Article Text

Abstract
Objectives To determine the prevalence of diabetes and awareness, treatment and control of cardiovascular risk factors in population-based participants in India.
Methods A study was conducted in 11 cities in different regions of India using cluster sampling. Participants were evaluated for demographic, biophysical, and biochemical risk factors. 6198 participants were recruited, and in 5359 participants (86.4%, men 55%), details of diabetes (known or fasting glucose >126 mg/dL), hypertension (known or blood pressure >140/>90 mm Hg), hypercholesterolemia (cholesterol >200 mg/dL), low high-density lipoprotein (HDL) cholesterol (men <40, women <50 mg/dL), hypertriglyceridemia (>150 mg/dL), and smoking/tobacco use were available. Details of awareness, treatment, and control of hypertension and hypercholesterolemia were also obtained.
Results The age-adjusted prevalence (%) of diabetes was 15.7 (95% CI 14.8 to 16.6; men 16.7, women 14.4) and that of impaired fasting glucose was 17.8 (16.8 to 18.7; men 17.7, women 18.0). In participants with diabetes, 27.6% were undiagnosed, drug treatment was in 54.1% and control (fasting glucose ≤130 mg/dL) in 39.6%. Among participants with diabetes versus those without, prevalence of hypertension was 73.1 (67.2 to 75.0) vs 26.5 (25.2 to 27.8), hypercholesterolemia 41.4 (38.3 to 44.5) vs 14.7 (13.7 to 15.7), hypertriglyceridemia 71.0 (68.1 to 73.8) vs 30.2 (28.8 to 31.5), low HDL cholesterol 78.5 (75.9 to 80.1) vs 37.1 (35.7 to 38.5), and smoking/smokeless tobacco use in 26.6 (23.8 to 29.4) vs 14.4 (13.4 to 15.4; p<0.001). Awareness, treatment, and control, respectively, of hypertension were 79.9%, 48.7%, and 40.7% and those of hypercholesterolemia were 61.0%, 19.1%, and 45.9%, respectively.
Conclusions In the urban Indian middle class, more than a quarter of patients with diabetes are undiagnosed and the status of control is low. Cardiovascular risk factors—hypertension, hypercholesterolemia, low HDL cholesterol, hypertriglyceridemia, and smoking/smokeless tobacco use—are highly prevalent. There is low awareness, treatment, and control of hypertension and hypercholesterolemia in patients with diabetes.
- Cardiovascular
- Hypertension
- Hypercholesterolemia
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
-
More than a quarter of patients with diabetes in the Indian urban middle class are undiagnosed.
-
In patients with diabetes, cardiovascular risk factors—hypertension, hypercholesterolemia, low high-density lipoprotein cholesterol, and hypertriglyceridemia—are highly prevalent.
-
The status of awareness, treatment, and control of hypertension and hypercholesterolemia is low.
Introduction
Diabetes is endemic in India.1–3 The International Diabetes Federation has estimated that India currently has more than 65 million people with type 2 diabetes and the numbers are poised to double in the next 20 years.1 It has been reported that the prevalence of diabetes among urban participants in India is among the highest in the world and comparable to the high prevalence countries of West Asia and the Pacific.3 ,4 Cardiovascular diseases (coronary heart disease, stroke, peripheral arterial disease) are the major causes of morbidity and mortality in type 2 diabetes. It has been reported that 60–80% of patients with diabetes die of cardiovascular events.5 ,6 Reasons for the increased risk include the high prevalence of major cardiovascular risk factors (hypertension, lipid abnormalities, and smoking) as well as factors specific to diabetes (hyperglycemia, diabetic dyslipidemia, and oxidation-related and glycation-related vascular injury).7
Control of cardiovascular risk factors in diabetes can prevent or delay cardiovascular events. Studies have reported that therapies directed toward the control of blood pressure (BP) and low density lipoprotein (LDL) cholesterol can significantly decrease macrovascular events in diabetes.8 ,9 In India, a high prevalence of metabolic cardiovascular risk factors has been reported among clinic-based patients with diabetes.10 Only a few population-based studies in India have determined the prevalence of various cardiovascular risk factors in patients with diabetes.11–13 No study has evaluated the status of awareness, treatment and control of hypertension and hypercholesterolemia in population-based patients with diabetes . Therefore, we performed this study to determine the prevalence of diabetes, impaired fasting glycemia (IFG) and various cardiovascular risk factors in population-based patients in India with diabetes. We also studied the awareness, treatment, and control of hypertension and hypercholesterolemia, two of the most important cardiovascular risk factors.
Methods
A multisite study to identify the prevalence of cardiovascular risk factors and their sociodemographic determinants was conducted among middle-class urban participants in India.14–17 The rationale for the study has been reported.18 The protocol was approved by the institutional ethics committee of the national coordinating center. Written informed consent was obtained from each participant. The study case report form was developed according to the guidelines of the WHO.19
Regions and investigators
We planned the study to identify the prevalence of cardiometabolic risk factors and their determinants in middle-class urban participants in India.18 Briefly, medium-sized cities were identified in each of the large states of India and investigators with track record of research in cardiovascular or diabetes epidemiology were invited. A steering committee and investigators meeting was organized at the initiation of the study where the study protocol was discussed and developed. The meeting was followed by training in the salient features of the questionnaire and techniques of examination and evaluation to ensure uniformity in recruitment and data collection. Eleven investigators in 11 cities finally performed the survey.14 These cities are distributed in all the geographic regions of the country—northern (Jammu, Chandigarh), western (Bikaner, Ahmedabad), southern (Belgaum, Madurai), central (Nagpur, Jaipur), and eastern (Lucknow, Patna, Dibrugarh).
Sampling
The study data were collected in the years 2006–2010 at various locations. Simple cluster sampling was performed at each site. A middle-class location was identified at each city by the investigator. The middle-class location is based on municipal classification and is derived from the cost of land, type of housing, public facilities (roads, sanitation, water supply, electricity, gas supply, etc), and educational and medical facilities as reported earlier.14 A sample size of about 250 men and 250 women (n=500) at each site is considered adequate by the WHO to identify a 20% difference in the mean level of biophysical and biochemical risk factors.19 We invited 800–1000 participants in each location to ensure participation of at least 500 participants at each site, estimating a response of 70% as observed in previous studies.20 At each site, a uniform protocol of recruitment was followed. A locality within the urban area of the city was identified on ad hoc basis by each investigator, houses enumerated, number of participants >20 years living in each house determined and all these individuals were invited to a local community center or healthcare facility (clinic, dispensary) for examination and blood investigations. This procedure ensured that the study was representative even if the survey was prematurely abandoned.14 The surveys were preceded by meetings with community leaders to ensure good participation. Participants were invited in the fasting state to a community center or medical center within each locality, either twice or thrice a week, depending on the investigator's schedule.
Measurements
The study case report form was filled by the research worker after details were inquired from the participant. Apart from demographic history, details of socioeconomic status based on educational status and years of formal education, type of family, any major previous illnesses, history of known hypertension, diabetes, lipid abnormalities, and cardiovascular disease were inquired. Smoking details were inquired for the type of smoking or tobacco use, number of cigarettes or bidis smoked, and years of smoking or smokeless tobacco use. Intake of alcohol was assessed as drink per week. Details of other diet and physical activity were inquired using focused questions.14 All the equipments for measurements of height, weight, waist and hip size, and BP were similar at the centers to ensure uniformity. Height and weight were measured using a stadiometer and calibrated weighing machines, respectively, and waist and hip circumference was measured using the WHO guidelines.19 Sitting BP was measured after at least 5 min rest using standardized instruments. Three readings were obtained and were averaged for the data analysis. A fasting blood sample was obtained from all individuals after at least 8–10 h fast. The blood samples were obtained at community centers by technicians from an accredited national laboratory—Thyrocare Technologies Ltd, Mumbai, India (http://www.thyrocare.com). Blood glucose was measured at the local biochemistry facility of these laboratories. Blood for cholesterol, cholesterol lipoproteins, and triglyceride estimation was transported under ambient temperature to the national referral laboratory at Mumbai. All the blood samples were analyzed at a single laboratory and a uniform protocol was used for measurements.16 Cholesterol, high-density lipoprotein (HDL) cholesterol, and triglyceride levels were measured using enzyme-based assays with internal and external quality control. LDL cholesterol was calculated using Friedwald's formula.16
Diagnostic criteria
Smokers included participants who smoked cigarettes, bidis, or other smoked forms of tobacco daily, while past smokers were participants who had smoked for at least 1 year and had stopped more than a year ago. Use of other forms of tobacco (oral, nasal, etc) was classified as smokeless tobacco. Individuals with greater than moderate physical activity (30 min of work-related or leisure-time physical activity, >5 times a week) were classified as moderately active. Those with a high dietary intake of visible fat (>30 g visible fat intake/day) and ≤2 dishes of fruits or green vegetables/day were classified as having an unhealthy diet. Hypertension was diagnosed when systolic BP was >140 mm Hg and/or diastolic BP was >90 mm Hg or a person was a known hypertensive.15 Hypercholesterolemia was defined by total cholesterol >200 mg/dL, low HDL cholesterol by levels <40 mg/dL in men and <50 mg/dL in women, and hypertriglyceridemia as >150 mg/dL.16 Diabetes was diagnosed when either a participant was diagnosed by a physician or the fasting blood glucose was >126 mg/dL. Participants with fasting glucose 100–125 mg/dL were diagnosed as those with IFG. Known diabetes by history, those on any drug therapy as being on treatment, and control was defined by fasting glucose ≤130 mg/dL according to American Diabetes Association/European Association of Study of Diabetes criteria.21 The prevalence of various cardiovascular risk factors was determined in participants with and without diabetes. The status of awareness, treatment, and control of hypertension and hypercholesterolemia was also determined using previous definitions.15 ,16 Hypertension control was defined when systolic BP was <140 mm Hg and diastolic BP was <90 mm Hg. Controlled hypercholesterolemia was defined by the presence of total cholesterol <200 mg/dL.21
Statistical analyses
All the data were entered into the SPSS database (V.10.0, SPSS Inc, Chicago, Illinois, USA). More than 90% of the data for various variables were available, and in about 85% of participants the data for all the variables were available. Categorical variables are reported as per cent and 95% CIs. The prevalence of diabetes and IFG in various age groups is reported. Age-related trends were examined by the Mantel-Haenszel χ2 test. Age adjustment was performed using the direct method with the 2001 Indian census population as the standard. Prevalence (%) of various risk factors in participants with diabetes and without diabetes is reported and significance of differences evaluated using χ2 test. p Values <0.05 are considered significant.
Results
The study was performed at 11 cities located in all geographic regions of India as reported earlier.14 In total, 6198 participants (men 3426, women 2772) of the targeted 9900 participants were evaluated (response 62%). Recruitment at individual sites and data for social and demographic characteristics in men and women have been reported.14 Among 5359 participants (men 54.8%, women 45.2%), details of diabetes and various cardiovascular risk factors were available, and therefore these data have been used in the present study.
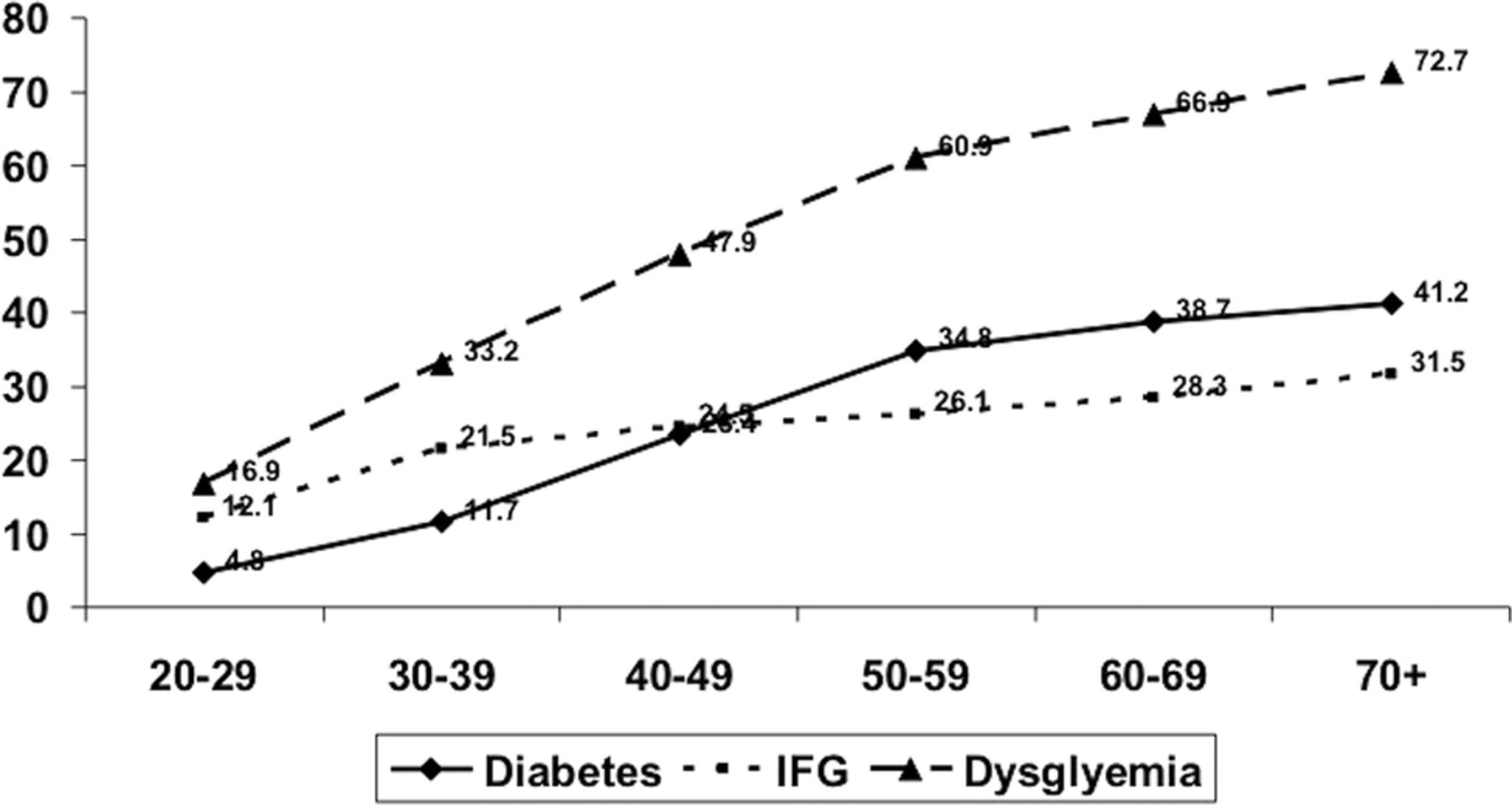
The age-specific prevalence (%) of diabetes and IFG and 95% CI is shown in table 1. There is a significant age-associated increase in the prevalence of diabetes in men and women (p<0.001). The age-adjusted prevalence of diabetes was 15.7% (CI 14.8% to 16.6%); in men, it was 16.7% (CI 15.4% to 17.9%), and in women it was 14.4% (13.1% to 15.7%). The age-adjusted prevalence of IFG was 17.8% (CI 16.8% to 18.7%); in men, it was 17.7% (CI 16.4% to 19.0%), and in women it was 18.0% (CI 16.6% to 19.4%). The prevalence of IFG was greater than that of diabetes in the younger age groups and lower in the older age groups (figure 1). The prevalence of diabetes and IFG equalized at a younger age in men as compared with women (table 1). The prevalence of any dysglycemia (diabetes or IFG) also shows an age-associated increase and is present in more than 60% among older participants (figure 1).
Age-specific prevalence of diabetes and impaired fasting glycemia in men and women

Age-specific prevalence of diabetes, impaired fasting glycemia (IFG), and any dysglycemia.
Of the study participants with diabetes, presence of known disease was in 72.4% (CI 69.6% to 75.2%) and was greater in older participants (table 2). Almost a quarter were undiagnosed (27.6%, CI 24.8% to 30.4%). Of the total patients with diabetes, drug treatment was present in 54.1% (CI 51.0% to 57.2%), and in those with previous diagnosis it was present in 74.7% (CI 71.8% to 77.6%). The status of diabetes control was defined using fasting glucose <130 mg/dL.21 Among all patients with diabetes, control was present in 39.6% (CI 36.5% to 42.7%), and in those with previously diagnosed diabetes it was present in 48.2% (CI 44.5% to 51.9%).
Prevalence (%, 95% CI) of diabetes and status of diagnosis, treatment, and control in various age groups
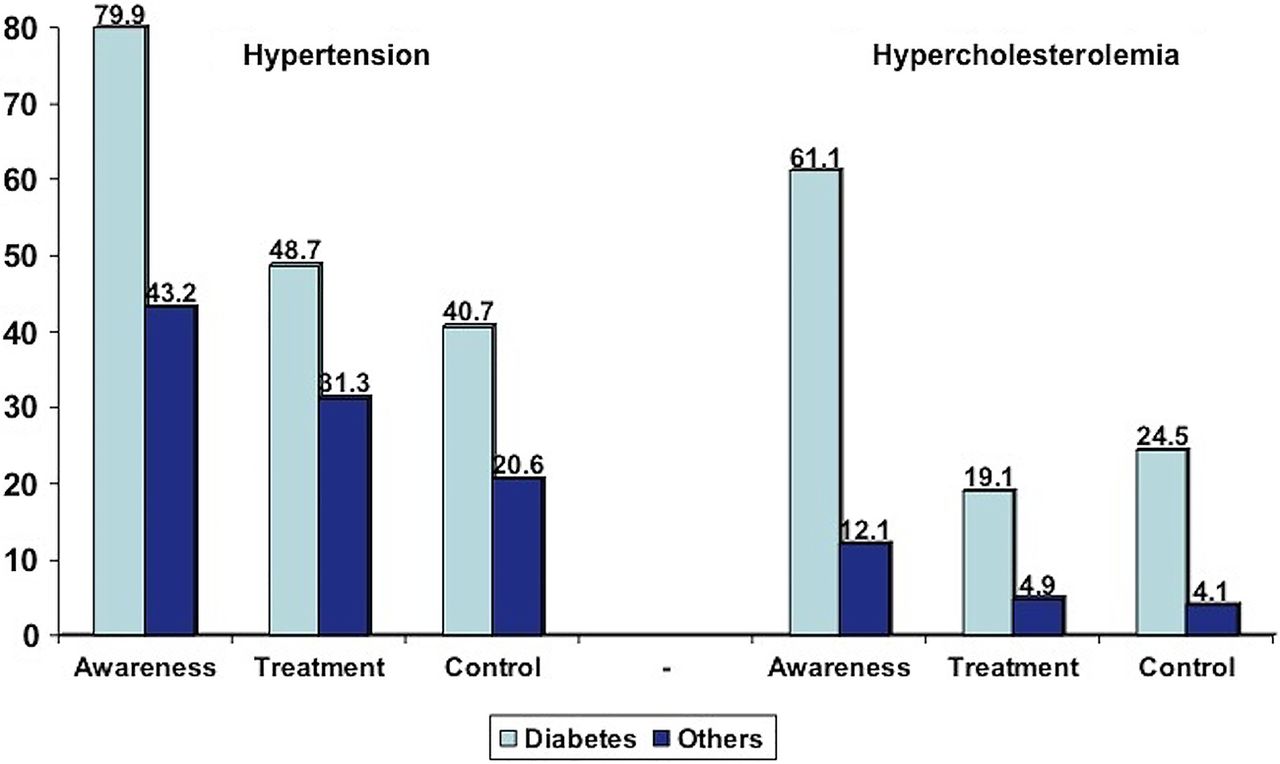
The age-specific prevalence of various risk factors in participants with diabetes is shown in table 3. Among participants with diabetes versus those without, age-adjusted prevalence of hypertension was in 73.1% (CI 67.2% to 75.0%) vs 26.5% (CI 25.2% to 27.8%), hypercholesterolemia in 41.4% (CI 38.3% to 44.5%) vs 14.7% (CI 13.7% to 15.7%), low HDL cholesterol in 78.5% (CI 75.9% to 80.1%) vs 37.1% (CI 35.7% to 38.5%), hypertriglyceridemia in 71.0% (CI 68.1% to 73.8%) vs 30.2% (CI 28.8% to 31.5%), and smoking and/or smokeless tobacco use in 26.6% (CI 23.8% to 29.4%) vs 14.4% (CI 13.4% to 15.4%); (p<0.01; figure 2). The prevalence of smoking was in 18.2% vs 8.9% while that of smokeless tobacco use was present in 13.5% vs 7.9% (p<0.01). In known patients with diabetes versus others, hypertension awareness (79.9% vs 43.2%), treatment (48.7% vs 31.3%), and control (40.7% vs 20.6%) as well as hypercholesterolemia awareness (61.0% vs 12.0%), treatment (19.1% vs 5.0%), and control (total cholesterol <200 mg/dL, 45.9% vs 6.8%; LDL cholesterol <100 mg/dL, 66.5% vs 8.6%) were significantly greater (p<0.01; figure 3).
Prevalence (%, 95% CIs) of various cardiovascular risk factors in participants with diabetes
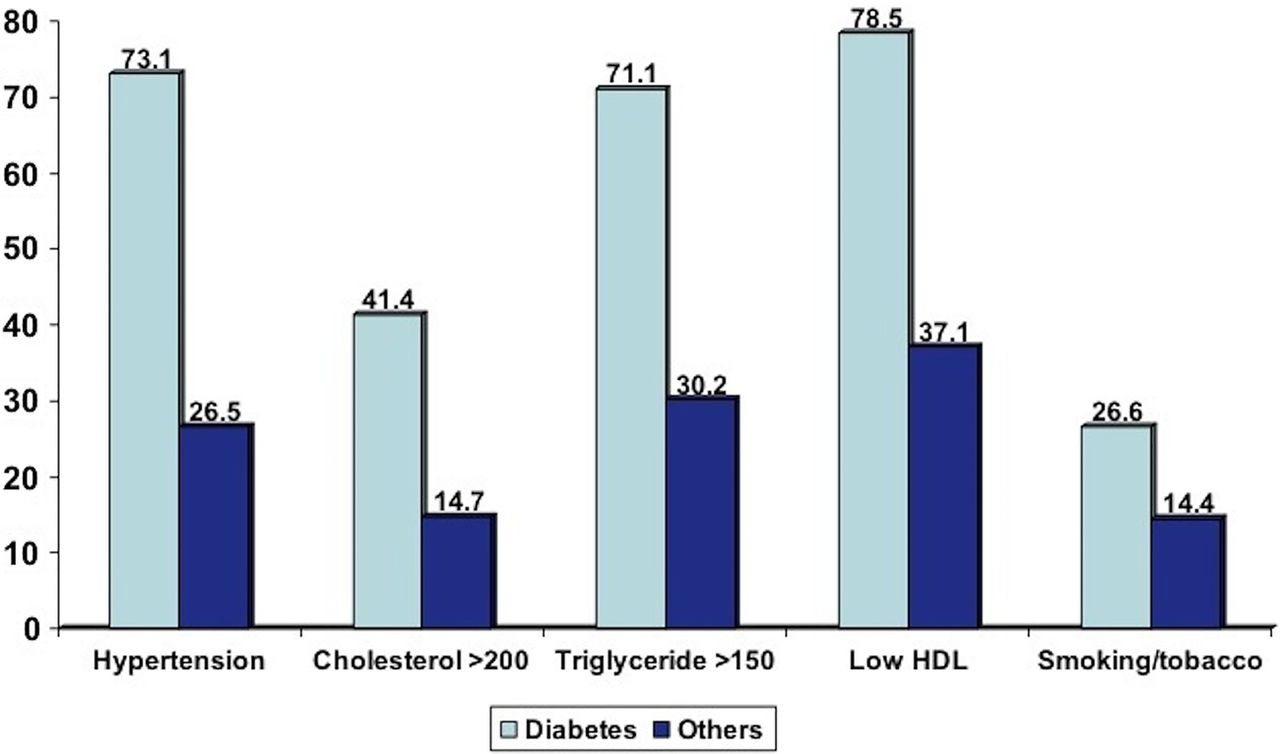
Age-adjusted prevalence of various cardiovascular risk factors in diabetes and others. The prevalence of all risk factors is significantly greater in diabetes (p<0.01). HDL, high density lipoprotein cholesterol; values of cholesterol and triglycerides are in mg/dL.

{kind=link}
{kind=link}
{kind=link}
Status of awareness, treatment, and control of hypertension and hypercholesterolemia (total cholesterol >200 mg/dL) in study participants with known diabetes and others.
Discussion
The International Diabetes Federation has reported that the prevalence of diabetes in adults in India is 7.1%. The prevalence in urban areas is 9%.1 This study shows a greater prevalence among the middle-class urban Indians. The study also shows that participants with diabetes have a high prevalence of major cardiovascular risk factors—hypertension, hypercholesterolemia, low HDL cholesterol, and high triglycerides. The status of diabetes control as well as treatment and control of two important cardiovascular risk factors (hypertension and hypercholesterolemia) is low.
Previous studies in India have reported a greater diabetes prevalence in urban adults as compared with rural adults.2–4 Recent studies have reported urban diabetes prevalence rates of 8–20% and rural diabetes prevalence rates of 5–15%.2 There are only a few multisite studies of diabetes prevalence in India. Using criteria similar to that used in this study, the Indian Industrial Population Surveillance Study evaluated the prevalence of diabetes at seven industrial sites in the country and reported a diabetes prevalence of 8%.22 The Indian Women's Health Study evaluated diabetes in middle-aged women, 35–70 years, in different rural and urban locations of the country and reported diabetes in 2.2% rural and 9.3% urban women.23 The India Migration Study reported diabetes in 13.5% urban, 14.3% migrant, and 6.2% rural participants.24 Multisite studies such as DESI,25 PODIS,26 and INDIAB27 used fasting as well as 2 h glucose estimation for diagnosis of diabetes, and therefore the results are not comparable to those of this study. Regional studies have reported a greater prevalence of diabetes in Southern India as compared with the north, east, and central India.2 ,4 This study reports a prevalence of 15.7%, which is similar to that reported in recent studies from India. We have not presented data on the regional differences in diabetes prevalence due to the small sample sizes (500–1000) at different locations. However, we have earlier shown that regional differences in diabetes prevalence are related more to the Social Development Index28 of the cities and not to the geography; cities with lower poverty indices and better social development indices have a greater prevalence of diabetes and other cardiometabolic risk factors.29 These results are similar to those of studies from China30 and other middle-income countries.31 Larger and more comprehensive studies are required to identify regional differences in diabetes and to evaluate the causes of these differences.32
This study also shows a high prevalence of major cardiovascular risk factors (hypertension, hypercholesterolemia, low HDL cholesterol, hypertriglyceridemia, and smoking/smokeless tobacco use) in participants with diabetes (figure 2). This finding is similar to those from studies from other parts of the world.6 ,7 The greater prevalence of smoking as well as smokeless tobacco use in participants with diabetes is an important finding and is similar to those of previous Indian studies.33 Another important finding is the low prevalence of these risk factors in the population without diabetes and suggests that diabetes is a major driver of cardiometabolic risks in India.7 A high prevalence of undiagnosed diabetes in younger participants (<40 years) is also important and highlights the importance of surveillance and screening among the younger populations for early diagnosis of diabetes in India. This study also shows that diabetes is associated with multiple cardiovascular risk factors and its prevention and elimination can have important consequences for cardiovascular disease prevention.
The prevalence of known diabetes in this study is more than 70% of all individuals with diabetes and is more than those shown by previous reports from India.11–13 We studied the urban middle-class participants and found that the greater prevalence of known diabetes in this population was indicative of greater health literacy.14 We have previously reported higher awareness of hypertension in the present study participants15, this is similar to high awareness of diabetes in the present study. However, only half of the patients with diabetes are controlled to the target of fasting glucose <130 mg/dL. This is similar to previous reports from India.11 The American Diabetes Association and the European Association for Study of Diabetes recommend three markers for the assessment of diabetes control (blood fasting glucose, postprandial glucose, or glycated hemoglobin (HbA1c)).21 We defined control using fasting glucose levels only and did not measure blood HbA1c. This is an important study limitation.
The low status of awareness, treatment, and control of cardiovascular risk factors among participants with diabetes is also an important finding in this study. Only a few international studies have evaluated the status of cardiovascular risk factor control in patients with diabetes. Gakidou et al34 compared the management of diabetes and associated cardiovascular risk factors in seven countries (Colombia, England, Iran, Mexico, Scotland, Thailand, and the USA). This study reported that a substantial proportion of individuals with diabetes remain undiagnosed and untreated in various developed and developing countries and ranged from 24% in Scotland and the USA to 62% in Thailand. The proportion of individuals with diabetes reaching treatment targets for blood glucose, systolic BP, and cholesterol ranged from 1% in Mexico to 12% in the USA.34 Low control of diabetes and hypertension has also been reported in a study in India.35 Our study also shows a low status of control of hypertension and hypercholesterolemia. More studies are required to confirm these findings. The greater awareness, treatment, and control of cardiovascular risk factors in participants with known diabetes observed in this study (figure 3) is similar to that reported in studies in the USA.36
Other limitations of the study are biases introduced because of sampling, non-representation of the Indian population, inclusion of only urban participants, low response rates, measurement techniques, and failure to correct for regression dilution. However, many of the limitations are inherent in a cross-sectional epidemiological study and the data are therefore subject to similar biases.14 Urban locations are hotbeds of the cardiovascular disease epidemic in India,4 and this study is therefore important. Moreover, similar methodology has been used in previous Indian studies and the present data are similarly representative.18 The low response rate in the study (62%) is also a matter of concern and it is possible that those excluded were either more or less healthy as compared with the study participants; however, these response rates are similar to those of other population-based studies in India and elsewhere19 and are within acceptable limits.37 Finally, there are multiple determinants of awareness, treatment, and control of cardiovascular risk factors in patients with diabetes. We have not analyzed the ‘causes of the causes’ or the societal factors38 that lead to greater cardiovascular risk and better awareness of risk factors in study participants. On the other hand, the strengths of the study include a nationwide scope and study of multiple risk factors.
In conclusion, our nationwide study shows that the prevalence of diabetes among the urban middle-class participants in India is greater than that reported by the International Diabetes Federation.1 There is a low status of treatment and control. This study also shows a high prevalence of multiple cardiovascular risk factors among participants with diabetes. The low status of control of hypertension and hypercholesterolemia in participants with known diabetes is a cause for concern. Suitable strategies for improvement of risk factor management and control should be developed in India to prevent premature cardiovascular disease in diabetes.
References
Footnotes
-
Funding The study was financially supported by the South Asian Society for Atherosclerosis and Thrombosis, Bangalore (India) and Minneapolis (USA) grant number Nil of 2006.
-
Contributors RG, PCD, and AG designed the study and developed the protocol; they were also involved in obtaining funding, investigator training, and supervised the whole study. AG and RG jointly wrote the first draft and subsequent drafts of the article. VA, AJA, AB, BG, SG, MVJ, TGM, AM, BS, and JS were the site investigators and supervised the conduct of the study locally. They were involved in data collection and provided inputs for the article and also critically reviewed the whole article and provided suggestions. AG, RG, and KKS were involved in the study supervision, data management, and statistical analyses. All authors have read the manuscript and agree to its contents.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Institutional Ethics Committee, Fortis Escorts Hospital, Jaipur, India.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.