Article Text

Abstract
Objective To describe adverse events in pediatric insulin pump users since universal funding in Ontario and to explore the role of socioeconomic status and 24-hour support.
Research design and methods Population-based cohort study of youth (<19 years) with type 1 diabetes (n=3193) under a universal access program in Ontario, Canada, from 2006 to 2013. We linked 2012 survey data from 33 pediatric diabetes centers to health administrative databases. The relationship between patient and center-level characteristics and time to first diabetic ketoacidosis (DKA) admission or death was tested using a Cox proportional hazards model and the rate of diabetes-related emergency department visits and hospitalizations with a Poisson model, both using generalized estimating equations.
Results The rate of DKA was 5.28/100 person-years and mortality 0.033/100 person-years. Compared with the least deprived quintile, the risk of DKA or death for those in the most deprived quintile was significantly higher (HR 1.58, 95% CI 1.05 to 2.38) as was the rate of diabetes-related acute care use (RR 1.60, 95% CI 1.27 to 2.00). 24-hour support was not associated with these outcomes. Higher glycated hemoglobin, prior DKA, older age, and higher nursing patient load were associated with a higher risk of DKA or death.
Conclusions The safety profile of pump therapy in the context of universal funding is similar to other jurisdictions and unrelated to 24-hour support. Several factors including higher deprivation were associated with an increased risk of adverse events and could be used to inform the design of interventions aimed at preventing poor outcomes in high-risk individuals.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
Adverse outcomes in pediatric insulin pump users are associated with socioeconomic deprivation but not with access to 24-hour support.
We identified groups of pump users at higher risk for adverse events for whom targeted interventions may prevent adverse events: those with previous diabetes-related emergency department visits or hospitalizations, baseline poor glycemic control, and adolescents.
The underlying causes of socioeconomic disparities in the risk of diabetic ketoacidosis require further investigation to inform the design of interventions aimed at reducing the inequity of this preventable and serious complication.
Type 1 diabetes can be managed with multiple daily injections of insulin or an insulin pump.1 Pediatric pump use has become increasingly popular and it is uncommon for patients to revert to injections.2–4 Ontario has a population of over 13 million and one of the highest incidences of type 1 diabetes in the world (>20/100 000/year).5 The Ontario Pediatric Diabetes Network, comprised of 35 centers, oversees pediatric diabetes care.6 The cost of pump therapy has been provided by the Ontario government since 2006. We have shown that number of individuals with government pump funding has increased since 2006, and that in 2012, mean percent pump use across Ontario centers was 38.0% with variability across centers.3
In the context of universal funding, potentially increased work load and less capacity to provide education and support, it is important to establish the safety of pediatric pump therapy. We have described differences in the Ontario Network center characteristics including 24-hour support, center type, physician model of care, and nursing patient load.6 In non-experimental settings, the rate of diabetic ketoacidosis (DKA), a preventable and acute life-threatening complication of type 1 diabetes, does not appear to be increased in pump users.2 However, in a study from Newfoundland and Labrador, Canada, 58.5% of children with previously diagnosed diabetes presenting in DKA were using an insulin pump, with the root cause of DKA identified as failure to recognize and respond to problems with interruption of insulin delivery.7
The International Society for Pediatric and Adolescent Diabetes (ISPAD) recommends that the diabetes care team should provide emergency telephone or other support 24 hours a day to patients and families.8 We have shown that in 2012, funded 24-hour support was available at 10 (29%) of all Ontario Pediatric Diabetes Network centers.7 Results from clinic-based studies of youth with type 1 diabetes suggest that provision of 24-hour telephone support may reduce the incidence of acute diabetes adverse events such as diabetes-related emergency department (ED) visits and DKA.9 ,10 Other factors such as socioeconomic status (SES) have been associated with pediatric diabetes management and outcomes11 ,12 including DKA.13 ,14 In Ontario, low-income children are less likely to be on pumps,3 ,12 and there is an inverse relationship between the rate of diabetes-related adverse events and income in children and adults.15 ,16
Our objective was to describe the rate of DKA in the context of a public funding program for pumps and to explore the relationship between access to 24-hour support, SES, and the risk of DKA or death. Our secondary objective was to describe rates of diabetes-related admissions and ED visits, as a marker of other acute diabetes-related complications, and to explore the relationship between center and patient characteristics and the rate of these events. We hypothesized that lack of 24-hour support and lower SES would be associated with an increased risk of adverse events.
Research design and methods
This is an observational population-based cohort study using survey data from 33/35 pediatric diabetes centers in Ontario linked to population-based health administrative databases from 1 November 2004 to 31 March 2013. We excluded two centers as they followed <6 individuals with type 1 diabetes.
Data sources
Pediatric Diabetes Network resource survey data were collected from January to June 2012 and we had 100% response rate. Details of the questionnaire development and dissemination have been previously described.7
We used the following administrative health databases at the Institute for Clinical Evaluative Sciences (ICES; Toronto, Canada), linked via unique encoded identifiers: (1) the Assistive Devices Program (ADP) database (information about new and renewal applications for pediatric insulin pump funding) to create the pump cohort and ascertain pump discontinuation; (2) the Pediatric Ontario Diabetes Database (ODD), a validated registry of all Ontario residents (<19th birthday) with a diagnosis of diabetes17 to determine date of diabetes diagnosis; (3) the Hospital Discharge Abstract Database (DAD; information on discharges from acute care facilities) to describe healthcare utilization and describe other chronic condition comorbidity; (4) the Ontario Health Insurance Plan Database (physician billing claims) to describe healthcare utilization; (5) the National Ambulatory Care Reporting System (information on ED visits) to describe healthcare utilization; (6) the Registered Persons Database (RPDB; demographics and vital statistics including outmigration of all legal residents in Ontario); (7) the Ontario Registrar General-Death (ORGD) for cause of death; (8) the 2006 Canadian Census to assign neighborhood income quintile and the material deprivation index, a component of the Ontario Marginalization Index (ON-MARG); (9) the Ontario Drug Benefit (ODB) database (medication insurance data for those families on social assistance) to indicate low-income status; (10) two validated pediatric chronic disease registries: the Ontario Asthma Surveillance Information System Database (ASTHMA);18 and (11) the Ontario Crohn's and Colitis Cohort (OCCC),19 to describe other chronic condition comorbidity.
Research ethics board approval was obtained from the University of Toronto, The Hospital for Sick Children, and Sunnybrook Health Sciences Center.
Study cohort
We created the study cohort of children using data from the ADP database which contains records of initial applications for pump funding and annual renewal applications. To be eligible to receive government funding individuals must be <19 years of age, have type 1 diabetes, have three glycated hemoglobin (HbA1c) levels from the previous year of which the last two levels taken prior to pump initiation are <10% (86 mmol/mol), monitor blood glucose before each meal and bedtime, demonstrate ongoing recording and review of blood glucose results, rotate insertion sites, practice appropriate sick day management, attend diabetes clinic at least three times per year, and complete a pump education program.20 All individuals who had an approved ADP application for pediatric pump funding between 1 November 2006 and 31 March 2011 and were <19 years of age on the date of the application were included. The index study date was the date of application for pump funding.
Outcomes
The primary outcome is first admission for DKA or death. International Classification of Diseases, 10th Revision, Canadian Enhancement (ICD-10-CA) codes for diabetes-related preventable hospitalizations, using the Agency for Healthcare Research and Quality (AHRQ) specifications,21 translated to ICD-10 codes for Ontario were used to identify DKA-related and diabetes-related admissions (see online supplementary appendix 1). All-cause deaths were included in our main outcome, as not all sources of mortality data include cause of death.
Supplementary appendix
The secondary outcome is the combined rate of diabetes-related admissions and ED visits computed as the number of events per person-months follow-up. We also examined the rate of diabetes-related admissions and ED visits separately. The number of events were calculated from the index study date to the earliest of 19th birthday, pump discontinuation, outmigration, death, or the end of the study (31 March 2013). Diabetes-related inpatient and ED visits were categorized by ICD-10-CA codes of the most responsible diagnosis (see online supplementary appendix 1). All diagnostic codes of the most responsible diagnosis for all inpatient and ED visits were independently reviewed by two pediatric endocrinologists (RS and JDW) and assigned as DKA-related or diabetes-related. The classification of each diagnosis was based on the endocrinologists' clinical knowledge of its specificity for DKA or diabetes. Discrepancies were resolved through consensus.
Primary exposures
The primary center-level exposure was the availability of funded 24-hour/7-day/week support for patients using insulin pumps (from the survey). The primary patient-level exposure was SES. We used a number of measures of SES including a postal code-derived neighborhood material deprivation index, neighborhood income quintile, and family qualification for the ODB plan. The material deprivation dimension of the ON-MARG is a validated census-based and geography-based index that measures differences in marginalization between geographic areas.22 We chose this index to represent the SES effect because it includes an indicator of education and family structure. Both parental education23 and family structure24 have been associated with diabetes outcomes. For descriptive purposes, we also reported the neighborhood income quintile, based on postal code, at the level of the dissemination area (representing a population of ≈400–700 individuals) adjusted for household and community size.25
Other variables
Center-level variables obtained from the survey included center type (tertiary, small community, or large community center), model of physician care, and the annual number of patients per nurse. The five tertiary centers are located in the pediatric academic health science centers in Ontario's major cities. Small community centers were defined as those with a patient volume <150 and large community centers as those with a patient volume ≥150. This categorization is based on the recommendation by the ISPAD that the number of patients per center should be at least 150 for members of the diabetes team to obtain sufficient experience.8 The model of physician care at each clinic was defined as (1) pediatric endocrinologist; (2) generalist (general pediatrician(s) or family physician(s) but no pediatric endocrinologist) and (3) generalist with a visiting pediatric endocrinologist. Annual nursing patient load was categorized as <200 and ≥200 based on volume.
We controlled for prior risk of adverse events as the occurrence of at least one event in the 2 years prior to the index date. Age was categorized into three groups according to the Canadian Diabetes Association guidelines.26 The duration of diabetes was the difference between the index date and the incident date of diabetes diagnosis in the ODD and categorized as <5 and ≥5 years. Baseline glycemic control for each individual in the pump cohort was determined by taking the mean of all HbA1c values recorded on the initial ADP application for pump funding and categorized as optimal (<7.5% (58 mmol/mol)), suboptimal (7.5–9.0% (58–75 mmol/mol)), and high risk (>9.0% (75 mmol/mol)) according to the ISPAD clinical practice guidelines.27 Other chronic condition comorbidity included asthma and inflammatory bowel disease18 and a commonly used list of other conditions, the ‘pediatric complex chronic conditions’, defined as conditions that are expected to last at least 12 months and that involve multiple organ systems or one system but that require inpatient specialist pediatric care, using prior diagnoses from hospital admissions.28 All comorbidities were grouped together with asthma the most common comorbidity. We used the Rurality Index for Ontario (RIO) score to describe rurality. The RIO score is based on community characteristics, including access to health services.29 We categorized the RIO into three groups based on scores ranging from 0 to 100 (0 is the most urban and 100 the most rural).
Analysis
We used a Cox proportional hazards model to test the association between risk of admission for DKA or death and the two main exposures, 24-hour center support and material deprivation. We also controlled for center type, model of physician care, sex, age group, baseline HbA1c, duration of type 1 diabetes, patients per nurse, and the occurrence of DKA in the baseline period. We used generalized estimating equations (GEEs) to account for patient clustering at centers. Since rurality is correlated with center type and model of physician care, it was described but not included in the model.
Individuals were censored on the date of pump discontinuation, 19th birthday, or outmigration from Ontario. ADP data were used to ascertain pump discontinuation. Individuals with no renewal within 24 months from their initial application or last renewal application were considered discontinued. If there was more than one initial application, all subsequent initial applications were counted as renewal applications if they occurred <24 months from the previous either initial application or renewal applications. We allowed 24 months to capture 99% of those who ultimately submit a renewal rather than the administratively defined 12 months. If an individual was deemed to have discontinued, the discontinuation date was assigned as 12 months from the last renewal application. Collinearity was assessed using variance inflation factors. The proportionality of hazards was assessed using a time interaction variable. We examined the distribution of deviance residuals for influential outliers.
We used a Poisson model to test the association between rate of diabetes-related ED visits and admissions and our main exposures, 24-hour support and material deprivation. We also tested the same associations with the rate of admissions and ED visits separately. For all models, we controlled for center type, model of physician care, sex, age group, baseline HbA1c, duration of type 1 diabetes, patients per nurse, and the occurrence of a diabetes-related admission or ED visit during the baseline period.
We used GEEs to account for patient clustering at centers. The time on pump, calculated from the date of initial application for pump funding to the earliest of 19th birthday, death, pump discontinuation, outmigration, or the end of the study (31 March 2013) was used as an offset. To assess for influential outliers, we examined Pearson deviance residuals.30 All statistical tests were performed at the 5% level of significance and were two-sided. Analyses were performed using SAS Enterprise Guide V.6.1 using procedures PHREG and GENMOD.
Results
Baseline characteristics
The baseline characteristics of the pump cohort are reported in table 1 according to availability of 24-hour support. A slightly higher proportion of those without access to 24-hour support are in the lowest income and most SES-deprived quintiles and are more likely to have had a baseline adverse event. Those with access to 24-hour support are less likely to be followed at a small community center and more likely to be at a center with a visiting pediatric endocrinologist model.
Baseline characteristics of the pump cohort by availability of 24-hour support at the index date
DKA or death
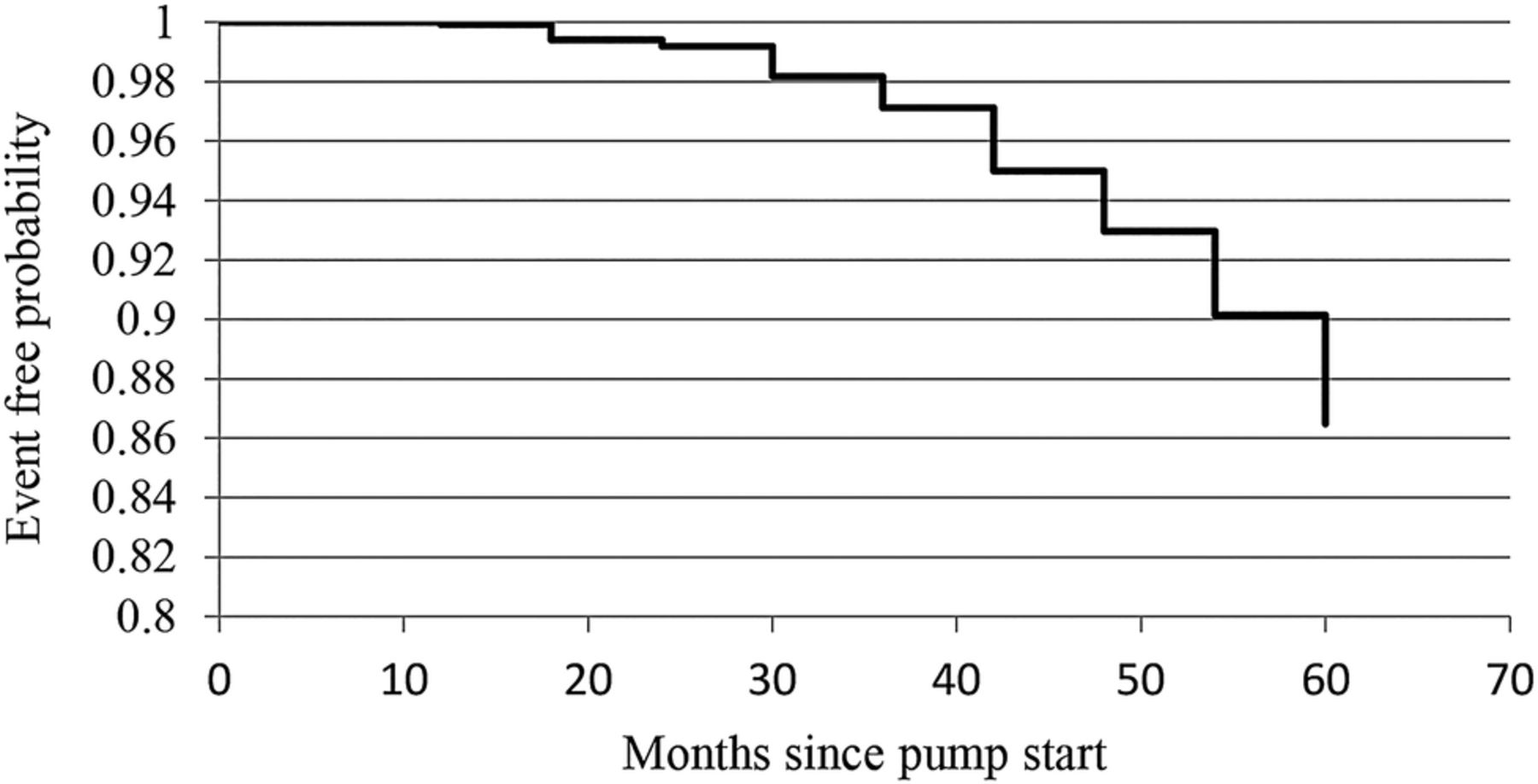
Mean time on pump was 3.77 years (SD 1.64) and the rate of DKA was 5.28 per 100 person-years. This compares to a baseline DKA rate of 6.97 per 100 person-years. The mean age at the time of first DKA admission or death was 12.8 years (SD 3.8). There were <6 deaths during the study period (for privacy reasons event numbers <6 cannot be reported); the rate of death was 0.033/100 person-years. Figure 1 illustrates that the probability of having DKA or death in the first 24 months of pump use was low (0.01).

{kind=link}
The cumulative probability of diabetic ketoacidosis (DKA) or death according to time since pump start.
Table 2 shows the results of the multivariable Cox proportional hazards model of DKA or death. Access to 24-hour support was not associated with DKA or death, but being more deprived was associated with a 58% higher risk (HR 1.58 (95% CI 1.05 to 2.38), p=0.0272). Other significant associations included having a higher baseline HbA1c (HR 2.63 (1.89 to 3.67), p<0.0001), DKA in the baseline period (HR 1.63 (1.28 to 2.07), p<0.0001), older age (13th to <19th birthday (HR 2.35 (1.90 to 2.90), p<0.0001), and being followed at a center with a higher nursing patient load (HR 1.24 (1.00 to 1.52), p=0.0468). Having diabetes for ≥5 years was associated with a lower risk of DKA or death (HR 0.76 (0.64 to 0.89), p=0.0007).
Association between time to first DKA admission or death and patient-level and center-level characteristics among pediatric pump users in Ontario (n=3193)
Diabetes-related admissions or ED visits
The number of diabetes-related admissions or ED visits per person ranged from 0 to 30 with 70.0% of individuals having no events. The rate of diabetes-related admissions and ED visits was 14.73 per 100 person-years. This is compared with a baseline rate of 27.59 per 100 person-years. Results from the Poisson model show that while being more deprived was associated with a higher rate of diabetes-related acute care use (HR 1.60 (95% CI 1.27 to 2.00), p≤0.0001), access to 24-hour support was not. Analyses limited to diabetes-related admissions or ED visits only showed similar results to the main analysis.
Other significant associations with patient-level characteristics included higher baseline HbA1c, the occurrence of a baseline diabetes-related admission or ED visit, older age (13th to <19th birthday), being female, and having a longer diabetes duration. Center-level characteristics including center type, physician model, and nursing patient load were not associated with the rate of diabetes-related admissions and ED visits (table 3).
Association between rate of diabetes-related admissions and ED visits and patient-level and center-level characteristics among pediatric pump users in Ontario (n=3193)
Conclusions
In this population-based study with the longest duration of follow-up of any published studies to date of children and youth on insulin pump therapy, we find the rate of DKA to be similar to what others have reported.31 ,32
Unlike the findings of another population-based study documenting most DKA episodes occurring within the first year of pump use,31 the risk of DKA or death in the first 2 years of pump use in our study is low, suggesting that the process for selecting patients for pump therapy and initial pump education in Ontario is effective. Further, the rate of adverse events after pump start in our cohort was lower compared with baseline. Although this cannot be interpreted as being causally related to pump therapy alone, it is reassuring about the current implementation of pediatric pump therapy in Ontario.
Results from our multivariable analyses question previous work around the need for 24-hour support. Our hypothesis around the association of 24-hour support with adverse events was not borne out. Other studies have shown that provision of 24-hour support is associated with a reduction in ED and office visits.10 Another found that those who accessed the support service were more likely than those who did not to have an ED visit, however, were less likely to lead to a hospital admission.33 In our study, there was no association between 24-hour support and either admissions or ED visits when analyzed separately. This suggests that in Ontario either availability of 24-hour support may not be an important gap in service delivery or that barriers to its effective use may exist such that its benefits were not realized. Future research should more closely examine potential barriers to accessing 24-hour telephone care as well as the full range of potential benefits including impact on parental anxiety and its ability to reduce disparity in SES of diabetes outcomes.
Our finding that having a higher nursing patient load is associated with a higher risk of adverse events supports older data that provision of care by a comprehensive diabetes management program including intensive education is associated with a lower rate of diabetes-related adverse events.34 Although no other studies have investigated the association between diabetes nurse patient volume and adverse events of pump therapy, we have shown that providers of pediatric pump therapy recognize the importance of a multidisciplinary diabetes team, including nursing, in ensuring good outcomes of pump therapy and feel that this resource is insufficiently recognized in the Ontario funding policy.35 Increases in funding for additional nursing support may be an effective strategy for preventing adverse events in pump users and in children with diabetes in general and should be further explored.
Even in the context of a universal access healthcare system, our hypothesis about SES was confirmed. Individuals who were more deprived had both a higher risk of DKA and a higher rate of diabetes-related admissions and ED visits, adding evidence to an established body of literature suggesting that lower SES is associated with disparities in diabetes management and outcomes. In the US Type 1 Diabetes Exchange Clinic Registry, a cohort study of 13 487 patients, found that low income was associated with a higher frequency of severe hypoglycemia and DKA.14 In Ontario, with a healthcare system that provides funding for insulin pumps, children of lower SES are less likely to be using pumps,3 ,12 and we have now demonstrated that pump outcomes are also worse in more deprived populations. Although a single center in Ontario found no association between measures of material and social deprivation and glycemic control in pump users,12 our findings are population-based. While we did not explore reasons for these disparities, these findings may relate to the additional financial burden of the uncovered 25% ($C800) of the annual cost of the insertion sets required for pump therapy. This may restrict the ability of lower income families to purchase glucose test strips, not universally covered. Those on social assistance receive reimbursement for up to 3000 strips annually (∼8 strips per day), while those who have no other private insurance plan can receive up to a maximum of $C820 per year (∼3 strips per day). Those not on social assistance and who do not have private insurance that covers 100% of the cost of strips, can receive coverage for strips after paying a deductible equal to ∼4% of the household's combined net income. Decreased access to test strips may restrict the frequency of blood glucose monitoring, known to be associated with diabetes outcomes.36 Similarly, the costs of transportation and missed work may reduce the frequency of routine diabetes care visits and opportunities for education and guidance that may prevent adverse events. We have shown that physicians perceive that outcomes of pump therapy are influenced by the degree of family and school support available.35 If families of lower SES have less robust family and school support, this may be another reason for the higher rate of adverse events in this group.
Finally, our findings of factors associated with an increased risk of DKA (older age, worse glycemic control, and history of DKA) are consistent with those previously identified in youth with type 1 diabetes not restricted to those using pumps.14 ,37 ,38 This suggests the need for targeted interventions and additional support for groups of youth with type 1 diabetes at highest risk for adverse events.
Limitations
We measured applications for pump funding, not actual pump use. Some individuals who applied for pump funding may have been using a pump prior to universal funding. Both the deprivation and neighborhood income quintiles are ecological measures of SES. However, these are measured at the dissemination area level which contains ∼400–700 individuals and as such are likely good proxies for individual-level SES. We were not able to measure HbA1c as an outcome because HbA1c at the time of pump funding renewal is not available. We did not have information about sensor-augmented pump therapy use from available data. Finally, the self-reported nature of the center data is a limitation. We did not independently verify answers; however, an internal network survey in 2013 showed close correlation of common data elements.6
In the context of universal funding for pediatric insulin pumps, we report a positive safety profile that is not related to access to 24-hour support; however, adverse outcomes are associated with socioeconomic deprivation. We have identified groups of pump users at higher risk for adverse events for whom targeted interventions may prevent adverse events: those with previous diabetes-related ED visits or hospitalizations, baseline poor glycemic control, and adolescents. The underlying causes of socioeconomic disparities in the risk of DKA in this population require further investigation to inform the design of interventions aimed at reducing the inequity of this preventable and serious complication.
Acknowledgments
The authors would like to thank the research participants. AG is the guarantor for this manuscript.
References
Footnotes
Contributors RS conceptualized and designed the study, designed the data collection instrument, collected the data, carried out the initial analyses, contributed to the analysis and interpretation of data, drafted the initial manuscript, critically reviewed the manuscript, and approved the final manuscript as submitted. TAS conceptualized and designed the study, contributed to the analysis and interpretation of data, critically reviewed the manuscript, and approved the final manuscript as submitted. FAM conceptualized and designed the study, contributed to the interpretation of data, critically reviewed the manuscript, and approved the final manuscript as submitted. DD conceptualized and designed the study, contributed to the interpretation of data, critically reviewed the manuscript, and approved the final manuscript as submitted. AN contributed to the design and the analysis of the study, critically reviewed the manuscript, and approved the final manuscript as submitted. JDW contributed to the analysis and interpretation of data, critically reviewed the manuscript, and approved the final manuscript as submitted. AG conceptualized and designed the study, provided oversight of the analysis and interpretation of data, reviewed and revised the manuscript, and approved the final manuscript as submitted.
Funding This study was supported by the Institute for Clinical Evaluative Sciences (ICES), which is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care (MOHLTC). These data sets were linked using unique encoded identifiers and analyzed at the ICES. This study was approved by the Institutional Review Boards at Sunnybrook Health Sciences Centre, Toronto, Canada, the University of Toronto, and The Hospital for Sick Children. Parts of this material are based on data and information compiled and provided by CIHI. RS receives salary support from the Canadian Child Health Clinician Scientist Program. DD is the RS McLaughlin Foundation Chair in Paediatrics. AG receives salary support from a Canadian Institute for Health Research Applied Chair in Child Health Services and Policy Research. This research was supported by a Creative Professional Activities grant from the Department of Pediatrics, Hospital for Sick Children and by funding through AG's research chair award.
Disclaimer The opinions, results and conclusions reported in this paper are those of the authors and are independent from the funding sources. No endorsement by ICES or the MOHLTC is intended or should be inferred. The analyses, conclusions, opinions and statements expressed here are those of the author, and not necessarily those of CIHI.
Competing interests None declared.
Ethics approval Research ethics board approval was obtained from the University of Toronto, The Hospital for Sick Children, and Sunnybrook Health Sciences Center.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Public availability of ICES data would compromise patient privacy. More information can be found at http://www.ices.on.ca/Data-and-Privacy/Privacy%20at%20ICES. Requests to access data may be submitted to Data & Analytic Services at das@ices.on.ca or via the following link http://www.ices.on.ca/Data-Services.