Article Text

Abstract
Objectives Investigate potential association between pioglitazone exposure and risk of prostate cancer.
Research design and methods Nested, matched case–control study. UK primary care data (Clinical Practice Research Datalink (CPRD) GOLD) linked to inpatient (Hospital Episode Statistics (HES)) and cancer registry (National Cancer Information Network (NCIN)) data. English men aged ≥40 years diagnosed with type 2 diabetes mellitus, January 1, 2001 to January 5, 2015. Cases, with prostate cancer diagnosis, matched with up to 4 controls by age, cohort entry date and region. ORs for association of exposure to pioglitazone to incident prostate cancer, adjusted for potential confounders.
Results From a cohort of 47 772 men with 243 923 person-years follow-up, 756 definite cases of prostate cancer were identified. Incidence was 309.9/100 000 person-years (95% CI 288.6 to 332.8). Pioglitazone use was not associated with prostate cancer risk; adjusted OR 0.759, 95% CI 0.502 to 1.148. Analyses showed no difference when possible cases, prostate cancer in CPRD GOLD only, included (adjusted OR 0.726, 95% CI 0.510 to 1.034). No association when adjusted for channeling bias (OR 0.778, 95% CI 0.511 to 1.184) or limited to an index date prior to July 1, 2011 (adjusted OR 0.508, 95% CI 0.294 to 0.879), despite prostate-specific antigen screening occurring more frequently among cases than controls (81.6% of 756 definite cases cf. 24.2% of 2942 controls (p<0.01)). No association with duration of pioglitazone use, increasing pioglitazone dose or increasing time since initiation.
Conclusions In this real-world, nested matched case–control study, exposure to pioglitazone was not associated with increased risk of prostate cancer.
- Type 2 Diabetes
- Prostate Cancer
- Thiazolidinediones
- Humans
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
In this observational, real-world, nested matched case–control linkage study using the large, representative, primary care Clinical Practice Research Datalink (CPRD) GOLD database from the UK, exposure to pioglitazone was not associated with an increased risk of prostate cancer in patients with type 2 diabetes mellitus; OR 0.759, 95% CI 0.502 to 1.148.
There was no association with increasing pioglitazone dose or duration or with increasing time since pioglitazone initiation.
There was no association between any other types of antidiabetic medication and the risk of prostate cancer.
Data from this observational, real-world, population-based study provides additional new evidence to support a positive benefit:risk profile for pioglitazone.
Introduction
Diabetes mellitus is one of the most common chronic diseases worldwide and its global prevalence continues to increase due to urbanization, ageing population, obesity and changes associated with lifestyle such as physical inactivity. The WHO estimated that, in 2014, there were ∼422 million adults (8.5% of the population) with diabetes compared with 108 million (4.7%) in 1980.1 According to Diabetes UK reports, there are ∼4 million people living with diabetes in the UK.2
Among men, prostate cancer is the most common cancer, with an overall reported incidence of 307/100 000 men aged 40 years and older3 and is the second most common cause of cancer-related death, after lung cancer. One in eight men will be diagnosed with prostate cancer during their lifetime. Prostate cancer incidence rates have more than doubled since the late 1970s, though this is thought to be associated with intensified diagnostic efforts and, with greater screening, over 90% of men aged 50–69 years diagnosed with prostate cancer survive for 5 years or more.4 Evidence indicates that the incidence of prostate cancer among patients with type 2 diabetes mellitus (T2DM) is 320/100 000 person-years.5
Pioglitazone is an agonist of peroxisome proliferator-activated receptor-γ (PPARγ) and an antidiabetic drug in the thiazolidinedione (TZD) class used to treat T2DM. First authorized for use in the European Union (EU) in October 2000, pioglitazone has been used in the UK as a third-line treatment to improve glycemic levels in patients with T2DM, following patient education and treatment with metformin.6 ,7
In the preclinical studies of pioglitazone, tumors were observed in the urinary bladder of male rats, but not in female rats or mice of either gender.8 Drug-induced tumors were not observed in any other organ. Specifically, there were no treatment-related prostate tumors in the 2-year carcinogenicity studies in rats and mice. In a mechanistic study, expression of PPARγ and the inhibitory effects of TZDs on tissue samples from patients with prostate cancer, benign prostatic hyperplasia (BPH) and normal prostate tissue were investigated.9 Significant expression of PPARγ was observed in prostate cancer cells, whereas normal prostate cells and BPH cells had minimal expression of PPARγ. Exposure of prostate cancer cell lines to TZDs resulted in marked inhibition of tumor cell growth. This finding suggests that pioglitazone may play a role in the prevention and/or treatment of prostate cancers.
Following continued concern suggesting a potential association between exposure to pioglitazone and the risk of bladder cancer, a US-based long-term study using the Kaiser Permanente Northern California (KPNC) database was carried out, which investigated both bladder cancer and also other common cancers in patients with diabetes. In this analysis, there was no association with 8 of the 10 additional cancers; however, ever use of pioglitazone was associated with a small increase in the HR for prostate cancer (HR 1.13, 95% CI 1.02 to 1.26).10
To investigate whether cardiovascular and macrovascular effects observed with pioglitazone during the PROspective pioglitAzone Clinical Trial In macroVascular Events (PROactive) trial would be maintained over time, a 10-year, observational, follow-up study was conducted after the double-blind treatment phase had been completed. During both study periods combined (original clinical trial and 10-year observational period), prostate cancer was reported in 58 men in the pioglitazone group (3.3%) and 35 men in the placebo group (2.0%; risk ratio 1.59, 95% CI 1.04 to 2.41).11
In the Insulin Resistance Intervention after Stroke (IRIS) trial, which was an international, double-blind, placebo-controlled clinical trial and was designed to test the hypothesis that pioglitazone would reduce the rates of stroke and myocardial infarction after ischemic stroke or transient ischemic attack in patients without diabetes who have insulin resistance, the primary outcome of stroke or myocardial infarction occurred in 175 of 1939 patients (9.0%) in the pioglitazone group and in 228 of 1937 (11.8%) in the placebo group (HR in the pioglitazone group 0.76; 95% CI 0.62 to 0.93). In this study, the total incidence of cancer did not differ significantly between the two groups and the number of patients with adjudicated prostate cancer was reported as 28 (1.4%) and 25 (1.3%) for pioglitazone and placebo, respectively (p=0.68).12
In addition, a retrospective population-based cohort study of 204 741 Taiwanese men aged 40 years and older showed no association between pioglitazone use and the risk of prostate cancer (OR 0.77, 95% CI 0.10 to 5.75).13
Considering the mixed results from these randomized trials and observational studies and the fact these studies were not specifically designed to evaluate prostate cancer risk, this current study using data from the Clinical Practice Research Datalink (CPRD) GOLD database was designed to further investigate a potential association between pioglitazone use and prostate cancer. Specifically, a matched case–control study nested in a cohort of men aged 40 years and older diagnosed with T2DM between January 1, 2001 and January 5, 2015 was conducted to evaluate the potential association of exposure to pioglitazone and risk of prostate cancer in a cohort of male patients with T2DM.
Research design and methods
Setting
The study protocol was approved by the Independent Scientific Advisory Committee (ISAC). CPRD GOLD is one of the largest primary care databases in the UK, containing electronic records from 643 general practices, which include patients' demographics, diagnoses, referrals, tests and prescriptions. CPRD has been used for a range of safety studies involving commonly prescribed drugs.14–16 Following ISAC approval, data for patients in the CPRD GOLD was linked to their medical records in Hospital Episode Statistics (HES) inpatient data (containing details of all admissions and day case management of patients to National Health Service (NHS) hospitals in England)17 and the National Cancer Information Network (NCIN), a UK-wide partnership operated by Public Health England, driving improvements in standards of cancer care and clinical outcomes by improving and using information collected about patients with cancer for analysis, publication and research. The National Cancer Registration Services (NCRS) in England, Northern Ireland, Scotland and Wales collect information about every patient diagnosed with cancer. The NCIN brings this data together for England into a National Cancer Data Repository (NCDR) and links it to additional data including surgery, radiotherapy and care in general practice. Where possible, data are linked at the UK level.18
Participants
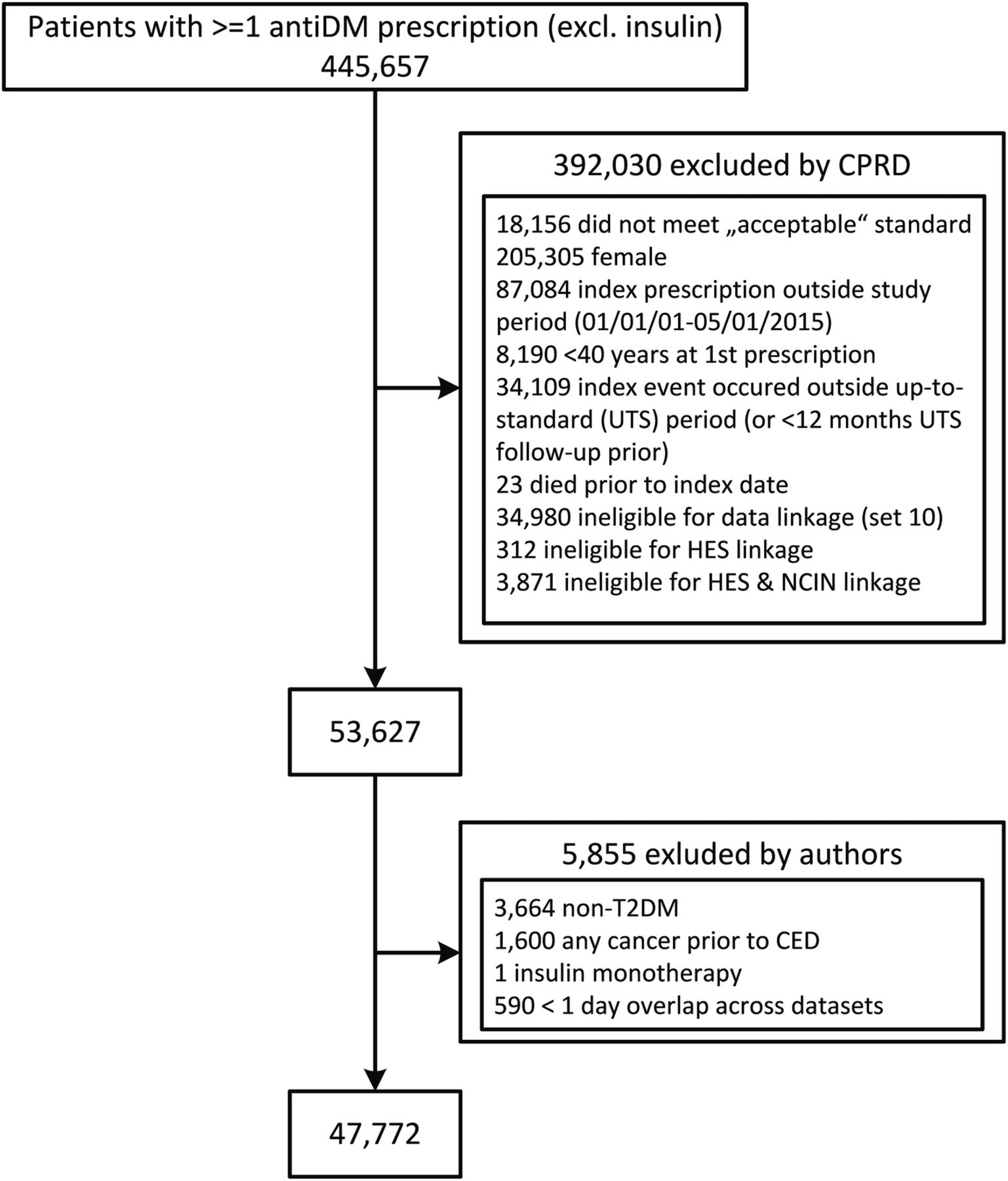
Cohorts of acceptable16 male patients aged ≥40 years who received their first prescription for an antidiabetic medication (other than insulin monotherapy) between January 1, 2001 and January 5, 2015, who were registered at general practices considered ‘up to standard’16 and had at least 1 day of overlapping follow-up time in the CPRD GOLD, HES and NCIN data at any time during the study period were identified. To identify the first antidiabetic medication prescription, patients' entire available medical histories were reviewed, starting from enrolment in the CPRD GOLD. The date of first prescription was considered their cohort entry date (CED) and patients were excluded if they were <40 years of age at CED, had a diagnostic record of type 1 diabetes mellitus at any time or were diagnosed with prostate cancer, prostate carcinoma in situ (CIS), prostatic intraepithelial neoplasia (PIN), prostatic neoplasms of uncertain behaviors or metastatic cancer of any site (including secondary malignancies of the prostate) in the CPRD GOLD, HES or NCIN data prior to their CED (figure 1).
{kind=link}
Creation of study population for the nested case–control study. CED, cohort entry date; CPRD, Clinical Practice Research Datalink; DM, diabetes mellitus; HES, Hospital Episode Statistics; NCIN, National Cancer Information Network; T2DM, type 2 diabetes mellitus.
Outcome definition
Definite cases were defined as those with a first recorded (ie, incident) diagnosis of prostate cancer in either HES or NCIN, recorded between the CED and the end of follow-up. A possible case was a patient whose diagnosis of prostate cancer had been recorded in CPRD GOLD only.
Matching
Each case was matched with up to four controls by age at CED ±3 years, CED ±6 months and region. All controls were alive and registered with the general practice on the date of the first recorded diagnosis of cancer in their matched case, which was defined as the index date for each case and their matched controls. Patients were included only if they had at least 1 year of data before their index date, to ensure the completeness of records.
Statistical analyses
The primary measure of exposure to pioglitazone was assessed from prescription information within the observation period from the date of patient's registration with the general practice to the index date. A patient was considered to be exposed to pioglitazone if they had at least two prescriptions within a 6-month period, the first of which was on or after the CED; the date of their second pioglitazone prescription was deemed the start of their exposure. Exposure was treated as unidirectional time-dependent variables, that is, once a patient met the exposure definition, the patient was considered exposed from that point forward, even if they discontinued the medication. Exposure to each of the other antidiabetic medications was classified in a similar fashion. Eligible cohort members were categorized as ‘ever exposed’ to another antidiabetic medication at the time they received at least two prescriptions for that medication within a 6-month period.
Cumulative duration of exposure was calculated in days, by counting the number of days between prescriptions, starting with the second prescription, considering gaps of fewer than 30 days between proximate prescriptions as continuous treatment and was truncated at the index date. Duration was evaluated as a continuous and categorized variable (evaluated in months: <12, 12–23, 24–35, 36–59, ≥60). The cumulative dose of pioglitazone exposure was calculated by summing the doses of each prescription and was similarly truncated at the index date. Dose was evaluated as a continuous and as a categorized variable (evaluated in mg as 1–9000, 9001–25 000, 25 001–50 000, ≥50 001). Tests for trend were performed.
All available data were used in the analyses; p<0.05 was considered as significant, but to create a parity of presentation with other studies, a 95% CI is quoted in the results.
The detectable ORs for a range of powers (derived from Fisher's exact test), assuming α=0.05, two-sided, four controls per case and 1000 cases, and 10% usage of pioglitazone among controls,19 indicated that an OR of 1.38 would be detected with a power of 0.8, 1.4 with 0.85, 1.44 with 0.9 and 1.49 with 0.95.
SAS V.9.4 was used for the statistical analyses.
Covariates
Several covariates were assessed to evaluate confounding caused by established risk factors for cancer; patients' entire available medical histories were reviewed, from enrolment in CPRD GOLD.
Body mass index (BMI)20 ,21 as a continuous variable was measured at the date up to 3 months before or 1 month after the index date. Smoking status22 ,23 (‘yes’ if he had one or more records of current or past smoking in their record in the period up to, or 1 month after, either the CED or the index date and ‘no’ if he had at least one smoking status record of ‘never’ having smoked in their record in the same period), alcohol consumption24 ,25 (using Read codes for alcohol status) and ethnicity26 ,27 (white or not recorded, black, Asian, other) were based on the latest values recorded before the index date.
Diabetes-related variables were also assessed as potential confounders; duration of diabetes, exposure to antidiabetic medications other than pioglitazone (metformin, sulfonylureas, insulins, TZDs and other antidiabetic medications than the classes above), history of diabetic renal complications and congestive heart failure.
Other potential confounders of interest included history of testosterone replacement therapy,28 ,29 history of vasectomy,30 ,31 history of prostate inflammation/prostatitis,32 ,33 history of BPH diagnosis, treatment or procedure,34 history of bladder cancer, other urological cancers and hematuria.35 ,36
Owing to a media announcement in July 2011, when risk minimization measures were introduced in the pioglitazone products EU prescribing information regarding bladder cancer, heart failure and the need for regular review of the benefits of therapy, which may have affected the prescribing of pioglitazone and/or the detection of prostate cancer among those exposed, the analysis was limited to only cases and controls where the index date occurred prior to July 1, 2011. Detection bias was further explored by examining whether there was differential use of prostate-specific antigen (PSA) screening in the 3 years prior to index date, between patients exposed and unexposed to pioglitazone.
Potential confounders were defined as variables that changed the unadjusted OR for pioglitazone use by >5%—a more conservative approach than the often used 10%.
No imputation of missing data was conducted; analysis was limited to the observed data. For categorical covariates, missing data were included as a separate stratum.
Main outcome measure
Conditional logistic regression was used to estimate ORs with 95% CIs based on Wald tests to examine the effects of pioglitazone exposure, duration and dose of exposure on prostate cancer risk.
The primary analysis was based on exposure to pioglitazone after CED and before the index date. Several sensitivity analyses were carried out. First, a wider case definition may increase the sample size and include patients who had yet to be formally diagnosed with prostate cancer, so an analysis including the possible cases definition of prostate cancer was conducted. Second, the analyses were replicated using a broader definition of prostate cancer and included CIS or PIN. Third, pioglitazone dose and duration was investigated based on the date of the first prescription, to eliminate immortal time bias.
Results
Patient characteristics
In the total cohort (n=47 772), the mean age at CED was 62.36 years (SD 11.53, range 39–99). The mean duration of follow-up (from CED) was 5.16 years (SD 3.51, range 0.00–14.81) and there was a total of 243 923 person-years.
Patients entered the cohort between 43 and 92 years of age and cases were slightly older than controls (70.3 c.f. 69.5, p<0.01; table 1).
Characteristics of prostate cancer cases and matched controls at CED
More cases were of black British ethnicity (18, 2.4%) than controls (17, 0.6%; table 2). Cases had lower BMI than controls at both time points (p<0.01; tables 1 and 2). Neither smoking history nor alcohol consumption differed between cases and controls at either time point.
Characteristics of prostate cancer cases and matched controls at index date
At index date, cases were more likely to have had more evidence of BPH (history of diagnosis (p<0.01), treatment by surgical procedure (p<0.01)) and less history of heart failure (p=0.04) than controls (table 2).
Cases remained slightly older than controls by their index date (73.4 c.f. 72.6, p<0.01; table 2). Additionally, cases had more months of exposure to sulfonylureas (35.6 c.f. 34.6, p=0.02), fewer months of exposure to TZDs other than pioglitazone (23.8 c.f. 27.6, p=0.01), greater evidence of BPH (history of diagnosis (p<0.01), treatment with 5α reductase inhibitors (p<0.01) and α-blockers (p<0.01), treatment by surgical procedure (p<0.01)), history of hematuria (p<0.01), history of bladder cancer (p<0.01), PSA tests in the 3 years prior to index date (p<0.01), a PSA test result of ≥4 in the 3 years prior to index date (p<0.01), their most recent PSA test result ≥4 (p<0.01) and less history of congestive heart failure (p=0.03) than controls.
Seven hundred and fifty-six cases of prostate cancer were diagnosed in this population; the incidence rate was 309.9/100 000 person-years (95% CI 288.6 to 332.8).
Risk of prostate cancer with pioglitazone use
The analysis of definite cases indicated no risk of prostate cancer associated with exposure to pioglitazone, in either the unadjusted model (OR 0.800, 95% CI 0.560 to 1.143) or that adjusted by potential confounders identified (ie, most recent PSA screening test result prior to index date, history of BPH drug treatment (α-blockers) at index date; OR 0.759, 95% CI 0.502 to 1.148; table 3).
ORs for the association of pioglitazone exposure and prostate cancer
There was no statistically significant increasing risk of prostate cancer with increasing time since pioglitazone initiation (crude p=0.371, adjusted p=0.535; table 3).
There was no association with increasing duration of pioglitazone use (table 3). Cumulative duration of treatment with pioglitazone (included as a continuous variable) was not associated with increased risk of prostate cancer per month (OR 0.999, 95% CI 0.988 to 1.010), by deciles (p=0.370) or by predetermined categories (p=0.08; not presented).
Moreover, there was no association with increasing pioglitazone dose (table 3). The cumulative dose of pioglitazone prescribed (included as a continuous variable) was not associated with increased risk of prostate cancer per gram (OR 0.996, 95% CI 0.983 to 1.009), by deciles (p=0.425) or by predetermined categories (p=0.380; not presented).
All variables were examined as to whether they changed the unadjusted OR for ever exposure to pioglitazone by ≥5%. Two different types of confounders were identified, associated with history of PSA screening/tests at index date (most recent PSA test result, count of PSA tests during 12 months prior to index date and count of PSA tests during 24 months prior to index date) and history of drug treatment for BPH at index date (history of BPH drug treatment with α-blockers at index date). With regard to the PSA variables, that which altered the OR by the largest amount was selected; most recent PSA test result prior to index date.
Ever exposure to pioglitazone, adjusted for most recent PSA test result prior to index date and history of BPH drug treatment (α-blockers) at index date, was not associated with the risk of prostate cancer (OR 0.759, 95% CI 0.502 to 1.148).
No association was observed when the adjusted model included variables to control for channeling bias (ie, adjusted for the following at initiation of pioglitazone; duration of diabetes, history of renal complications and history of congestive heart failure); OR 0.778, 95% CI 0.511 to 1.184.
When analysis was limited to subjects with an index date occurring prior to July 1, 2011, among definite cases, the adjusted OR was 0.508 (95% CI 0.294 to 0.879). PSA screening in the 3 years prior to index date occurred more frequently among cases than controls (81.6% of 756 definite cases c.f. 24.2% of 2942 controls (p<0.01)). To avoid detection bias due to more intensive observation imparted on those with existing cancers, analysis was replicated limited to those with no neoplasms observed prior to the index date. In this population of 386 cases and 1499 controls, pioglitazone exposure was not associated with risk of prostate cancer (OR 0.720, 95% CI 0.408 to 1.273).
Sensitivity analysis
Similar results were observed in the sensitivity analysis when the specificity of the case definition was relaxed to include the possible cases. The analysis of definite and possible cases indicated no risk of prostate cancer associated with exposure to pioglitazone, in either the unadjusted model (OR 0.787, 95% CI 0.584 to 1.059) or that adjusted by potential confounders identified (most recent PSA test result prior to index date and treatment duration with other TZDs at index date), OR 0.726, 95% CI 0.510 to 1.034.
Using a broader prostate neoplasms definition, including CIS and PIN, increased the number of definite cases by 12 (from 756 to 768), to whom 2981 controls were matched; exposure to pioglitazone was not associated with risk of prostate cancer, OR 1.174 (95% CI 0.680 to 2.026). Although this increased the number of cases exposed to pioglitazone from 244 to 256, no association was seen when the exposure period was widened to include exposure from the first prescription of pioglitazone, rather than the second (adjusted OR 0.775, 95% CI 0.518 to 1.161).
Risk of prostate cancer with other antidiabetic medications
No association was found between exposure to any other antidiabetic medication prior to index date and risk of prostate cancer (metformin: OR 1.102, 95% CI 0.879 to 1.380, sulfonylureas: OR 1.120, 95% CI 0.937 to 1.337, insulins: OR 0.936, 95% CI 0.587 to 1.493, TZDs other than pioglitazone: OR 0.847, 95% CI 0.596 to 1.202, other antidiabetic medication: OR 1.017, 95% CI 0.688 to 1.502).
Discussion
This is the first real-world, population-based CPRD GOLD study with linkage to HES and NCIN data that investigated the use of pioglitazone and risk of prostate cancer in men with T2DM. Previously conducted studies were not specifically designed to study the outcome of prostate cancer. In the current study, none of the categories of time since initiation of pioglitazone, cumulative dose, duration of therapy or tests for trend across these categories, were associated with the risk of prostate cancer and indicate no association between pioglitazone use and development of prostate cancer.
The incidence rate of prostate cancer in this diabetic population of English men aged 40 years and older was 309.9/100 000 person-years. This is in line with the officially published incidence of 307/100 000 men aged 40 years and older.3 Pioglitazone exposure was not found to be associated with the risk of developing prostate cancer and no dose or duration responses were observed. This was true regardless of the time period during which analysis was conducted (ie, previous to July 1, 2011, when risk minimization measures were introduced in the pioglitazone products EU prescribing information regarding bladder cancer, heart failure and the need for regular review of the benefits of therapy), the specificity of the case definition (ie, definite cases c.f. definite cases and possible cases c.f. definite cases including those with CIN/PIN) or the specificity of the exposure (ie, from first prescription or from the second prescription within a 6-month period). There was no association between exposure and risk of prostate cancer when channeling bias (ie, duration of diagnosed diabetes prior to index date and history of either renal complications or congestive heart failure at the beginning of pioglitazone therapy) was explored.
A 10-year epidemiological study of 193 099 persons conducted by the University of Pennsylvania using the KPNC database found a small increased HR of prostate cancer among subjects treated with pioglitazone (HR 1.13, 95% CI 1.02 to 1.26).10 However, there was no clear pattern of increased risk with increasing time since initiation, dose or duration of pioglitazone use, which suggests that the observed association is unlikely to be a causal association. Similarly, once adjusted for PSA screening, BPH treatment and proteinuria testing, no statistically significant association remained. Certainly, the KPNC study was a hypothesis generating study and due to the large number of comparisons made in the original study and the post hoc analyses, the observed small (13%) risk of prostate cancer among persons treated with pioglitazone could be due to chance alone and may account for the observation.
Similarly, although prostate cancer was reported more frequently among subjects who had been exposed to pioglitazone than those who received none during the combined 13-year study period of the PROactive observational extension study (relative risk 1.65, 95% CI 1.02 to 2.67), these data require careful interpretation. The PROactive observational extension study was not specifically designed to evaluate the risk of prostate cancer. TZD use and other antidiabetic therapy were not controlled for or specified during the observational period and only a small percentage of the subjects that were randomized to pioglitazone in the original double-blind period of the PROactive study also took pioglitazone during the observational study period. Thus, pioglitazone exposure in subjects in the pioglitazone group during the observational study period was likely to be very low. Also, following the increased media interest in bladder cancer subjects exposed to pioglitazone, there is the possibility of detection bias for urological cancers, which may have resulted in more cases of prostate cancer being identified in the pioglitazone group. In addition, information on PSA testing was not collected in the PROactive observational extension study. Furthermore, age, which is an important risk factor for prostate cancer, may have impacted the results; the age at onset of prostate cancer was higher in the pioglitazone group (median age of 72.0 years) compared with those in the placebo group (median age of 69.0 years).37
In IRIS, the longest double-blind, randomized clinical trial of pioglitazone, involving subjects without diabetes who had a recent history of ischemic stroke or transient ischemic attack and who had insulin resistance, the total incidence of cancer did not differ significantly between the two groups (133 and 150 subjects, respectively; p=0.29). Specifically, during a median follow-up of 4.8 years, the number of subjects with adjudicated prostate cancer was reported as 28 (1.4%) and 25 (1.3%) for the pioglitazone and placebo groups, respectively (p=0.68).11
Strengths and limitations of study
This study has several important strengths. First, this study assembled a large cohort; cases and controls were derived from a study population consisting of 47 772 English men aged 40 years or older with T2DM. Cases and controls contributed 24 052 years of follow-up data (mean duration 6.5 years, SD 3.41). Second, an advantage of using data that have been collected for clinical purposes is the minimization of recall bias. Although subjects may obfuscate the truth around certain exposures (eg, alcohol, smoking) the exposure of interest in this study was based on a prescription record, using an exposure variable that disregarded people who may have never filled their first prescription, or moved to a different drug after one prescription, for any reason. Third, unlike previously conducted studies, this study focused solely on the outcome of prostate cancer. Fourth, pre-recorded information in the CPRD GOLD, completed by general practitioners using an autocomplete function during a routine visit, limits the degree of misclassification of exposure expected. Further, although information regarding potential confounders may have been slightly distorted, the presence of age, BMI and glycated hemoglobin variables in the CPRD GOLD database means that these potential confounders can be examined more closely; sometimes impossible with administrative databases. The nested case–control analyses also allowed for control of potential confounders such as age, region of residence and duration of T2DM. Finally, the CPRD GOLD data was linked with HES and NCIN data, which helped to improve the validity and precision of cancer data diagnosis; thus, improving the confidence of the results and conclusions.
As an observational study, there remains the potential for unmeasured confounding. A very long-term, adequately powered randomized clinical trial, however, would not be possible. Other limitations, such as poor adherence to therapy regimen, still remain. These cannot always be accounted for during design or analysis. This study excludes prescriptions written during inpatient stays in hospital or by specialists. It is, however, expected that these are non-differential, which would bias results towards the null. Additionally, the CPRD GOLD database does not collect information pertaining to risk factors for prostate cancer (eg, familial history, genetic screening), although this limitation would affect both the exposed and unexposed group; therefore, it is unlikely to affect the internal validity of this study. This study showed that PSA tests were conducted more due to suspicion of prostate cancer than due to exposure to pioglitazone; there was no difference between the proportion of pioglitazone users subjected to PSA screening (81/244, 33.2%) and non-pioglitazone users (1248/3454, 36.1%; p=0.356).
Our findings support a positive benefit:risk profile for pioglitazone. This study provides reassurance to clinicians and policymakers as to the safety of pioglitazone as an important agent within the modern management of patients with T2DM. It is the first, large study focused solely on the observation of prostate cancer as a potential outcome and has used data collected in a rigorous, unbiased manner from across a representative sample of general practices in England16 and, as such, should be considered alongside other studies focused on prostate cancer risk in these populations.13 ,38 ,39 This study also provided estimates of the risk of prostate cancer with ever use of other antidiabetic medications—none was observed.
Conclusions
In this observational, real-world, a nested matched case–control linkage study using a large, representative, primary care database and cancer registry from the UK, exposure to pioglitazone was not associated with an increased risk of prostate cancer in patients with T2DM.
Acknowledgments
The authors would like to thank Dr James D Lewis, Dr John D Seeger and Dr Eileen Ming for their thoughtful review and comments on our protocol and statistical analysis plan.
References
Footnotes
Contributors PLT, NB, DB and PD designed the study and provided methodological input. NB, DB and PD participated in the process of application for protocol approval by ISAC. NB, MH and DB contributed to the CPRD GOLD, HES and NCIN data acquisition. MH, NB and PLT processed the data and conducted the statistical analyses. NB wrote the first draft of the manuscript. All authors contributed to discussion, reviewed and interpreted the data, provided critical comments and revised the manuscript.
Funding This study was supported by the Takeda Pharmaceutical Company Limited.
Competing interests All authors have completed the ICMJE form for disclosure of potential conflicts at http://www.icmje.org/coi_disclosure.pdf. PD and DB are employees of Takeda Pharmaceutical Company Limited.
Ethics approval Ethics approval was granted by ISAC. The presented CPRD GOLD, HES and NCIN data are anonymised and, thus, the risk of patient identification is extremely low. The European Network of Centres for Pharmacoepidemiology and Pharmacovigilance (ENCePP) study registration ENCEPP/SDPP/11750.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.