Article Text

Abstract
Objective Gestational diabetes mellitus (GDM) is a known harbinger of future type 2 diabetes mellitus (T2DM), hypertension, and cardiac disease. This population-based study was designed to identify gaps in follow-up care relevant to prevention of T2DM in a continuously insured sample of women diagnosed with GDM.
Research design and methods We analyzed data spanning 2005–2015 from OptumLabs Data Warehouse, a comprehensive, longitudinal, real-world data asset with deidentified lives across claims and clinical information, to describe patterns of preventive care after GDM. Women with GDM were followed, from 1 year preconception through 3 years postdelivery to identify individual and healthcare systems characteristics, and report on GDM-related outcomes: postpartum glucose testing, transition to primary care for monitoring, GDM recurrence, and T2DM onset.
Results Among 12 622 women with GDM, we found low rates of glucose monitoring in the recommended postpartum period (5.8%), at 1 year (21.8%), and at 3 years (51%). A minority had contact with primary care postdelivery (5.7% at 6 months, 13.2% at 1 year, 40.5% at 3 years). Despite increased population risk (GDM recurrence in 52.2% of repeat pregnancies, T2DM onset within 3 years in 7.6% of the sample), 70.1% of GDM-diagnosed women had neither glucose testing nor a primary care visit at 1 year and 32.7% had neither at 3 years.
Conclusions We found low rates of glucose testing and transition to primary care in this group of continuously insured women with GDM. Despite continuous insurance coverage, many women with a pregnancy complication that portends risk for future chronic illness fail to obtain follow-up testing and may have difficulty navigating between clinician specialties. Results point to a need for action to close the gap between obstetrics and primary care to ensure receipt of preventive monitoring as recommended by both the American Diabetes Association and the American Congress of Obstetricians and Gynecologists.
- gestational diabetes
- type 2 diabetes onset
- glucose testing
- prevention
- primary care
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Low rates of postpartum glucose testing after gestational diabetes mellitus (GDM) have been reported for limited samples of women, despite national guidelines requiring glucose monitoring and transition to primary care.
What are the new findings?
New findings include: (1) description of characteristics, outcomes, and preventive care pathways for 12 699 women with GDM, using a national big data source, in contrast to studies drawn from regional or institutional settings; (2) 3 years of longitudinal follow-up postdelivery in a group of continuously insured women; (3) investigation of rates of contact with primary care predelivery and postdelivery.
How might these results change the focus of research or clinical practice?
Strategies need to be developed to bridge the postdelivery transition between obstetric services and primary care.
Gestational diabetes mellitus (GDM) is a known harbinger of future type 2 diabetes mellitus (T2DM), hypertension, and cardiac disease.1–5 As many as 60% of women with GDM develop T2DM in the decade after a GDM pregnancy.6–8 Several prevention modalities have been shown to be effective for women with a GDM history who do not meet formal criteria for diagnosis of T2DM. Guidelines from the American Diabetes Association9 and the American Congress of Obstetricians and Gynecologists10 recommend postpartum glucose testing, referral to primary care, early identification, counseling, nutritional modification, exercise programme, and antiglycemic agents.11 12 However, fewer than half of women with GDM receive postpartum glucose testing,13–15 and at least half of women with any serious pregnancy complication are not subsequently followed in primary care.6–8 16 17
We undertook an extended-time, population-based study with national data from OptumLabs Data Warehouse (OLDW), a comprehensive, longitudinal, real-world data asset with deidentified lives across claims and clinical information, to investigate gaps in follow-up after GDM. We report here on: (1) characteristics of continuously insured women with a GDM-associated delivery; (2) outcomes of postdelivery glucose testing, transition to primary care, GDM recurrence, and onset of T2DM within 3 years postdelivery; and (3) pathways to follow-up: care gaps, incomplete surveillance, and optimal care.
Research design and methods
Protection of human subjects
OLDW has extensive, regularly monitored deidentification processes in place. This study was determined to be ‘not human research’ by the Boston University Institutional Review Board.
Sample
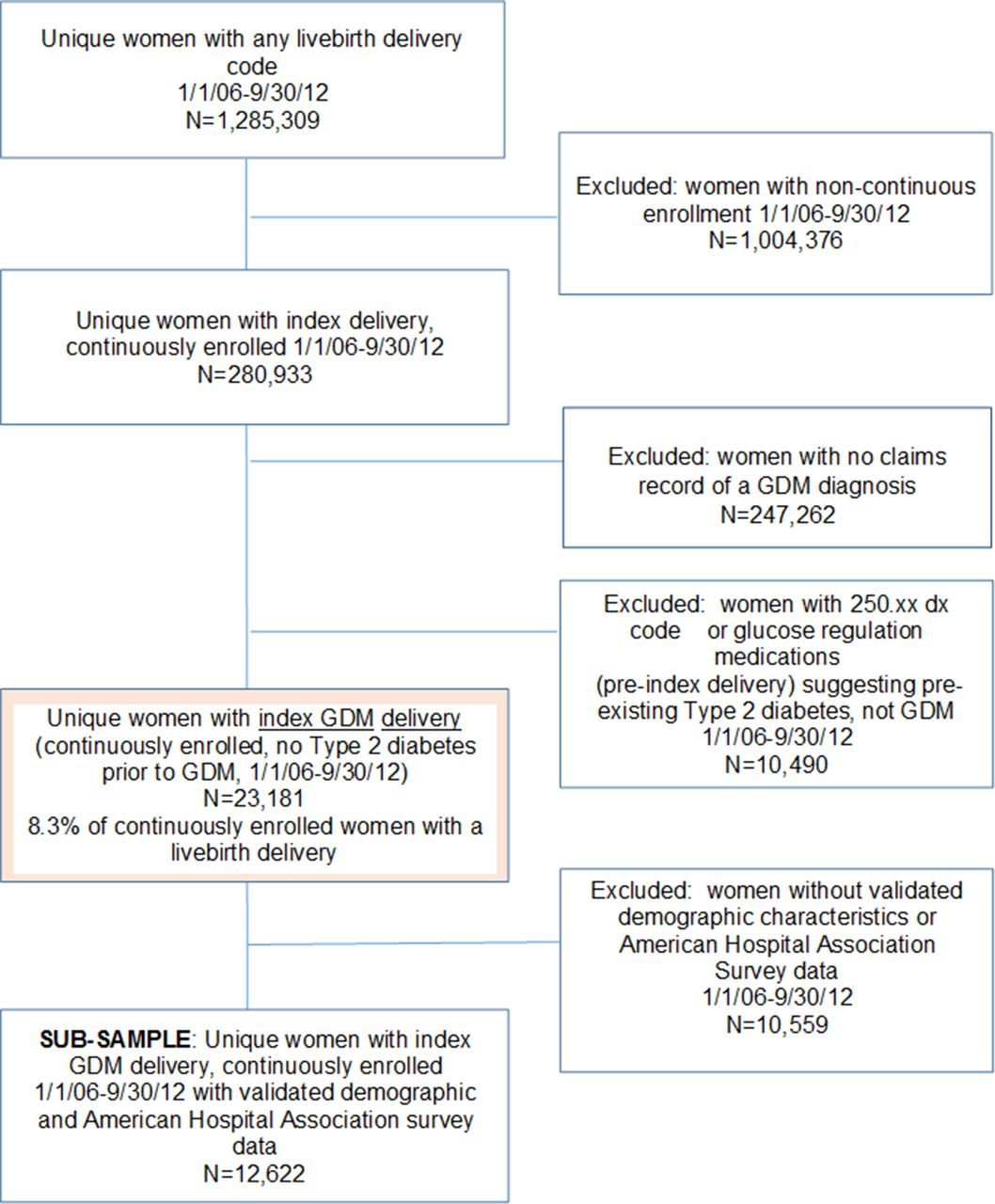
(see Strobe Diagram, figure 1)
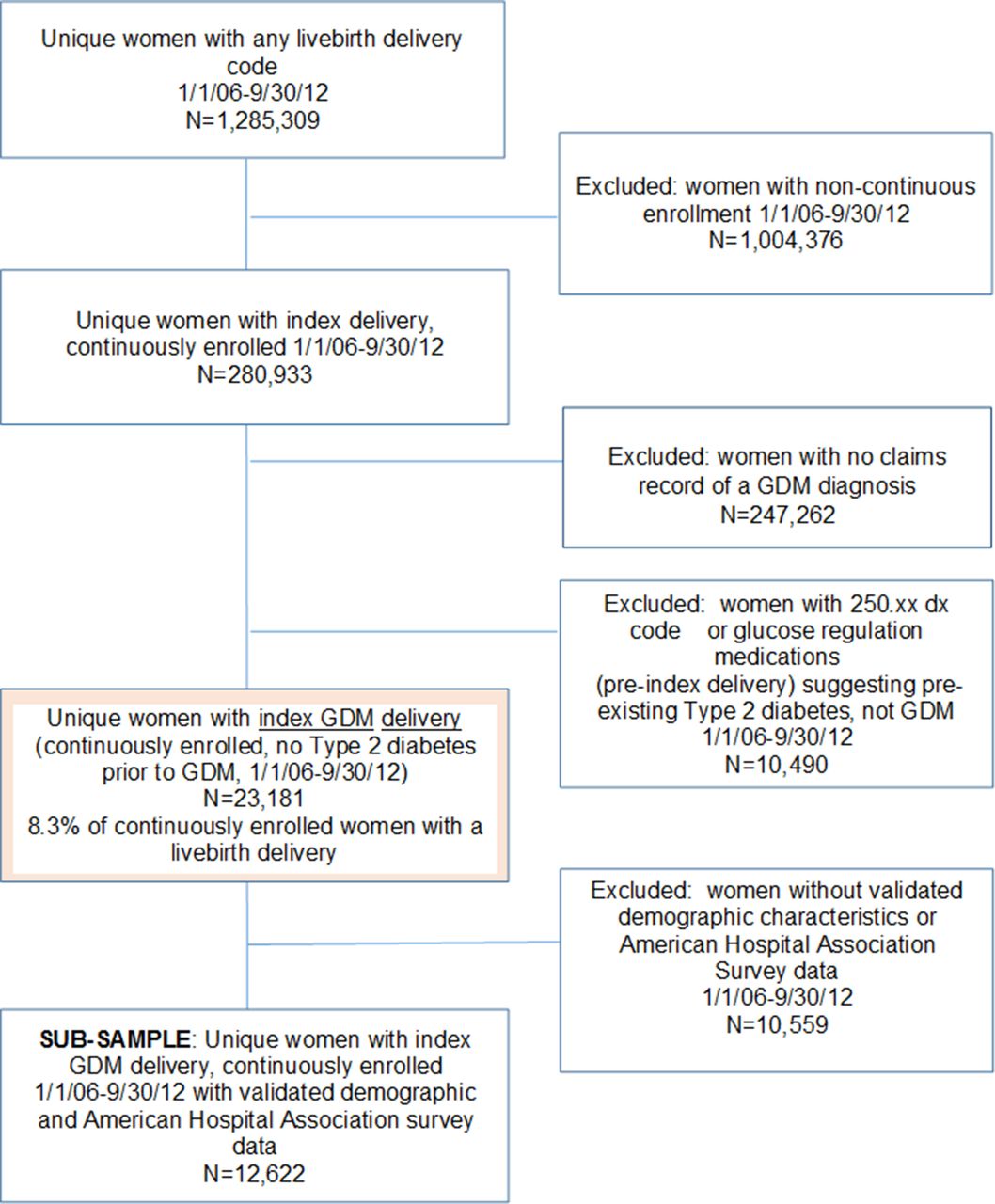
Strobe diagram. GDM, gestational diabetes mellitus.
Inclusions
We identified all unique women with delivery of a live birth from January 31, 2006 to September 30, 2012, as represented by single or multiple claims for pregnancy, delivery and/or postpartum care, using the International Classification of Diseases, ninth revision (ICD-9). We specified the first GDM-affected live birth in the system (ICD-9 GDM code 648.8x) as the index delivery. This study was limited to live birth deliveries because fetal demise and stillbirths present a different risk pattern and different challenges to follow-up care. While these groups are of great interest, our aim was to understand the usual course of care after a pregnancy complicated by GDM.
Exclusions
We then identified women with continuous enrollment during the 5-year interval surrounding their index pregnancy, and excluded those with episodic coverage or ICD-9 codes indicating pre-existing T2DM. We also excluded women who lacked validated demographic data and/or were missing information about service providers and delivery institutions.
Variable construction
A detailed description of processes employed to specify cases and select and refine independent variables and outcome measures is included as online supplemetary table S1.
Supplementary file 1
Case selection: We defined a GDM diagnosis as either one inpatient or two outpatient ICD-9 codes of 648.8, excluding cases with evidence for pre-existing T2DM.
Demographic characteristics include age, race/ethnicity, educational attainment, type of insurance coverage, net worth of assets, and geographic region.
Coexisting conditions include a modified Charlson Comorbidity Index that excluded diabetes,18 and documentation of substance use disorder or mental health diagnoses.19
Prevention behavior indicators include: (1) an influenza shot prior to conception, (2) any visit with a primary care clinician in the preconception year and (3) early initiation of prenatal care.20
Conditions associated with pregnancy and delivery include gestational hypertension, pre-eclampsia/eclampsia, excess prenatal weight gain, prescription of oral hypoglycemic agents during pregnancy, substance use and mental health diagnosis in pregnancy, preterm birth, cesarian section, obstructed labor, hemorrhage and traumatic delivery.
Postpartum conditions include postpartum depression in the year following delivery and postpartum visit.
Healthcare system variables include: characteristics of hospital where delivery occurred, type of provider attending the delivery, and the time frame before or after the implementation of the 2010 Affordable Care Act.
Outcome variables include: (1) glucose testing within the recommended period of 56–84 days postdelivery, and by 6 months, 1 year and 3 years postdelivery, and the number and type of glucose tests during those three periods; (2) any all-cause visit to a primary care clinician (Internal Medicine or Family Medicine) by 6 months, 1 year and 3 years postdelivery, and the number of primary care visits for any cause over the 3-year postdelivery period; (3) the occurrence of repeat GDM pregnancy among those with a subsequent pregnancy during follow-up; and (4) diagnosis of T2DM in the 3 years after an index GDM delivery.
Analytic measures
We conducted descriptive analyses to: (1) estimate the prevalence of GDM and identify characteristics of women in this sample; (2) determine the prevalence of our key outcomes: glucose testing, primary care visits, GDM recurrence in a subsequent pregnancy, and onset of T2DM; and (3) report on factors with the potential to contribute to these outcomes.
Results
Context
Comparability of OLDW data to US data
We used an example year of 2012, and found 17 million individuals across ages and genders with both medical and pharmacy benefit coverage. Compared with US privately insured individuals, OLDW clients are racially representative, somewhat over-represent the South, under-represent the Northeast, and over-represent those aged 18–44 (see online supplementary table S2).
Comparison of OLDW data for 2014 to US data for women of reproductive age, 2014
We identified 7 353 294 unique persons who identified as female (11.7% of US women) and 214 323 live births (5.4% of all US births for that year)21 (see online supplementary table S3).
Sample
Inclusions and exclusions are reported in figure 1. Of the 1 285 309 unique women with live birth deliveries in 2006–2012, 280 993 were continuously enrolled for 1 year prior to delivery and the 3 years of post-delivery follow-up, for an analytic time period of 5 years for each woman within the study time period of January 1, 2005–September 30, 2015. Among continuous enrollees, we found 23 181 women with GDM, 10 490 with pre-existing T2DM mislabeled as GDM, and 247 262 with no evidence for GDM (a GDM prevalence rate of 8.3%). The final sample for this analysis consisted of 12 622 women with GDM, after limitation to women with validated demographic characteristics and provider and institutional data.
Sample generalizability
Comparisons of women retained in the sample with those who did not meet inclusion criteria are found in online supplementary table S4.
Continuity of enrollment
Women with continuity of enrollment (n=2 80 933) were generally similar to those excluded for enrollment gaps (1 004 376), although statistical differences were present (p<0.001), magnified by large sample size. For example, those with continuous coverage were on average 31.6 years old (SD 5.3) compared with 30.0 (SD 5.7) for non-continuous enrollees. Their race was equally likely to be listed as White (50%) with some small differences (<2%) in the racial distributions between Blacks and Asians. Continuously enrolled women were more likely to reside in the Northwest or Midwest and were slightly less likely to be covered under restrictive health insurance plans.
Known versus ‘unknown’ demographic characteristics
Women with validated demographics were similar to the original group of 23 181 GDM women with continuous coverage from whom they were drawn. Those who met inclusion criteria for a complete set of data for age, race/ethnicity, education, net worth of income, provider and hospital characteristics were similar to those who lacked survey data in age and race, coexisting chronic illness, prevention-related behaviors prior to pregnancy, almost all pregnancy-related conditions and all outcomes of interest, but differed slightly in the distribution of type of insurance coverage and geographic location. Those with known demographics had a greater likelihood of receiving medication for GDM versus only nutrition and exercise advice.
Characteristics of women with an index GDM-complicated delivery
Table 1 lists demographic characteristics, health conditions and prevention behaviors, pregnancy and delivery-related conditions, type of provider, and hospital systems characteristics for the final sample of women with GDM (n=12 622).
Demographic, health and systems characteristics of insured women with gestational diabetes, by Consolidated Framework for Implementation domain
This commercially insured sample was primarily white, but still diverse in that it included Asians (12.3%), African Americans (7.4%), and Hispanics (12.9%). Most had some college or a college degree (67.0%), but there were many women with a high school diploma (30.9%) and a small sample of women with no diploma. The majority had comprehensive Preferred Provider Organization (PPO)-type coverage. Net worth of assets was limited (<$25 k) for only a quarter of the women (29.3%), and there was a much smaller proportion (6.5%) in the highest income bracket ($500k+). The Northeast and Mid-Atlantic (10.8%), Pacific (10%) and Mountain (7.9%) regions of the USA were least well represented, and the South most represented (41.1%).
Coexisting chronic illness was relatively rare (mean Charlson Index 0.20, SD 0.59). Among prevention behaviors, less than a quarter of the women received an influenza shot (22.8%) and fewer than one-fifth had a visit of any type with a primary care practitioner (17.5%) in the year before conception. However, 65.5% had a prenatal visit in the first trimester.
Among pregnancy or delivery events and complications, 9.4% experienced preterm birth, and the cesarean delivery rate was 13.2%, consistent with rates reported in other studies.22 Late prenatal visit initiation (third trimester) was a risk factor for 9.4%. The majority of the sample were treated for GDM with diet and exercise advice and monitoring; only 20.8% received medications to control blood glucose. Postpartum depression was an infrequent occurrence (1.2%). Only 39.6% attended a postpartum visit within 56 days postdelivery.
Delivery by obstetricians was most common (93.7%). Certified nurse midwives attended 0.8% of index deliveries, and 5.5% of women were delivered by a Family Medicine physician, Internist or Generalist. An endocrinology visit was recorded during pregnancy for 19.9% of women and a visit with a nutritionist for only 3.3%.
All categories of hospitals were represented, from the very small (1–49 beds and 0–600 admissions) to the very large (400+ beds and 10 000+ admissions). The majority of the women with GDM delivered in medium to large (79.3%), non-government (93.4%), not-for-profit (77.4%) hospitals.
Outcomes
Only 5.8% of women diagnosed with GDM during their pregnancies received any glucose testing within the guideline-recommended time period (table 2). The proportion of women who received at least one glucose test increased during the years following delivery: 21.8% by the end of year 1, and 51.0% by the end of year 3. On average, women who were tested at all had a mean of 2.6 (SD 2.1) glucose tests during the 3 years postdelivery. Slightly more than half of the initial postpartum glucose tests performed in the recommended time period used the guideline-recommended test (an oral glucose tolerance test). In the second and third years after delivery, hemoglobin A1c (HbA1c) testing, which is recommended for continued monitoring, was more common (63.2%).
Pathways to care and outcomes after gestational diabetes (n=12 622)
Within 6 months after delivery, 5.7% of the women in the GDM sample had a visit with a primary care practitioner, 13.8% within 1 year, and 40.5% by year 3. Women in the non-GDM sample (n=247 262) had a similar pattern of care: 12.6% had a primary care visit within 1 year and 36.8% a primary care visit by year 3.
A small number of women (n=2184, 17.4%) delivered another live birth during the 3 years postindex delivery. Among them, 52.2% experienced repeated GDM.
The onset of a new diagnosis of T2DM was recorded for 7.6% of the women in this sample within 3 years of a GDM delivery. No information is available for anyone beyond the 3-year limit. Among the 32.7% of women who had no follow-up of any kind within 3 years (a complete care gap), an unknown number may have had undiagnosed T2DM or rising glucose levels.
Care pathways
At 1 year postdelivery
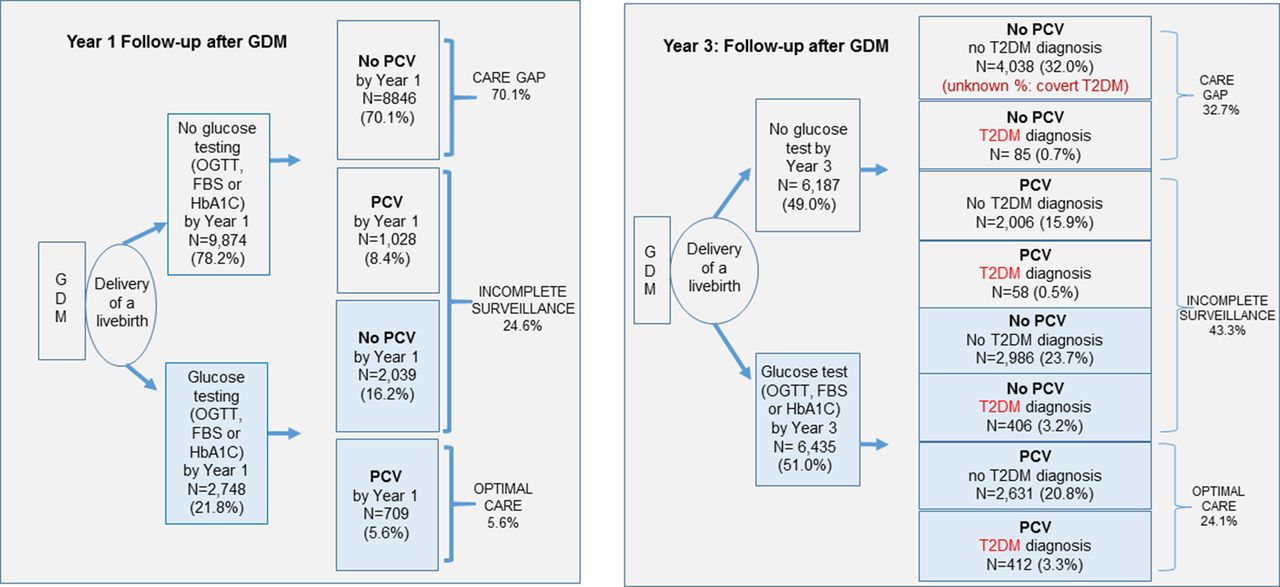
In this study, 8846 women with GDM (70.1%) had a complete care gap at 1 year after delivery (neither glucose testing nor a visit with a primary care clinician), 3069 (24.6%) had incomplete surveillance (either a glucose test or a visit to primary care but not both), and only 709 women (5.6%) received appropriate/optimal care according to the American Congress of Obstetrician and Gynecologist (ACOG) and the American Diabetes Association (ADA) guidelines (testing and visit) (figure 2).
{kind=link}
{kind=link}
Pathways to follow-up after gestational diabetes mellitus (GDM) (n=12 622): glucose testing and primary care visit (PCV). FBS, fasting blood sugar; HbA1c, hemoglobin A1c; OGTT, oral glucose tolerance test; T2DM, type 2 diabetes mellitus.
At 3 years postdelivery
A similar pattern emerges at 3 years, with a care gap for many (n=4123, 32.7%), incomplete surveillance for many more (n=5456, 43.3%), and optimal care (glucose testing and transition to primary care) for a minority (n=3033, 24.1%).
Among women who were diagnosed with T2DM onset by 3 years postdelivery
Within the 49.0% of women who had no glucose testing during the postdelivery interval, 1.2% were newly documented with T2DM onset but received no primary care. Among the women who did receive glucose testing, 406 women in the incomplete surveillance group (3.2% of the sample) developed new onset of T2DM, but did not visit a primary care physician during the study period for follow-up.
Conclusions
This study adds novel information about contact with primary care and glucose monitoring up to 3 years postdelivery. In a large, demographically and geographically diverse sample of continuously insured women, we found that 8.3% of index live birth deliveries were affected by GDM. DeSisto et al estimated a 9.2% prevalence based on self-report and birth certificate data for 2012,23 and a study of claims data in a similar sample produced a 7.2% estimate.17 Differences in estimates may reflect variations in time, sample selection, and restriction to live births.
GDM can herald T2DM and other chronic disease in later life. Specifically, all women with GDM are at high risk of T2DM, and diabetes is a significant and modifiable contributor to cardiovascular disease, the #1 cause of mortality in US women. Evolving data suggest that women who screen negative for glucose metabolism disorders during the postpartum period should be involved in primary prevention (diet and exercise programme).12 We found a 52.2% rate of subsequent GDM recurrence among those with a second delivery in 3 years, and a 7.6% rate of early conversion to T2DM within 3 years postdelivery. Despite this high risk, we report a low rate of postpartum glucose testing in the recommended period (5.8%) and few women with a postdelivery primary care visit (5.7% initially and 40.5% within 3 years). Primary care follow-up after delivery presents opportunities to delay T2DM or prevent deterioration or prevent complications associated with T2DM onset. Insurance access may be necessary for follow-up and prevention, but as this study shows, coverage is not sufficient to prevent gaps in the pathway to recommended care.
In our sample, rates of postpartum glucose testing during the recommended time period were extremely low, and only 60% of the women who were tested received the recommended oral glucose tolerance test (OGTT). Other tests commonly used in the postpartum period have important limitations: fasting blood glucose may only identify 40% of women with impaired glucose tolerance in a diverse population,24 and HbA1c, a more stable measure, may not be sufficiently specific because the time frame it measures can include the third trimester of pregnancy.9
This study confirms known low rates of postdelivery glucose testing, the high risk of GDM recurrence, and early T2DM onset.8 13 15 17 25 26 Early onset T2DM has been reported for 2%–28% of women with GDM within 5 years.27 In our study, the rate was 7.6% within 3 years, underscoring the substantial contribution of GDM to rates of T2DM, and the importance of follow-up. Study results suggest that continuous quality insurance coverage is not sufficient, in itself, to accomplish the necessary transition from obstetrics to primary care after delivery. Lifestyle changes and possibly early intervention with oral hypoglycemic agents can prevent or delay the onset of T2DM in women who have experienced GDM.28 29 The women in this large sample had continuous insurance coverage, yet still had unacceptably low rates of primary care follow-up (5.7% at 6 months, 13.2% at 1 year, and 40.5% at 3 years postdelivery), considering their high risk of GDM recurrence and early T2DM onset. Our study shows that women with GDM are not receiving specialized monitoring compared with women with no GDM, despite wide dissemination of guidelines requiring testing and referral for preventive care.
In the time since women’s healthcare was first described as a patchwork quilt with gaps in 1998,30 there has been little improvement in continuity of care across the life cycle. Transfer of patient care between obstetrics and primary care is still problematic. This large study of a high-risk sample of insured women demonstrates low rates of primary care contact prior to pregnancy and low rates of follow-up with glucose testing and primary care visits after delivery, despite coverage that should ensure access to coordinated care and clear guidelines for testing and referral issued by leading professional organizations. Pathways to care documented in this study demonstrate significant care gaps or incomplete care for the majority of women with GDM, including many of those who experienced new onset of T2DM during the follow-up period.
In a novel consensus meeting to establish research priorities, patients and clinicians in Alberta, Canada31 identified barriers to follow-up, including screening methods, risk communication, lifestyle challenges and the metabolic health of offspring. In a prior study, we interviewed patients and providers, and found a ‘perfect storm’ of missed opportunities.32 Others identify lack of information and multiple roles as patients, parents, jobholders, and family caregivers.33 Work is being done to refine risk calculation for more effective targeting of preventive measures.34 In the Translating Research Into Action for Diabetes study, Ferrara et al 8 successfully implemented a nurse-delivered reminder that raised glucose-testing rates, but other attempts at preventive intervention have encountered barriers to engaging and sustaining patients.35 36 Findings in this study argue for systems changes to create a more obvious pathway from primary care to obstetrics and back to primary care.
American Diabetes Association guidelines for postpartum glucose testing were revised in 2017 to include a 75 gm OGTT at 4–12 weeks instead of the former guidance to test at 42–84 days postdelivery.37 This change puts the time frame for glucose testing squarely within the purview of the obstetric clinician, and allows testing to occur concurrently with the postpartum visit. Under this guideline, a patient with a GDM-affected pregnancy would continue in the care of the delivering practitioner until results of the OGTT are obtained, the patient notified, and an appropriate referral made for follow-up. This new approach has the potential to resolve some of the major aspects of the gap between specialties, but it requires a change in traditional practices that may be slow to implement. An alternative would be to intensify efforts to connect women promptly and more effectively with primary care services. This study shows that women who have a primary care visit prior to conception have higher rates of connection with primary care after delivery. In our sample, 70% of women had neither glucose monitoring nor a primary care visit within 1 year after a GDM delivery, despite having an elevated risk for repeat GDM (52.2% of subsequent pregnancies) and early onset of T2DM (7.6%).
We have presented here key gaps and inconsistencies in care that have the potential to affect outcomes for a large sample of commercially insured women across a range of individual and systems factors. Fortunately, there are means for improvement within the grasp of most systems. Quality assessment of routine blood pressure monitoring for patients with hypertension is just one successful example. Follow-up after GDM could be enhanced by similar quality and accountability measures requiring that patients and providers discuss future risks and set up ongoing glucose testing and referral to primary care as a standard of practice.
Study limitations
We began with a diverse sample of 1 285 309 women with a live birth delivery, and winnowed down to 12 622 in order to meet study conditions. However, we were able to address potential effects of this reductive process on generalizability through comparisons of included versus excluded at each step, demonstrating no difference in key parameters or outcomes. This sample is continuously insured, as are 87% of reproductive-age women.38
Study strengths
Our findings document major gaps in the healthcare pathway. These missed opportunities for prevention emphasize the importance of strengthening the linkage between obstetrics and primary care.
References
Footnotes
Contributors JB and LM researched background data, designed the study, developed methods, analyzed and interpreted results and wrote the article. EQ and OA provided statistical programming and analysis, contributed to the discussion and reviewed/edited the manuscript. TH contributed to the design, planned and supervised the analysis, and reviewed/edited the manuscript. MC reviewed data, contributed to the discussion and reviewed/edited the manuscript. ALP, RI and BJ reviewed variables, contributed to the discussion and reviewed/edited the manuscript.
Funding This study was supported, in part, by NIH RO1 DK107528.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Applications for purchase of this data set may be directed to OptumLabsTM Data Warehouse (OLDW).