Article Text

Abstract
Objective We aimed to assess the accuracy and safety of presently available methods of estimating starting basal insulin rates for patients with type 1 and 2 diabetes, and to compare them against an empirically derived standard basal rate and a newly developed regression formula.
Research design and methods Data on 61 patients with type 1 diabetes on continuous subcutaneous insulin infusion (CSII) therapy and 34 patients with type 2 diabetes on CSII were reviewed. Patient data were first analyzed for correlations between initial patient parameters and final basal rates. Starting basal rates were then retrospectively calculated for these patients according to the weight-based method (WB-M), the total daily dose (TDD) of insulin method (TDD-M), a flat empiric value, and a new formula developed by regression analysis of clinical data. These 4 methods were subsequently compared in their accuracy and potential risk of hypoglycemia.
Results For type 1 diabetes, patient weight and TDD of long-acting insulin correlated with final basal rates. Both the regression formula and the TDD-M appeared safer than the WB-M and empirical estimates. For type 2 diabetes, only patient TDD of long-acting insulin correlated with final basal rates. The regression formula was significantly more accurate for patients with type 2 diabetes overall, but the TDD-M estimate was marginally safer.
Conclusions The pre-existing TDD-M was found to be the safest presently recommended estimate of initial basal rates for pump initiation in both type 1 and 2 diabetes. The best-fit regression was found to have potential use for type 2 CSII initiation.
- Insulin Pump
- Insulin Treatment in Type 2 Diabetes
- Basal
- Insulin Dose Management
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
Using multiple regression analyses, it was confirmed that both weight and total daily dose (TDD) of long-acting insulin correlated with the final titrated basal rate for type 1 diabetes, but only TDD of long-acting insulin correlated for type 2 diabetes.
The present method of estimating basal rate from the TDD of insulin was found to be the most effective for patients with type 1 and 2 diabetes when compared with the weight-based formula or use of an empiric value.
The regression formula generated from the data was the most accurate in estimating type 2 basal rates; there is potential for the utilization of this method in type 2 insulin pump initiations.
Introduction
The management of diabetes mellitus has evolved with the advent of new technologies developed for more effective and controlled delivery of exogenous insulin. For patients with type 1 diabetes, continuous subcutaneous insulin infusion (CSII) therapy, otherwise known as insulin pump therapy, is becoming more accessible and established, having been in clinical use for decades.1 ,2 A recent study of CSII in patients with type 2 diabetes has also shown clinically significant improvements in this group.3 In light of the perceived benefits of this new therapeutic technique, the transition period between old and new methods of insulin administration warrants further attention.
While there is evidence to support the advantages of CSII over multiple daily injections (MDIs),4–6 the initiation step in insulin pump therapy presents itself as a challenge.7 Ideally, a patient's initial basal rate estimate should be conservative enough to minimize any risk of hypoglycemia, while being sufficiently high to improve glycemic control. At our center, as part of a randomized control trial testing insulin pump therapy for patients with type 2 diabetes, we encountered an approximate 20% incidence of hypoglycemia during pump initiation. With this in mind, we sought to investigate presently established guidelines for basal rate estimations.
Current strategies for determining appropriate starting basal rates involve calculations utilizing the total daily dose (TDD) of both short-acting and long-acting insulin taken by MDI or a patient's bodyweight.8–10 While these formulas are regularly used, there is a lack of literature supporting their efficacy.11–13 Some studies have attempted to improve on these basal estimation formulas,14 ,15 but their suggestions have yet to be incorporated into clinical guidelines.
The objective of this retrospective study was to provide a preliminary evaluation of the accuracy and safety of the pre-existing weight-based method (WB-M) and TDD of insulin method (TDD-M) estimates, a new empirically derived starting basal rate of 0.8 U/h, and a new formula developed by regression analysis of clinical data in CSII patients with type 1 and 2 diabetes.
Materials and methods
Data collection and subgrouping
Retrospective chart data on 61 adult patients with type 1 diabetes and 34 adult patients with type 2 diabetes were collected from a private diabetes clinic. To qualify for inclusion, patients must have utilized insulin pump therapy for greater than 3 months, with records of glycated hemoglobin (HbA1c), insulin dosage and weight available from before and after pump initiation. Only patients with type 1 diabetes with an HbA1c ≤7.5% were eligible for consideration. Baseline characteristics of the patients with type 1 and 2 diabetes are summarized in table 1.
Mean baseline characteristics of the type 1 and 2 diabetes patient groups. Error is calculated and reported in 95% CIs
Determining basal insulin infusion rates
The present scientific and industry consensus on insulin pump initiation supports the use of two formulas as guidelines for a patient's basal insulin infusion rate.10 ,16 In accordance with the judgment of a healthcare professional, these estimates aid in establishing an initial basal rate that is titrated further over the course of pump therapy.
The current formulas for estimating basal rates in adult patients with type 1 diabetes, in units per hour, using weight (in kg) or TDD of insulin are as follows:
 For the purposes of this study, an empirically derived standard basal rate of 0.8 U/h was also included in type 1 comparisons. This was based on the observation that many of these patients’ titrated basal rates appeared to converge on this single value.
For the purposes of this study, an empirically derived standard basal rate of 0.8 U/h was also included in type 1 comparisons. This was based on the observation that many of these patients’ titrated basal rates appeared to converge on this single value.
In order to evaluate the effectiveness of these pre-existing formulas and to generate a new formula for estimating basal insulin infusion rates, we generated a final basal rate for each patient from the study data. The basal rates for the patients reviewed in this study were estimated at the time of pump initiation using one of the two pre-existing formulas. These initial basal rates were adjusted incrementally over at least 1 month through weekly appointments with a healthcare professional and continued monitoring and feedback. The final basal rate was calculated as a daily average of each patient's most recent basal rates, and we assumed that this basal rate approximated a therapeutic end goal for pump initiation. The type 1 group had undergone CSII therapy for 41 months on average, while all type 2 data were collected after 4 months. Within these timeframes, there was ample opportunity to closely titrate each patient's basal rate.
For patients with type 1 diabetes, only those with a final HbA1c ≤7.5% were considered, with a mean HbA1c of 6.9%±0.1%. Owing to sample size restrictions, all patients with type 2 diabetes were included irrespective of their final HbA1c, with a mean HbA1c of 8.1%±0.5%. The underlying assumption of this restriction is that an HbA1c near therapeutic goals reflects a more ideal final basal rate.
Statistical methods
Multiple regression analyses with least-squared percentage error were performed to determine statistically significant correlations between prepump initiation parameters and final basal rates for each group. Subsequent linear regressions, factoring in only the parameters deemed significant, were used to calculate new equations for estimating basal rates for the type 1 and 2 diabetes groups.
The newly generated regression formulas were then compared with the pre-existing basal rate formulas by assessing the deviations between each estimate and the final titrated basal rate of each patient. To provide a measure of the overall error of each method, we calculated the median absolute percentage error to represent the proportional difference between each of the four methods and the final basal rate. To compare safety of each method, we calculated the median percentage error, a measure of each method's bias toward underestimating a patient's insulin dosage (negative values indicate underestimation). For safety analysis, we also tabulated the frequency that each formula estimated a patient basal rate that was 10%, 20%, and 30% higher than the final basal rate in our data.
To account for the non-normal data observed, multiple Wilcoxon signed-rank tests were used to test for significant differences between the estimate methods. To control the risk of inflated type I error that accompanies this method, a sequential Bonferroni correction was performed as necessary to adjust accepted p values.17 All statistical analyses were carried out using the statistical software packages R and JMP.
Results
Type 1 diabetes group
A multiple regression analysis was run on the type 1 final basal rates, factoring HbA1c, weight, TDD of long-acting insulin, TDD of short-acting insulin, and age. It was found that HbA1c, weight and TDD of long-acting insulin positively correlated to clinical basal rates (R2=0.556; p<0.05, <0.01, and <0.001, respectively), whereas patient age and TDD of short-acting insulin showed no significant relationship.
The type 1 final basal rates were used to derive a linear regression using weight (kg) and TDD of long-acting insulin (R2=0.507; p<0.005 and <0.001, respectively), which approximates to:
To assess the accuracy of the regression equation, the pre-existing formulas, and the empirical value, the absolute differences between each method's basal rate estimate and the final basal rate were calculated and compared (figure 1A). The median absolute percentage error was 11.9% for the linear regression formula, 17.5% for the TDD-M, 18.6% for the WB-M, and 26.5% for the empiric value. The regression formula was found to be significantly more accurate than the WB-M and empirical estimates (p<0.01 and <0.001, respectively), but not the TDD-M (p=0.117). The TDD-M and WB-M estimates were not found to be significantly more accurate than the empiric value, or each other.
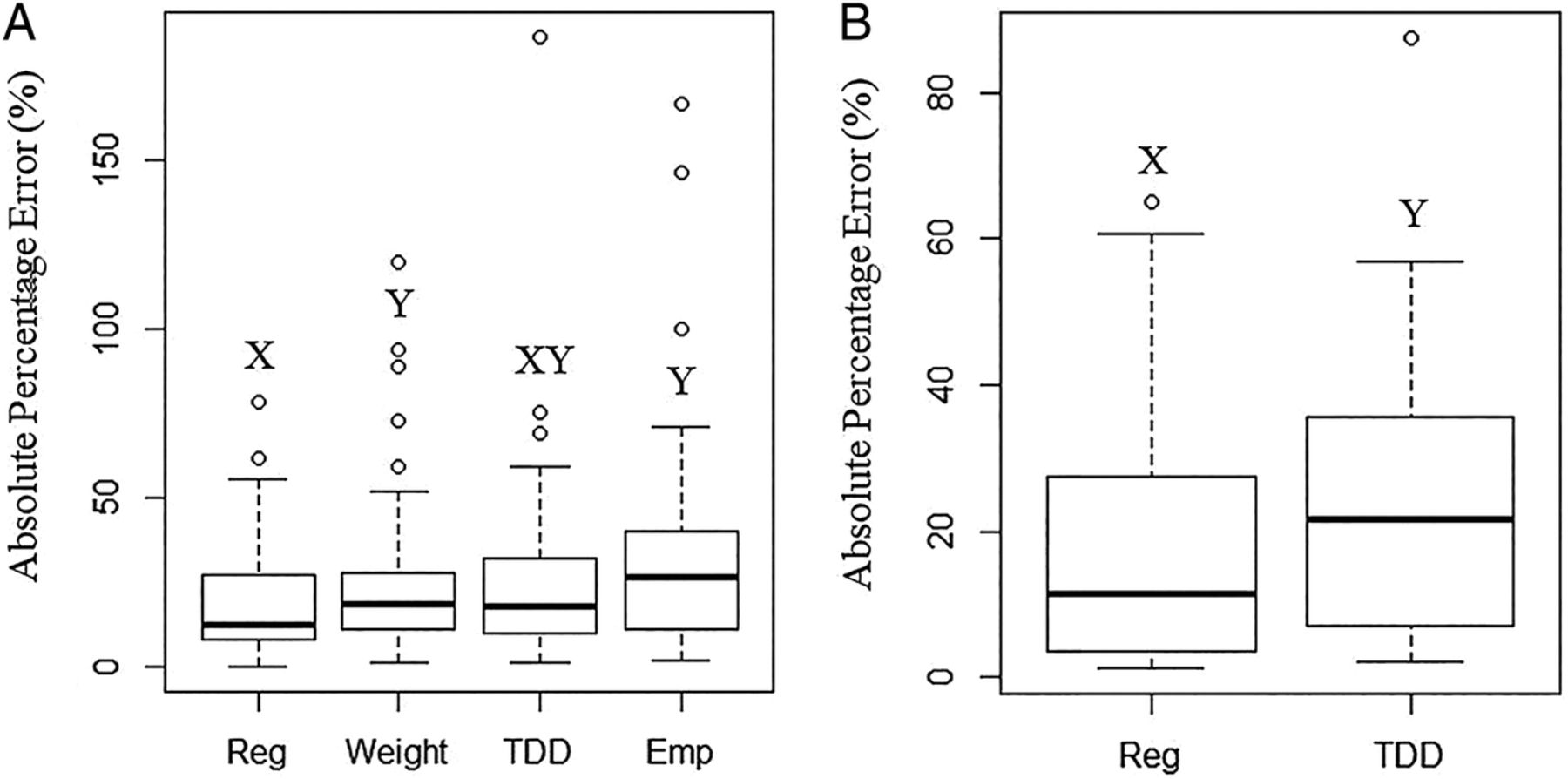
Distribution of the absolute percentage differences of each basal rate estimate to final basal rates. Estimate methods include a regression, weight formula, total daily dose (TDD) of insulin formula and an empirical value. Different letters denote a significant difference between estimates. (A) Patients with type 1 diabetes (n=61). (B) Patients with type 2 diabetes (n=34).
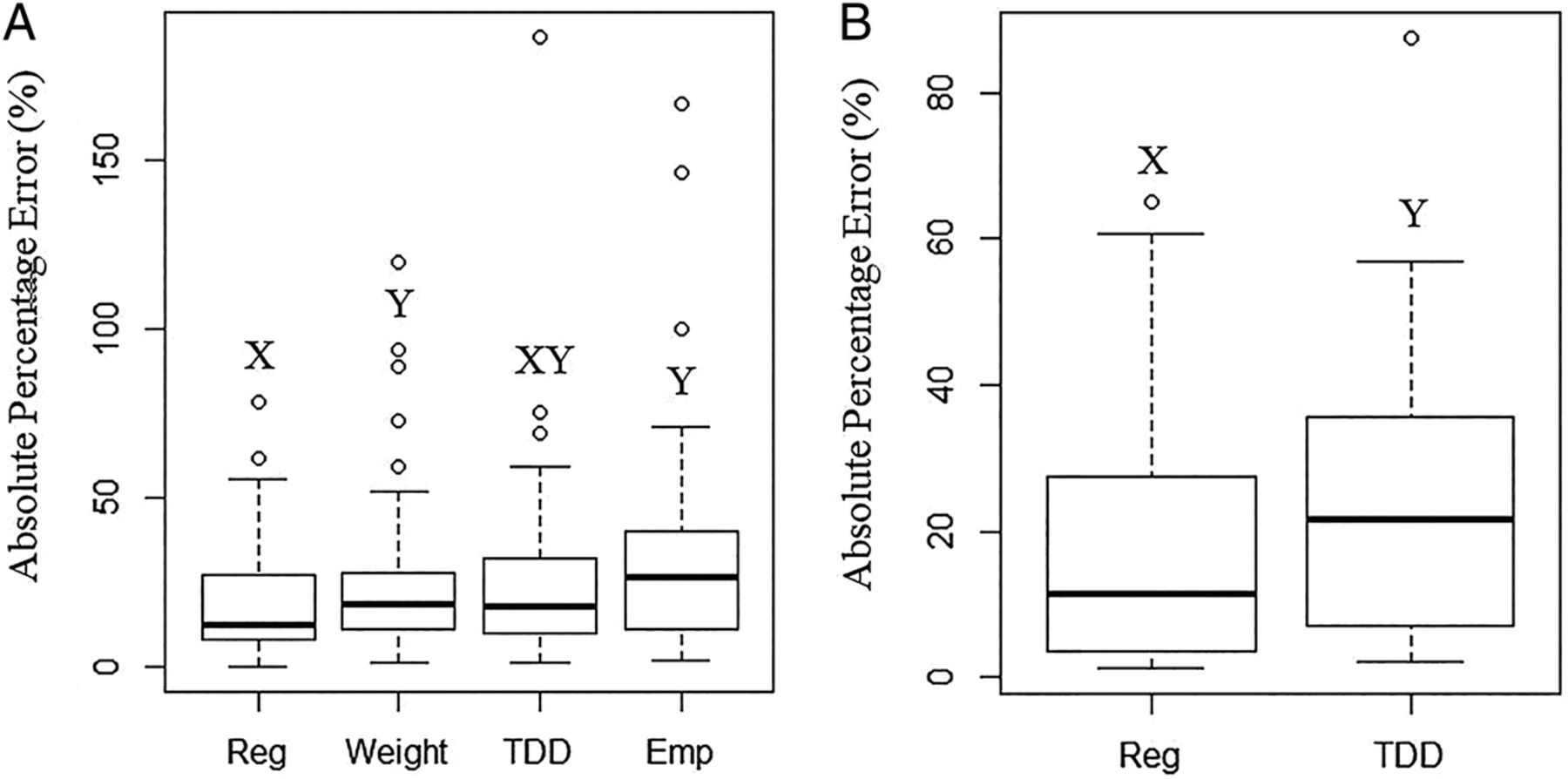
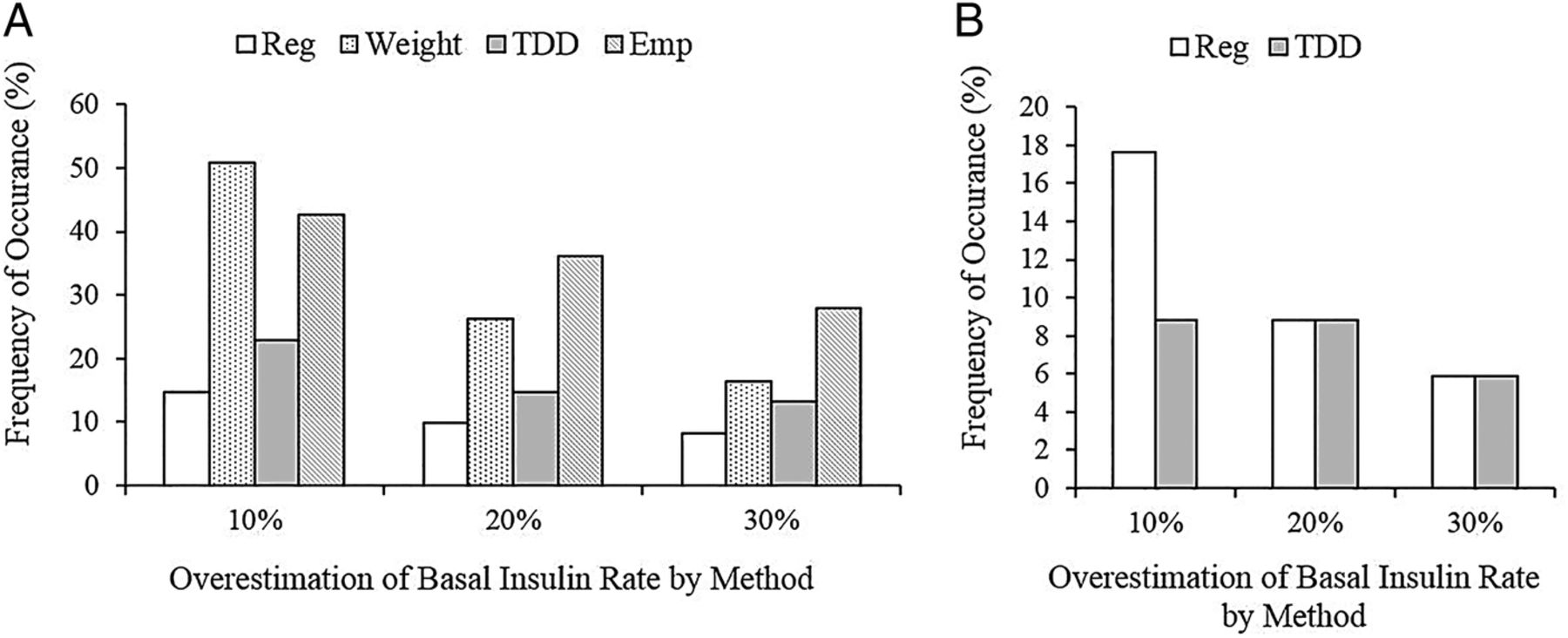
To assess the relative safety of each formula, basal rate estimates were analyzed for their potential risk of hypoglycemia (figure 2A). Both the regression and TDD-M tended to underestimate each patient's basal rate, with a median error of –9.17% and −10.06%, respectively, while the empiric value overestimated by 6.67%. The WB-M overestimated the greatest, with a median error of 11.1%. The regression error was statistically different from both WB-M and empirical estimates (p<0.001 and <0.001); the TDD-M error was similarly different from both weight and empirical estimates as well (p<0.01 and 0.014). No significant difference was observed between the regression and TDD-M formulas nor the WB-M and empirical estimates. Observational evidence of the overestimation frequency of each method is shown in figure 3A. Although the distribution of overestimation occurrences reflects the same trend observed in the study errors, it is noted that all methods generated a major overestimation in a minority of patients.

Distribution of the percentage differences of each basal rate estimate to final basal insulin rates. Estimate methods include a regression, weight formula, total daily dose (TDD) of insulin formula and an empirical value. Different letters denote a significant difference between estimates. (A) Patients with type 1 diabetes (n=61). (B) Patients with type 2 diabetes (n=34).

{kind=link}
{kind=link}
{kind=link}
Frequency of potential risk of hypoglycemia for each estimate method, defined as a percentage difference between the estimate and final basal rate. Estimates include a regression, weight formula, total daily dose (TDD) of insulin formula and an empirical value. (A) Patients with type 1 diabetes (n=61). (B) Patients with type 2 diabetes (n=34).
Type 2 diabetes group
For patients with type 2 diabetes, we similarly assessed the correlation between weight, TDD of long-acting insulin, TDD of short-acting insulin, and age against the final basal rates via multiple regression. It was found that only TDD of long-acting insulin was correlated with final basal rate (R2=0.558; p<0.001). A simple linear regression gives the formula:
There is no specific formula widely recommended for estimating the basal rate for patients with type 2 diabetes initiating pump therapy; however, we included the pre-existing type 1 TDD insulin formula for comparison.
Comparing accuracy between methods, the median absolute percentage error was 11.4% for the regression formula and 21.6% for the TDD-M (figure 1B). These absolute errors were shown to be statistically significant (p=0.0341). Both methods were shown to exhibit a general underestimation bias, with a median error of −4.0% for the regression formula and −13.2% for the TDD-M (figure 2B). Again, this was shown to be a statistically significant difference (p=0.0172). Observational evidence of the overestimation frequency of each method is shown in figure 3B; the regression formula was shown to have a higher frequency of minor overestimations when used to predict the patient sample.
Discussion
For type 1 diabetes, the basal rate estimation formula based on TDD-M is the safest pre-existing estimate for pump initiation:
For type 2 diabetes, the use of our new regression formula provided an overall more accurate alternative to the TDD formula:
Our analysis of patients with type 1 diabetes showed that weight and TDD of long-acting insulin were found to be correlated with final basal rate, providing support for the use of present formulas that use these parameters in the estimation of starting basal rates.16 ,18 Our finding that TDD of short-acting insulin was not statistically correlated with the final basal rate could be explained by the variability of its usage as both a bolus and correctional dose (generally used in patient management). Basal dosing, in comparison, may be dependent on more stable factors such as bodyweight.
When retrospectively compared with both the weight formula and our flat empiric value, the TDD-M initial basal rate estimation was shown to be the safest formula presently recommended in CSII initiation guidelines for patients with type 1 diabetes.10 Although the TDD-M was not found to be significantly different from the weight (WB-M) and empirical estimates in terms of its absolute error, it was found to be more biased toward underestimation of the basal rate. Theoretically, this bias would be expected to reduce a patient's risk of hypoglycemia.
For patients with type 2 diabetes, only TDD of long-acting insulin was shown to correlate with a patient's final basal rate, making the TDD-M the only pre-existing estimate method supported, in part, by these initial study findings. Weight was not found to correlate with final basal rates, possibly due to confounding factors such as insulin resistance.
The regression formula derived from the data shows a high degree of utility in estimating basal rates for patients with type 2 diabetes. The regression formula was shown to be the more accurate overall estimate when compared with the TDD-M, although it exhibited a slightly higher tendency toward overestimation, and therefore potential hypoglycemia. At this time, as our study found no support for the use of the WB-M estimate in initiating patients with type 2 diabetes on pump therapy, there appears to be potential for the use of a new regression formula in tandem with the TDD-M.
These results are only to be considered as the product of a preliminary investigation; naturally, the adoption of a new regression formula would require a larger and more robust study before any recommendations for clinical practice could be made. Although the study was powerful enough to detect differences between estimate methods in patients with type 2 diabetes, the smaller sample size and heterogeneous nature of the patient pool limits the widespread conclusions that can be drawn from the data. Furthermore, it is important to recognize that the regression formulas discussed in this study were generated from the patient data; therefore, they would be expected, intrinsically, to provide better estimates than more generalized formulas. With preliminary evidence suggesting there is room for improvement over pre-existing estimates, further development of these regression formulas may yield a new clinical tool for CSII initiation in both patients with type 1 and 2 diabetes. Better calibrated estimate methods may be safer and require less intervention during the time of pump initialization, improving patient satisfaction and overall treatment efficiency for this period.
This study has several limitations. First, it is a retrospective study, and the comparison between basal estimates is a hypothetical extrapolation of each patient's initial prepump characteristics. This study also assumes that each patient's final basal rate represents their true, stable, therapeutic goal. For patients using multiple basal rates per day, the final basal rate was averaged into one value for the purposes of the analysis, potentially obscuring a nuance in pump therapy that may have an important influence on HbA1c or hypoglycemic events. The dawn phenomenon, well established in CSII research,19 ,20 is recognized as one such challenge in pump patient management.
The low R2 values of the regression analyses and the high degree of variation observed in each estimate method for both patient groups suggest that basal insulin requirements are part of a complex physiological mechanism that is not easily predicted. The observation of frequent basal rate overestimations in all methods and major inaccuracies in a small number of outliers underscores the importance of expert judgment when determining initial basal rates. Basal insulin rate estimators are provided only as a tool; with knowledge of each estimate method's strengths and weaknesses, trained healthcare professionals are better equipped to safely bridge the gap between old and new insulin therapies.
Acknowledgments
Portions of this study have been presented in abstract form at the International Diabetes Federation World Diabetes Congress, Vancouver, Canada, on December 2015.
References
Footnotes
Contributors HDT is the guarantor of this work and, as such, had full access to all of the data in the study and takes responsibility for the integrity of the data and accuracy of the data analysis. HDT, NC and DS wrote, reviewed and edited the manuscript. NC collected data, with assistance from JAP and BP. JAP, BP, HGT, AW and MP reviewed/edited the manuscript. All authors read and approved of the final manuscript.
Competing interests None declared.
Ethics approval Providence Health Care Research Ethics Board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Original raw data are encrypted and will be kept on file at the site of collection for 5 years after publication. It will be accessible only by the authors or with proper legal authority.