Article Text

Abstract
Objective To evaluate variables associated with hemoglobin A1c (HbA1c) and weight reduction when adding liraglutide to persons with type 2 diabetes treated with multiple daily insulin injections (MDI).
Research design and methods This was a reanalysis of a previous trial where 124 patients were enrolled in a double-blind, placebo-controlled, multicenter randomized trial carried out over 24 weeks. Predictors for effect on change in HbA1c and weight were analyzed within the treatment group and with concurrent interaction analyses. Correlation analyses for change in HbA1c and weight from baseline to week 24 were made.
Results The mean age at baseline was 63.7 years, 64.8% were men, the mean number of insulin injections was 4.4 per day, the mean daily insulin dose was 105 units and the mean HbA1c was 74.5 mmol/mol (9.0%). The mean HbA1c and weight reductions were 12.3 mmol/mol (1.13%; P<0.001) and 3.8 kg (P<0.001) greater in liraglutide than placebo-treated persons. There was no significant predictor for greater effect on HbA1c that existed in all analyses (univariate, multivariate and interaction analyses against controls). For a greater weight reduction when adding liraglutide, a lower HbA1c level at baseline was a predictor (liraglutide group P=0.002, P=0.020 for liraglutide group vs placebo). During follow-up in the liraglutide group, no significant correlation was found between change in weight and change in HbA1c (r=0.09, P=0.46), whereas a correlation existed between weight and insulin dose reduction (r=0.44, P<0.001).
Conclusion Weight reduction becomes greater when adding liraglutide in patients with type 2 diabetes treated with MDI who had a lower HbA1c level compared with those with a higher HbA1c level. There was no correlation between reductions in HbA1c and weight when liraglutide was added, that is, different patient groups responded with HbA1c and weight reductions.
Trial registration number EudraCT nr: 2012-001941-42.
- liraglutide
- predictive variables
- HbA1c
- weight
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Predictors for the effect of glucagon-like peptide-1 receptor agonist on HbA1c and weight in individuals with type 2 diabetes treated with multiple daily insulin injections (MDI) have not been studied.
Observational studies without control group have shown that higher baseline HbA1c is associated with a greater HbA1c reduction in other treatment groups.
What are the new findings?
This study showed that lower baseline HbA1c was a predictor of greater weight reduction when liraglutide was added, both within the liraglutide group and when liraglutide group was compared with the placebo group. High HbA1c values did not predict a greater effect of liraglutide on HbA1c when compared with the placebo group.
In this study, there was no association between patients responding with HbA1c reduction and patients responding with weight reduction.
How might these results change the focus of research or clinical practice?
Effects of liraglutide on HbA1c and weight need to be evaluated separately in patients with MDI in clinical practice. Hence, our results indicate that certain patients respond with greater HbA1c reductions and others with greater weight reductions. Those with lower HbA1c levels will decrease more in weight, while those with higher HbA1c levels likely will benefit more from the glucose-lowering effect, since it is known that decreasing from high glycemic levels reduces the risk for complications more than decreasing from lower HbA1c levels.
The use of a control group seems to be important, since many significant predictors in the liraglutide group showed a similar effect in the placebo group.
Background
Diabetes is rapidly increasing worldwide. It is estimated that in 2030 there will be over 500 million adults with diabetes across the world, most with type 2 diabetes.1 Good glycemic control is crucial to avoid complications in type 2 diabetes.2–4 The international guidelines on treatment of hyperglycemia in type 2 diabetes focus on individualizing treatments using combinations of the different available treatment options.5 6 The final treatment option in the recommendations is multiple daily insulin injections (MDI) or basal insulin plus a glucagon-like peptide-1 receptor agonist (GLP-1 RA).6 However, many patients still do not reach glycemic targets.7 In the original analysis of these data, we showed that the GLP-1 RA liraglutide is effective also as add-on therapy to MDI in type 2 diabetes.8
GLP-1 RAs are injectable incretin hormones that enhance glucose-dependent insulin secretion and reduce glucagon secretion by influencing beta cells.9 These agents also exert their effect by centrally increasing feeling of satiety and by slowing gastric emptying.10 This has been shown to reduce both HbA1c and body weight.8 Overall, little is known on predictors for the effect of GLP-1 RAs, and in particular predictors for the effect of GLP-1 RA in individuals with type 2 diabetes treated with MDI have not been studied.
The aim of this study was to evaluate predictors for a beneficial effect of liraglutide on HbA1c, weight and insulin doses in individuals with type 2 diabetes treated with MDI using data from the MDI Liraglutide trial.8 11 We also studied correlations between the different outcome variables to see if the same patients respond with HbA1c reduction and weight reduction.
Methods
The trial was registered in the EudraCT database before study start (EudraCT no 2012-001941-42).
Cohort
This study analyzed data from the MDI Liraglutide trial, a randomized, controlled, double-blind trial carried out at 13 hospitals and 1 primary care unit in Sweden. The design and the main results have previously been published.8 11 124 individuals with type 2 diabetes who were overweight, had poor glycemic control and were treated with MDI were included. The main inclusion criteria were HbA1c 58–102 mmol/mol (7.5%–11.5%), body mass index (BMI) 27.5–45 kg/m2, C-peptide ≥0.10 nmol/L and treatment with MDI for ≥6 previous months, with or without metformin. MDI was defined as any basal insulin combined with separate meal time insulin injections to main meals, with at least two meal time injections per day.
Overall study procedures
Participants were randomized to receive 1.8 mg liraglutide or placebo in addition to insulin therapy for 24 weeks. After randomization, participants had follow-up visits at weeks 6, 12, 18 and 24, where weight, blood pressure and insulin doses were recorded. HbA1c was measured at each follow-up visit, and more extensive blood samples, including blood lipids, proinsulin, C-peptide and adiponectin levels, were measured at baseline, week 12 and week 24. All blood samples were analyzed at the central laboratory, Karolinska University Laboratory (Stockholm, Sweden). At baseline, week 12 and week 24, measurements of waist and hip circumference and abdominal sagittal diameter were made. Participants also completed three separate weeks of masked continuous glucose monitoring (CGM), during the run-in period, week 12 and before week 24. The CGM system consists of a subcutaneous sensor, a wireless transmitter and a receiver, and measures glucose continuously for 1 week.12 When masked, the receiver does not display the glucose values, but stores them for downloading.
Liraglutide was added to insulin therapy according to an algorithm previously described.11 In short, insulin doses were generally not changed, but if blood glucose values were on or close to target at fasting or before a meal doses were reduced to avoid unnecessary hypoglycemia before uptitration of liraglutide or placebo. Insulin doses were then increased to original levels or until target blood glucose values were obtained according to the algorithm.
Predictors for liraglutide effect
To find predictors we evaluated the association between baseline variables and the effect of liraglutide on HbA1c, weight and total daily insulin dose in two steps. We first studied predictors both within the liraglutide group and within the placebo group. To understand if possible predictors were related to the use of liraglutide and not to other study-related causes, we also evaluated whether the predictors were significantly stronger in the liraglutide group compared with the placebo group through interaction analysis. The following baseline variables were evaluated as potential predictors: age, sex, diabetes duration, HbA1c, BMI, weight, abdominal sagittal diameter, waist circumference, waist:hip ratio, adiponectin levels, mean and SD of glucose levels measured by masked CGM, metformin use, fasting C-peptide level, fasting proinsulin level, percentage meal time insulin, and total daily insulin dose. HbA1c was measured according to the International Federation of Clinical Chemistry method, and all values were converted to per cent according to National Glycosylation Standard Program for dual reporting.13 Proinsulin was measured with a commercially available ELISA kit from Mercodia AB.
Correlations
To investigate whether the participants who had a reduction in HbA1c also had a weight reduction or reduced their total daily insulin doses, we studied the correlation between changes in these variables. Corresponding correlation analyses were performed between change in weight and change in insulin doses.
We also summarized the proportion of patients who achieved HbA1c reduction and weight reduction at week 24 in three categories: (1) weight loss ≥3%, (2) HbA1c reduction ≥11 mmol/mol (1% unit); and (3) weight loss ≥3% simultaneously as an HbA1c reduction ≥11 mmol/mol (1% unit).
Statistics
For descriptive purposes, data are presented as mean, SD, median, minimum and maximum for continuous variables, and as n (%) for categorical variables. Baseline comparisons of groups are performed with Fisher’s exact test for dichotomous variables and Fisher’s non-parametric permutation test for continuous variables.
Prediction analyses of change in HbA1c, weight and total daily insulin dose were performed using linear regression with the baseline variables described as predictors in the Predictors for liraglutide effect section, analyzed one at a time. Explanatory variables were treatment group and the baseline predictors, including also an interaction between treatment and baseline predictors. Statistical tests for the effect of the predictors were performed in the liraglutide group only, and tests for treatment with predictor interactions were performed only for predictors that were significant in the liraglutide group at the 5% level. Post-hoc multivariable analyses were also performed, including predictors significant at the 5% level in the liraglutide group.
Correlations between change in HbA1c and weight, between change in weight and total insulin dose, and between change in HbA1c and total insulin dose were studied with Pearson correlation coefficients.
All statistical tests were performed at 5% significance level. All analyses were performed with SAS V.9.4.
Results
Baseline characteristics
Of the 124 participants enrolled in the trial, 122 had at least one valid follow-up measurement and were included in the full analysis set. 63 persons received liraglutide and 59 persons received placebo. Baseline characteristics were comparable in both groups (table 1). More complete information on baseline characteristics has previously been published, including information on diabetic complications.8 The mean age in the cohort was 63.7 years, 64.8% were men, the mean number of insulin injections was 4.4 per day, the mean daily insulin dose was 105 units and the mean HbA1c was 74.5 mmol/mol (9.0%).
Baseline characteristics of the full analysis set
Overall effects on HbA1c, weight and insulin dose
HbA1c was reduced by 16.9 mmol/mol (1.54%) in the liraglutide group, compared with 4.57 mmol/mol (0.42%) in the placebo group, with a difference of −12.3 mmol/mol (95% CI −15.8 to –8.8 (−1.13%, 95% CI −1.45 to –0.81); P<0.001). Body weight was reduced by 3.8 kg in subjects treated with liraglutide, but not placebo (+0.0 kg), with a difference of −3.8 kg (95% CI −4.9 to –2.8; P<0.001). The total daily insulin dose was reduced by 18.1 U with liraglutide and 2.3 U with placebo, with a difference of −15.8 U (95% CI −23.1 to –8.5; P<0.001).8 No severe hypoglycemias occurred during follow-up, and there was no difference in non-severe symptomatic hypoglycemia <4.0 mmol/L between the liraglutide group and the placebo group, with a mean of 1.29 and 1.24 events during follow-up, respectively.8
Predictors of HbA1c reduction
Possible predictors of change in HbA1c evaluated, with regression coefficients and P values, are shown in online supplementary table 1.
Supplemental material
In the liraglutide group the baseline variables HbA1c level (P=0.018), mean glucose level measured by masked CGM (P=0.012) and proinsulin level (P=0.047) predicted the effects on HbA1c, with higher baseline values being associated with greater reduction in HbA1c. Comparing the effect of these predictors between treatment groups, proinsulin remained a significant predictor for change in HbA1c (test for treatment with proinsulin interaction P=0.026), while the effect of HbA1c and mean CGM glucose could not be shown to differ between the two treatment groups (P=0.64 and P=0.38, respectively).
The effects of liraglutide and placebo treatments in reducing HbA1c in relation to baseline proinsulin and HbA1c levels are shown in figure 1A,B. While the effect of liraglutide on HbA1c reduction decreased with lower proinsulin levels, the effect remained significant over the entire range of observed proinsulin levels compared with placebo.
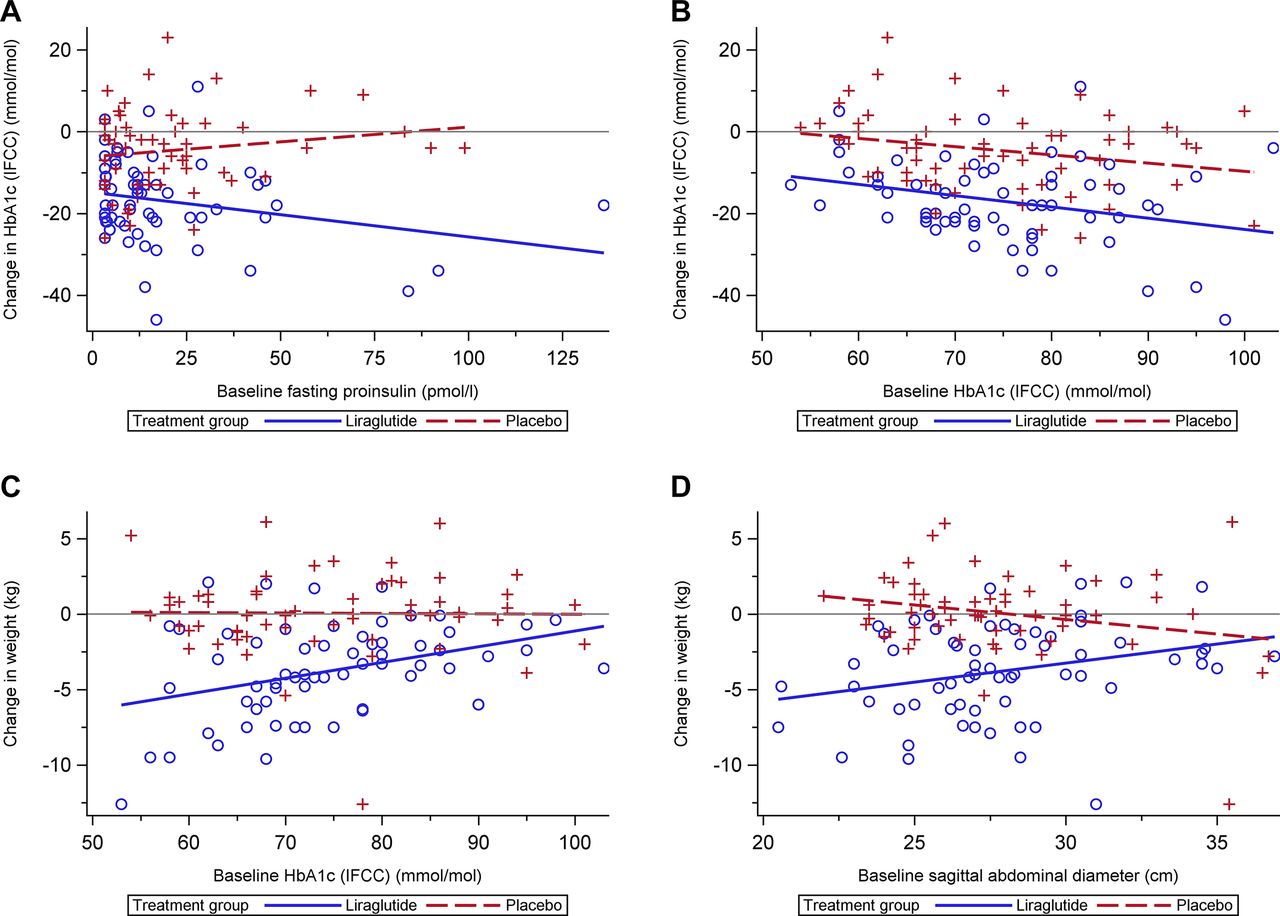
Change in HbA1c and weight compared with baseline variables for the liraglutide group and the placebo group. (A) Change in HbA1c from baseline to week 24 versus baseline fasting proinsulin. (B) Change in HbA1c from baseline to week 24 versus baseline HbA1c. (C) Change in weight from baseline to week 24 versus baseline HbA1c. (D) Change in weight from baseline to week 24 versus baseline sagittal abdominal diameter. HbA1c, hemoglobin A1c; IFCC, International Federation of Clinical Chemistry.
Predictors of weight reduction
Possible predictors of change in weight evaluated, with regression coefficients and P values, are shown in online supplementary table 2.
In the liraglutide group the baseline variables HbA1c level (P=0.002), mean glucose level measured by masked CGM (P=0.003) and abdominal sagittal diameter (P=0.016) predicted the effects on weight, with lower baseline values predicting greater weight reduction. Comparing the effect of these predictors between treatment groups, HbA1c and abdominal sagittal diameter remained significant predictors for change in weight (P=0.020 and P=0.004, respectively), while the effect of mean CGM glucose could not be shown to differ between the two treatment groups (P=0.08).
The change in weight for liraglutide and placebo-treated patients in relation to baseline HbA1c and baseline abdominal sagittal diameter is shown in figure 1C,D. The effect of liraglutide on weight reduction decreased with higher HbA1c levels and greater abdominal sagittal diameter, but remained significant compared with placebo up to HbA1c levels of 92 mmol/mol and baseline sagittal abdominal diameter of 32.5 cm.
Predictors for change in total daily insulin dose
Possible predictors of change in total insulin dose evaluated, with regression coefficients and P values, are shown in online supplementary table 3.
In the liraglutide group, higher total insulin dose (P=0.001) and lower abdominal sagittal diameter (P=0.048) at baseline predicted a greater effect in reducing total insulin dose. Comparing the effect of these predictors between treatment groups, neither could be shown to be stronger in the liraglutide group than in the placebo group (test for treatment with predictor interaction, P=0.50 and P=0.22, respectively).
Post-hoc sensitivity analysis of predictors for change in HbA1c, weight and insulin dose
HbA1c, proinsulin and mean glucose level measured by masked CGM were evaluated further for prediction of change in HbA1c in multivariable analyses. Proinsulin did not remain a significant predictor in the liraglutide group when adjusting for HbA1c (P=0.11) or mean CGM glucose (P=0.23), although the predictor with treatment interaction was on the borderline of significance (P=0.06 adjusted for HbA1c and P=0.08 adjusted for mean CGM glucose).
Similarly, HbA1c, mean CGM glucose and abdominal sagittal diameter were studied in multivariable analyses for prediction of change in weight. HbA1c remained a significant predictor both within the liraglutide group (P=0.003) and compared with placebo (P=0.031) when adjusting for abdominal sagittal diameter. The CGM mean was excluded from the model due to multicollinearity issues arising when simultaneously including HbA1c and mean CGM glucose. Abdominal sagittal diameter also remained a significant predictor in the liraglutide group both when adjusting for HbA1c (P=0.027) and CGM mean (P=0.031), and when evaluated versus placebo (P=0.005 adjusted for HbA1c, P=0.004 adjusted for mean CGM glucose).
Abdominal sagittal diameter, sex and total daily insulin dose at baseline were evaluated in multivariable analyses for prediction of change in total daily insulin dose. Studying the three variables together, all remained significant in the liraglutide group (P<0.001 for abdominal sagittal diameter, P=0.028 for sex and P<0.0001 for insulin dose), but only abdominal sagittal diameter showed a significant effect compared with placebo (P=0.042). Baseline abdominal sagittal diameter did however not show a significant effect when liraglutide addition was evaluated versus placebo in univariable analyses (P=0.22).
Correlation analyses
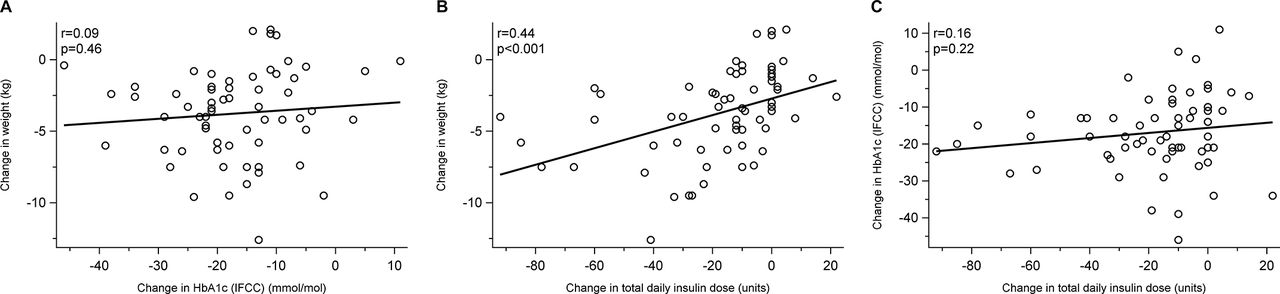
There was no significant correlation between change in HbA1c from baseline to week 24 and change in weight from baseline to week 24 (r=0.09) (figure 2A; P=0.46). Reduction in weight from baseline to week 24 was correlated with reduction in total insulin dose from baseline to week 24 (r=0.44) (figure 2B; P<0.001). There was no significant correlation between change in HbA1c from baseline to week 24 and change in total daily insulin dose from baseline to week 24 (r=0.16) (figure 2C; P=0.22).
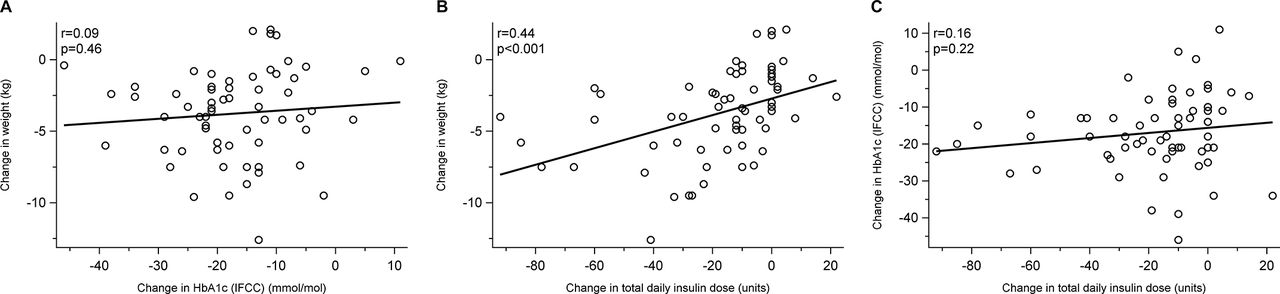
(A) Correlation between change in HbA1c and change in weight from baseline to week 24 in the liraglutide group. (B) Correlation between change in weight and change in total daily insulin dose from baseline to week 24 in the liraglutide group. (C) Correlation between change in HbA1c and change in total daily insulin dose from baseline to week 24 in the liraglutide group. HbA1c, hemoglobin A1c; IFCC, International Federation of Clinical Chemistry.
Figure 3 summarizes the proportion of patients who achieved HbA1c reduction and weight reduction at week 24 by treatment group in three categories: (1) weight loss ≥3%, (2) HbA1c reduction ≥11 mmol/mol (1% unit); and (3) weight loss ≥3% simultaneously as an HbA1c reduction ≥11 mmol/mol (1% unit). There were 76% individuals in the liraglutide who experienced HbA1c reduction of 10.9 mmol/mol (1% unit) and 56% who experienced a weight reduction of 3%. There were 44% who experienced both of these effects simultaneously.

{kind=link}
{kind=link}
{kind=link}
Proportion of patients with HbA1c reduction >1% unit (11 mmol/mol), weight loss >3% and combination of the two from baseline to week 24. HbA1c, hemoglobin A1c.
Discussion
To our knowledge, this is the first placebo-controlled analysis of predictors of response to GLP-1 receptor analog treatment among persons with type 2 diabetes with a complex insulin regimen, MDI. While the original analysis showed an overall HbA1c and weight reduction of 12.3 mmol/mol (1.13%) and 3.8 kg in favor of liraglutide compared with placebo, the current analysis showed that the weight reduction became greater when adding liraglutide in patients with lower compared with higher baseline HbA1c levels. Moreover, there was no correlation between HbA1c and weight reductions when adding liraglutide, that is, different patient groups responded with HbA1c and weight reductions.
Comparison with previous studies
GLP-1 RAs have different effects on the body. The one affecting the beta cells to secrete more insulin9 would lead to a greater HbA1c reduction, while the one affecting feeling of satiety and gastric emptying is believed to be responsible for weight reduction.10 It is because of this that it is not implausible to imagine that the effects on weight and HbA1c are not correlated, as our study shows in persons with type 2 diabetes treated with MDI. Moreover, since patients with lower baseline HbA1c reduced weight more and there was a tendency for greater HbA1c reduction in those with high HbA1c, it may also partly explain the fact that effects on HbA1c and weight do not correlate. Previous studies have shown similar results with liraglutide and dulaglutide in other populations.14 15
Several studies have been performed on predictors of GLP-1 RA effect on HbA1c but not in the current population of persons with type 2 diabetes treated with MDI. Observational and retrospective studies have shown that higher baseline HbA1c is associated with a greater HbA1c reduction in populations switching from insulin or adding GLP-1 RA to current treatment with long-acting insulin analogs. These studies are limited by their observational nature and their lack of placebo controls.14 16
A relatively recent randomized trial evaluated the influence of baseline factors on effect when adding exenatide, another GLP-1 RA, twice daily or placebo to basal insulin. They showed that baseline HbA1c did not predict HbA1c change, similar to our results. Exenatide participants with longer diabetes duration and those with lower BMI had greater HbA1c reductions.17 An open-label, randomized study that compared exenatide once per week with insulin glargine showed that higher baseline HbA1c predicted higher HbA1c reduction within the treatment group.18 In that study, no interaction analyses were performed.
In our study we found that a high HbA1c level at baseline predicted a greater HbA1c reduction in the liraglutide group, but when comparing the same predictor with the placebo group the significance did not remain. This can likely be explained by the phenomenon regression to the mean or study-related causes.19 This illustrates the need for a placebo control group when evaluating predictors of effects of GLP-RA.
To our knowledge little has been done earlier on evaluating the predictors of effect on weight; research has rather been focused on HbA1c effect.20–23 The finding that lower HbA1c predicts greater weight loss has to our knowledge not been described before. This finding could possibly be explained by a previous loss of calories via leakage of glucose to the urine in those with higher HbA1c. When achieving better glycemic control, these calories can instead be used and stored.
Lower abdominal sagittal diameter was a predictor for greater weight loss. In the SCALE study on non-diabetic participants, those with higher BMI had less effect on weight reduction with liraglutide treatment.24 This could indicate that the weight loss is dependent on factors associated with lower BMI and abdominal sagittal diameter.
There were indications that a higher fasting proinsulin level predicted a greater reduction in HbA1c. Fasting proinsulin is believed to be related to insulin resistance and beta cell dysfunction.25 26 A possible explanation for the relation between higher baseline proinsulin and potential greater HbA1c reduction is that GLP-1 RA influences insulin resistance by decreasing visceral abdominal fat.22 Moreover, it is also possible that the association between proinsulin and HbA1c reduction could be explained by GLP-1 RA working by increasing the processing of proinsulin to insulin in beta cells, something that has been shown in mice.27 If this is the case, it could be imagined that those with a higher proinsulin level, and thus a higher insulin resistance and beta cell dysfunction, would have the most effect from GLP-1 RA treatment. Further and more basal research is needed to confirm these findings.
Strengths
A strength of the current study is its double-blinded, randomized design. By performing the interaction analysis as we have done, we take into consideration how the liraglutide group and the control group relate to each other. This means we can rule out other study-related effects or regression to the mean when evaluating predictors.19 We also get an indication if something other than the trial arm is influencing the predictive effect.
Limitations
The trial is somewhat limited by the small number of participants: 122, of whom 63 received liraglutide. We cannot make detailed subgroup analyses or complex multivariable interaction analyses without losing statistical power. It is therefore possible that additional weak predictors would have been detected in a larger patient material. Another potential limitation is the relatively short duration of 24 weeks, which means we can mainly draw conclusions about the predictors for short-term efficacy. However, other studies have shown sustained effects of liraglutide over longer periods of time,28 29 so the same predictors may apply over longer time periods.
Multiple testing
Due to the exploratory nature of this analysis, it was decided to perform all significance tests at 5% level without adjustments for multiple testing. However, the probability of false discoveries was somewhat reduced by the two-step procedure used for evaluation of predictors, followed by post-hoc multivariable analyses, as significance within the liraglutide group, in interaction analyses and in multivariable analyses was required for a predictor to be interpreted as significant. Also, all predictors evaluated in the prediction analyses were predetermined prior to analyzing the data.
Implications
Higher HbA1c did not predict a greater HbA1c reduction in the liraglutide group when comparing with the HbA1c change in the placebo group. This suggests that this drug should be evaluated as a treatment option not only to those with the poorest glycemic control. The fact that those with lower HbA1c at baseline had the greatest weight reduction suggests the same.
The recommendation for usage of GLP-1 RA is still somewhat restricted in national guidelines. For example the National Institute for Health and Care Excellence in the UK has recommended continued treatment with GLP-1 RA only if the patient has lost at least 11 mmol/mol (1.0%) in HbA1c and 3% of body weight in 6 months.30 On the contrary, our results suggest that there is no correlation between improved glycemic control and weight loss during treatment. Our results indicate a need to start looking at these efficacy variables separately when evaluating the treatment. Substantial weight loss may have benefits for the overall health of the patient even if glycemic control remains the same.31 At the same time improved glycemic control has positive health effects even in the absence of weight loss.32
The findings in the current study suggest that fasting proinsulin may be a predictor of the beneficial effects of liraglutide on HbA1c. This needs to be evaluated in other studies to be confirmed. Finding predictors for effective therapy is important since it can increase our understanding of how the drug acts in an in vivo environment. There has been an ongoing discussion why patients seem to vary in their response to treatment, and it is essential in clinical practice to evaluate the effect on an individual basis.
Conclusions
Weight reduction was greater when liraglutide was added in patients with type 2 diabetes treated with MDI who had lower compared with higher HbA1c levels. There was no correlation between reductions in HbA1c and weight when liraglutide was added, that is, different patient groups respond with HbA1c and weight reductions. Hence, when considering initiating therapy and evaluating whether a patient responds to therapy, effects on HbA1c and weight must be judged individually. A composite effect on HbA1c and weight to define a responder should be used with caution.
Acknowledgments
We thank the participants, the staff at participating care units, the local laboratories that assisted in taking blood samples and logistics of laboratory transports, the central laboratory Karolinska University Laboratory, Gothia Forum for monitoring the trial and NordicInfu Care for training on masked continuous glucose monitoring and support with continuous glucose monitoring receivers.
References
Footnotes
Contributors ML, SA, JT and IH designed the study. SD, KF and ML were involved in carrying out the study. HI analyzed the data, and all authors took part in interpreting the data. SD and EA wrote the first draft of the manuscript. All authors revised the manuscript and approved the final version.
Funding The current study was an investigator-initiated trial, where Novo Nordisk provided financial support and study drugs but had no role in the design or execution of the trial; the interpretation, analysis or publication of data; or the decision to submit the written report. NordicInfu Care provided continuous glucose monitoring systems.
Competing interests SD’s institution received grants from Novo Nordisk during the conduct of the study. KF has been a consultant or speaker for Novo Nordisk, Eli Lilly and Boehringer Ingelheim. IH has been a consultant for Abbott Diabetes Care, Adocia, Intarcia, Roche, Bigfoot and Valeritas. JT has received grants from Bayer Pharma, Boehringer Ingelheim, Merck Serono and MSD outside the submitted work, and has acted as a consultant, advisory board member or speaker for Merck Serono, Orion Pharma, Renova and MSD, and is a share owner in Orion Pharma. BA has received lecture fees from Novartis, Merck, Sanofi and Novo Nordisk, and has received grants from Novartis and Merck outside the submitted work. ML’s institution received grants from Novo Nordisk during the conduct of the study. ML has received honoraria or been a consultant for AstraZeneca, Eli Lilly and Novo Nordisk, participated in advisory boards for Novo Nordisk and received research grants from AstraZeneca and Dexcom outside the submitted work.
Patient consent Obtained.
Ethics approval The trial was approved by the ethics committee of the University of Gothenburg, Gothenburg, Sweden (diary no 956–12).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The relevant anonymized patient-level data are available on reasonable request from the senior author (lind.marcus@telia.com).