Article Text

Abstract
Objectives We aimed to estimate the prevalences of diabetes and impaired fasting glucose (IFG) in a national sample in Peru and assess the relationships with selected sociodemographic variables.
Methods We estimated prevalence in PERUDIAB study participants, a nationwide, stratified urban and suburban population selected by random cluster sampling. Between 2010 and 2012, questionnaires were completed and blood tests obtained from 1677 adults ≥25 years of age. Known diabetes was defined as participants having been told so by a doctor or nurse and/or receiving insulin or oral antidiabetic agents. Newly diagnosed diabetes was defined as fasting plasma glucose ≥126 mg/dL determined during the study and without a previous diabetes diagnosis. IFG was defined as fasting plasma glucose of 100–125 mg/dL.
Results The estimated national prevalence of diabetes was 7.0% (95% CI 5.3% to 8.7%) and it was 8.4% (95% CI 5.6% to 11.3%) in metropolitan Lima. No gender differences were detected. Known and newly diagnosed diabetes prevalences were estimated as 4.2% and 2.8%, respectively. A logistic regression response surface model showed a complex trend for an increased prevalence of diabetes in middle-aged individuals and in those with no formal education. Diabetes prevalence was higher in coastal (8.2%) than in highlands (4.5%; p=0.03), and jungle (3.5%; p<0.02) regions. The estimated national prevalence of IFG was 22.4%, higher in males than in females (28.3% vs 19.1%; p<0.001), and higher in coastal (26.4%) than in highlands (17.4%; p=0.03), but not jungle regions (14.9%; p=0.07).
Conclusions This study confirms diabetes as an important public health problem, especially for middle-aged individuals and those with no formal education. 40% of the affected individuals were undiagnosed. The elevated prevalence of IFG shows that nearly a quarter of the adult population of Peru has an increased risk of diabetes.
- Adult Diabetes
- Impaired Fasting Glucose
- Epidemiology
- Population-Based Studies
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
The estimated prevalence of diabetes in Peruvian urban adults ≥25 years of age was 7%; 4.2% in known, and 2.8% in newly diagnosed diabetes.
Forty per cent of participants with diabetes were previously undiagnosed.
The prevalence estimates for metropolitan Lima have almost doubled in the past 7 years, increasing from 4.4% to 8.4%.
Diabetes was more frequent in middle-aged adults with no formal education and in those living in coastal cities.
The estimated national prevalence of impaired fasting glucose was 22.4%
Introduction
The International Diabetes Federation (IDF) estimates that in 2013, 381 million people had diabetes worldwide.1 Diabetes management is a challenge for health systems in developed countries and also a threat to developing countries. In South and Central America, the number of people with diabetes is expected to grow from 24.1 in 2013 to 38.5 million in 2035.1 The situation in Peru is especially difficult because the country is currently undergoing an epidemiological transition, with a high—and still unresolved—burden of communicable diseases such as tuberculosis along with increases in chronic non-communicable conditions, such as diabetes.
Current estimates of the national prevalence of diabetes in Peru are based on a few regional and/or small studies. The task is complicated by the country’s complex geographical characteristics comprising three natural regions (coast, highlands, and jungle) and the location of several important cities at altitudes from 0 to 4000 m above sea level. Peru also comprises several populations with very different regional diets, sociodemographic characteristics, and ethnic backgrounds. Also, differences in methodology and selection criteria for study populations, and the cities included in local studies, do not permit a reliable estimate of the national prevalence of diabetes. Most important, no reliable baseline data are available to assess whether the frequency of diabetes really is increasing over time.
In 1997, our study group estimated the prevalence of diabetes in a cross-sectional study that enrolled a probabilistic random sample of residents in four cities, including one district of Metropolitan Lima, Piura (on the coast), Huaraz (in the highlands), and Tarapoto (in the jungle). The prevalence of diabetes in these cities was found to be 7.6%, 6.7%, 1.5%, and 4.0%, respectively.2 A nationwide, self-reported, non-random survey, Risk Factors of Cardiovascular Diseases on Peru (TORNASOL), conducted in 2003–2005 estimated that the prevalence of diabetes in people ≥18 years of age was 4.3%, 2.1%, and 3.9% in representative coastal, highlands, and jungle cities, respectively.3 The Cardiovascular Risk Factor Multiple Evaluation in Latin America (CARMELA), conducted in 2003–2005, reported that the diabetes prevalence in a single city (Lima) was 4.4% (95% CI 3.4% to 5.4%). The estimate was based on fasting plasma glucose concentrations in a probabilistic random sample of people 25–64 years of age.4 Thus, none of the previous studies has been simultaneously nationwide in scope, population-based, and probabilistic.
PERUDIAB is a nationwide, population-based, three-wave longitudinal, probabilistic study that is expected to answer important questions related to diabetes, obesity, hypertension, and kidney disease in the Peruvian population ≥25 years of age. This study reports the estimated diabetes and impaired fasting glucose (IFG) prevalence in a representative cross-section of Peruvian urban and suburban adults.
Methods
Participants, sample size, and study setting
PERUDIAB used the national sampling framework developed by the Peruvian National Institute for Statistics and Informatics (INEI), which is based on 2007 National Census data and cartographic information. The study enrolled a stratified, three-stage, cluster-panel random sample designed to represent both urban and suburban populations. The first wave (cross-section) of this longitudinal study was conducted during 2010–2012, the second wave started in 2014, and the start of the third wave is planned for 2016. People living in rural areas, including approximately 15% of the Peruvian population, were not enrolled in this study because they lived in isolated geographical areas that are very difficult to access. The primary sampling units were clusters of approximately 120 households, secondary sampling units were individual households, and tertiary sampling units were the household members who were interviewed.
The sample size was calculated using standard random sampling procedures for each study domain with an adjustment for the design (cluster) effect. We assumed separate a priori diabetes prevalence rates of 8% for the capital city and 5% for the subdomain that included the rest of the country in order to obtain reliable estimates that were within precision limits of 2% and 1.5%, respectively. Correcting for the design effect and non-response rates yielded a required sample size of 1230 households for the capital city and 850 for the subdomain. After ensuring that at least one eligible adult ≥25 years old was living in the selected household, random selection of participants was conducted based on the nearest birthday date.
Numerous climatic and logistical difficulties including a heavy rainy season made access to several districts difficult. Consequently, 83% of the samples were collected between 2010 and the first half of 2011, but 16% could only be collected after the end of winter in 2012. A few samples that were collected in December 2009 were considered valid for inclusion in the statistical analyses. Finding suitable healthcare workers permanently living/working in each district—in order to maximize the response rate—proved to be quite challenging, and that prolonged the time needed to complete the fieldwork beyond the planned date.
Participants
Eligible participants ≥25 years of age of either sex and living in the sampled household, including in-house paid or unpaid service personnel. The household definition was the same as that used by the INEI. Thus, shelters housing up to nine people as well as people who were not family members but who had lived in a household for the prior 30 consecutive days were included in the selection process. Participants with previously diagnosed or known mental disorders (according to family members) and pregnant women were excluded. The study obtained full ethical approval from an accredited ethics committee, and signed informed consent was required for inclusion in the study.
Questionnaires
Questionnaires were designed and tested in a pilot study conducted on a group of participants who were not included in the final assessment. Households were visited one or more times as needed in order to complete the questionnaires. In order to maximize the response rate, the visits and interviews were performed by trained healthcare workers living/working in the local health center. Completed questionnaires were validated in telephone interviews with selected participants. If telephone communication was not possible, supervising personnel who were unaware of the results obtained in the previous visit went to the household.
Blood samples
At the first household visit, participants were asked to fast overnight for 12 h before blood collection scheduled for the next morning. Fasting was confirmed verbally by the participants immediately before collecting the blood sample and again when they were given the blood glucose results. If fasting could not be confirmed, then a new specimen for repeat testing was obtained at a later date. Blood samples were collected in tubes (Terumo Venosafe Glycaemia) containing citrate buffer, NaF, and disodium EDTA, which stopped glucose consumption by red blood cells.5 Additionally, most samples were centrifuged and plasma separated at the nearest available laboratory facility, usually within 2 h. The samples were then sent to central laboratories using the fastest available transport and under cold chain conditions. Samples were processed using glucose oxidase spectrometric assays with semiautomated procedures.
Diabetes and IFG
Participants with known diabetes had been told by a physician or a nurse that they had the condition and/or were being treated with insulin or oral antidiabetic agents. Participants with newly diagnosed diabetes had a fasting blood plasma glucose ≥126 mg/dL during the study and had not previously been told that they had diabetes. IFG was defined as a fasting plasma blood glucose of 101–125 mg/dL. Oral glucose tolerance tests (OGTTs) were not performed.
Data processing and statistical analysis
Data were captured from questionnaires and validated using Optical Markup Recognition (OMR) software (Remark Office OMR, Gravic, Inc). For a few non-structured data items, double data entry was done in Microsoft Excel work sheets, and checked for consistency before importing the data set into Stata/SE V.11.0 software (StataCorp LP, College Station, Texas, USA).
A poststratification procedure was performed to approximate the age and sex composition of data included in the 2007 Peruvian National Census, and to account for the non-response rate. All prevalence estimations and comparisons were performed using complex survey commands for logistic regression models taking into account the stratification of the primary sampling units (ie, city, town, or human settlement size) and household clustering. Effect modifiers were assessed, and interaction terms were tested using design-adjusted Wald tests for linear combination of coefficients. Logistic regression response surface models using linear, quadratic and corresponding interaction terms were fitted. Non-parametric Spearman rank correlation coefficients were used to determine bivariate correlations. p Values <0.05 were considered significant.
Results
A total of 1677 surveys were collected from the planned sample of 2080 eligible participants, a response rate of 80.6%. Data from the 2007 national census indicated that the study sample was representative of an urban and suburban population of approximately 10 861 400 people of both sexes and ≥25 years of age. The main reasons for not being included in the survey were inability to locate or meet with the selected participant, not agreeing to participate in the survey, and inability to validate the completed questionnaire and/or biological sample requirements.
The national prevalence of diabetes (table 1) was estimated as 7.0% (5.3% to 8.7%), indicating an affected population of approximately 763 600 people among the 10 861 400 individuals living in the urban and suburban areas that were sampled. The prevalence of known diabetes was estimated as 4.2%, and that of newly diagnosed diabetes was estimated as 2.8%. The estimated prevalence of IFG was 22.4%.
Prevalence of diabetes and impaired fasting glucose by study domains, natural regions, and selected demographic variables
The estimated prevalence of diabetes in metropolitan Lima (table 1) was higher, but not significantly different from the estimated prevalence in the rest of the country (8.4% vs 6.0%; p=0.16). However, prevalence estimates across the Peruvian natural regions (coastal, highlands, and jungle) were different. The prevalence was significantly higher in coastal populations than it was in both highlands (8.2% vs 4.5%; p=0.03) and jungle (8.2% vs 3.5%; p=0.02) populations. Prevalence estimates for the highlands and in the jungle were not significantly different (4.5% vs 3.5%; p=0.62). However, a statistically significant pattern of decreasing prevalence was discernible across the three populations (8.2% vs 4.5% vs 3.5%; p=0.02, logistic regression test for trend). A similar pattern was evident for IFG.
The diabetes prevalences in men and women were not different (7.01% vs 7.04%, respectively; p=0.99), but IFG was found more frequently in men than in women (28.3% vs 19.1%, p<0.001). Diabetes prevalence increased with age (p<0.001) and then decreased in the 65+ age group. No interaction was found between age and sex (p=0.52). There were no significant differences between age groups in prevalence of IFG (p=0.061, table 1).
The prevalence of diabetes was higher in people with no formal education than in those who had attended school. However, as noted below, educational level was negatively correlated with age, that is, younger people had higher educational levels (p<0.001, Spearman rank correlation coefficient). No differences in IFG prevalence were found among educational levels (p=0.06, table 1).
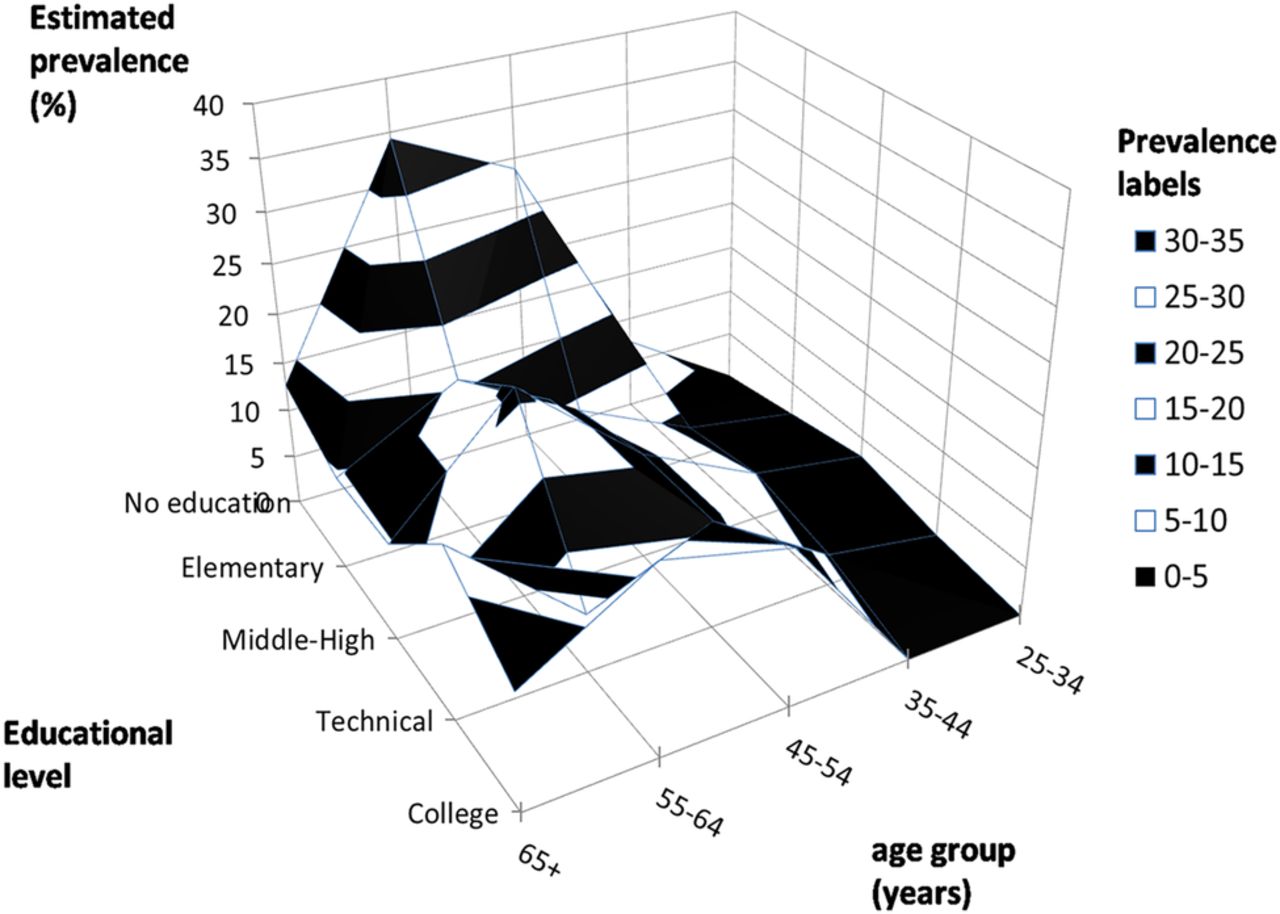
To assess the distribution of diabetes by age, gender, and educational level, logistic regression response surface models including main and interaction terms for age, age2 (quadratic term), gender, educational level, and study regions (Metropolitan Lima, coastal, highlands, and jungle domains) was performed, and the resulting final best-fitting model included age, age2, educational level, and the age by educational level interaction term (table 2). The complex relationships between the prevalence of diabetes, age, and educational level show (figure 1) that in addition to the linear and quadratic relationship with age, the relationship was dependent on the particular combination of age and educational level (ie, the interaction term for age and educational level was statistically significant).
Logistic regression response surface model for diabetes and the interaction of age and educational level interaction, adjusted for sex and region

{kind=link}
Diabetes prevalence and its relation to age and educational level. Logistic regression response surface model shows a complex relationship between age and educational level groups. Diabetes was more prevalent in middle-aged individuals with no formal education.
Discussion
The overall prevalence of diabetes in this study was 7.0%. According to the Sixth (2013) Edition of the IDF Atlas,1 the prevalence in Peru was 4.3% of the adult population between 20 and 79 years of age, including those living in rural areas. The 2014 edition of the IDF Atlas, which was published after we completed our study, updated the national estimate to 6.1%.6 The IDF estimate takes into account both the rural population and people 20–24 years of age, neither of which were included in our sample.
Importantly, the IDF methodology for estimating the prevalence of diabetes in individual countries, as previously described by Guariguata et al,7 allows for comparing, and adjusting, prevalence rates across countries. Consequently, taking into account those countries with enough data to estimate their national prevalence and excluding those countries whose prevalence was extrapolated from similar or neighboring countries, the IDF-adjusted estimate for Peru is 6.5%.8 This places Peru in a low-prevalence group of South and Central American countries, the others being Argentina (5.7%), Ecuador (5.9%), Venezuela (6.9%), and Bolivia (7.3%). Countries in the region comprising an upper-prevalence group include Puerto Rico (13%), Nicaragua (12.5%), the Dominican Republic (11.4%), and Chile (11.2%), all with prevalences above 10%. The prevalence in Peru is below that of the USA (9.4%) and other countries in North America and the Caribbean region, most of which have a diabetes prevalence greater than 10%, including Mexico (12.6%). Finally, our prevalence estimate is similar to that in most Southeast Asian countries, including Bhutan (5.83%), Bangladesh (6.89%), and Sri Lanka (7.8%), and also most European countries, which rarely exceed 10%. The prevalence of diabetes in Peru is well below compared with countries in the Middle East and North Africa, which have some of the highest prevalences of diabetes in the world, including 23.9% in Saudi Arabia, 23.1% in Kuwait, and 21.9% in Bahrein. This does not mean that diabetes is not a serious problem in Peru, but that this is the right time to prevent further increase in prevalence.
The increased prevalence found in this study, compared with previous estimates in Peru, could be explained by several factors including the adoption of new lifestyles9 ,10 in parallel with the strong economic growth our country has experienced in the past 20 years. It should be noted that in 2005, 35% of Peruvians older than 19 years of age were overweight and 17% were obese,11 but by 2013, the corresponding percentages in those older than 14 years of age were 33.8% and 18.3%.12 Other factors affecting the increase in diabetes prevalence could be differences in the ethnic and sociodemographic characteristics of the studied populations.13 ,14 Finally, some previous estimates were determined in relatively small studies and/or in only a few cities.2 ,15 ,16 They were also limited by not being nationwide,2 ,15 ,17 ,18 probabilistic,3 ,19 or population-based.15 ,19 The only national, probabilistic, population-based, diabetes prevalence estimate—of 2.8% in 2005—was reported in 2006 by a government health agency,11 but its diagnostic criteria (ie, fasting plasma glucose >100 and having been previously diagnosed or fasting plasma glucose ≥200 and not having been previously diagnosed or a history of pharmacological treatment) were different from ours. Thus, no firm comparisons can be made to assess the change in national prevalence over time.
An important finding of our study was that, using the CARMELA study4 as a reference, the estimated prevalence of diabetes in metropolitan Lima almost doubled in 7 years, increasing from 4.4% in 2004 to 8.4% in 2011. We see a similar increase using the FRENT study as a reference. It estimated the prevalence of diabetes in metropolitan Lima as 3.9% (95% CI 3.0% to 4.8%) in 2006 for individuals 15–94 years of age and 4.4% in those 20–94 years of age.18 Therefore, we might expect an even higher prevalence estimate if the analysis had been limited to those 25–94 years of age, the age group that matches our sample. It is important to note that in those studies, as in PERUDIAB, no rural population of any significant size was involved. The three studies used the same criteria to define diabetes, allowing an assessment of the trend in increased prevalence over time. Overall, our analysis suggests a rapid increase of the prevalence of diabetes in both the capital city and the country.
Consistent with studies carried out in low-income and middle-income countries,20 we found the highest prevalence of diabetes was in the middle-age category. The IDF reports that this age category comprises the greatest number of people living with diabetes, with more than 80% living in low-income and middle-income countries in 2014.8 This is in sharp contrast with high-income countries, where the majority of people with diabetes are older.21
In our study, 40% (95% CI 32.6% to 43.6%) of people with diabetes were undiagnosed. However, no local reports are available for comparison. Using the figures available in the IDF 2014 update,8 our estimates are above the mean percentage (27%) estimate for other countries in South and Central America, above the mean estimate for North America and the Caribbean (27%), and similar to that for Europe (34%). It is below the mean estimate for countries in Southeast Asia (53%) and the Middle East and North Africa (50%).
Our study showed that 22.4% of the entire study population and 24.9% of those in Lima had IFG. Men were more frequently affected than women with a ratio of approximately 2:1. The prevalence of IFG was lowest in those 25–34 years of age and was approximately 22% across all educational levels. Our estimate for metropolitan Lima is higher than that found in the CARMELA study, which reported figures lower than 3%.4 Furthermore, 3 years later, the FRENT study reported a 7.8% (95% CI 6.6% to 9.1%) prevalence of IFG in their study population. However, as has been previously discussed, a higher estimate would be expected in both studies if their age groups matched ours. In addition, our estimates are higher than the 25.3% prevalence reported in New York City22 and higher than the 16.7% reported in the UK.23 IFG is a risk factor for the future occurrence of diabetes, which would mean that almost one-third of the Peruvian adult population is likely to be affected by glucose metabolism disorders, including diabetes.
Previous studies in our country,2 ,3 ,19 although conducted using different methodologies, consistently showed descending estimates for the prevalence of diabetes in the coastal, jungle, and highlands regions, in that order. The low prevalence found in the highlands could be explained by a greater sensitivity to insulin due to hypoxia in high altitude zones.13–16 ,24–27 However, our results show for the first time that the prevalence of diabetes in the highlands has increased compared with that previously reported for the jungle. Furthermore, a logistic regression test for trend for the new sequence (ie, coast, highlands, and jungle) was statistically significant, and the estimates of the prevalence of diabetes between these two regions were not statistically different (ie, 4.5% vs 3.5% for the highlands and jungle regions, respectively). If confirmed, this finding would indicate that new lifestyles are already affecting the metabolism patterns in the highland populations.
Our study has several limitations. First, we did not repeat the fasting blood glucose testing in all study participants as required by the American Diabetes Association for clinical purposes.28 However, the WHO considers that for epidemiological purposes, a single fasting plasma glucose estimation is acceptable.29 Second, we did not perform confirmatory OGTTs. We may thus have underestimated the true diabetes prevalence, as it has been reported that the OGTT may detect more participants with diabetes than fasting plasma glucose testing.30 ,31 Third, due to financial constraints, our study did not include rural areas, which represent approximately 15% of our national population. However, it is expected that prevalence is lower in rural than in urban areas, and that the impact on the overall estimation was small. Fourth, we assumed most of the detected cases were type 2 diabetes. However, even though our study participants were all ≥25 years of age, we did not determine whether they had type 1, 2 or latent autoimmune diabetes in adults (LADA). According to the IDF,8 Peru has one of the lowest prevalence rates in the world for type 1 diabetes (0.5 cases per 100 000 population). We are not aware of any report on LADA in our country, and this is a pending research agenda.
Overall, our analysis suggests a rapid increase in the prevalence of diabetes in our capital city and in other regions of our country, and suggests the need for a health plan with a strategy based on screening and early diagnosis, aiming to avoid the social and economic consequences of this disease, in accordance with WHO and United Nations recommendations.32 The PERUDIAB study is an ongoing effort to gather epidemiological support to enable the design of an evidence-based policy for approaching this serious public health problem in Peru.
Acknowledgments
The PERUDIAB is an epidemiological research project supported by Sanofi Peru. The PERUDIAB authors express their gratitude to all the dedicated field workers involved in this project.
References
Footnotes
Contributors SNS, MER, AJA, CAM, and EH conceptualized and designed the study, contributed to the interpretation of the results, were involved in critical revisions, and have read and approved the final manuscript. MER wrote the analysis plan, conducted the statistical analyses, and drafted the manuscript. CAM reviewed the study materials and questionnaires and trained the field workers for the pilot phase. SNS is the guarantor of this work.
Funding This study was approved by the ethical committee of San Martin de Porres University, Lima, Peru.
Competing interests SNS has received honoraria from Sanofi for participation in advisory/consultant activities. He has also provided ad hoc consultancy to Novo Nordisk. EH and CAM are employees of Sanofi Peru.
Ethics approval This study was approved by the ethical committee of San Martin de Porres University, Lima, Peru.
Provenance and peer review Not commissioned; internally peer reviewed.
Data sharing statement No additional data are available.