Article Text

Abstract
Background Poor medication adherence can have negative consequences for the patients, the provider, the physician, and the sustainability of the healthcare system. To our knowledge, the association between medication adherence and glycemic control among newly diagnosed diabetes patients has not been studied. This study aims to bridge the gap.
Method This is a retrospective cohort study of 2463 patients managed in the National Healthcare Group in Singapore with newly diagnosed diabetes. Patients were followed up for the first two years from their first medication dispensed for measuring medication adherence, proportion of days covered (PDC); and for another three years for investigating outcomes of glycemic control, emergency department visit, and hospitalization. Multivariable regressions were performed to study the association between medication adherence and the outcomes as well as the risk factors of poor adherence.
Results The prevalence of medication adherence (PDC≥80%) was 65.0% (95% CI 63.1% to 66.9%) among newly diagnosed diabetes patients in Singapore. Male, Indian, or patients without hypertension or dyslipidemia were associated with poorer medication adherence. The HbA1c level of poor adherent patients (PDC <40%) increased by 0.4 (95% CI 0.2 to 0.5) over the two years, and they were also more likely to have hospitalization (OR 2.6,95% CI 1.7 to 3.8) or emergency department visit (OR 2.4,95% CI 1.7 to 3.4) compared with the fully adherent patients (PDC=100%).
Conclusions The medication adherence in the early stage of diabetes is important for maximizing the effectiveness of pharmaceutical therapy. Health policies or interventions targeting the improvement of medication adherence among newly diagnosed diabetes patients are in need.
- adherence to medications
- adult diabetes
- hospitalization
- glycemic control
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Some studies have showed that greater medication adherence was associated with improved glycemic control, less hospitalization. However, there was no evidence for newly diagnosed diabetes patients.
What are the new findings?
This study shows that greater medication adherence is also associated with improved glycemic control, less hospitalization for newly diagnosed diabetes patients.
How might these results change the focus of research or clinical practice?
This study demonstrates that medication adherence in the early stage of diabetes is important in maximizing the effectiveness of pharmaceutical therapy and preventing healthcare use among diabetes patients. Health policies should emphasize the importance of early medication treatment and adherence among newly diagnosed diabetes patients.
Introduction
Adherence to pharmacotherapy is a critical aspect of medical treatment, particularly the treatment of chronic conditions such as diabetes. Despite the importance of adherence, medication non-adherence is a serious problem, with WHO noting that the average non-adherence rate is 50% among those with chronic illnesses.1 Poor medication adherence can have negative consequences for the patients, the provider, the physician, and the sustainability of the healthcare system.2 In the USA, estimated direct and indirect costs of non-adherence were as high as $337 billion in 2013, which is approximately one-ninth of total healthcare spending in the same year.3
Diabetes is at epidemic levels, with the costs of treatment placing a significant economic burden on healthcare systems worldwide. Good long-term glycemic control is essential for preventing diabetes patients from developing microvascular and macrovascular complications, which result in substantial medical resource uses and medical care costs.4–6 There is evidence showing that poor glycemic control leads to higher health resource use and medical care costs.7 8 Oral hypoglycemic and insulin injection are recommended for glycemic control. However, medication non-adherence is common and the benefit of the pharmaceutical therapy is discounted. A literature review indicated that of nine studies using objective measure of adherence such as medication possession ratio (MPR), seven found greater adherence was associated with improved glycemic control9–16; of eight studies that evaluated hospitalization, seven showed higher adherences were associated with fewer hospitalizations9 14 17–22; and of three studies that evaluated emergency department (ED) visits, two found higher adherences were associated with fewer visits.9 17 19
In view of the chronic and progressive nature of diabetes, early medication intervention has the potential to optimize the glycemic control. Hong and Kang found that among newly diagnosed type 2 diabetes patients non-adherence of oral medication for the first two years increased the risk of hospitalization in the third year by 26%.23 The association between medication non-adherence and glycemic control among newly diagnosed diabetes patients has not been studied. As far as we know, there was no study on assessing the prevalence and the negative consequences of medication non-adherence among diabetes patients in Singapore. This study aimed to fill the gap. The evidences generated suggest diabetes patients to play a greater role in the management of their illnesses by adhering to their medication regimens. And the evidences could be used by clinicians to educate their patients on the importance of medication adherence on the early stage of diabetes.
There are two objectives of this study: the first is to study the prevalence of the medication adherence in Singapore; the second is to examine the association between initial medication adherence and glycemic control as well as healthcare use among newly diagnosed diabetes patients.
Method
Study design and data
This is a retrospective cohort study using multicenter data. Patients newly diagnosed with diabetes mellitus and with random or fasting glucose being normal in previous year in the National Healthcare Group (NHG) from 2005 to 2010 were included in the study. This is to ensure patients were newly incident diabetes patients. Patients not on medication treatment for diabetes or died in the first two years were excluded from the study because their medication adherence could not be measured in our study design. Patients who developed diabetic-related complications were also excluded because it is likely that they had had diabetes for a long time though newly diagnosed. And we would like to focus on the early stage of diabetes in this study. The study was approved by the NHG's ethics reviewing board. NHG is one of six regional healthcare systems in Singapore and serves a population of about 1.1 million.
Study patients’ data were extracted from the chronic disease management system (CDMS), a disease registry developed in the NHG. The CDMS database stores data of demographics, healthcare use, clinical diagnosis, lab test, medication and payment for all diagnosed diabetes patients.24
Patients were followed up for the first two years from their first medication prescribed for measuring medication adherence; and for another three years for investigating outcomes of glycemic control, ED visit, and hospitalization. Separately measuring adherence and outcomes in two different periods of time was to avoid the possibility that adherence was affected by outcomes.
Measure of medication adherence
All medication prescriptions with the Anatomical Therapeutic Chemical code A10, which is the group of drugs used for lowering blood glucose and insulins, were reviewed in the study, which included alpha-glucosidase inhibitors, biguanides, dipeptidyl peptidase 4 inhibitors, meglitinides, sulfonylureas, thiazolidinedione, and insulin. Proportion of days covered (PDC) was calculated for each study subject as a measure of medication adherence.20 Whether patients for each day had any medication in the group A10 at hand was examined. The denominator is 730 days (2 years). To calculate the numerator, a time vector which reflected the days that were encompassed by each fill was created for each patient.25 If the patient had early refill of the same medication, the start date of the refill was adjusted. The number of days that each fill covered was recorded in the pharmacy data; thus, changing doses was accounted for. If multiple medications were taken concurrently, PDC reflected at least one medication was taken in those days.26 Calculating PDC in this way can avoid inflating adherence by simply summing up medication supplies.
Outcome variable
The primary outcome of this study is glycemic control, and the secondary outcomes are hospitalization and ED visit. Glycemic control was measured by the change of HbA1C, which is defined as the average HbA1c in the three years of outcome period subtracted by the HbA1c tested at or before the first medication dispense (or baseline Hba1c), as medication adherence could be affected by the HbA1c level at the time when medication was prescribed.
ED visit and hospitalization was recorded as dichotomous variable: whether a patient had ED visit due to any cause in the three-year outcome period, and similarly whether a patient had any hospital admission due to any cause in the same period.
Covariates
The covariates included in the study were patients’ demographics of age, gender, ethnic group (Chinese, Malay, Indian, and others), marital status (married, single, or unknown), comorbidity conditions of hypertension and dyslipidemia, as well as baseline Hba1c level. Age2 was included to adjust for the possible non-linear association between age and medication adherence or the outcomes. Square of HbA1c level was also included for the similar reason. Hypertension and dyslipidemia were included in the form of years from the diagnosed date to the start of the outcome period for the nature that years in disease may greatly affect patients’ outcomes. There were very few patients having other comorbidities than hypertension and dyslipidemia in the sample.
Statistical analysis
Medication adherence was grouped into six categories (PDC <20%, 20%≤PDC<40%, 40%≤PDC<60%, 60%≤PDC<80%, 80%≤PDC<100%, and 100%). Following the convention, we also defined a dichotomous variable that <80% PDC (PDC <80%) was medication non-adherence and ≥80% (PDC≥80%) was adherence.
The association between patient characteristics and medication adherence was identified by ordinal regression. The adjusted association between medication adherence and glycemic control was examined by linear regression with change in average HbA1c level as the dependent variable. The association between medication adherence and ED visit or hospitalization was investigated by logistic regression.
Results
Of the 2463 study patients, 65% (95% CI 63% to 67%) were in the adherence group (PDC≥80%) and 35.0% (95% CI 33.1% to 36.9%) were in the non-adherence group (PDC <80%). In total, 445 patients had PDC=100%. The average age of all study patients was 57.1 (SD 10.3) years. There were fewer male than female (40% vs 60%; p value=0.00) study patients. The detailed profiles of all six adherence groups (PDC <20%; 20%≤PDC<40%; 40%≤PDC<60%; 60%≤PDC<80%; 80%≤PDC<100%; PDC=100%) are shown in table 1. Age or marital status had no significant association with medication adherence. Male, Indian, or patients with less years of hypertension or dyslipidemia were more likely to be poorly medication adherent. The relationship between baseline HbA1c and medication adherence was an inverted U-shaped curve (table 1).
Medication adherence (PDC) and patient characteristics at baseline
After adjusting for other covariates by ordinal logistic regression, patients with longer years of hypertension or dyslipidemia were associated with better medication adherence. Both HbA1c level and its square were significant, which indicated an inverted U-shaped relationship between baseline Hba1c and medication adherence. The relationship between age and medication adherence was an inverted U-shaped too. There were ethnic differences in medication adherence. Indian was associated with poorer adherence compared with other ethnic groups in Singapore (table 2).
Association between patient characteristics and medication adherence by ordinal logistic regression*
Association between medication adherence and glycemic control
The average HbA1c levels at both baseline and during outcome period for the six adherence groups are plotted in figure 1. One may expect better medication adherence among patients with a higher HbA1c; however, we did not see this relationship in the study. The graph shows a bell shape with the peak HbA1c at the 40%–60% adherence group for the baseline. The 20%–40% adherence group had the highest HbA1c level during the outcome period.
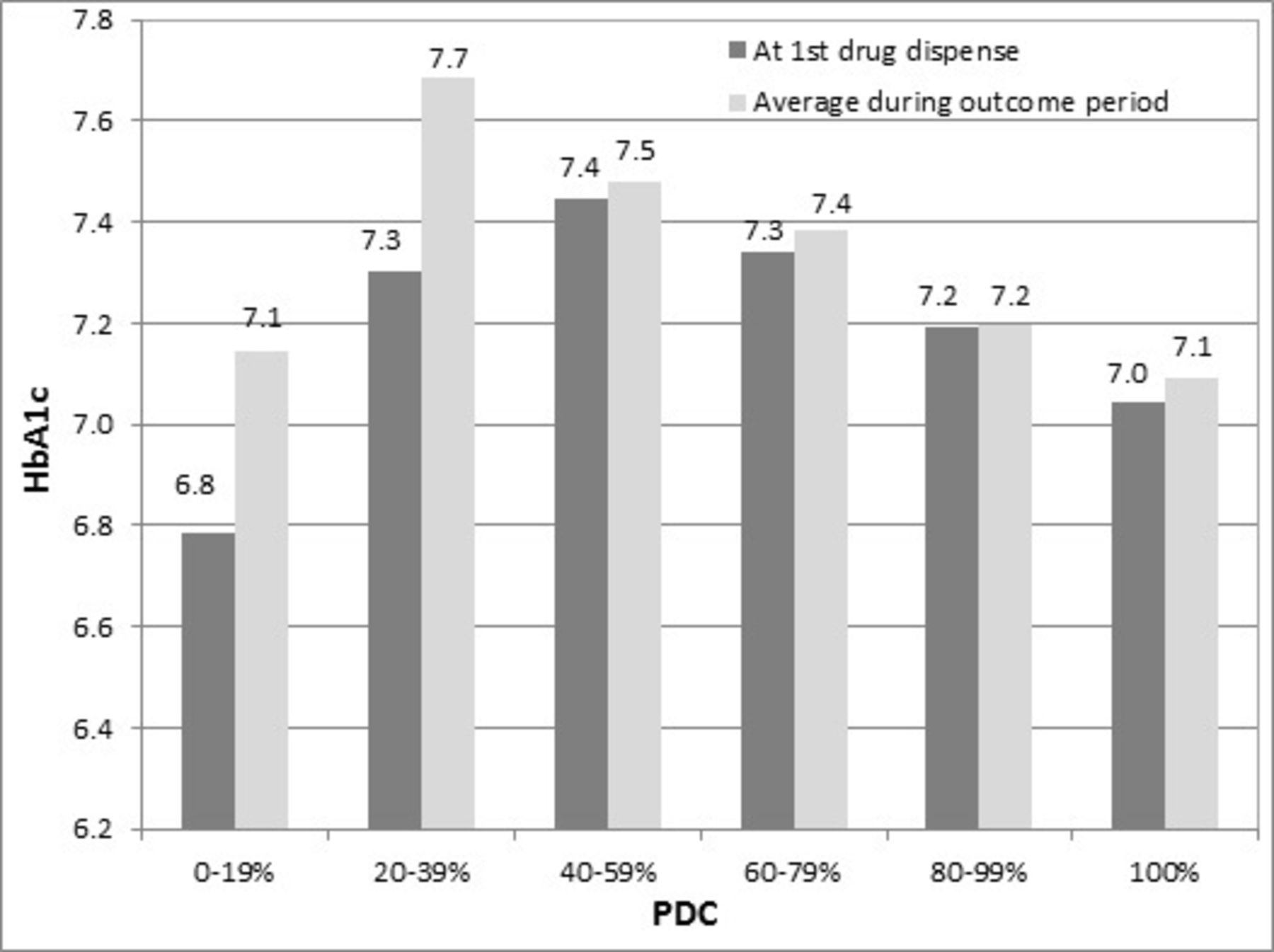
Average Hab1c levels: at first drug dispense versus during outcome period. PDC, proportion of days covered.
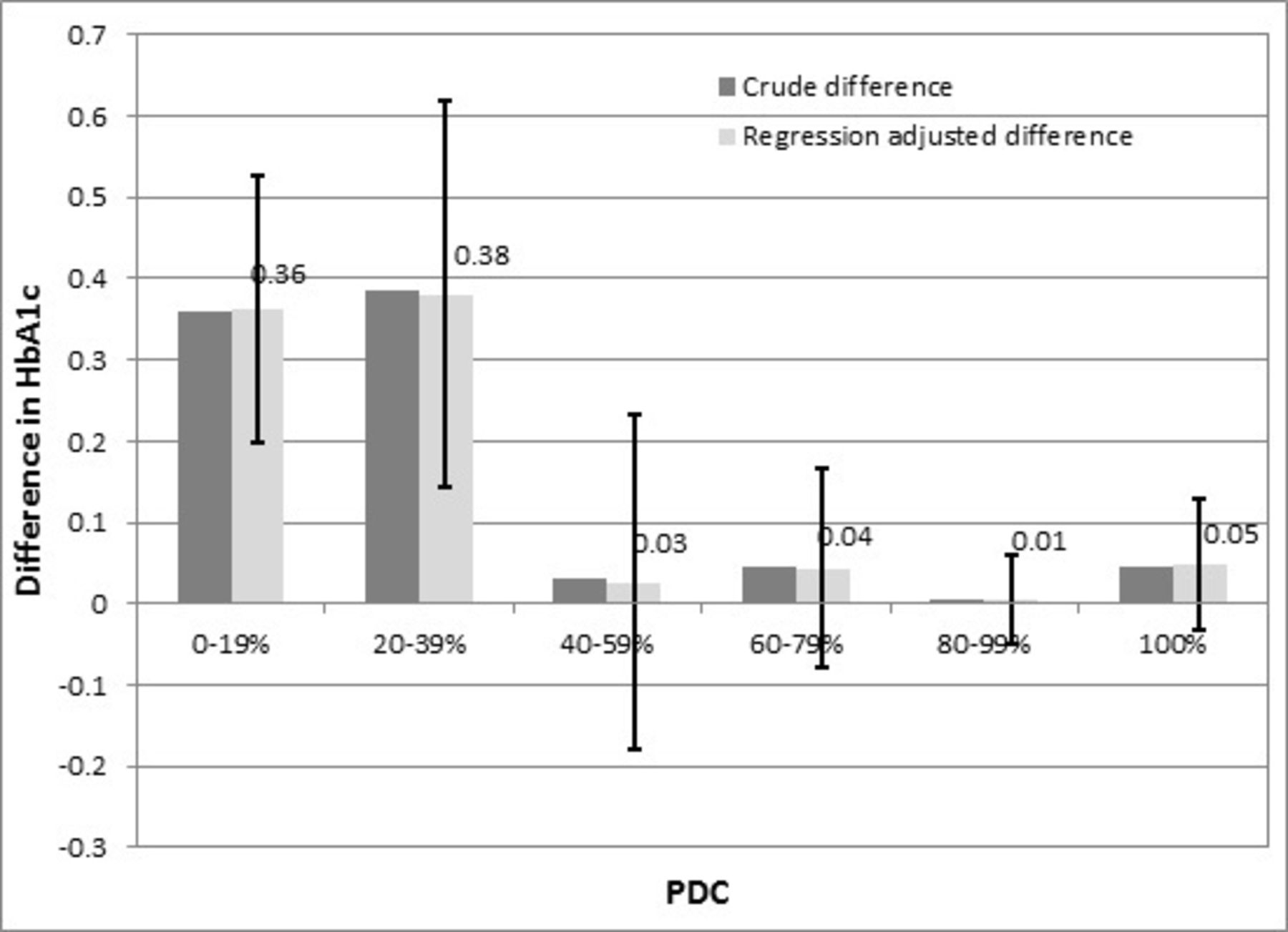
Both the crude and adjusted changes of HbA1c level from baseline to outcome period are shown in figure 2. Average HbA1c level increased for all six adherence groups. The biggest changes were seen in the lowest two adherence groups. After adjusting for patients’ demographics, the changes of HbA1c were not statistically significant for the four higher adherence groups (PDC 40%–100%). However, the two lower adherence groups had significant differences of 0.36 (95% CI 0.20 to 0.53) and 0.38 (95% CI 0.14 to 0.62) over 2 years, respectively.
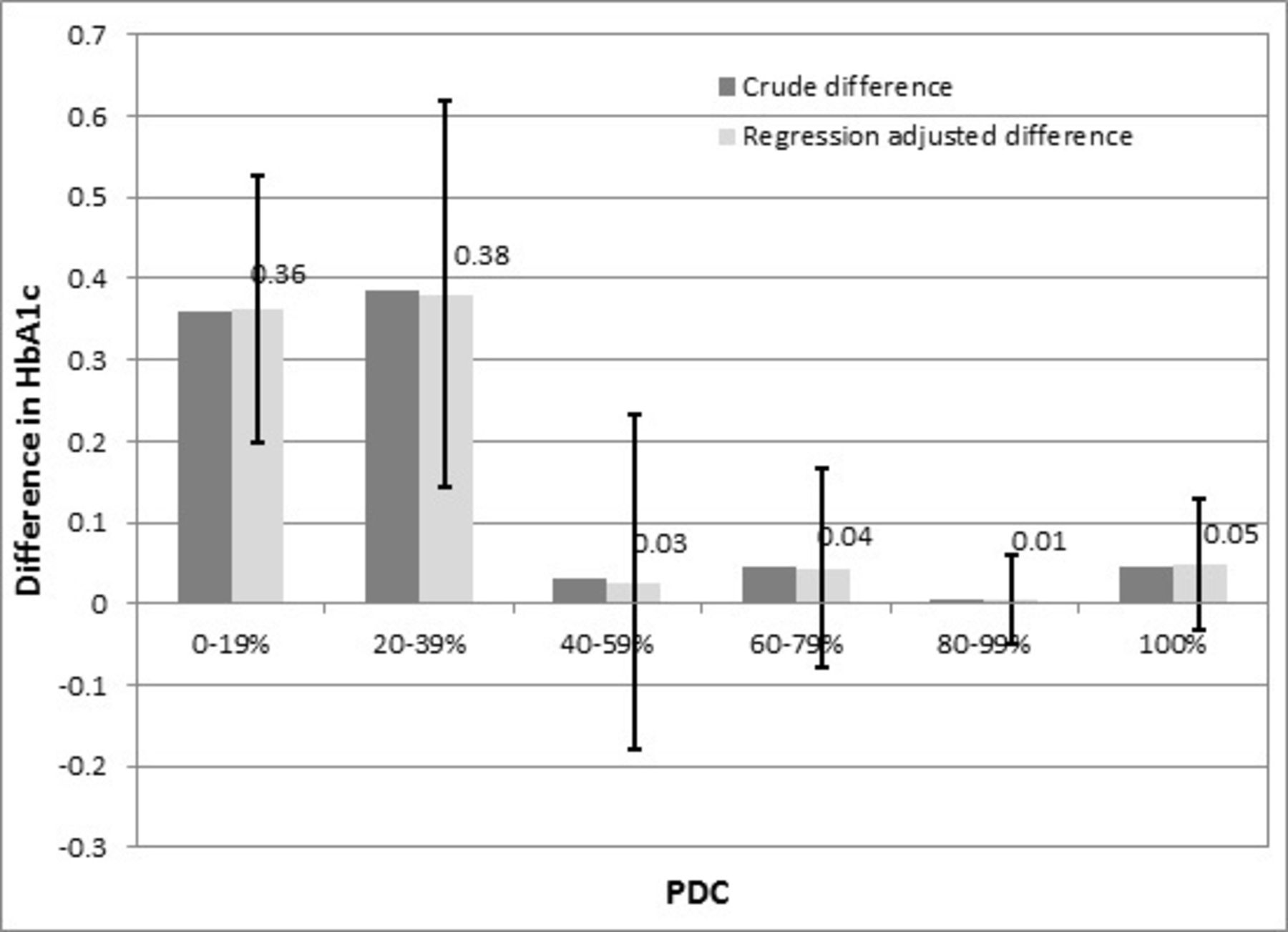
Crude and adjusted HbA1c change by medication adherence group (proportion of days covered (PDC)) by linear regression, controlling for age, age2, gender, race, and marital status (error bar representing 95% CI).
There were some patients who did not have any record of HbA1c test in the outcome period. According to current clinical guidelines for diabetes treatment, patients are recommended to follow-up at primary care centers every six months to monitor HbA1c level and to get medication refilled. If patients do not follow the recommendation, most likely they have no record of HbA1c test and are in low adherence group. The no-record rate was 27% in the lowest adherence group while 0% in the 100% adherence group (table 3). The higher adherence the group was, the lower the no-record rate. The no-record patients were excluded from the calculation of average HbA1c change, which might bias the estimation of the association between adherence and glycemic control. To understand how the no record affects our estimates, we applied another multivariable logistic regression with an indicator of whether there was no record of any HbA1c test in the outcome period as the dependent variable. The associated covariates also included indicators of whether the patient had inpatient visit and whether they had ED visit besides patient demographics, hypertension, dyslipidemia, and baseline HbA1c level. The regression showed strong positive associations between no record and both hospitalization (OR 5.2, 95% CI 3.5 to 7.8) and ED visit (OR 2.0, 95% CI 1.3 to 3.1). It means that patients with hospitalization or ED visit during the outcome period were also more likely to have no record of HbA1c test during the same period. Since lower adherence groups have larger proportion of no-record patients and the failure of glycemic control leads to more medical resource use, we were likely to underestimate the impact of medication adherence on glycemic control.
Primary and secondary outcomes by medical adherence group (proportion of days covered (PDC))
Association between medication adherence and healthcare use
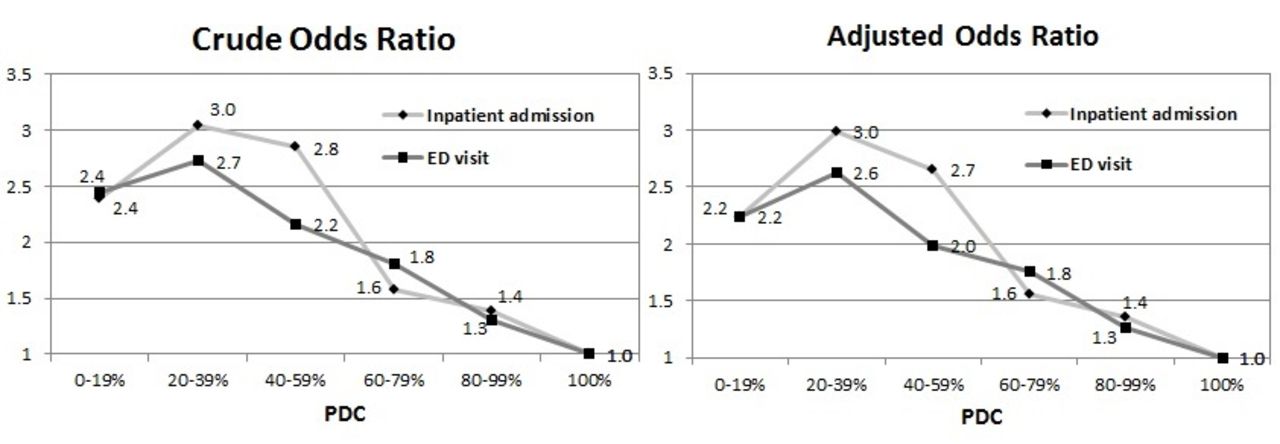
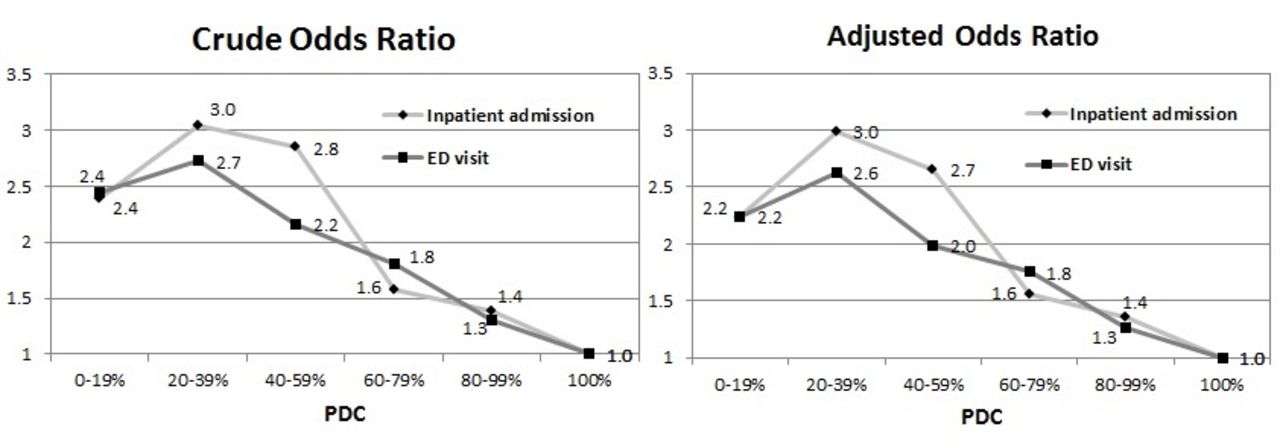
Non-adherence patients (PDC <80%) accounted for 35% of all study subjects. These patients were 73% and 75% more likely to have ED visits and hospitalization compared with adherence patients (PDC ≥80%). When we further classified PDC into six groups and set the group of PDC=100% as reference, the lower the adherence the higher the probability of ED visit and hospitalization except the lowest adherence group. After adjusting for all other covariates, all other adherence groups except that of 80%≤PDC<100% had higher risk of hospital admission or ED visit during the outcome period compared with the reference group (PDC=100%) with ORs significantly >1 (p=0.04) (figure 3).
{kind=link}
{kind=link}
{kind=link}
Crude and adjusted ORs of hospitalization or emergency department (ED) visit by medication adherence group (proportion of days covered (PDC)) by linear regression, controlling for age, age2, gender, race, marital status, years in hypertension, years in dyslipidemia, and baseline Hba1c level (reference group: PDC=100%).
Discussion
In this study, we examined the risk factors of poor medication adherence as well as the association between medication adherence and glycemic control in newly diagnosed diabetes patients. Medication adherence for diabetes patients has been reported in various studies.27–29 We extracted dispensed medication records from our disease registry and calculated PDC as a measure of adherence since it is the preferred method of measuring medication adherence.30 The prevalence rate of medication non-adherence (PDC <80%) among the newly diagnosed diabetes patients was 35%, which was higher than that reported by Ho et al (21.3%)27 but lower than that reported by Boye et al (36.9%)28 and Huber et al (57.6%).29
We found that there were ethnic differences in medication adherence. Indian was more likely to be medication non-adherent compared with Chinese, Malay, and others in Singapore. Strong evidence of racial and ethnic disparities in long-term medication adherence has been reported in a systematic review of medication adherence and racial differences in diabetes in the USA.31 The disparities could be caused by both non-modifiable factors like financial burden of medications, competing demands, cultural and social barriers, family support; and modifiable factors like health literacy, language barriers, clinical support services, the patient–provider relationship. In Singapore, highly subsidized primary cares are available to all residents through the public sector primary care clinics. The subsidized monthly flat rate for one diabetic drug is about 5.6 Singapore dollars. It is generally believed that there are few financial barriers for Singaporeans to adhere to medication treatment for diabetes.32 Further studies are needed to investigate the reasons behind. The relationship between patient age and medication adherence was an inverted U-shape. Morrell et al reported a similar relationship between age and adherence to antihypertensive medications. Lower adherence in the oldest group might be due to declines in cognitive functioning, while that in the youngest group might be due to competing life demands.33
We found that patients with longer years of hypertension or dyslipidemia were more likely to be medication adherent. The reason might be that patients with multiple chronic conditions cared more about their health conditions or they had been accustomed to take a daily medication and therefore they are more likely to adhere to medical treatment. We also found an inverted U-shaped relationship between baseline HbA1c level and medication adherence, that is, patients with the highest and lowest baseline Hba1c level were associated with poorer medication adherence compared with other groups. DiMatteo et al reported similar results in their meta-analysis on disease severity and patient adherence. They concluded that better patient adherence was associated with objectively poorer health only for patients experiencing disease conditions lower in seriousness; among conditions higher in seriousness, worse adherence was associated with objectively poorer health.34
The relationship between medication adherence and glycemic control has been reported.27 35 Schectman et al found that for each 10% increment in medication adherence HbA1c level decreased by 0.16%.35 Ho et al found that each 25% increase in medication adherence to oral hypoglycemics was associated with −0.05% reductions in HbA1C.27 In this study, we had the similar finding that higher medication non-adherence was associated with poorer glycemic control. Patients with PDC <40% had an increase in HbA1c by 0.38 (about 5%) while those with PDC >40% had no significant change in their HbA1c.
We also studied the association between adherence and the risk of all-cause hospital admission or ED visit. Our results confirm that the poorer the medication adherence the higher the medical resource use. These results are similar to those found in other published studies.23 27–29 Ho et al found that the risk of all-cause hospitalization was 1.58 times for non-adherence patients (PDC <80%) as for adherence patients (PDC ≥80%).27 Huber et al showed that the PDC of antihyperglycemic medication was associated with a 7% decrease in the risk of hospitalization.29 Boye et al also provided evidence that the probability of a hospitalization and emergency room visit decreased monotonically as PDC increased.28 Hong and Kang found that among newly diagnosed type 2 diabetes patients, patients with MPR <80% had a 1.26 times risk in hospitalization compared with patients with MPR ≥80%.23
While adherence itself leads to better glycemic control and fewer ED visits and hospitalizations, patients who are adherent to their medications are also likely to adhere with behavioral modification, glucose self-monitoring, attendance with medical care, and other components of diabetes self-management. These factors are also likely contributing to improved outcomes; thus medication adherence could be both a cause and an effect for a patient who is going to do well.
This study has some advantages/strengths. First, PDC was used as the measure for medication compliance. PDC is more conservative and accurate than the MPR, which is the most popular measure of medication adherence.30 Second, our sample included multiple ethnic groups in Asia, where little literature on medication adherence is available. Third, we focused on newly diagnosed patients and studied their adherence to early pharmacological therapies. The results showed the importance of early medication treatment for diabetes patients. Fourth, the 2-year adherence measure period was longer than other studies. Hence, the evaluation of the effect of long-term medication adherence is possible. Lastly, the adherence measure period and outcome period were separate. The separation would avoid the confusion that health condition affects medication adherence.
This study suffers from a few limitations. First, PDC, which was calculated based on pharmacy records, only indicated the medication refills, but could not reveal whether the patients were actually administered the medications. Self-reported adherence is commonly used in adherence research, but it is limited by patients’ memory/recall. Therefore, to measure longer-term adherence, PDC is still a better option. Second, although our medical records included major public hospitals in Singapore, it was still possible that patients went to private institutions for medical services. This might slightly bias our results. Third, patients with no record of HbA1c test were more likely to be in the lower adherence groups. Our results would be conservative in estimating the impact of medication adherence on glycemic control. Fourth, the hospitalization and ED visits were for all causes, they might not relate to diabetes or its complications. Thus the results are noisier than those if we only include diabetes-related health conditions. However, defining diabetes-related conditions is challenging and might be another source of bias if not properly done. Fifth, there are other possible factors such as obesity and smoking that might be linked to behavioral change and medication adherence. Socioeconomic factors, health literacy, social or family support, and adverse reaction to medication might also be associated with medication adherence. We leave these factors for future studies as they are not available in this study. Lastly, in this study, the medication adherence in the first two years was measured and used to predict the outcomes of glycemic control and healthcare uses in the following three years. The level of medication adherence among patients may change during the following three years, which could affect the outcomes too. However, 2 years of measuring adherence is relatively long enough to capture long-term adherence behavior. Thus the change of adherence level in outcome period would unlikely be significant.
Conclusion
In this study, the prevalence and the negative consequences of medication non-adherence among the newly diagnosed diabetes patients in Singapore were studied. Medication adherence in the early stage of diabetes is important in maximizing the effectiveness of pharmaceutical therapy and preventing healthcare use among diabetes patients. Health policies or interventions targeting the improvement of medication adherence among newly diagnosed diabetes patients are in need.
Acknowledgments
The authors acknowledge the chronic disease management system (CDMS) team from the National Healthcare Group for their efforts on database design, development, and maintenance. The authors thank Dr Chun Wei Yap and Alex You from the National Healthcare Group for providing the data, Dr Gary Ang from the National Healthcare Group for insightful discussions on this research.
References
Footnotes
Contributors L-KL designed the study, performed the analyses, drafted the initial and revised manuscript. YS conceptualized the study, assisted in study design and data analysis, drafted the initial and revised manuscript, and had final responsibility for the decision to submit for publication. BHH provided guidance on study design and critically reviewed the manuscript. DEKC and P-NC critically reviewed the manuscript. All authors approved the final manuscript as submitted. YS is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Competing interests None declared.
Ethics approval NHG's ethics reviewing board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.