Article Text

Abstract
Objective We recently showed that Roux-en-Y gastric bypass (RYGB) reduces risks of mortality, cardiovascular death and myocardial infarction in obese individuals compared with matched patients with diabetes mellitus (DM). We have examined changes in risk factors after RYGB, with the aim of explaining these effects.
Research design and methods We matched (1:1) 6132 RYGB patients with DM reported to the Scandinavian Obesity Surgery Register with patients who had not undergone RYGB, based on sex, age, body mass index (BMI) and time, and assessed effects 2007–2014. We used causal mediation analysis to study effects mediated through changes to BMI and risk factors at 1 year based on Cox proportional hazards models.
Results Baseline BMI was 42 kg/m2. Following RYGB, the lowest BMI was observed after 2 years (mean 31.9 kg/m2), and hemoglobin A1c (HbA1c) after 1 year (mean 6.32% (45.6 mmol/mol)). Maximum high-density lipoprotein (HDL) cholesterol was observed after 3–5 years (mean 1.46 mmol/L). Differences in BMI, HbA1c and HDL between the groups were statistically significant up to 6 years, and 2–3 years for low-density lipoprotein (LDL) and blood pressure, despite fewer glucose-lowering, hypertensive and lipid-lowering treatments. The causal mediation analysis suggested that RYGB has a positive effect on mortality risk, mainly by means of weight reduction (as opposed to changes to the risk factors analyzed).
Conclusions Improvements in risk factors might contribute to the reduction of mortality risk after RYGB in obese individuals with type 2 diabetes, but the main effect seems to be mediated through a decrease in BMI, which could serve as a proxy for several mechanisms.
- diabetes mellitus
- obesity
- bariatric surgery
- mortality
- cardiovascular disease
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Significance of this study
What is already known about this study?
In a registry-based study we have examined changes in risk factors after Roux-en-Y gastric bypass (RYGB),since that procedure has recently been shown to reduce risks of mortality, cardiovascular death and myocardial infarction in obese individuals comparedwith matched patients with diabetes mellitus.
What are the new findings?
Following RYGB, there were beneficial changes in body mass index (BMI), hemoglobin A1c, blood lipids and blood pressure compared with control persons,despite fewer glucose-lowering, hypertensive and lipid-lowering treatments. A causal mediation analysis suggested that RYGB has a positive effect on mortality risk, mainly by means of weight reduction,as opposed to changes to the risk factors analyzed.
Improvements in risk factors might contribute to the reduction of mortality risk after RYGB in obese individuals with type 2 diabetes, but the main effect seems to be mediated through a decrease in BMI, which could serve as a proxy for several mechanisms.
How might these results change the focus of research or clinical pactice?
Which mechanisms, apart from changes intraditional cardiovascular risk factors, explain the lower risk of mortality after bariatric surgery in obese persons? Are there mechanisms that couldexplain the transient effects in blood pressure and LDL cholesterol after RYGB?
Is it possible to investigate predictors of long term beneficial effects after bariatric surgery to individualize such treatment?
Introduction
Bariatric surgery has been regarded as the most effective method of treating obesity due to its long-term beneficial effects on weight, as well as on cardiovascular (CV) risk factors, CV outcomes and mortality.1–3 Similar effects have also been demonstrated in individuals with diabetes mellitus, along with improved glycemic control, less use of glucose-lowering medications, and remission of diabetes.4–8
A few studies, however, have had sufficient statistical power to assess mortality following bariatric surgery, particularly in patients with diabetes. Swedish Obese Subjects, an American retrospective cohort study, and a systematic review have found reduced mortality risk after various bariatric surgical procedures, although they included only a limited or unknown number of patients with diabetes.2 9 10
We recently performed a nationwide retrospective longitudinal observational study that matched 6132 obese individuals with diabetes who had undergone Roux-en-Y gastric bypass (RYGB) with the same number of individuals who had not undergone bariatric surgery.11 After a median follow-up period of 3.5 years, there was a 58% relative risk reduction in overall mortality, a 59% lower risk of CV death and a 49% lower risk of myocardial infarction in the RYGB group. The beneficial effects were observed mainly in those who achieved pronounced weight reduction, as well as those who were in remission of diabetes.11
The present report is a continuation of the recent study among 12 264 individuals with diabetes mellitus and obesity in which we merged data from five national quality registers and databases in Sweden.11 Our aims were to describe detailed changes in weight, glycemic control, CV risk factors and use of medication, as well as to evaluate the impact of such changes on the risks of CV disease and death up to 8 years after RYGB or in matched individuals, using a causal mediation analysis.
Research design and methods
Our methods have largely been presented in recent reports.11 To summarize, this is an observational study approved by the regional ethical review boards in Gothenburg and Örebro, based on merging data from national quality registers and official databases with nationwide coverage in Sweden: the National Diabetes Register (NDR),12 the Scandinavian Obesity Surgery Register (SOReg),13 Statistics Sweden, the Inpatient Register and the Cause of Death Register, all of which have been previously described and validated.14
We used the SOReg to identify individuals with diabetes and obesity who had undergone RYGB between 1 January 2007 and 31 December 2014, and matched them with patients from the NDR. Participants were monitored for up to 6.99 years with respect to weight, glycemic control, CV risk factors, pharmacologic treatments, CV events and death. We defined remission of diabetes as hemoglobin A1c (HbA1c) levels of less than 6.5% (48 mmol/mol), smokers as current users of tobacco, and physical activity as equivalent to walking 30 min at least 3 days a week.
Missing data are usually present in registries and unless we are willing to assume missing completely at random some form of imputation is very difficult to avoid. Here we combine data from two sources: the NDR which is a registry for a chronic disease contains repeated (yearly) registrations, and SOReg, which is a registry for a specific intervention, from which we for this study only use the preintervention entry. Missing baseline data for SOReg patients were thus imputed by means of a single imputation from a multivariate normal model based on a Monte Carlo Markov chain approach, while missing data for potential control patients in NDR were imputed prior to matching by means of last value carried forward, due to high within-patient correlations for many variables in the NDR. The proportion of missing data in SOReg ranges from 0% (age, gender and body mass index (BMI)) to 38% (systolic and diastolic blood pressure (SBP, DBP)), and in NDR between 0% (age and gender) and 42% (high-density lipoprotein (HDL) and low-density lipoprotein (LDL) cholesterol). Only successfully imputed NDR records were entered in the matching process.
Controls (not surgically treated) were matched 1:1 without replacement with RYGB patients based on sex, BMI (five intervals), age (four intervals) and time in four categories (2007–2008, 2009–2010, 2011–2012, 2013–2014), each from the NDR population as yet untreated. A selected control that was subsequently treated with RYGB was censored on the date of treatment. The index date for a matched control was set to a random entry in the NDR for the 2-year period during which the corresponding case received the treatment.
Patient characteristics at baseline were evaluated using standardized difference (not presented in this report), as well as t-tests for continuous variables and χ2 test for discrete variables. Observations of BMI, HbA1c, LDL, HDL, SBP and DBP were evaluated as functions of time from index by means of a linear mixed repeated measure model, while observations of smoking status, use of antihypertensive and lipid-lowering medications were evaluated by means of generalized mixed repeated measures models (in the previous report we only used ordinary arithmetic means and percentages to describe baseline characteristics).11 Both types of models used a covariance matrix with compound symmetry. To allow convenient estimation of yearly mean values, we attributed measurements performed between 6 and 18 months to 1 year, between 18 and 36 months to 2 years, etc.
Causal mediation analysis, which has been formulated and implemented within the framework of linear structural equation modeling, attempts to identify intermediate variables (or mediators) that lie in the causal pathway between the treatment and the outcome. In our study, the treatment is the RYGB procedure, and the outcomes are serially overall mortality, cardiovascular death and myocardial infarction. The mediators that we examined were changes in BMI, HbA1c, SBP, HDL and LDL. The direct effect is the effect of the treatment without the corresponding effect of the mediator, that is, the direct effect of RYGB to the overall mortality is the procedure as such, without the mediated effect on change in BMI.
The direct and indirect effects were estimated using weighted Cox regression models where the weights were derived from separate multinomial logistic regression models, including either the actual or the counterfactual exposure, in addition to variables that might confound the relation between exposure and the mediator. Both the multinomial regression models and the weighted Cox regression were adjusted for previous myocardial infarction (MI), chronic heart failure (CHF) or stroke, HbA1c, SBP, DBP, smoking status, use of drugs lowering blood pressure and lipids, treatment for diabetes, income, education and marital status. The estimation process included template SAS version 9.4 and R code was described in detail by Lange et al.15
Results
Baseline and follow-up data after 1 year have been reported recently.11 Table 1 shows complete data for up to 6.0 years (mean 3.7 years, median 3.7 years in RYBG; mean 3.3 years, median 3.1 in controls) for the 6132 RYGB subjects and 6132 matched controls. At baseline, the two groups were well matched with respect to sex, duration of diabetes, glycemic control-HbA1c and LDL (standardized differences less than 0.1), although there were minor and statistically significant numerical differences (t-tests) in HbA1c and LDL, as well as other risk factors and treatments (table 1).
BMI, HbA1c, cardiovascular risk factors and pharmacologic treatments after RYGB or in control objects (means and proportions)
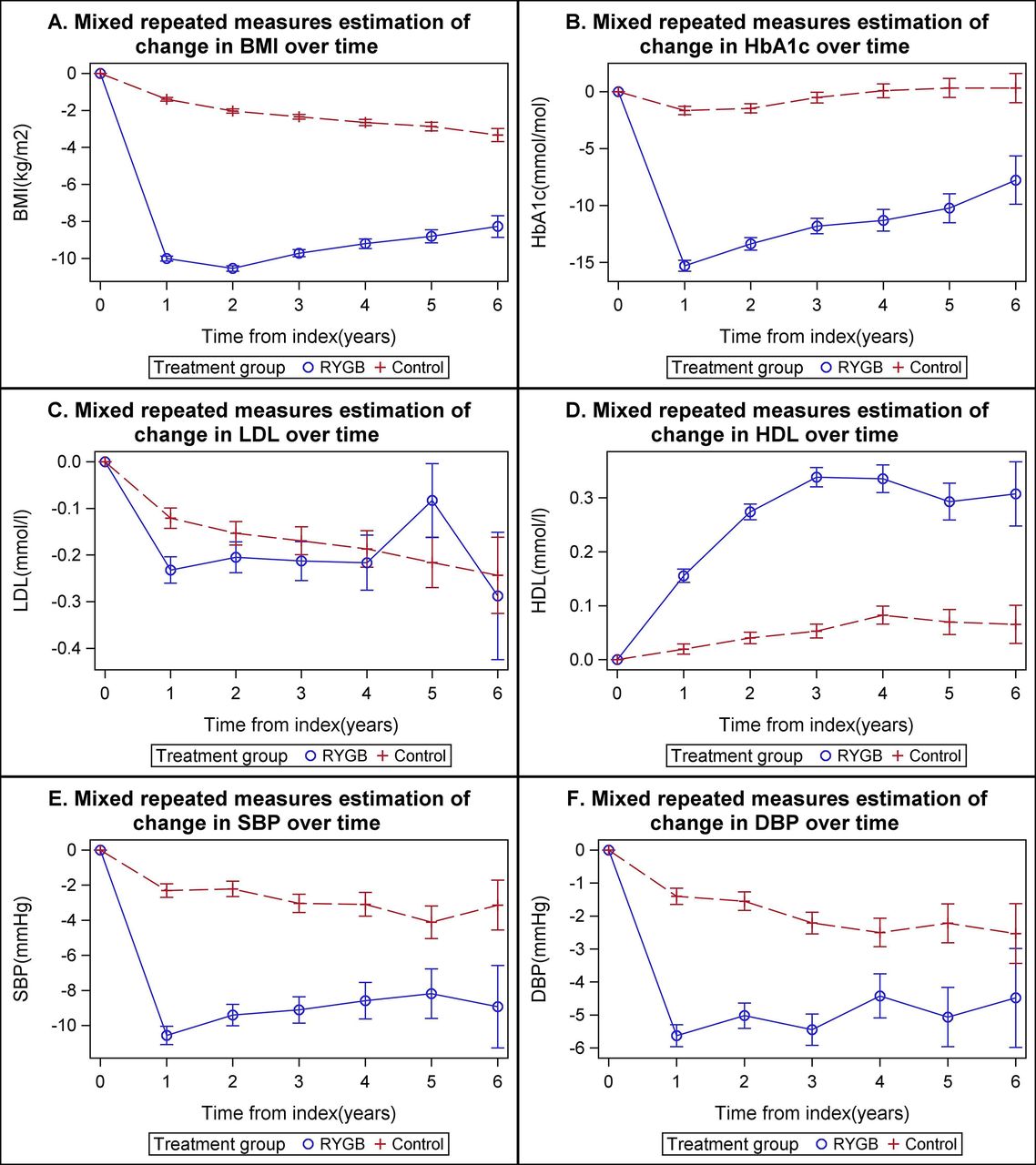
Changes from baseline in BMI, HbA1c, LDL, HDL, SBP and DBP for up to 6 years are also shown in figure 1A–F. The lowest value in BMI (31.9 kg/m2, 95% CI 31.7 to 32.1) was observed after 2 years in the RYGB group (figure 1A), although the difference in BMI remained statistically significant for 6 years. The minimum value in HbA1c (6.32%, 95% CI 6.27 to 6.38 (45.6 mmol/mol, 95% CI 45.0 to 46.3)) was observed after 1 year (figure 1B) but remained statistically significantly lower in RYGB subjects than controls during the entire follow-up period. Remission of diabetes after 1 year occurred in 36.8% of the RYGB patients and 9.3% of controls. Use of glucose-lowering medications was clearly lower throughout the follow-up period.
{kind=link}
(A–F) Changes to BMI, HbA1c, LDL, HDL, SBP and DBP during 6 years of follow-up after RYGB and in controls (mixed repeated measures). BMI, body mass index; DBP, diastolic blood pressure; HbA1c, hemoglobin A1c; HDL, high-density lipoprotein; LDL, low-density lipoprotein; SBP, systolic blood pressure.
LDL was also slightly but significantly lower during the first 3 years (figure 1C), while HDL slowly increased in the RYGB group, peaking and plateauing after 3 years (mean 1.46 mmol/L, 95% CI 1.43 to 1.48), with a statistically significant difference between the groups for 6 years. The differential effects on LDL and HDL were observed despite a clearly higher use of lipid-lowering agents in the control group throughout the follow-up period.
SBP levels were slightly but significantly lower in the RYGB group than the control group for 4 years. DBP levels were lower for 3 years, although the control group used antihypertensive medications more frequently during 6 years of follow-up. Smoking was more common among the controls during the first 3 years, whereas physical activity was significantly higher in the RYGB group.
Table 2 shows the results of the casual mediation analysis, that is, an evaluation of the significance of the surgical procedure per se, or the changes to BMI and selected risk factors with respect to CV and all-cause mortality as recently demonstrated.11 The effect of RYGB was shown to be mediated indirectly through BMI for all-cause mortality (HR 0.384, 95% CI 0.179 to 0.821) and CV death (HR 0.145, 95% CI 0.028 to 0.750), thus suggesting a strong beneficial effect of weight reduction regardless of other covariates included in the statistical model. There was no evidence that any effect on myocardial infarction is mediated through BMI. The direct effect of the RYGB procedure (thus not mediated through a reduction in BMI) was shown to be an increased risk of all-cause death by 96% (HR 1.956, 95% CI 1.002 to 3.821) but a reduced risk of myocardial infarction (HR 0.317, 95% CI 0.133 to 0.756). Furthermore, we found no evidence of any effect mediated through changes to HbA1c, SBP, HDL or LDL (table 2), although the effects of RYGB could not always be broken down into direct and indirect paths. Our overall conclusion from these results is that the effect of RYGB on all-cause and CV mortality is mediated mainly through changes in BMI rather than HbA1c, SBP, HDL or LDL, while the effect on myocardial infarction cannot be attributed to either BMI or HbA1c, SBP, HDL or LDL.
Causal mediation for patients treated with gastric bypass
Conclusions
This study demonstrates clear improvements in BMI, HbA1c and HDL during the entire follow-up period among obese individuals with diabetes after RYGB, compared with controls who have not undergone surgical obesity treatment. There were also minor transient beneficial effects on LDL and blood pressure levels during the first few years after RYGB. These results were observed despite reduced use of glucose-lowering, lipid-lowering and antihypertensive agents. The causal mediation analysis suggests that RYGB has a positive effect on mortality risk mainly through weight reduction (indirect effect) rather than changes in HbA1c, blood lipids or blood pressure. The procedure of the surgical intervention (direct effect) appears to be associated with an increased risk of all-cause and CV mortality regardless of changes to BMI, as well as with a lower risk of myocardial infarction regardless of changes to BMI, HbA1c, SBP, HDL or LDL. Some fatalities might thus be caused by other effects, such as surgical complications or trauma, as opposed to myocardial infarction which is always caused by atherosclerosis.
The course of the changes to BMI and HbA1c was similar to the observations of recent clinical trials,5 8 as were BMI levels achieved (approximately 32 kg/m2).8 16 Mean HbA1c levels at baseline in the present study were not as high as in recent randomized clinical trials among patients with diabetes5 8 but were perfect during the follow-up period. This finding translates into lower rates of microvascular diabetes complications, as recently proposed by an uncontrolled retrospective study.17 There is certainly a strong association between glycemic control and mortality in patients with both type 1 and type 2 diabetes,18 19 but it seems unlikely—and is unsupported by our results—that the difference in HbA1c between the two groups in the present study would explain why the mortality risk is lower following RYGB than conventional diabetes treatment.
Remission of diabetes after bariatric surgery has been repeatedly demonstrated5 8 16 20 and is an undisputed objective of this treatment. In the present study, the proportion of patients in remission of diabetes (36.8%) according to our definition was comparable to the findings of the Surgical Treatment and Medications Potentially Eradicate Diabetes Efficiently (STAMPEDE) trial,5 as well a recent Italian single-center study.8 Although sleeve gastrectomy is increasingly used, RYGB is still the most common surgical procedure in Sweden, particularly during the time frame of this study. Thus, our results only apply to the latter, although many of the effects may be present using any surgical method.
Obesity is characterized by atherogenic dyslipidemia, including increased triglyceride levels, decreased HDL and abnormal LDL composition, all of which are known to improve with weight loss and physical exercise.21 The key metabolic mechanisms are hepatic overproduction of large triglyceride-rich very low density lipoproteins and delayed clearance of triglyceride-rich lipoproteins.22 Our study confirms previously established effects on blood lipids after RYGB.8 There was a limited decrease in LDL serum levels from quite normal values, generating a temporary statistical difference between the two groups. These results can be influenced by the use of lipid-lowering medications (almost always statins), which increased in both groups, although controls used them more frequently throughout the study period. The limited effect on LDL and the pronounced and persistent increase in HDL are in line with the results of studies that have addressed CV risk factors after lifestyle changes that include physical exercise and even moderate weight loss.23 24 It is unlikely, however, that these differences in LDL and HDL levels, or lipid-lowering treatment, can explain the discrepancies in mortality risk identified by our study, particularly because there is still no evidence that treatment of HDL reduces CV risk.
Although beneficial changes in all risk factors but HbA1c were seen in the control persons, there were minor but statistically significant differences in blood pressure levels and use of antihypertensive medications, as well as smoking habits and amount of physical activity, between the groups during follow-up. The impact of smoking cessation on risks of CV disease and mortality has long been established,25 while the hypothesis that lifestyle interventions in patients with type 2 diabetes might improve survival rates remains to be proven in a randomized trial.26 The benefits of physical activity have, however, been very clearly documented in a major meta-analysis.27 Nevertheless, there might be a number of other factors, such as additional lifestyle factors or comorbidities, that contribute to the effects of RYGB compared with the treatment offered during the course of this study that we cannot capture in the registers and databases used (residual confounding). The reasons for the lower risk of dying following RYGB may thus be multifactorial so that weight change—as supported by our results—may be a proxy for several different mechanisms, such as reduced mechanical loading, inflammatory stress, as well as neurohormonal alterations, nutrition changes and perhaps also increased physical activity.
The key limitation of our study is that the number of individuals available for follow-up gradually decreased with only 25% of clinical data available after the first year in the RYGB group, and 45% in the control group. It is likely that some persons have not been reported at normal intervals due to clinically significant improvement or even remission of diabetes. NDR is a quality registry to which one can report patients with diabetes annually or at intervals to suit their own practice. In the previous report, we mainly used data on cardiovascular outcomes and death from the Swedish Inpatient and Cause of Death Registers, thus allowing follow-up of substantially higher proportion of the study population. However, we are confident that the high quality of data is substantiated by relatively stable mean values and narrow CIs for at least 6 years. We used state-of-the-art methodology to impute missing baseline data, and missing values during the follow-up time were handled by using the mixed repeated measures model, but can only describe the role of changes in risk factors in persons available for follow-up. Due to the data sources used and the selection of patients in the two treatment groups, there were minor differences in clinical characteristics. As previously discussed,11 we used careful matching of people based on sex, age, BMI and time, followed by a Cox proportional hazards regression model, including all baseline characteristics, to minimize the effects of confounding. Residual confounding, by for example, lifestyle variables or comorbidities, however is possible contributing to the effects of the study. The causal mediation analysis is a new method not widely used yet, but we employed it in an attempt to evaluate the significance of changes to traditional risk factors following bariatric surgery for the main results of our study—the lower risk of all-cause and CV mortality.11 15 The main strength of the study is its nationwide scope—the use of registers with 95% participation of all patients with obesity and diabetes who underwent RYGB during the period covered.
There were pronounced beneficial effects, mainly with respect to BMI, HbA1c and HDL, while changes in LDL and blood pressure were minor and transient following RYGB among patients with diabetes and obesity compared with those who had not undergone surgery—despite less frequent use of pharmaceutical treatment for risk factors. The11 lower risk of all-cause and CV death that has been shown recently seems to be mediated primarily by the decrease in BMI, as opposed to CV risk factors. This suggests that several different mechanisms contribute to the beneficial effects.
References
Footnotes
Contributors All authors contributed to the conception and design of the study. SF, AMS, JO and IN contributed to the acquisition of data and SF performed the statistical analyses. All authors contributed to the interpretation of data. VL and BE drafted the article, and all authors contributed to the critical revision of the article. BE is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Funding The Swedish Association of Local Authorities and Regions funds the National Diabetes Register (NDR) and the Scandinavian Obesity Surgery Register. Region Västra Götaland also provides funding for the NDR.
Patient consent All patients are informed of the reporting to national quality registries and are given the opportunity to be excluded. No formal written consent is required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data may be available on request to the corresponding author or to BE.