until they returned to baseline.
Participants were required to fast overnight for at least 6 h prior to breakfast and for 2 h following the test meal. The bolus administration was started immediately prior to the participant eating the test breakfast. Administering the insulin bolus immediately before the meal is common practice in our clinic as it decreases the likelihood of it being forgotten or the child becoming distracted and not eating at the specified time. Participants were required to consume the test meal within 20 min. If patients developed hypoglycemia (BGL ≤3.5 mmol/L or symptoms of hypoglycemia and BGL ≤4.0 mmol/L) 15 g of oral carbohydrate was given and analysis stopped at that point.
Participants changed their insulin pump site on days 1, 3, and 5 of the study.
A capillary blood glucose, food and activity diary was kept by each participant and their caregiver to assess adherence to the study protocol. Only sedentary activity was permitted during the 2 h postprandial period.
Blood glucose measurement
The iPro2 Continuous Glucose Monitoring System (Medtronic MiniMed, Northbridge, California, USA) was used to determine postprandial BGLs over the 6 days of the study. Participants and their guardians were blinded to the CGM analysis.
Participants attended the clinic on the afternoon prior to the start of the study for insertion of CGM. The instructions for use of the CGM, as per the manufacturer's guidelines, were discussed with the participant and/or their caregiver. Participants were asked to record at least four capillary blood glucose measurements per day into their study diary for calibration of the CGM.
At the completion of the study, data was downloaded from the CGM using the Medtronic CarelinkiPro data system (Medtronic MiniMed).
Statistical analysis
A sample size of 20 participants was calculated to provide 80% power to detect a difference of postprandial blood glucose excursions of 3 mmol/L at 60 min with a 5% significance level, assuming a within-person SD in BGL of 2 mmol/L.
The primary outcome measure was the postprandial glucose excursion at 60 min. This measure was chosen as we sought to determine whether increasing the rate of the EB could prevent the postprandial hyperglycemia seen at 60 min following an EB in previous studies.6 ,7 Secondary outcomes included the postprandial glucose excursions at 30 min intervals from 30 to 120 min, the peak postprandial glucose excursion, the time to peak postprandial glucose excursion, and hypoglycemic events defined as capillary BGL ≤3.5 mmol/L or capillary BGL ≤4.0 mmol/L with symptoms of hypoglycemia.
Data was analyzed in STATA V.11. A mixed models logistic analysis was used to compare postprandial glycemic excursions. McNemar's test was used to examine differences in hypoglycemic events. Regression analysis was used to compare area under the curve.
Results
Twenty participants (10 male) aged 7–36 years were included with a mean age of 18±2.4 years. Mean HbA1c was 7.0±0.2% (53 mmol/mol). Mean duration of diagnosis of T1DM was 7.4±1.5 years and duration of insulin pump therapy was 3.9±0.6 years. The mean insulin bolus dose at breakfast was 1 unit/8.6±0.2 g of carbohydrate.
Preprandial BGLs
There was no difference in the preprandial BGLs between the different bolus types (p<0.05; see table 1).
Mean preprandial BGL, mean PPGE at 1 and 2 h, peak PPGE, time to peak PPGE and mean 2 h AUC following an SB and five different insulin infusion rates for an EB given for a test meal
Postprandial glycemic excursion
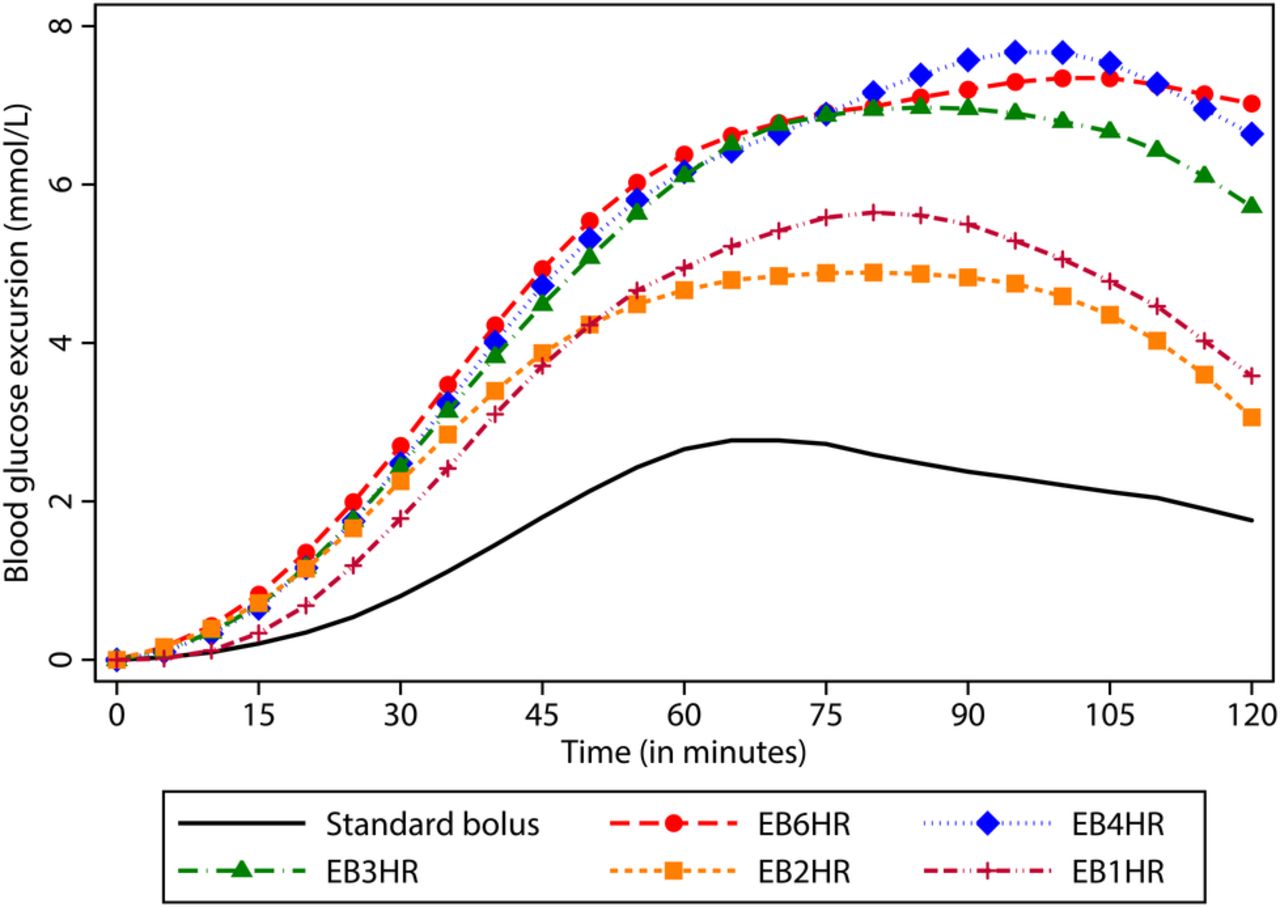
Figure 1 illustrates the mean postprandial glycemic excursion for 120 min following the meal for each of the bolus types. At 60 min following the test meal, the glycemic excursion was significantly lower following the SB than all EBs (SB 2.9±2.8 mmol/L vs EB1HR (4.9±3.1 mmol/L, p<0.02), EB2HR (4.7±4.2 mmol/L, p<0.05), EB3HR (5.8±4.4 mmol/L, p<0.01), EB4HR (6.2±4.0 mmol/L, p<0.01), and EB6HR (6.4±3.4 mmol/L, p<0.01)). At 90 min following the test meal, the glycemic excursion remained significantly lower following the SB than all EBs (SB 2.4±0.9 mmol/L vs EB1HR (5.4±0.9 mmol/L, p<0.02), EB2HR (4.8±1.0 mmol/L, p<0.04), EB3HR (6.6±1.1 mmol/L, p<0.01), EB4HR (7.6±1.0 mmol/L, p<0.01), and EB6HR (7.2±1.0 mmol/L, p<0.01)). At 120 min following the test meal, the mean glycemic excursion remained lower following the SB than all EBs, however a statistically significant difference was found only for EB3HR, EB4HR, and EB6HR (SB 1.76±4.4 mmol/L vs EB1HR (3.6±4.0 mmol/L, p=0.09), EB2HR (3.1±4.3 mmol/L, p=0.18), EB3HR (5.4±3.9 mmol/L, p<0.01), EB4HR (6.6±4.0 mmol/L, p<0.01), and EB6HR (7.2±4.2 mmol/L, p<0.01; see table 2)).

Postprandial glycemic excursions for 120 min following a standard bolus and five different insulin infusion rates for an extended bolus (EB) given for a standardized test meal.
Postprandial glycemic excursions from 15 to 120 min following an SB and five different insulin infusion rates for an EB given for a test meal
Peak glycemic excursion
The peak glycemic excursion was lower for SB (4.1±3.5 mmol/L) compared with EB1HR (6.6±3.2 mmol/L, p<0.02), EB2HR (5.9±3.5 mmol/L, p=0.06), EB3HR (7.3±5.2 mmol/L, p<0.01), EB4HR (8.4±4.0 mmol/L, p<0.01), and EB6HR (8.1±3.6 mmol/L, p<0.01; see table 2).
Time to peak glycemic excursion
The time to peak glycemic excursion was less for an SB (60.0±35.1 min) compared with EB1HR (75.3±18.2 min, p<0.05), EB2HR (71.1±45.2 min, p=0.20), EB3HR (94.2±47.0 min, p<0.01), EB4HR (85.0±20.9 min, p<0.01), and EB6HR (95.3±35.4 min, p<0.01; see table 2).
Area under the curve
The area under the curve was significantly less for SB (249.1±68.7 mmol/h/L) compared with EB1HR (443.9±90.1 mmol/h/L, p<0.04), EB2HR (440.3±91.6 mmol/h/L, p<0.04), EB3HR (564.8±90.1 mmol/h/L, p<0.01), EB4HR (593.5±91.6 mmol/h/L, p<0.01), and EB6HR (596.2±91.6 mmol/h/L, p<0.01; see table 2).
Hypoglycemic events
There was one hypoglycemic event in the SB group and one in the EB1HR bolus group.
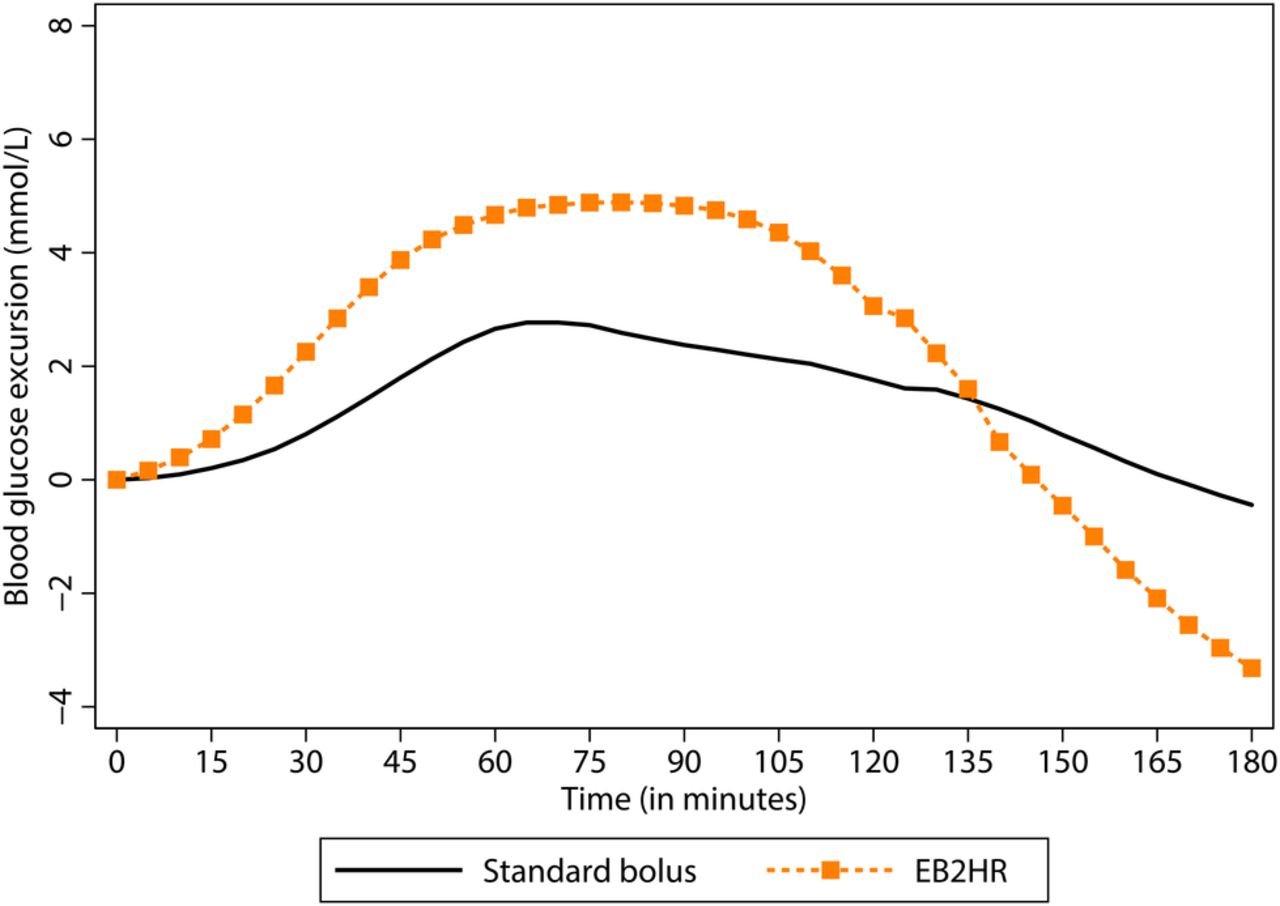
SB versus EB2HR
Figure 2 illustrates the mean postprandial glycemia excursion for SB and EB2HR for 180 min following the test meal. The postprandial glycemic excursion following the test meal was significantly lower for SB compared with EB2HR from 15 to 60 min and at 90 min following the test meal. By 180 min after the test meal, the glycemic excursion was significantly higher for SB compared with EB2HR (see table 3).
{kind=link}
{kind=link}
Postprandial glycemic excursions for 180 min following a standard bolus and an extended bolus (EB2HR) of identical total insulin dose given for a standardized test meal.
Mean preprandial BGL, mean postprandial glycemic excursion at 60, 120, and 180 min, peak postprandial glycemic excursion, time to peak postprandial glycemic excursion and mean 120 min AUC following an SB and an EB of equal total insulin dose delivered over 120 min
Discussion
We found that for a standardized moderate GI test meal of mixed macronutrient composition, an extended insulin bolus was unable to control the early postprandial glucose rise as well as an SB. In particular, we found that even when the total insulin dose was double the ICR, as demonstrated by EB1HR, the extended insulin bolus was still unable to control postprandial glycemia over a 2 h period as well as an SB. Furthermore, there was no increase in the rate of hypoglycemia with SB compared with EB.
This is the first study known to the authors to compare early postprandial glycemia following a standardized meal for EBs given at five different rates, as well as an SB. We aimed to determine whether increasing the rate of delivery of the EB could prevent postprandial hyperglycemia for up to 120 min shown in previous studies using an EB.6 ,7 We only studied the 2 h postprandial period, however, we hypothesize the loss of blood glucose control in the initial postprandial period with the extended insulin bolus negates any possible finding of improved control in the later postprandial period. Studies extending the period of observation after the test meal would have defined a period of hyperglycemia for the different EBs.
We used a standardized test meal that reflected a common breakfast meal eaten by Australian children and adults. This allowed us to study the postprandial glucose control achieved with an EB and SB following a typical meal, in order to provide advice to patients and families wishing to utilize the EB. We considered the test meal to be a moderate-GI, moderate-fat, moderate-protein meal. As the extended insulin bolus has been suggested for low GI meals and high-fat, high-protein meals, as well as for persons with gastroparesis, our study may have been bolstered if different meal types were used.1–5 Nonetheless, all meal types, including high-fat and low-GI meals, result in an initial postprandial glucose rise. Smart et al11 found that the glycemic excursion following a high-fat meal was 2.2 mmol/L at 60 min. Ryan et al12 showed a peak glycemic excursion of 4.6 mmol/L for a low-GI meal. Future studies could be conducted using an extended insulin bolus for a variety of meal types.
There are only two studies known to the authors, which utilize the EB feature of insulin pumps. Chase et al6 found that for a pizza meal, an extended insulin bolus delivered over 2 h was not able to control postprandial glycemia as well as SB for up to 120 min following the test meal. However, postprandial control at 4 h after the meal was improved compared with an SB. Our study, while only including 20 participants, is larger than this study of 9 participants. We also compared multiple rates of EB delivery with an SB, rather than a single rate. However, the period of observation of the Chase et al6 study was 6 h, providing valuable insight into postprandial glucose levels for many hours after the test meal. Both studies suggest that the extended insulin bolus is ineffective in controlling early postprandial hyperglycemia.
Lindholm-Olinder et al compared an SB, EB and combination bolus given for two meals with different fat, carbohydrate and protein contents in 14 adolescent girls with T1DM. At 60 min following the higher fat meal, the BGL was significantly higher for the ED compared with SB and combination bolus.10 This study adds weight to our finding that an extended insulin bolus is unable to control hyperglycemia in the early postprandial period.
Our study demonstrated that for a standardized meal, the extended insulin bolus is not able to control the early postprandial glucose rise as well as an SB, irrespective of the rate of insulin delivery. This finding suggests that the EB may only be a useful tool in certain clinical scenarios, such as in a person with gastroparesis. We suggest that further studies of the EB in such situations, as well as across meal types, are required to determine whether recommendations for using the EB should be amended.
Circadian variations in cortisol, growth hormone and other hormones may increase insulin requirements in the morning hours.13 We chose breakfast for our study as we have successfully utilized this methodology in other studies as it permits meal and activity supervision.11 ,12
The timing of the mealtime insulin bolus may impact postprandial glycemia. Studies suggest that giving the insulin bolus up to 30 min before a meal may be beneficial.13 ,14 In everyday life most persons living with T1DM deliver mealtime insulin boluses immediately prior to eating, hence for this study we chose to deliver the EB just prior to the test meal. However, the EB may be able to better control the postprandial glucose rise if delivered 20–30 min before a meal, and thus may be beneficial for certain meal types that result in prolonged glucose absorption.
Only a single meal type was used in this study. Altering the amount or type of carbohydrate may have impacted postprandial glycemic control in the study participants. Furthermore, fat and protein have been shown to impact postprandial BGLs.13 ,15 Smart et al found a higher rate of hypoglycemia after a low-fat meal.13 In this situation, there may be some benefit for an EB in preventing early postprandial hypoglycemia. Adjusting the fat and protein content of the study meal may have also impacted the postprandial glucose levels in the study.
The participants in this study had well-controlled T1DM and did not have any known complications of the disease. Extended insulin boluses have been recommended for persons with gastroparesis.2 Future studies including persons with known gastroparesis, or persons with higher HbA1c and therefore increased likelihood of complications of diabetes, may be useful to determine the utility of the EB in these patient groups.
In this study, we demonstrated that an extended insulin bolus was inferior to SB in controlling postprandial glycemia following a standard breakfast meal. Future studies comparing the EB and SB across a range of meal types and times may be performed to determine the utility of EB in clinical practice.
Acknowledgments
The authors thank the John Hunter Children's Hospital Paediatric Diabetes Team for assistance with carrying out the study. They also thank Professor Roger Smith of the Hunter Medical Research Institute, Mothers and Babies Research Group, Newcastle, Australia for advice and support. And particularly would like to thank all the study participants and their families.
Footnotes
-
Contributors PL, CS, and BK designed the study. PL, BK, CS, and CM recruited the patients. PL and MP conducted the study and collected the data. PM analyzed the data. PL wrote the first draft of the manuscript, which was edited by CS and BK. BK is the guarantor.
-
Funding This study was supported by a 2012 NovoNordisk Regional Support Scheme grant.
-
Competing interests PL receives PhD funding support by a 2011 NovoNordisk grant.
-
Patient consent Obtained.
-
Ethics approval University of Newcastle and Hunter New England Human Research Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.