Article Text

Abstract
Objective Focusing on efficacy and tolerability, we compared linagliptin monotherapy with voglibose monotherapy in patients with type 2 diabetes undergoing hemodialysis (HD).
Research design and methods In this multicenter, randomized, open-label, parallel-group, active-controlled study, 78 patients were randomized (1:1) to receive a 12-week treatment with 5 mg linagliptin once daily or 0.2 mg voglibose three times a day. To assess whether linagliptin was superior to voglibose, the primary efficacy end point was the change in glycated hemoglobin (HbA1c) level between baseline and week 12. Secondary efficacy end points included changes between baseline and week 12 in glycated albumin (GA) and casual plasma glucose (PG) levels.
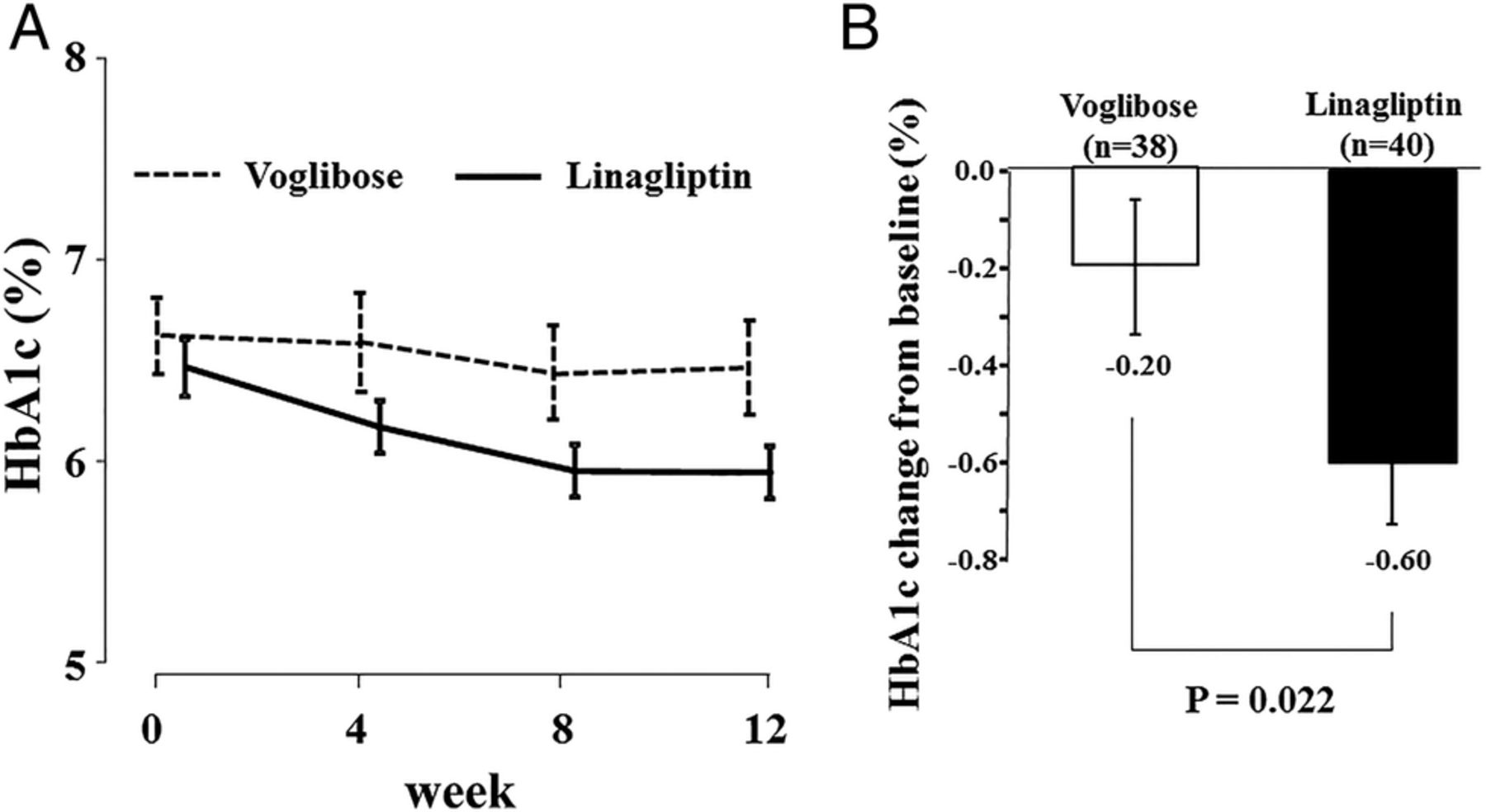
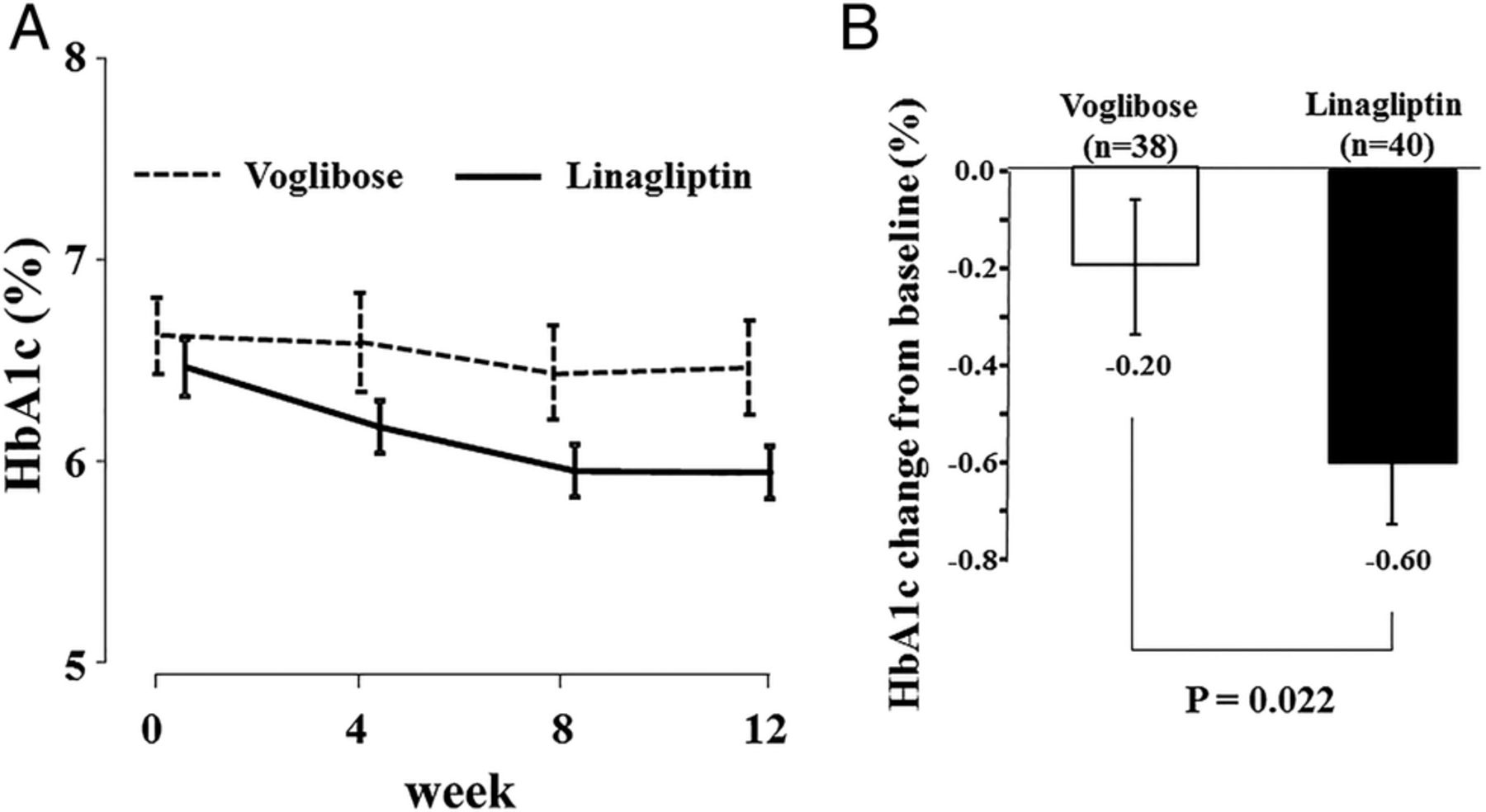
Results At week 12, the adjusted mean HbA1c levels had decreased by −0.60% after treatment with linagliptin and by −0.20% after treatment with voglibose (treatment difference: −0.40%, 95% CI −0.74% to −0.06%, p=0.022). A significant reduction in casual PG level was also observed after treatment with linagliptin compared with treatment with voglibose. Relative to voglibose, linagliptin tended to elicit reductions in GA, although without statistical significance. No hypoglycemic symptoms or severe hypoglycemia occurred during the study.
Conclusions In patients with type 2 diabetes undergoing HD, linagliptin monotherapy provided significantly better glycemic control without severe hypoglycemia than voglibose monotherapy. Linagliptin represents a promising agent for glycemic management in patients with type 2 diabetes undergoing HD.
Trial registration number UMIN000007635; results.
- Nephropathy
- A1C
- Oral Antidiabetics
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
Although appropriate glycemic control could decrease mortality in patients with diabetes and end-stage renal disease, an indication of oral antidiabetic drugs is limited in this population.
Under this situation, the emergence of dipeptidyl peptidase-4 inhibitors is delightful news. Among them, linagliptin does not require dose adjustment because of non-renal excretion.
In patients with type 2 diabetes undergoing hemodialysis, linagliptin monotherapy provided superior glycemic control without severe hypoglycemia, compared with voglibose monotherapy. Linagliptin represents a promising agent for glycemic management in this population.
Introduction
In contrast to the clear evidence in support of strict glycemic control in the early stages of diabetic nephropathy, strict glycemic control in patients with diabetes and advanced end-stage renal disease (ESRD) is challenging and controversial. Currently, hypoglycemia is considered harmful in patients with diabetes;1 this may also be true in patients with ESRD. Recent large observational cohort studies have shown that the association between glycemic control, represented by glycated hemoglobin (HbA1c) level, and mortality could produce U-shaped or J-shaped curves in patients with diabetes undergoing hemodialysis (HD)2 ,3 or in those with stage 3/4 chronic kidney disease (CKD).4 These findings suggest that antihyperglycemic treatment is necessary to prevent the progression of macrovascular complications and infection,5 ,6 but the avoidance of hypoglycemia is indispensable, although the most suitable range of glycemic control remains unclear.
Insulin therapy is the treatment of choice in patients with diabetes and renal insufficiency (RI).7 In clinical practice, the limited availability of oral antidiabetic drugs (OADs) suitable for use in patients with RI is a serious problem.8 ,9 The introduction of dipeptidyl peptidase-4 (DPP-4) inhibitors, which are characterized by a low risk of hypoglycemia, was a boon for patients with type 2 diabetes and moderate-to-severe RI. Indeed, a 12-week treatment with 2.5 mg saxagliptin (half of the regular dose) once daily in combination with background therapy, caused a significant reduction in HbA1c level compared with a placebo,10 and this reduction was maintained throughout a 52-week treatment.11 Furthermore, saxagliptin therapy was well tolerated, with a safety profile comparable to that of the placebo.10 ,11 Similarly, 50 mg vildagliptin (half of the regular dose) once daily added to ongoing antidiabetic therapy for 24 weeks elicited a significant decrease in HbA1c level relative to a placebo, and demonstrated a safety profile similar to that of the placebo.12 The efficacy and safety of sitagliptin monotherapy were compared with those of glipizide, a sulfonylurea, in patients with moderate-to-severe RI13 or ESRD undergoing dialysis.14 As a result, 50 mg (half of the regular dose) or 25 mg (a quarter of the regular dose) sitagliptin once daily exhibited a similar ability to reduce the HbA1c level to that of glipizide after 54 weeks of treatment, confirming the non-inferiority of sitagliptin relative to glipizide.13 ,14 Importantly, hypoglycemia was significantly lower in the sitagliptin group compared with the glipizide group.13 ,14
Although these findings belie the efficacy and safety of DPP-4 inhibitors, most DPP-4 inhibitors require dose adjustment because of the accumulation of the parent drugs and their active metabolites in patients with RI.8 ,9 ,15 Conversely, linagliptin exhibits unique drug kinetics: it is hardly metabolized and is mainly excreted by non-renal routes.16 A pharmacokinetic study demonstrated that the area under the curve of linagliptin exposure in patients with ESRD receiving HD did not exceed a twofold increase compared with individuals with normal renal function.17 Therefore, in contrast to most DPP-4 inhibitors, linagliptin does not require dose adjustment in patients with RI, making it an ideal OAD for use in this population. Although few reports are available, one randomized, placebo-controlled study reported that linagliptin significantly improved glycemic control without unacceptable adverse effects (AEs) in patients with type 2 diabetes and severe RI (mainly CKD stage 4/5).18 However, the efficacy and safety of linagliptin in patients with ESRD undergoing HD (CKD stage 5D) remain unclear because of the problems caused by HD in addition to the deleterious influence of RI.19 HD can have considerable yet unpredictable effects on glycemic control and the blood concentration of drugs.19
In this study, we compared the efficacy and tolerability of linagliptin monotherapy with those of monotherapy with the α-glucosidase inhibitor voglibose monotherapy, which was used in patients with type 2 diabetes receiving HD in Japan, during a 12-week treatment period.
Research design and methods
Study design and participants
This study (the Osaka Diabetes Mellitus and Kidney Diseases (Diamond) Study-1) was a multicenter, randomized, open-label, parallel-group, active-controlled study involving Japanese patients attending 15 centers in Japan. The first patient was enrolled on July 6, 2012, and the final patient visit occurred on July 8, 2014.
Eligible patients were men and women with type 2 diabetes undergoing stable maintenance HD aged ≥20 years and with a HbA1c level ≥4.6% and ≤10% or a glycated albumin (GA) level ≥18% and ≤30%. GA level was adopted as an inclusion criterion because HbA1c level is often underestimated in this population as a result of renal anemia and/or the use of erythropoiesis-stimulating agents (ESAs). The lower limit for HbA1c level (4.6%) was calculated based on the underestimation of HbA1c level by ∼30% in patients receiving HD,20 which is estimated to be equivalent to 6.5% in patients not receiving HD. The main exclusion criteria were: treatment with any type of insulin; impaired hepatic function (aspartate transaminase (AST) ≥100 IU/L or alanine transaminase (ALT) ≥100 IU/L); malignant tumors; and untreated diabetic retinopathy.
This study adhered to the Declaration of Helsinki. After an explanation of the study objectives, all patients gave written informed consent to participate. The study protocol was approved by the Local Ethics Committee at Osaka City University Graduate School of Medicine, Osaka, Japan (registration number 2209). It was also approved by the independent ethics committee or institutional review board at each participating center. The clinical trial registration number is University Hospital Medical Information Network-Clinical Trials Registry 000007635.
Study patients who met the eligibility criteria at screening were enrolled. Patients treated with any OAD underwent a washout period of at least 4 weeks. Blood samples were collected from the arteriovenous fistula just before starting the HD session. To prevent disparities between facilities, HbA1c, GA, and casual plasma glucose (PG) values were measured by a central laboratory (SRL, Tokyo, Japan) 2 weeks before randomization. HbA1c, GA, and casual PG levels were measured in the same manner every 4 weeks during the study period. HbA1c level was measured using the latex agglutination immunoassay, and was expressed as a National Glycohemoglobin Standardization Program equivalent value, as defined by the Japan Diabetes Society.21 GA was measured by an enzymatic method using the Lucica GA-L kit (Asahi Kasei Pharma, Corp., Tokyo, Japan), as previously reported.20 The estimated glomerular filtration rate was calculated as per guidelines proposed by the Japanese Society of Nephrology.22
On the basis of the preinterventional HbA1c values, patients were randomized (1:1) to receive either 5 mg linagliptin once daily or 0.2 mg voglibose three times a day for 12 weeks. The allocation was stratified by HbA1c level (≤6.4%, 6.5–8.4%, ≥8.5%), sex, and age (≤69 or ≥70 years), using a computer-generated allocation schedule. Participants were instructed to take linagliptin each morning after breakfast or voglibose immediately before the three main meals. During the study, participants were excluded (as considered appropriate by the investigator) if their casual blood glucose was ≥400 mg/dL or HbA1c level was ≥10% in two consecutive measurements.
Study end points and assessments
The prespecified primary efficacy end point was the change in HbA1c level between baseline and week 12. Secondary efficacy end points included changes in GA and casual PG levels between baseline and week 12. Safety evaluations included AEs, clinical laboratory tests, and documentation of hypoglycemia episodes. Hypoglycemia was defined as any hypoglycemia symptoms or a casual blood glucose level <50 mg/dL as evaluated by finger-stick blood testing.
Statistical analyses
The primary hypothesis of this study was the superiority of linagliptin over voglibose for HbA1c reduction at week 12. This analysis was performed on the full analysis set (FAS), using the last observation carried forward (LOCF) technique to impute missing data. The FAS included randomized participants who received at least one dose of the study drug and had a baseline HbA1c level measurement. To support this analysis, a sensitivity analysis of the change from baseline in HbA1c level was also performed in the FAS cohort without LOCF.
Sample size was selected by reference to a prior randomized controlled trial.23 We calculated that a sample of 36 participants per group would give the study 80% power, at a two-sided significant level of 5%, to demonstrate the superiority of linagliptin over voglibose, based on a difference of 0.4% and an SD of 0.6% for HbA1c changes between 50 mg sitagliptin once daily and 0.2 mg voglibose three times a day at week 12 in Japanese patients with type 2 diabetes lacking RI.23 Since we anticipated that some participants would discontinue the study, we planned to enroll 80 participants.
We used an analysis of covariance model, with the treatment and stratification factors as fixed effects and corresponding baseline values as covariates, to assess the primary and continuous secondary end points. The least squares (LS) mean differences and two-sided 95% CIs were estimated for the comparison of linagliptin and voglibose. Adherence to the treatment was evaluated based on patient self-reports every week. The adherence rate was calculated as follows: the actual number divided by the total planned number of drug administrations. For example, if a participant took five tablets of linagliptin a week, the adherence rate was 5/7=71.4%. The difference between each group was analyzed using the Mann-Whitney U-test. Data were expressed as means±SD or medians and IQRs as appropriate. A p value of <0.05 was considered statistically significant.
Results
Participant disposition and baseline characteristics
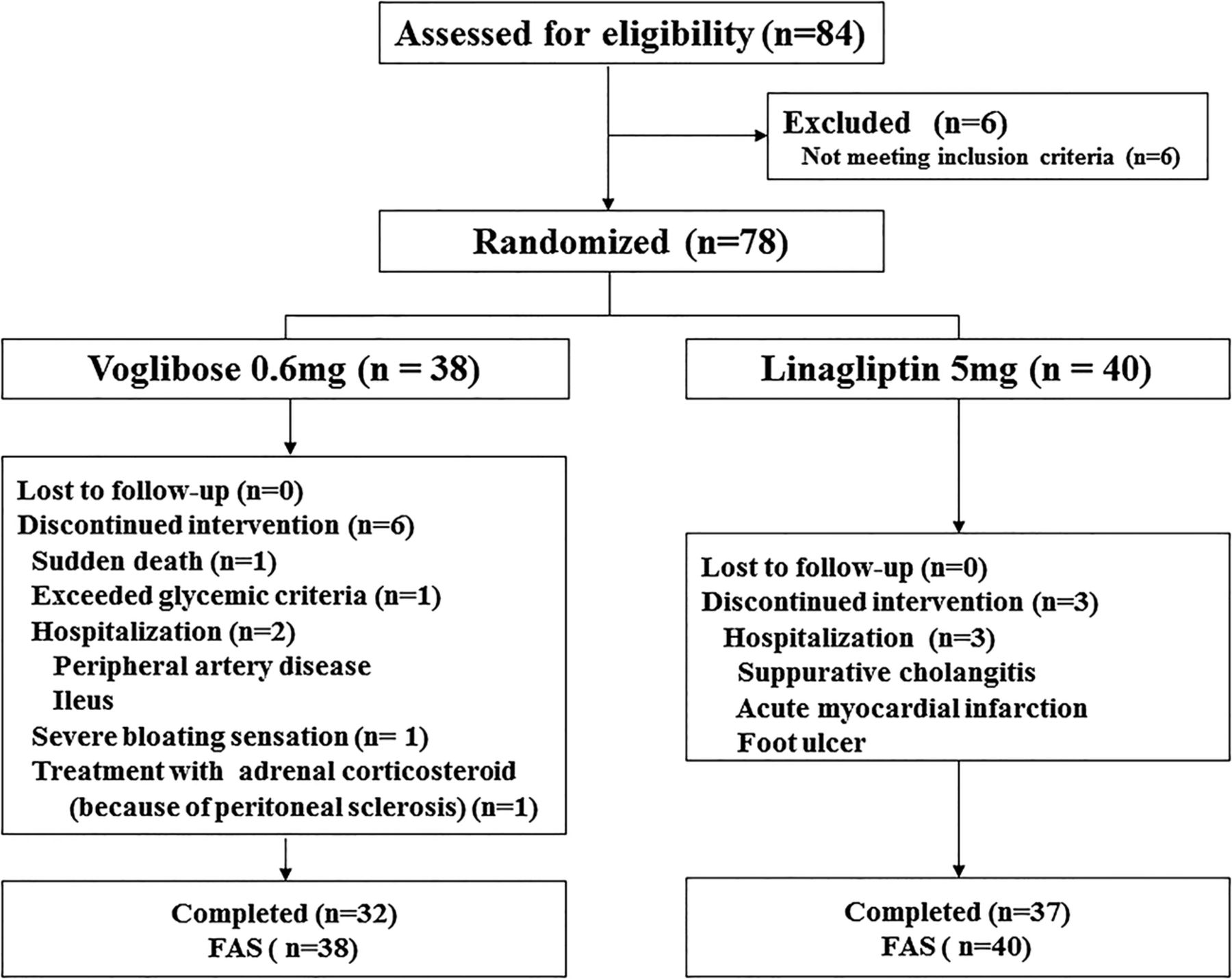
Of 84 participants screened, 78 were randomized to receive linagliptin (n=40) or voglibose (n=38). The treatment groups were balanced with respect to baseline characteristics including HbA1c level, age and sex (table 1). Fifty-one patients were drug naïve, and 27 were receiving other OADs before a washout period: 9 were receiving α-glucosidase inhibitors, 8 were receiving DPP-4 inhibitors, 3 were receiving insulin secretagogue (mitiglinide), and 7 were receiving combinations of these drugs. The details of OADs in both groups are shown in table 1.
Clinical characteristics of randomly assigned patients with type 2 diabetes undergoing hemodialysis
Every randomized participant received one or more doses of the study drug. Sixty-nine (88.5%) participants completed the 12-week treatment period. A higher rate of discontinuation was observed with voglibose (84.2%) than with linagliptin (92.5%). The main reason for discontinuation was AEs (figure 1).

Study flow diagram. FAS, full analysis set.
Efficacy
Figure 2A shows HbA1c levels in the two treatment arms. In the FAS cohort, the difference in the LS mean change between baseline and week 12 for patients receiving linagliptin versus those receiving voglibose was −0.40% (95% CI −0.74% to −0.06%, p=0.022; figure 2B). A similar result was obtained by a sensitivity analysis using the FAS cohort (non-LOCF; table 2).
Sensitivity analysis (change from baseline in glycated hemoglobin at 12 weeks)
{kind=link}
{kind=link}
(A) Time course of changes in glycated hemoglobin (HbA1c) (mean±SEM). (B) Changes from baseline to week 12 in adjusted HbA1c (mean±SEM) in the full analysis set (last observation carried forward).
Significantly greater reductions in the casual PG level from baseline to week 12 were attained with linagliptin than with voglibose (−25.38 mg/dL (95% CI −47.58 to −4.08 mg/dL, p=0.021)). Linagliptin tended to elicit a greater reduction in GA level at week 12 relative to voglibose, although the difference was not statistically significant (−1.12% (95% CI −2.37% to 0.13%, p=0.079)).
Safety, tolerability and adherence to drug administration
Severe hypoglycemia was the most common drug-related AE in this study population. Although the prespecified definition of hypoglycemia was any hypoglycemic symptoms or blood glucose <50 mg/dL, it did not occur during this study. The recorded lowest casual PG level was 84 mg/dL. Therefore, we concluded that no participant had a severe episode of hypoglycemia in this study. One patient in the voglibose group discontinued the study on the advice of the attending physician because of severe hyperglycemia (blood glucose: 544 mg/dL). Although one death occurred in the voglibose group during the study period, it was not considered treatment related. The adherence to treatment with voglibose and linagliptin was 85.8% and 94.4%, respectively. There was no significant difference between the groups (p=0.182).
Discussion
This 12-week, randomized, open-label, active-controlled study demonstrated that linagliptin monotherapy is superior to voglibose monotherapy for the reduction of HbA1c levels in patients with type 2 diabetes undergoing HD. Importantly, there were no episodes of severe hypoglycemia in either treatment group.
Although glycemic control in patients with type 2 diabetes and severe RI is challenging, the emergence of DPP-4 inhibitors has enabled antidiabetic treatment using OADs. Linagliptin is theoretically suitable for patients with RI because of its non-renal elimination,16 ,17 and unique antioxidant and anti-inflammatory effects.24 ,25 Indeed, McGill et al18 reported the efficacy and safety of linagliptin in patients with type 2 diabetes and severe RI (mainly CKD stage 4/5) in a randomized, double-blind, placebo-controlled study. However, a few questions remained unanswered by their report. First, since their study involved the addition of linagliptin to glucose-lowering background therapy that included insulin-injection therapy (∼80% of patients), the incidence of hypoglycemia was relatively high. The incidences of moderate (PG level <3 mM=54 mg/dL) and severe hypoglycemia were about 15% and 4.5%, respectively, although no difference was observed between the two groups. Therefore, it is uncertain whether linagliptin was responsible for the hypoglycemic episodes observed. Second, it is unknown whether the efficacy and safety of linagliptin are equivalent in patients receiving HD (CKD stage 5D), because HD itself can have profound effects on glycemic control and drug kinetics.19
In Japan and the USA, dialysates most commonly contain 100 mg/dL (5.55 mM) glucose. Glucose diffusion from the blood into the dialysate according to the gradient of glucose concentration is inevitable.19 Using continuous glucose monitoring (CGM), we previously demonstrated a drastic, HD-induced decline in blood glucose during HD sessions.26 Curiously, HD can lower blood glucose levels to <100 mg/dL (5.55 mM)–that is, the glucose concentration of the dialysate–by poorly understood mechanisms.19 Thus, HD-induced hypoglycemia can occur during or immediately after HD in some patients. To compound matters, insulin is known to be adsorbed by the dialyzer during HD.27 In some patients, especially those with poor glycemic control, HD-associated hyperglycemia persists long after HD because of insulin deficiency combined with stimulation of counter-regulatory hormones in response to glucose removal by HD.28 Therefore, hypoglycemia and/or hyperglycemia with large fluctuations in blood glucose levels can occur in an unpredictable fashion, especially on HD day.19
In this difficult situation, the glucose-dependent action of DPP-4 inhibitors such as linagliptin on insulin stimulation and glucagon suppression is very attractive. In this study, we first demonstrated the potency of linagliptin compared with its active comparator, voglibose, in patients with type 2 diabetes undergoing HD. The HbA1c-lowering efficacy of linagliptin was −0.6%, which is almost comparable to that of sitagliptin in patients with type 2 diabetes lacking RI, as described in a previous report.23 Considering that linagliptin has a high affinity with both serum proteins and DPP-4 compared with other DPP-4 inhibitors, it is unlikely that linagliptin is removed by HD.16 Taken together, our findings suggest that linagliptin shows an equivalent efficacy and a low frequency of hypoglycemia even in patients receiving HD, possibly through some degree of automatic glycemic stabilization, a unique characteristic of incretin-related drugs.
One fundamental problem is that no accurate marker of glycemic control exists in patients receiving HD. It is established that the absolute value of HbA1c underestimates the actual glucose level. Instead, GA is used as an alternative marker because it is less affected by renal anemia and/or the use of ESAs.20 ,29 However, in a recent report from the consensus conference of the American Diabetes Association (ADA) in collaboration with the American Society of Nephrology and the National Kidney Foundation, consideration of GA as a definitive marker on a worldwide scale was described as premature, because GA is unavailable, especially in the USA, and outcome studies are limited.30 ,31 The ADA also stated, “Measurement of A1C should still be performed, as the trending of the levels can assist in therapy decisions.”30 ,31 Indeed, we observed a time-dependent predictive improvement in HbA1c level following linagliptin treatment, although the exact HbA1c value was very low compared with GA level, which may indicate the absolute glycemic level more accurately than the HbA1c level. (In this study, baseline GA level was 23%, which is comparable to ∼8% of the HbA1c level).
In contrast to the improvement of HbA1c and casual PG, we did not detect statistically significant reduction of GA after treatment with linagliptin compared with treatment with voglibose. One possible explanation may be that we configured the sample size based on the changes in HbA1c but not GA in a previous randomized controlled trial.23 Another possibility may be due to the characteristic of voglibose which can effectively suppress postprandial glucose (PPG) level. It has been reported that GA showed stronger correlation with PPG, compared with HbA1c.32 Therefore, the suppression of PPG by voglibose might reduce the difference in GA between the groups.
Cardiovascular disease (CVD) events are a leading cause of death in patients undergoing HD.33 ,34 To prevent CVD, appropriate glycemic control is desirable in patients with type 2 diabetes undergoing HD. However, limited therapeutic options exist in terms of OADs, and the risk of hypoglycemia is profound in this population. In this situation, DPP-4 inhibitors are a suitable choice, although until now clear evidence that DPP-4 inhibitors improve CVD events and mortality is lacking. Currently, HbA1c is prevented from decreasing too much, because too much glycemic control by antidiabetic treatments prone to causing hypoglycemia, such as sulfonylureas and/or insulin, may lead to a poor prognosis. However, a recent prospective study has provided new insights into this stereotype. Trivin et al35 investigated the association between HbA1c levels in individuals without diabetes (<6.5%) and mortality in patients with CKD (mainly stage 3/4). Intriguingly, they found that a higher HbA1c level was associated with a significantly higher mortality risk, even in the prediabetic range.35 Therefore, we believe that antihyperglycemic treatment will achieve a better outcome in patients with type 2 diabetes undergoing HD, unless a hypoglycemic episode occurs.
This study has several limitations. First, the study period of 12 weeks was short. Therefore, we cannot make conclusions about the longer term efficacy and safety of linagliptin in patients with type 2 diabetes undergoing HD. Second, we were unable to evaluate mild or moderate hypoglycemia. However, in a previous study, we observed no apparent hypoglycemia, as evaluated by CGM, following monotherapy with the DPP-4 inhibitor teneligliptin in patients with type 2 diabetes undergoing HD.26 Thus, it is unlikely that linagliptin monotherapy would be prone to cause hypoglycemia. Finally, we did not directly measure the blood concentration of linagliptin before and after HD, although HD sessions did not seem to alter its glucose-lowering effects.
In summary, we have shown that, compared with voglibose monotherapy, linagliptin monotherapy provides superior glycemic control without severe hypoglycemia in patients with type 2 diabetes undergoing HD. We conclude that linagliptin is a promising agent for glycemic management in patients with type 2 diabetes undergoing HD.
References
Footnotes
Collaborators The Diamond Study Group: A Ochi (Ikeda Hospital); K Shidara (Izumiotsu Municipal Hospital); S Tsuchikura, N Kawano, N Shimomura, Y Tsujimoto, T Tabata (Inoue Hospital); H Shima, M Okamura (Ohno Memorial Hospital); T Fujii, S Okada (Okada Clinic); K Goto (Ono Naika Clinic); T Wakikawa (Sakai Onshinkai Hospital); N Tsuboniwa, K Norimine, S Shoji (Shirasagi Minami Clinic); K Adachi (Kitatatsumi Shirasagi Clinic); K Maekawa (Fujiidera Shirasagi Clinic); T Kitai, R Mori, H Nagayama (Nagayama Clinic); T Hamada (Marie Clinic); R Kakiya (Meijibashi Hospital); N Yoshida (Yoshida Toseki Clinic); M Kimura, H Fujii (Center for Drug and Food Clinical Evaluation, Osaka City University Hospital); M Fukui (Department of Stochastics, Osaka City University Graduate School of Medicine).
Contributors KM contributed to the design of the study; collection and statistical analysis of data; and to the writing of the manuscript. ME contributed to the design of the study; and to the collection and statistical analysis of data. TS and MI participated in conducting the study; interpretation of data; and in the writing of the manuscript. All of the authors are fully responsible for all content and editorial decisions and have approved the final version. KM is the guarantor of this work; he had full access to all data in the study and takes responsibility for the data.
Funding KM, ME, TS and MI received unrestricted research grants from Mitsubishi Tanabe Pharma Corporation, Daiichi Sankyo Co., Astellas Pharma, Asahi Kasei Pharm Corporation, Kyowa Hakko Kirin Co., Chugai Pharmaceutical Co., Teijin Pharma, Takeda Pharmaceutical Company, and Ono Pharmaceutical Co.
Competing interests KM received an honorarium for lecturing from Mitsubishi Tanabe Pharma Corporation, Daiichi Sankyo Co., Sanofi, and Nippon Boehringer Ingelheim Co. ME received an honorarium for lecturing from Sanofi, Nippon Boehringer Ingelheim Co., Mitsubishi Tanabe Pharma Corporation, Daiichi Sankyo Co., Takeda Pharmaceutical Company, Eli Lilly Japan K.K., Sumitomo Dainippon Pharma Co., and Ono Pharmaceutical Co. TS received an honorarium for lecturing and/or a research grant from Asteras, Bayer in Japan, Nippon Boehringer Ingelheim Co., Chugai Pharmaceutical Co., Daiichi Sankyo Co., Fuso, Kyowa Hakko Kirin Co., Mochida Pharmaceutical Co., MSD K.K., Novo Nordisk Pharma, Pfizer, and Takeda Pharmaceutical Company. MI received an honorarium for lecturing from Mitsubishi Tanabe Pharma Corporation, Daiichi Sankyo Co., Astellas Pharma, Asahi Kasei Pharm Corporation, Kyowa Hakko Kirin Co., Chugai Pharmaceutical Co., Teijin Pharma, Takeda Pharmaceutical Company, Eli Lilly Japan K.K., MSD K.K., Bayer in Japan, and Ono Pharmaceutical Co.
Patient consent Obtained.
Ethics approval The Local Ethics Committee at Osaka City University Graduate School of Medicine, Osaka, Japan (registration number 2209).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.