Article Text

Abstract
Objective Uncomplicated, acute upper respiratory tract infections (URTIs) occur in patients with diabetes at a similar frequency to the general population. This study (NCT00642681) investigated the effect of URTIs on the pharmacokinetic (PK) and pharmacodynamic (PD) properties of Technosphere inhaled insulin (TI) in patients with type 1 or type 2 diabetes.
Research design and methods This was a phase 2 study conducted in patients who developed a URTI while being treated with TI in a phase 3 study (N=20, mean age 50 years, 60% men). Patients underwent two 4-hour meal challenges, during which blood samples were drawn to measure serum fumaryl diketopiperazine (FDKP; the excipient representing an essential part of TI), serum insulin, serum C-peptide, and plasma glucose. The primary outcome was the ratio of serum FDKP area under the concentration–time curve from 0 to 240 min (AUC0–240 min) during URTI and after clinical resolution of URTI symptoms (≥15 to ≤45 days).
Results No significant differences in PK parameters were seen during URTI versus post-URTI for FDKP. The ratio of serum FDKP AUC0–240 min during URTI and post-URTI was 1.1 (SD 0.6), p=0.4462. Plasma glucose concentrations during each 4-hour meal challenge were similar, showing small non-significant differences. No adverse events, including hypoglycemia, occurred during meal challenge visits.
Conclusions Development of an active, symptomatic URTI during treatment with TI had no significant impact on the PK/PD properties of TI, suggesting that no adjustment in prandial insulin dosing is needed. However, if patients are unable to conduct proper inhalation, they should administer their prandial insulin subcutaneously.
Trial registration number NCT00642681; Results.
- Inhaled Insulin
- Type 1
- Type 2
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
Uncomplicated, acute upper respiratory tract infections are expected to occur in patients with diabetes at a similar frequency to the general population. Given the route of administration of Technosphere inhaled insulin, it is clinically relevant for healthcare providers to know whether an upper respiratory tract infection may have an effect on the glucose-lowering properties of Technosphere inhaled insulin and thus an impact on glycemic control.
The data from this study suggest that the development of an upper respiratory tract infection during treatment with Technosphere inhaled insulin had no significant impact on the pharmacokinetic or pharmacodynamic properties of Technosphere inhaled insulin, suggesting that no adjustment in prandial insulin dosing is needed.
If patients are unable to conduct proper inhalation, their prandial insulin should be administered subcutaneously.
Introduction
Technosphere inhaled insulin (Afrezza (insulin human) inhalation powder, MannKind Corporation, Valencia, California, USA) is a dry powder formulation of recombinant human insulin for inhalation, via the Gen2 inhaler device, in patients with diabetes. Technosphere inhaled insulin consists of Technosphere powder (microparticles of fumaryl diketopiperazine (FDKP)) to which insulin is adsorbed. When the microparticles are exposed to physiological pH in the deep lung after inhalation of Technosphere inhaled insulin, they rapidly dissolve, allowing insulin and FDKP to be absorbed rapidly into the blood. FDKP is biologically inactive and is excreted unchanged in the urine; FDKP and insulin, delivered as Technosphere inhaled insulin, have a terminal clearance half-life from the lung of ∼1 hour.1 ,2
After subcutaneous injection, regular human insulin has a time to maximum concentration of 80–120 min and a duration of action of 5–8 hours. Rapid-acting insulin analogs (eg, insulin aspart and insulin lispro) have a time to maximum concentration of around 50–120 min, and a duration of action of 3–5 hours.3–6 Technosphere inhaled insulin, however, has a shorter time to maximum concentration of 12–17 min as well as a shorter duration of action of ∼2–3 hours.7 The faster absorption and shorter duration of Technosphere inhaled insulin is closer to the physiological release of mealtime insulin boluses, and provides the potential for faster glucose-lowering onset, improved postprandial glucose control, reduced hypoglycemia, and less weight gain, resulting from reduced lag time and less likelihood of overinsulinization.8 Furthermore, Technosphere inhaled insulin use avoids the inconvenience associated with subcutaneous injections and might be helpful for insulin requiring individuals with ‘injection or needle phobia’.
In a 2-year, phase 3 clinical study comparing Technosphere inhaled insulin with subcutaneous injection of rapid-acting insulin analogs in patients with type 1 or type 2 diabetes, a gradual decrease in lung function was observed in the treatment groups. Differential changes in lung function associated with Technosphere inhaled insulin were small: ∼1% reduction in forced expiratory volume in 1 s, ∼1% reduction in forced vital capacity, and ∼2% reduction in diffusing capacity of the lung for carbon monoxide. All of these changes occurred early after treatment initiation, were non-progressive, resolved rapidly after discontinuation of Technosphere inhaled insulin, and are considered not to be clinically meaningful.6 On the other hand, acute bronchospasm has been observed in patients with asthma and chronic obstructive pulmonary disease. Technosphere inhaled insulin has a black box warning contraindication in patients with chronic lung disease.9
Uncomplicated, acute upper respiratory tract infections (URTIs; eg, common colds) are the most common infectious illness in the general population, represent the most frequent acute diagnosis in the primary care setting, and occur in adults 2–4 times per year with symptoms persisting up to 7–10 days.10 URTIs are expected to occur in patients with diabetes at a similar frequency to the general population.11 Given the inhaled method of administration of Technosphere inhaled insulin, it is clinically relevant for healthcare providers to know whether a URTI may have an effect on the glucose-lowering properties of Technosphere inhaled insulin and thus impact on glycemic control; that is, is there an increased risk of hypoglycemic or hyperglycemic events when using this product? In fact, inquiries relating to the effect of URTIs on insulin therapy with inhalation of Technosphere inhaled insulin are among the most frequent questions healthcare providers ask the manufacturer.
Here, we report results of a phase 2 study conducted in patients already enrolled in a phase 3 study. This study aimed to investigate the interaction of URTIs with the pharmacokinetic (PK) and pharmacodynamic (PD) properties of insulin and FDKP (as administered in the form of Technosphere inhaled insulin) in patients with type 1 or type 2 diabetes during a URTI, and at least 2 weeks following full recovery from a URTI.
Research design and methods
Study design and patients
This study (MKC-TI-112; ClinicalTrials.gov identifier: NCT00642681) included patients with type 1 and type 2 diabetes who developed a symptomatic URTI while being treated with Technosphere inhaled insulin using the MedTone inhaler in a phase 3 randomized controlled trial (MKC-TI-030 study; ClinicalTrials.gov Identifier: NCT00308737). The study took place between July 2005 and August 2008. URTI was defined as ≥3 URTI symptoms from a questionnaire with a list of symptoms (eg, runny nose, nasal stuffiness, sneezing, sore throat, scratchy throat, hoarseness, new-onset cough, sinus pain/pressure, head congestion/headache, and plugged ears/ear discomfort) in the 24 hours prior to and/or on the day of a clinic visit.
Patients were excluded from the study if there was evidence by medical history, physical examination, or laboratory findings of an acute bacterial infection, including but not limited to purulent sputum production, purulent nasal/eye/ear discharge, chest examination abnormalities on auscultation or percussion, throat exudates, or chest X-ray findings of pneumonia (if clinically indicated).
Each patient underwent two 4-hour meal challenges. The first 4-hour meal challenge was performed during the active phase of the URTI (‘during URTI’). The second 4-hour meal challenge was performed after clinical resolution of URTI symptoms (≥15 days but ≤45 days; ‘post-URTI’). Patients arrived in a fasting state and had not taken their morning dose of prandial Technosphere inhaled insulin; patients taking morning basal insulin or oral antidiabetes agents took them as usual. Following administration of a single dose of Technosphere inhaled insulin, patients ingested a standardized liquid meal of 540 kcal/67.5 g of carbohydrates (12 oz. Boost Plus, Novartis). Blood samples for measurement of serum FDKP, insulin, C-peptide, and plasma glucose were obtained 30 min before dosing, at dosing (0), and 5, 10, 15, 20, 30, 45, 60, 90, 120, 180, and 240 min after insulin dose administration. Blood glucose was measured at a central laboratory (BARC-US, Lake Success, New York, USA). Patients received the same Technosphere inhaled insulin dose they were currently taking in the MKC-TI-030 study at the time of the meal challenge; that is, a standard insulin dose was not applied. It was intended that each patient served as his or her own control.
The study was conducted in accordance with the ethical principles of Good Clinical Practice as defined by the International Conference on Harmonization and Declaration of Helsinki.12 Independent ethics committees or institutional review boards approved the protocol, and all participants gave written informed consent.
End points
The primary end point was the serum FDKP area under the concentration–time curve from 0 to 240 min (AUC0–240 min). Serum FDKP AUC and not the AUC under the serum insulin profile was used as the primary end point to avoid interference from endogenously secreted insulin in patients with type 2 diabetes.
The primary outcome was the ratio of serum FDKP AUC0–240 min during URTI and post-URTI. Other PK parameters assessed included insulin concentrations overtime (AUC0–240 min), maximum FDKP and insulin serum concentration (Cmax), time to reach Cmax (tmax), and FDKP half-life (t½).
PD parameters assessed during URTI and post-URTI included plasma glucose concentrations, maximum and minimum plasma glucose (Cmax, Cmin), and baseline-corrected plasma glucose Cmax and Cmin.
Safety parameters assessed during URTI and post-URTI included vital signs, physical examination findings, and adverse events (AEs).
Statistical analyses
Descriptive statistics of the PK, PD, and safety parameters were calculated during URTI and post-URTI. Natural log transformation was performed on AUC0–240 min and paired Student's t-tests were used to assess the between-period differences. The p<0.05 was considered significant.
For five patients, Technosphere inhaled insulin doses during URTI and post-URTI were different, so AUC for FDKP and insulin was normalized for these patients to the lower of the two Technosphere inhaled insulin doses. The ratio was calculated on the log-transformed normalized AUC.
Efficacy analyses were performed on the intent-to-treat population, defined as all randomized patients who received ≥1 dose of trial medication and had values for the primary efficacy variables during URTI and post-URTI. Safety analyses were performed on the safety population, defined as all randomized patients who received ≥1 dose of trial medication during the study.
Results
Patients
From 23 sites with a population of 283 individuals, a total of 20 patients were screened and enrolled in the study, six with type 1 and 14 with type 2 diabetes. All 20 patients received a single dose of Technosphere inhaled insulin at each of the two 4-hour meal challenges (during URTI and post-URTI) and all patients completed the study. Hence, the safety, intent-to-treat, and per protocol populations were identical. Of the 20 patients, 12 (60%) were men and eight (40%) were women; mean (SD) age was 49.8 (13.6) years (range 21–65 years). Three (15%) patients were aged 18–30 years, six (30%) were aged 31–49 years, 10 (50%) were aged 50–64 years, and one (5%) was aged ≥65 years.
During the study, Technosphere inhaled insulin doses were individualized and ranged from 15 to 90 units (corresponding to 4–24 units of subcutaneous rapid-acting insulin). Therefore, comparison of mean FDKP and insulin Cmax and AUC is not meaningful. The variation in doses was addressed by normalizing within each patient and by using individual AUC ratios as the primary outcome.
Pharmacokinetics
FDKP
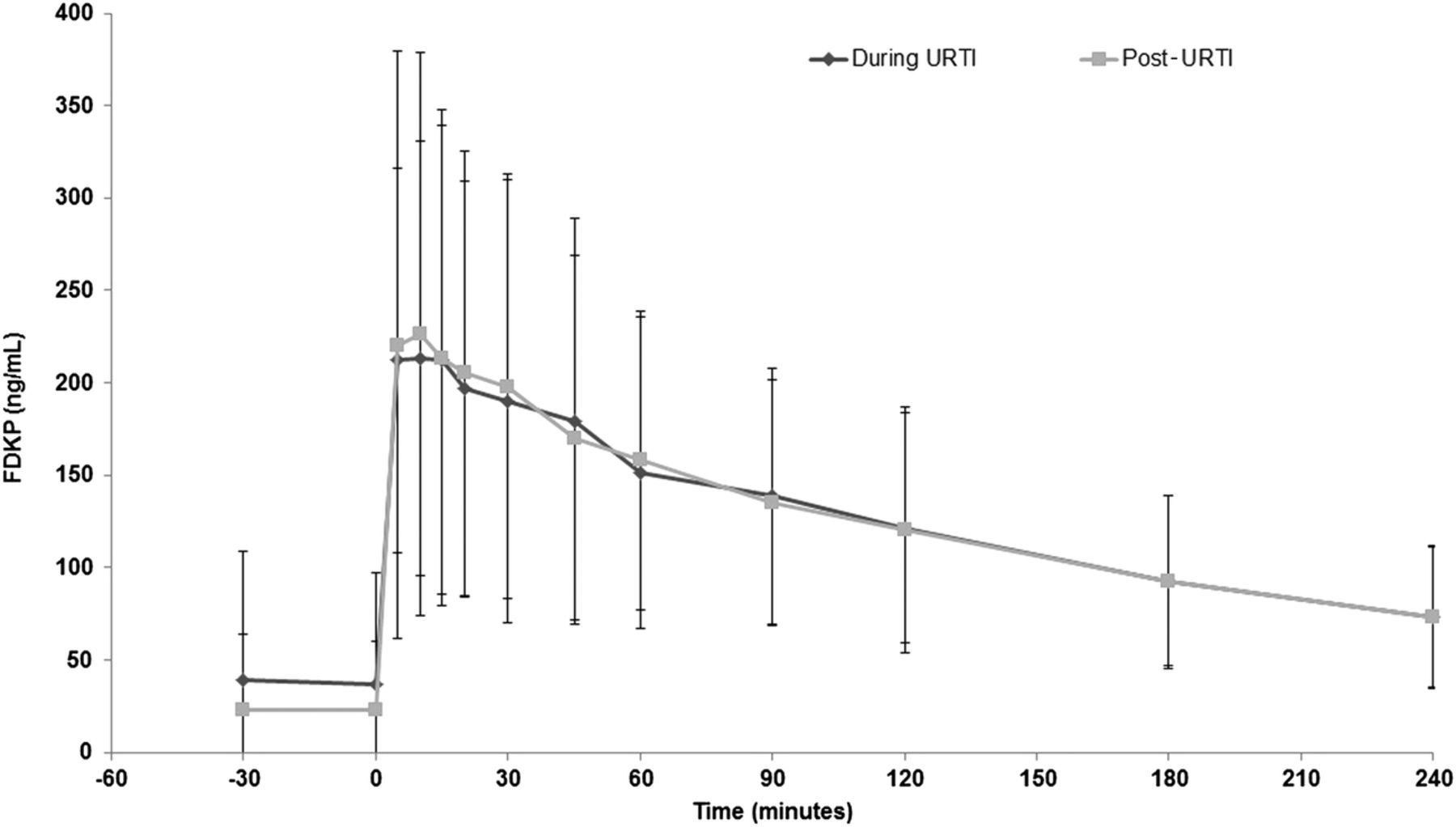
The PK profile of FDKP measured by AUC0–240 min after dosing was similar during URTI and post-URTI (figure 1). The dose-normalized mean (SD) FDKP AUC0–240 min during URTI was 23 315 (12 586) ng min/mL and the post-URTI FDKP AUC0–240 min was 26 763 (14 782) ng min/mL. The ratio (SD) was 1.1 (0.6) (p=0.4462; table 1). No significant differences were noted during URTI and post-URTI for tmax or t½ (table 1).
FDKP and insulin pharmacokinetic parameters during URTI and post-URTI

Fumaryl diketopiperazine (FKDP) concentrations over time during upper respiratory tract infection (URTI) and post-URTI. Data are mean±SD.
Serum insulin
The serum insulin profile (AUC0–240 min) after dosing with Technosphere inhaled insulin was similar during URTI compared with post-URTI: the ratio was 0.9 (0.4) (p=0.1754) (table 1, figure 2). No significant differences were noted during URTI or post-URTI for tmax (25.5 (44.4) vs 21.3 (25.1) minutes, respectively; p=0.7194). The individualized dose administration precluded statistical comparison of insulin concentrations and Cmax during URTI and post-URTI.

Serum insulin concentrations overtime with Technosphere inhaled insulin during upper respiratory tract infection (URTI) and post-URTI. Data are mean±SD.
Pharmacodynamics
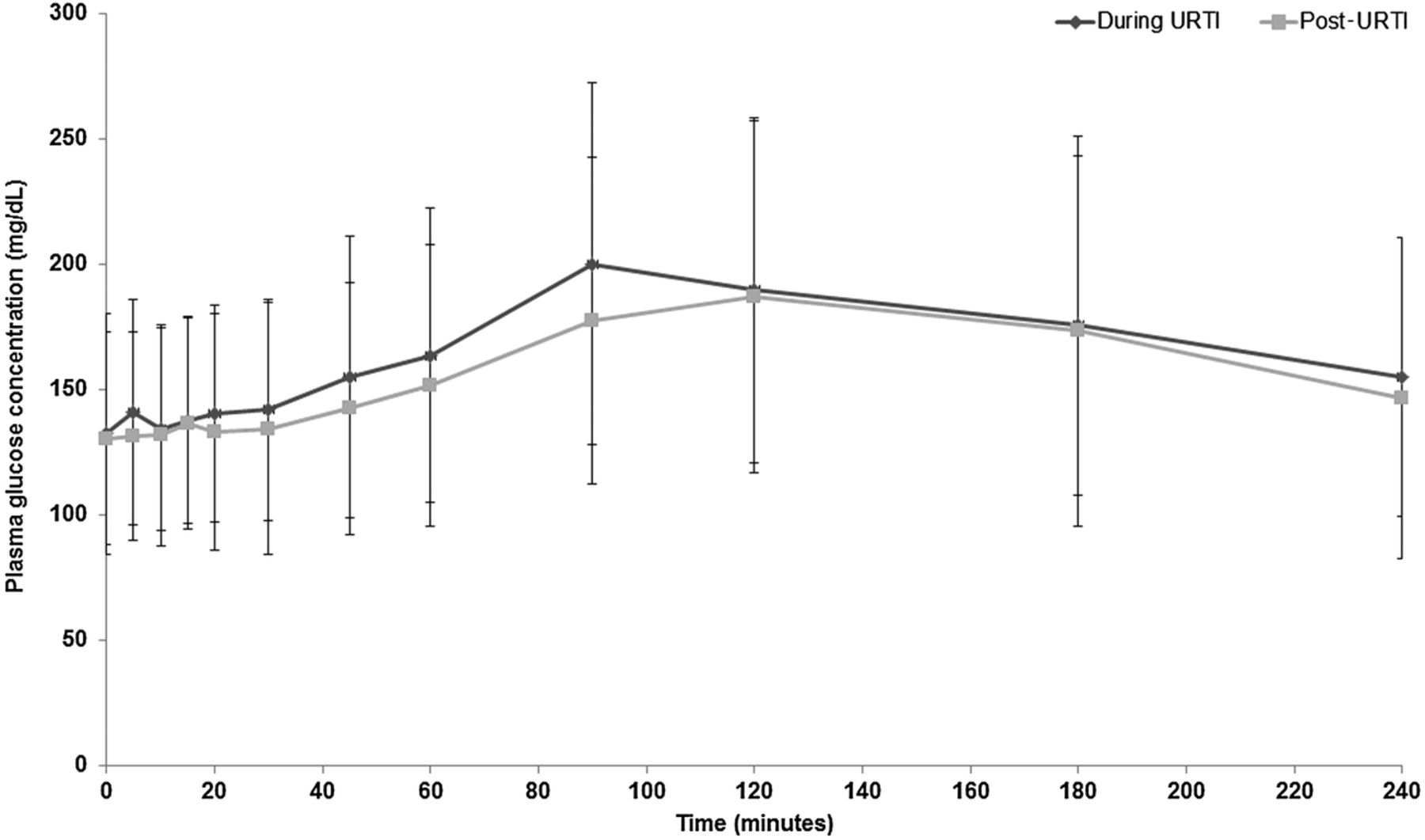
The maximal plasma glucose concentrations during each 4-hour meal challenge were similar during URTI and post-URTI (table 1, figure 3). Differences in plasma glucose parameters Cmax and Cmin (unadjusted and baseline corrected) during URTI and post-URTI were small. However, owing to the study design, statistical analysis of these data is not meaningful.
{kind=link}
{kind=link}
{kind=link}
Plasma glucose concentrations during a 4-hour meal challenge during upper respiratory tract infection (URTI) and post-URTI. Data are mean±SD.
Safety
All 20 patients completed the MKC-TI-112 study; there were no premature discontinuations, no deaths, and no AEs (including hypoglycemia). No clinically relevant findings were reported for vital signs or physical examination.
Conclusions
Symptomatic URTIs, a common and frequent ailment among the general population as well as among those with diabetes, might cause concern for healthcare providers and patients with coincident use of Technosphere inhaled insulin. This study showed that active, symptomatic URTIs during treatment with Technosphere inhaled insulin had no impact on the PK and PD properties of Technosphere inhaled insulin, as assessed by the primary end point of FDKP AUC0–240 min. Furthermore, the other PK parameters of FDKP and insulin were found to be similar during URTI and following recovery from an URTI. The PD properties of Technosphere inhaled insulin, as assessed by unadjusted and baseline-corrected blood glucose Cmax and Cmin, were also similar during URTI and post-URTI. Moreover, Technosphere inhaled insulin was well tolerated by participants in this study. Therefore, for individuals accustomed to using Technosphere inhaled insulin as a part of their insulin therapy who develop an active, symptomatic URTI, no difference in Technosphere inhaled insulin absorption is expected; that is, coverage of prandial insulin requirements should be identical. However, dose adjustments may be needed due to the infection itself; that is, the decreased insulin sensitivity seen with URTI might require higher insulin doses.
A limitation of this study is the small number of participants (N=20) enrolled. However, the data reported here are supportive of other studies that have been conducted to assess the suitability of using inhaled insulins during acute URTIs. The PK and PD properties of AERx insulin Diabetes Management System and AIR inhaled insulin have been assessed during URTI in normal individuals.11 ,13 Both studies also suggested no significant differences in PK and PD properties of both inhaled insulins during a URTI. The incidence and clinical effect of intercurrent respiratory tract infections have also been investigated with Exubera. In a retrospective analysis of pooled data from 14 phase 2 and 3 clinical studies, no apparent changes in glycated hemoglobin (HbA1c) or in the rate of overall hypoglycemic events were observed with intercurrent respiratory tract infections in any treatment group.14 Another limitation of our study is that patients with lower respiratory tract infections were not studied.
Given the route of delivery of Technosphere inhaled insulin, one question that may arise is whether the drug itself causes URTIs or their symptoms. Isolated and brief cough, categorized as mild, non-productive, and occurring within ≤10 min of inhalation of Technosphere inhaled insulin without other symptoms of URTI, is a commonly reported AE (frequency 25–29%).6 However, when data from the phase 2 and 3 clinical studies of Technosphere inhaled insulin for all-cause respiratory treatment-emergent AEs are pooled, URTIs were reported more frequently with comparators than with Technosphere inhaled insulin (10.9% vs 9.4%, respectively) (Data on file, MannKind Corporation). It is plausible that the slightly lower URTI incidence in Technosphere inhaled insulin-treated patients is due to cough being assigned as related to the drug, rather than as a symptom of URTIs. Bronchitis was reported in 3.0% of patients treated with Technosphere inhaled insulin and 2.6% of patients treated with comparators, suggesting no significant difference in the occurrence of lower respiratory tract infections.
In conclusion, the results of this study suggest that Technosphere inhaled insulin can be used successfully for prandial insulin coverage by patients with diabetes during an active, symptomatic URTI. However, it should be noted that if patients with type 1 or type 2 diabetes are unable to conduct proper inhalation during URTI, they should administer their insulin subcutaneously.
References
Footnotes
Contributors AB was involved in the design of the study protocol. PAL and PDR collected the data. PAL, LH, AB, and PDR interpreted the data and revised the manuscript critically, provided final approval of the version to be submitted, and are accountable for its accuracy and integrity.
Funding This study was funded by MannKind Corporation. The authors received writing/editorial support in the preparation of this manuscript provided by Katherine Roberts, PhD, of Excerpta Medica, funded by Sanofi US. Afrezza and Technosphere are registered trademarks of MannKind Corporation.
Competing interests PAL reports serving on an advisory panel for Novo Nordisk and Sanofi US, serving as a consultant for Novo Nordisk and Sanofi US, providing research support for Novo Nordisk, Sanofi US, Eli Lilly and Company, Amylin Pharmaceuticals, GlaxoSmithKline, Boehringer Ingelheim, and AstraZeneca, and being a member of the speakers bureau for Novo Nordisk, Sanofi US, Eli Lilly and Company, Amylin Pharmaceuticals, MannKind Corporation, and AstraZeneca. LH is an employee of Science & Co., serves on an advisory panel for Biodel, Eli Lilly, Halozyme, Novo Nordisk, and Sanofi, and is a partner of the Profil Institut für Stoffwechselforschung (Neuss, Germany) and the Profil Institut for Clinical Research (San Diego, California, USA). AB is an employee of Sanofi US, and was employed by MannKind at the time the study was conducted. PDR reports serving as a member of the speaker/teaching faculty for AbbVie, AstraZeneca (Bristol-Myers Squibb), Boehringer Ingelheim, GlaxoSmithKline, Janssen, Kowa, Merck, and Takeda, providing clinical research trial support for Amgen, AstraZeneca (Bristol-Myers Squibb), Dexcom, Eisai, Lilly, GlaxoSmithKline, Merck, Novo Nordisk, Orexigen, Pfizer, and Sanofi, and having acted as consultant/advisor for Amarin, AstraZeneca, Lilly, Merck, and Sanofi-Regeneron.
Ethics approval Coast IRB, LLC 5475 Mark Dabling Boulevard, Suite 351, Colorado Springs, Colorado 80918, USA. Komisja Bioetyki Uniwersytetu Medycznego w Lodzi, ul. Zeligowskiego 7/9 90-752 Lodz, Poland. Central IEC for Russia: Ethics Committee under the Federal Service on Surveillance in Healthcare and Social Development, Bldg 1, Slavyanskaya Square, Moscow 109074, Russia. Local IEC for Russia: Ethics Committee of FSI ‘Principal Military Clinical Hospital na Academician NN Burdenko for the Ministry of Defense of RF’ 3, Hospitalnaya Square, Moscow 105229, Russia.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.