Article Text

Abstract
Objective To compare the risk of lower extremity amputation (LEA) in people with diabetes with and without comorbid depression.
Research design and methods A systematic review of the published literature was conducted. Six databases were searched including PubMed, CINAHL, EMBASE, Medline, the Cochrane Library and PsycARTICLES from inception to 22 June 2016, using a detailed search strategy and cross-checking of reference lists for potentially eligible studies published in English. No date restrictions were employed. All studies were reviewed independently for inclusion by two review authors. Data extraction was performed using a standardized data abstraction form, and study quality was assessed independently by two reviewers. A meta-analysis was performed reporting pooled hazard ratios (HRs) and 95% CIs in Review Manager software.
Results In total, seven studies were eligible for inclusion in the systematic review. Data on 767 997 patients from five studies were included in the meta-analysis. Pooled estimates across the studies were obtained using a random-effects model due to significant heterogeneity (I2=87%). People with diabetes and depression had an increased hazard of LEA (HR 1.76, 95% CI 1.19 to 2.60) compared to people with diabetes and no depression.
Conclusions Based on the available evidence, comorbid depression appears to increase the risk of LEA in people with diabetes. Limited data were available, however, with significant heterogeneity between studies. Further research is needed to inform intervention and clinical practice development in the management of diabetes.
- diabetes
- amputation
- depression
- systematic review
- meta-analysis
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Significance of the study
What is already known about this subject?
People with diabetes are at increased risk of lower extremity amputation (LEA). As the prevalence of diabetes escalates worldwide, it is anticipated that there will be an increase in the number of LEAs. The effect of comorbid depression on the risk of LEA in people with diabetes is unclear.
What are the new findings?
Very limited data are available. Based on the available evidence, however, there appears to be an unfavorable effect of comorbid depression on the risk of LEA in people with diabetes.
How might these results change the focus of research or clinical practice?
Further research on the effect of comorbid depression on the risk of developing the long-term outcome of LEA in people with diabetes is warranted.
Introduction
Depression and diabetes
The presence of diabetes doubles the odds of comorbid depression.1 In the USA, the 2006 Behavioral Risk Factor Surveillance System documented that depression was highly prevalent among people with diabetes and that the prevalence rate varied greatly by demographic characteristics and diabetes types.2 The Diabetes Attitudes, Wishes and Needs study (DAWN2) assessed psychosocial outcomes in people with diabetes across 17 countries and documented that the proportion with likely depression (WHO-5 Well-Being Index score ≤28) was 13.8% (country range 6.5%–24.1%).3
The etiology of the relationship between depression and diabetes is multifactorial.4 Risk factors for the development of depression among people with diabetes include gender, age, years since diagnosis, socioeconomic status, HbA1c control (HbA1c refers to glycated haemoglobin (A1c), which identifies average plasma glucose concentration), number of complications, insulin dose, number of injections, ketoacidosis admission and living alone.5
Depression, diabetes and lower extremity amputations
When diabetes and depression coexist, depression is negatively associated with adherence to diabetes management including self-care of diet, medication, exercise, blood glucose monitoring and medical appointment attendance.6 This increases the risk of complications in people with diabetes.
LEA is one complication of diabetes, is multifactorial7 and negatively impacts on a patient’s quality of life.8 Diabetes is associated with a significantly increased risk of LEA.9 LEA rates vary between populations with estimates ranging from 46 to 9600/105 people with diabetes.10 The International Diabetes Federation (IDF) and the International Working Group on the Diabetic Foot have prioritised reducing LEA rates in people with diabetes.11
Little is documented on the role of comorbid depression on LEA rates in people with diabetes. The relationship between depression and foot complications in people with diabetes is likely to be bi-directional.12 Previous research has suggested that comorbid depression is associated with risk factors for the development of diabetes-related complications. A retrospective cohort study showed a 33% higher risk of major LEA in veterans with diabetes and comorbid depression.13 Also, in a veteran population, a five-point increase in mental health functioning score was associated with a 5% decrease in risk of major LEAs (OR 0.95, 95% CI 0.94 to 0.96) after controlling for independent variables14.
Rationale for the current systematic review and meta-analysis
LEA is a concrete and easily definable outcome that is more common in people with diabetes.10 Significant reductions in the incidence of LEA have been shown with various interventions that target risk factors in people with diabetes.10 15 The role of comorbid depression as a risk factor for LEA in people with diabetes is uncertain. Given that there are a number of successful treatments available for depression, it could be a modifiable risk factor for the development of LEA in people with diabetes. Thus, the aim of this systematic review was to identify all of the published literature to date and to provide an overall quantitative estimate of the relationship using a meta-analysis.
Research design and methods
Primary objective
The primary objective of this systematic review was to synthesize the available published literature to date on the relationship between depression among people with diabetes and the risk of LEA.
The secondary objective was to quantify the findings from each included study and to report an overall pooled estimate of the relationship between depression and risk of LEA in the form of a meta-analysis.
Primary outcome
The outcome of interest in this review was LEA in people with diabetes and depression compared to people with diabetes and no depression. This outcome was used in the meta-analysis to estimate the pooled risk of LEA among people with diabetes and depression.
Exposure
Depression defined by self-report, clinical diagnosis or a combination of both.
Search strategy
The protocol for this systematic review and meta-analysis was registered on PROSPERO, the international prospective register of systematic reviews (unique identification number: CRD42014013897), and is available in full on the National Institute for Health Research website.16 This systematic review and meta-analysis was conducted in accordance with the preferred reporting items for systematic reviews and meta-analyses statement (PRISMA),17 which is a detailed checklist of items specifically designed for this purpose. The following databases were searched from inception until 22 June 2016: PubMed, CINAHL, EMBASE, Medline, the Cochrane Database of Systematic Reviews and PsycARTICLES. The key search terms used included ‘diabetes’, ‘amputation’ and ‘depression’ (online supplementary table 1). MeSH (Medical Subject Heading) terms and truncation as appropriate according to the principles of Boolean logic were used (eg, diabet* was used to include studies referring to diabetes, diabetic, etc). There were no date restrictions applied; however, only published studies in the English language were considered for review. We supplemented our electronic searches by cross-checking the reference lists of all included studies.
Supplementary file 1
Study selection
Titles, abstracts and full texts of potentially eligible studies were assessed by two reviewers (SON and CMB) for inclusion using a priori defined inclusion exclusion criteria (online supplementary table 2). Where the reviewers could not agree on study eligibility, consensus was reached by asking a third reviewer (ZK). Regarding multiple reports from the same dataset, only one report was included in the systematic review and meta-analysis based on the primary outcome of the study, sample size and length of follow-up.
Supplementary file 2
Eligibility criteria for inclusion in the meta-analysis included
Data were from an original study (ie, no review articles, editorials or commentaries).
Randomized and non-randomized studies in which depression was measured at baseline and LEA was an outcome measure after a period of follow-up.
Reporting of an adjusted relative risk (RR), OR, HR or incidence rate ratio on the measured exposure of depression and the outcome of LEA.
Where only crude estimates (ie, potential confounders were not taken into account in the analysis) are presented in a study, these studies will not be included in the meta-analysis, and their results will be presented individually in a separate table.
Data abstraction
Data on eligible studies were summarized systematically by two reviewers (SON, CMB) using a standardised data abstraction form and included author and year of publication, the country the study was conducted in and time period, study design, data source, sample size, diagnosis of the exposure and outcome (table 1). Where data required for the review were missing, the authors were contacted.
Characteristics of studies included in the systematic review
Data synthesis and meta-analysis
Our principal analysis investigated the overall risk of LEA in people with diabetes and depression compared to people with diabetes and no depression. Pooled estimates across studies were obtained by means of a random-effects model where heterogeneity was considered substantial (ie, an I2 value of greater than 50%) based on the Cochrane criteria.18 Studies were weighted according to an estimate of statistical size defined as the inverse of the variance (IV) of the HR.19 Where data were presented in a way that could not be included in a meta-analysis, results of the studies are presented individually in a table. Statistical analysis was performed using the Cochrane Collaboration’s Review Manager V.5.1 software.20
A priori subgroup analyses
The review team decided on the following a priori defined subgroup analyses: by type of diabetes (type 1 vs type 2), by study design, by sample size (<10 000 vs >10 000), by country in which the study was conducted and by study quality (risk of bias minimal, low, moderate or high).
Heterogeneity assessment
The degree of variability between studies attributable to between-study heterogeneity was assessed using the χ2 heterogeneity test and the I2 statistic. In the χ2 test, a p value lower than 0.05 indicates statistical heterogeneity.21 When interpreting the I2 statistic, heterogeneity was measured according to the Cochrane Handbook guidelines with 0%–40% suggesting heterogeneity might not be important, 30%–60% may represent moderate heterogeneity, 50%–90% to be considered substantial heterogeneity and 75%–100% being considerable heterogeneity.21
Quality assessment
Quality assessment of the studies included in the review was conducted independently by two reviewers (SON, CMB) using the six types of bias tool described in detail in a previous study.22 Studies were assessed based on the perceived amount of each bias present (selection, exposure, outcome, confounding, analytical and attrition) and rated as minimal, low, moderate, high or not reported. An overall likelihood of bias was then estimated. The bias assessment tool is available in online supplementary table 3.
Supplementary file 3
Results
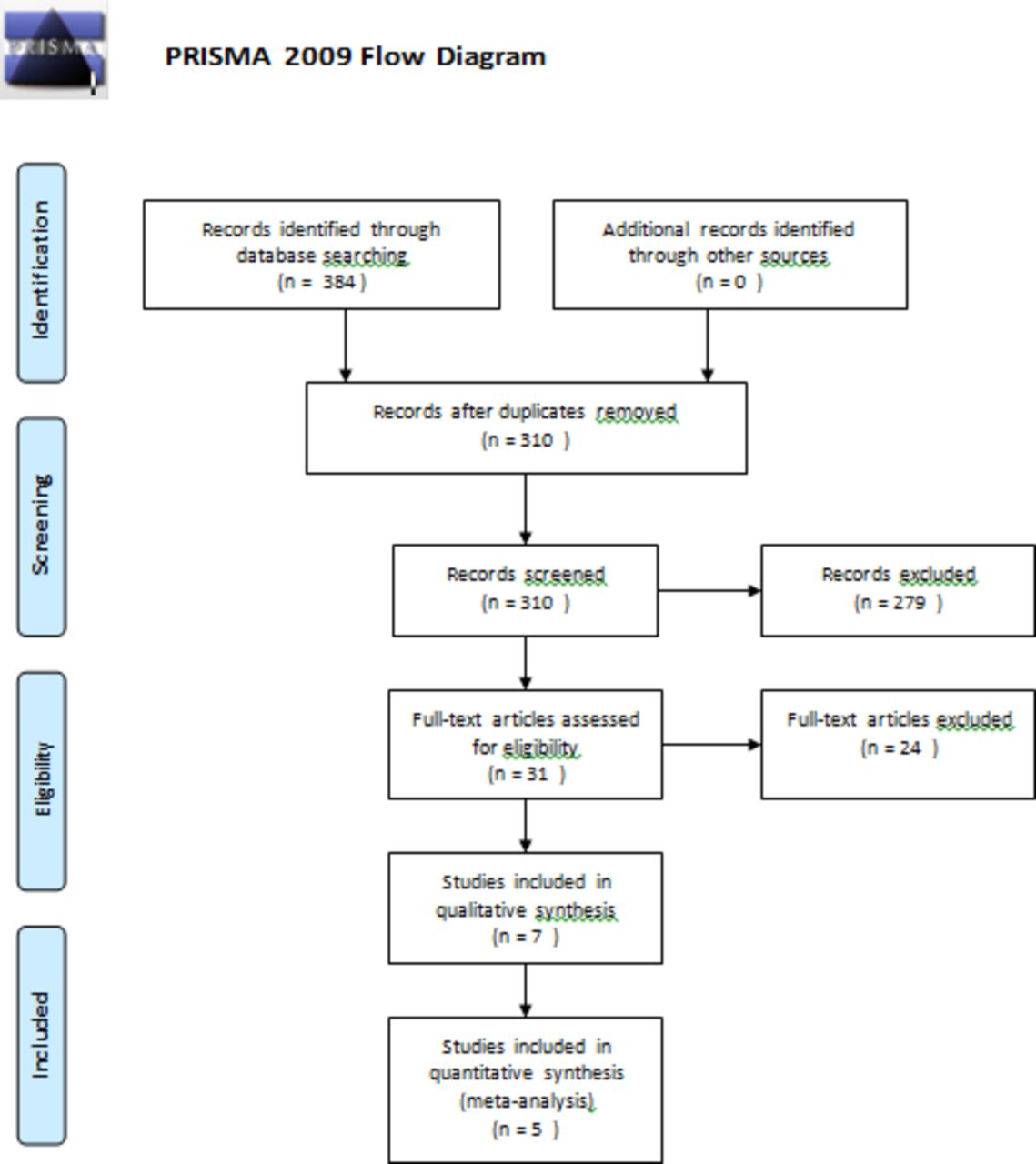
The initial electronic database searches yielded 384 studies with 74 duplicates to result in 310 studies eligible for screening. Of these, 279 were rejected based on reading the abstracts and application of the inclusion criteria. The full texts of 31 studies were retrieved and reviewed for inclusion or exclusion (figure 1). Studies were excluded based on population, exposure, comparison or outcome. Multiple studies from the same dataset were excluded if the dataset was already deemed included in another study. Studies measuring the exposure of depression after LEA or not relating to baseline were excluded. Studies not measuring the impact of depression at baseline and the outcome of LEA after a period of follow-up were excluded (n=24). In total, seven studies met the inclusion criteria for the systematic review,13 23–28 of which five studies provided data for the meta-analysis.13 23 25 27 28

Flow diagram outlining the selection of studies for inclusion in the systematic review. PRISMA, preferred reporting items for systematic reviews and meta-analyses.
Characteristics of studies included in the systematic review
Characteristics of studies included in the systematic review are presented in table 1.
All of the studies were conducted in the 21st century (one in 2003,23 one in 2007,28 one in 2009,24 one in 2010,25 two in 201113 27 and one in 201426). Four were conducted in the USA,13 23–25 one in Australia,26 one in Sweden27 and one in the UK.28 Five of the studies were prospective cohorts13 23 25 27 28 and two had a cross-sectional study design.24 26 The sample size ranged from 60 people26 to 531 973 people.13 One study included people with type 1 diabetes only,24 two studies included people with type 2 diabetes only,23 25 two studies included people with both type 1 and type 2 diabetes,26 28 and two studies did not report the type of diabetes.13 27 The exposure depression was diagnosed using a validated tool or measure in all seven studies. One study23 used the Center for Epidemiologic Studies Depression scale and the Composite International Diagnostic Interview tools, one study24 used the Beck Depression Inventory—version two tool, one study28 used the Schedules for Clinical Assessment in Neuropsychiatry tool, two studies25 26 used the Patient Health Questionnaire—version 9 tool and two studies13 27 used the ICD (International Classification of Diseases) codes. The outcome of LEA was self-reported in two studies,23 24 medical records were examined in two studies,25 26 ICD codes from large database registries were used in two studies13 27 and one study used a trained podiatrist to diagnose the outcome.28
Meta-analysis
Of the seven studies included in the systematic review, five13 23 25 27 28 provided sufficient data to be included in a meta-analysis. Data on 767 997 patients were included in the meta-analysis using the generic inverse variance method and reporting the log (HR) and SE for each study. In the fixed-effect model, an overall pooled estimate HR of 1.21 (95% CI 1.11 to 1.31) was found, implying a 21% increased hazard of LEA in people with diabetes and depression. Due to the evidence of substantial heterogeneity in the fixed-effect model (I2=87%, p≤0.00001), the random-effects model was deemed more appropriate. The pooled HR of risk of LEA due to depression was 1.76 (95% CI 1.19 to 2.60) (figure 2).
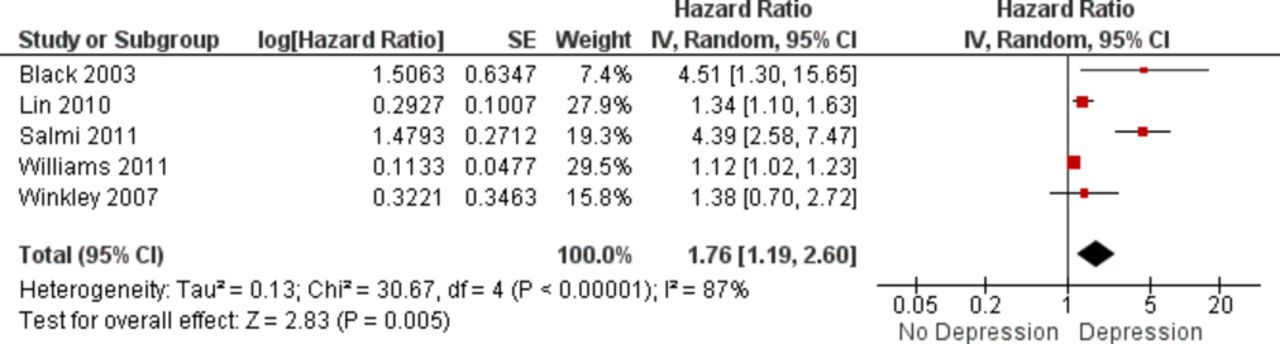
Random-effects model of the risk of lower extremity amputation in people with diabetes associated with depression compared with no depression from five published studies (IV=Inverse Variance).
Significant heterogeneity remained, however (I2=87%, p=0.005).
Subgroup analyses
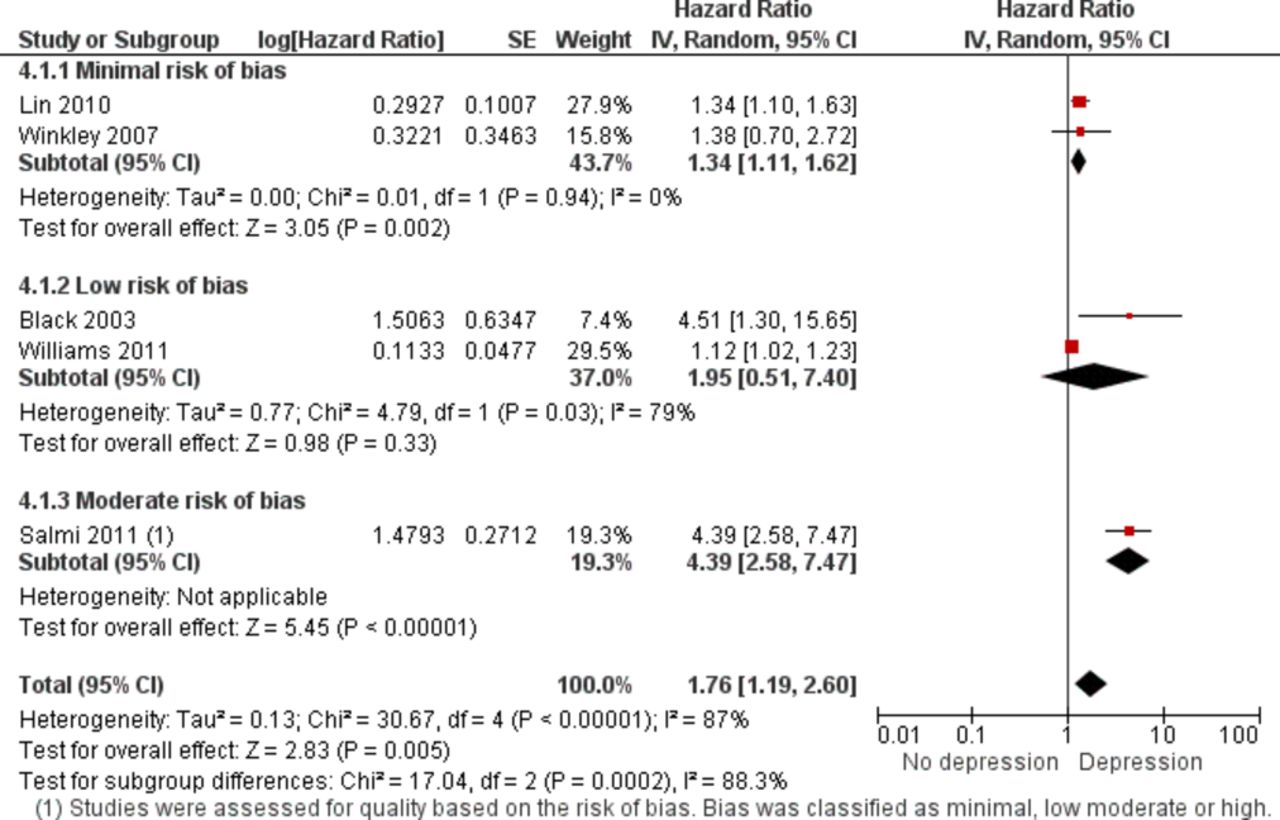
It was not possible to conduct a subgroup analysis based on type of diabetes as these data were not reported in the studies. In addition, we did not conduct a subgroup analysis by study design as all five studies were prospective cohorts. A subgroup analysis by sample size was conducted (figure 3). The overall pooled estimate for studies with a sample size <10 000 was 1.55 (95% CI 0.98 to 2.45, I2=44%, p=0.17) compared with studies with a sample size >10 000 for which the pooled estimate was 2.16 (95% CI 0.57 to 8.23, I2=96%, p≤0.00001). Neither was statistically significant, however. A subgroup analysis according to where the studies were conducted was also performed (figure 4). Studies that were conducted in the USA had a pooled HR of 1.28 (95% CI 0.99 to 1.66, I2=72%, p=0.03) compared with studies conducted in Europe, which had a pooled HR of 2.51 (95% CI 0.81 to 7.80, I2=0.009). A subgroup analysis according to study quality was also conducted (figure 5). Studies with a minimal risk of bias had a pooled HR of 1.34 (95% CI 1.11 to 1.62, I2=0%, p=0.94). Studies with a low risk of bias had a pooled HR of 1.95 (95% CI 0.51 to 7.40, I2=79%, p=0.03). One study had a moderate risk of bias and a HR of 4.39 (95% CI 2.58 to 7.47). We conducted a sensitivity analysis where two studies included the outcome LEA as a combined outcome with other microvascular complications (figure 6). This yielded a pooled HR of 1.86 (95% CI 0.78 to 4.48, I2=92%, p=0.00001).
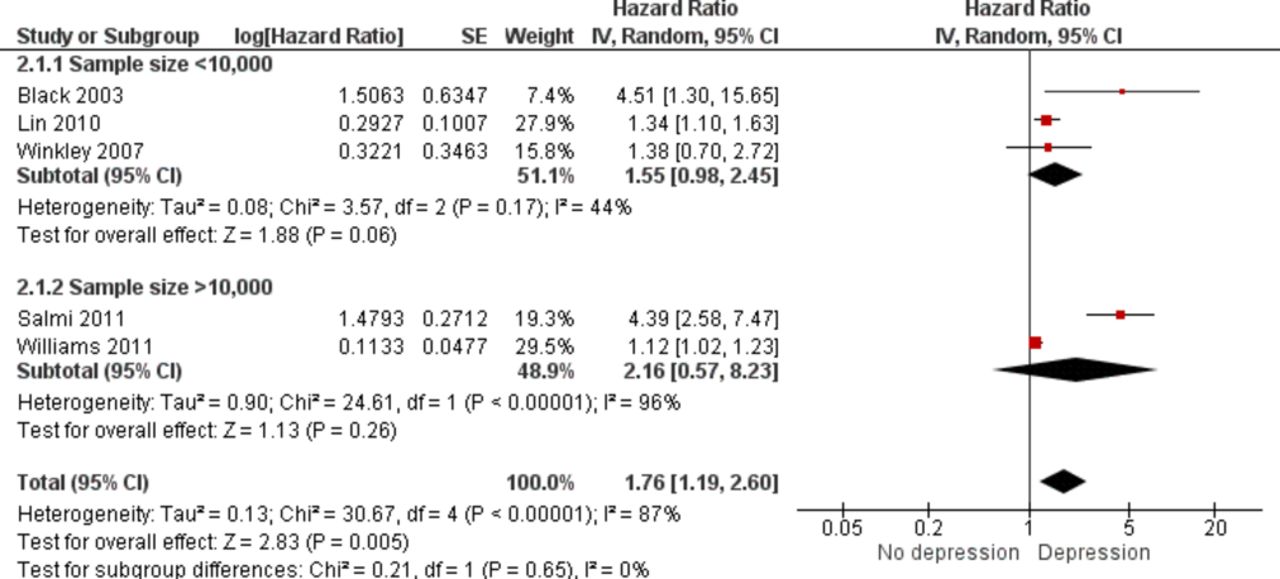
Subgroup analysis: random-effects model of the risk of lower extremity amputation in people with diabetes associated with depression compared with no depression according to sample size (<10 000, >10 000) [IV=Inverse Variance].
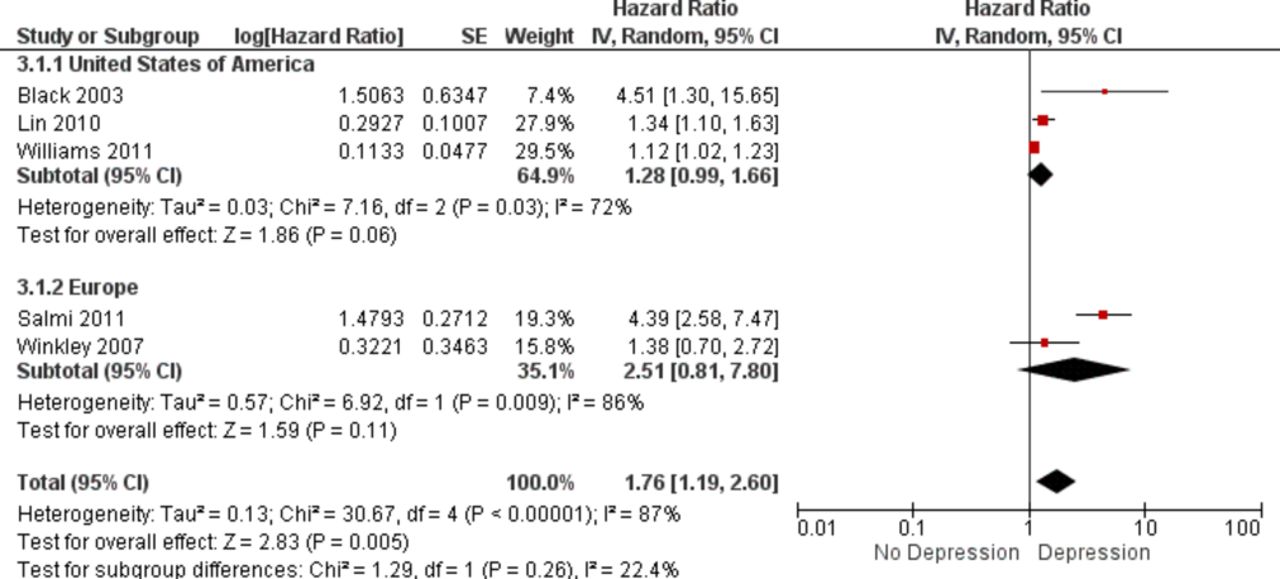
Subgroup analysis: random-effects model of the risk of lower extremity amputation in people with diabetes associated with depression compared with no depression according to region (USA vs Europe) [IV=Inverse Variance].

Subgroup analysis: random-effects model of the risk of lower extremity amputation in people with diabetes associated with depression compared with no depression according to study quality (minimal vs low vs moderate risk of bias) [IV=Inverse Variance].

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Sensitivity analysis: random-effects model of the risk of lower extremity amputation (LEA) in people with diabetes associated with depression compared with no depression where two studies were excluded (LEA was included in these studies as a combined outcome ‘microvascular complications’) (IV=Inverse Variance).
Studies not eligible for inclusion in the meta-analysis
Two studies24 26 were not eligible for inclusion in the meta-analysis as they did not provide adjusted estimates. The main findings and conclusions of these studies are presented in table 2. Both were small studies (one with 458 participants with diabetes, the second with 54 participants with diabetes), which only provided crude estimates.
Results and conclusions of studies not eligible for inclusion in the meta-analysis
Quality assessment
Two studies were assessed as having a minimal risk of bias,25 28 two were deemed to have a low risk of bias13 23 and three had a moderate risk of bias.24 26 27 No study was classified as having a high risk of bias (table 3).
Quality assessment of studies included in the systematic review
Discussion
Overall, in this pooled analysis, people with diabetes and depression had a 76% increased risk of LEA compared with people with diabetes without depression; this result was statistically significant. There was, however, a high level of heterogeneity between studies (I2=87%). To investigate this further, we conducted various subgroup analyses. Sample size did not explain our findings (with large and small studies both showing increased but insignificant findings) or the heterogeneity. Geographical variation in LEA rates has been previously documented.29 30 Potential reasons why results might differ between continents would include different population characteristics and healthcare systems.31 In this review, the region in which the studies were conducted (USA vs Europe) also yielded increased but insignificant results, and heterogeneity remained. The subgroup analysis by study quality showed that the studies with the least bias (minimal bias) produced a 34% increased risk of LEA in people with diabetes and depression, which was statistically significant.
While the outcome of interest was LEA, two of the included studies (Black et al and Lin et al) grouped the outcome of LEA with other microvascular outcomes. It was decided to include these studies due to the dearth of research in this area and to perform a sensitivity analysis removing studies that included LEA as a combined outcome under ‘microvascular complications’. This analysis produced an increased but insignificant result.
It must be acknowledged that only five studies were eligible for inclusion in the meta-analysis, and this limits the robustness of the subgroup analyses performed. Thus, while there is an overall increased risk of LEA in people with depression and diabetes, further research is needed including population-based registry data and more methodologically robust methods of recording depression, diabetes and LEA (ie, ICD codes or medical diagnoses).
Strengths and limitations of this review
This is the first systematic review that the authors are aware of that investigates the association of depression with LEA in people with diabetes. A comprehensive and systematic literature search examined six databases, yielding seven studies eligible for inclusion in the systematic review. Although a significant amount of heterogeneity was found between studies in the meta-analysis, this was examined using appropriate statistical measures as well as a priori defined subgroup analyses. The meta-analysis only included studies that reported adjusted estimates, as these would be considered less biased/confounded results, in order to more accurately represent the true effect of depression and risk of LEA.
The systematic review and meta-analysis is not without limitations, however. Caution needs to be applied when interpreting the results of the studies on depression prevalence as many included poor methodological practices such as small sample size and no confirmation of difference between type 1 and type 2 diabetes, and therefore a subgroup analysis by type of diabetes was not possible. There are fundamental differences between the conditions in relation to mean age of onset and the temporal relationship that could be explored in later systematic reviews as additional studies are conducted. In addition, all of the studies were conducted in high-income, developed countries such as the USA, UK and Australia, the results of which would not be generalisable to resource-poor settings. Differences in diet, lifestyle and culture between these countries may also play a role in diabetes care and thus impact the findings. One study included male war veterans only, and these findings would be very specific to this population. There was also significant variation in the number of potential confounders adjusted that may influence the plausibility of the different study findings.
The diagnosis of depression varied according to study and included different scales, self-reported diagnosis and ICD-9 classifications of depression. Self-reported depression is not a reliable method for obtaining true prevalence of this disorder, particularly among men. This could result in either an overestimate or underestimate of the association with LEA. Variability in the exposure definition may explain the heterogeneity in the meta-analysis
Also, depression status may change over time and measurement at one time point only in these studies is a limitation. As is a problem with most observational studies, unmeasured confounding cannot be ruled out.
Of note, Salmi et al reported on 229 956 patients from a national register-based cohort in Sweden, but only an abstract for this work was available. The abstract does not provide detailed information on the definition of depression and LEA, and efforts to contact the authors for clarity proved futile. We have inferred the diagnoses were made using ICD-9 codes (as this is the method used generally in previous research using the Swedish national data). This is an acknowledged limitation of the review, however.
Heterogeneity
There was a great degree of heterogeneity in the current meta-analysis and would be deemed ‘high’ according to the Cochrane criteria for I2 (>75%).21 The authors tried to control for this heterogeneity by using the random-effects model. Under the random-effects model, we allow that the true effect could vary from study to study. For example, the effect size might be a little higher if the subjects are older, or more educated, or healthier; or if the study used a slightly more intensive or longer variant of the intervention; or if the effect was measured more reliably. In addition, we quantified heterogeneity by using the I2 statistic that focuses attention on the effect of any heterogeneity in the meta-analysis, the percentage of total variation across studies is due to heterogeneity and most importantly in the case of the current meta-analysis, the I2 value does not depend on the number of studies in the meta-analysis.18 Ideally, to further explore reasons for heterogeneity, authors would conduct a priori defined subgroup and sensitivity analyses as well as meta-regression using different covariates. These are largely dependent on the number of studies in the meta-analysis, however, and were not feasible for the current meta-analysis.
Recommendations for future research
Differing definitions and assessment tools for diagnosing depression were used in the studies included in this systematic review. The reported prevalence of depression differs between self-report versus clinical interview diagnosis.32 The use of a standard assessment tool for depression would improve comparability of results from different settings. Further research is required to explore whether the level of severity of depression is predictive of complications. Potential confounders needing consideration in future research include age, gender, education, marital status/living alone, socioeconomic status, type of diabetes, duration of diabetes, insulin use,diabetes treatment/control, self-reported health status, risk behaviours, quality of life, foot care behavior, mood, smoking status, alcohol problems, macrovascular complications, microvascular complications, foot-specific complications, severity of complications, other medical or mental health conditions, and healthcare utilisation.
The literature review confirmed clinical practices vary per individual practitioner, per location and per patient.3 The evidence of under-diagnosing depression in patients with diabetes needs to be considered as a potential bias. Such bias would cause over-reporting of LEAs in patients with no comorbidity and under-reporting of LEAs in patients with comorbid depression.
Conclusions
In conclusion, there appears to be an unfavorable effect of comorbid depression in people with diabetes on the risk of LEA. Given the significant heterogeneity present between studies and the need for studies of a more robust methodological quality, the current findings need to be interpreted with caution. To detect the true effect, future longitudinal studies need to include large sample sizes with a breakdown by type of diabetes, assess confounders at baseline and follow-up and adjust for confounders in the statistical analysis. Further research is needed to explore the role of comorbid depression as a risk factor for LEA, to document the effect size and, thus, to inform intervention and clinical practice development. Considering the availability of various treatments for depression,33 efforts to detect the true effect of comorbid depression on the risk of LEA and indeed other complications in people with diabetes are worthwhile.
Acknowledgments
We would like to acknowledge the staff of the Department of Epidemiology and Public Health, University College Cork, in particular lecturers teaching on the Masters in Public Health.
References
Footnotes
Contributors This work was conducted as part of a Masters in Public Health qualification obtained by GM in 2014 from University College Cork, Ireland. GM, CMB and ZK conceived and designed the study. SON and GM performed the systematic searches. SON and CMB screened the titles for inclusion or exclusion, and performed the data extraction and quality appraisal of the studies. SON performed the meta-analysis and drafted the manuscript. All authors critically revised the manuscript for important intellectual content. CMB will act as guarantor for the paper.
Funding Health Research Board Interdisciplinary Capacity Enhancement Award ICE/2012/12 ‘ Lifestyle Transitions and Trajectories through the Lifecourse: Enhancing capacity in Irish cohort and cross-sectional studies’.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.
Data sharing statement Data from the meta-analysis are available from the corresponding author on request.