Article Text

Abstract
Background The free androgen index (FAI) calculated using total testosterone measured by immunoassay does not correlate with oocyte fertilization rates; however, there is considerable cross-reactivity for testosterone with other androgens by immunoassay that is not found using isotope dilution liquid chromatography–tandem mass spectrometry (LC/MS/MS).
Aims This study was done to determine relationship between total testosterone and androstenedione measured by LC/MS/MS and fertilization rates.
Study design 49 infertile women without polycystic ovary syndrome were recruited preceding an in vitro fertilization (IVF) cycle. Serum testosterone and androstenedione were measured by LC/MS/MS and correlated with IVF parameters non-insulin resistant compared with insulin resistant (homeostatic model assessment >2.5) women.
Results For non-insulin resistant women, total testosterone FAI and androstenedione did not correlate with oocyte fertilization rates. In insulin-resistant women, there was a negative correlation between both testosterone and FAI and fertilization rates (r=−0.62, p<0.03) and r=−0.73, p=0.02, respectively). There was a positive correlation between androstenedione and fertilization rates (r=0.87, p<0.01).
Conclusion For insulin-resistant women, increases in testosterone and FAI were associated with reduced fertilization rates and androstenedione was associated with increased fertilization rates when measured by LC/MS/MS that should be considered to be the measurement method of choice.
- Insulin Resistance
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Androgen levels appear to be correlated with oocyte response rate but not fertilization rate from hyperstimulation in in vitro fertilization (IVF)
Androgen measurement by immunoassay is imprecise and subject to interference due to cross-reactivity with other androgens.
What are the new findings?
State-of-the art measurement of testosterone confirmed that testosterone did not relate to oocyte fertilization rate in normal individuals, but conversely was detrimental to fertilization in the presence of insulin resistance.
Androstenedione was associated with an increased fertilization rate in insulin-resistant women.
How might these results change the focus of research or clinical practice?
Measurement of androgen levels, specifically by liquid chromatography–tandem mass spectrometry, may help guide treatment strategies in the presence and absence of insulin-resistant states such as polycystic ovary syndrome, to optimize fertilization rates during IVF cycles by improving insulin resistance through weight reduction and insulin-sensitizing agents.
Introduction
Metabolic factors such as insulin resistance (IR) and hyperandrogenemia have been suggested to have important roles in fertility including women undergoing assisted reproductive treatment. In women with polycystic ovary syndrome (PCOS), hyperandrogenemia is a key feature that is associated with a higher rate of an ovulatory infertility. We have shown that the free androgen index (FAI) calculated using total testosterone measured by immunoassay was positively correlated with the ovarian response to hyperstimulation in women without PCOS undergoing in vitro fertilization (IVF); however, there was no correlation of testosterone levels with oocyte fertilization rates.1 Others in a retrospective study have reported that androstenedione and testosterone measured by immunoassay had a positive and negative impact on IVF parameters, respectively.2
There is a considerable cross-reactivity of total testosterone with other androgens in women especially androstenedione and dehydroepiandrosterone sulfate. Liquid chromatography–tandem mass spectrometry (LC/MS/MS) is becoming increasingly available in clinical practice with greater specificity for testosterone and other androgens, and is free from assay interference.3 This study was undertaken to examine the relationship between testosterone and androstenedione determined by LC/MS/MS to the oocyte fertilization rates in women without PCOS.
Materials and methods
All patients gave written informed consent. The study was approved by Hull and East Riding Local Research Ethics Committee. Recruitment details and methods have been described previously.1 In short, 49 women with male factor infertility, without PCOS were recruited preceding an IVF cycle. All women had a regular menstrual cycle and none had polycystic ovaries on ultrasound. Women with a diagnosis of PCOS based on the Rotterdam criteria4 were excluded from the study.
Blood samples and measurements were undertaken after an overnight fast on day 4 of the menstrual cycle preceding the commencement of pituitary down-regulation for IVF. Fasting venous blood was collected into serum gel and fluoride tubes. Samples were separated by cooled centrifugation at 2000 g for 15 min at 4°C, and the aliquots stored at −20°C.
Serum insulin was assayed using a competitive chemiluminescent immunoassay performed on the manufacturer’s DPC Immulite 2000 analyzer (Euro/DPC, Llanberis, Wales, UK). The analytical sensitivity of the insulin assay was 2 µU/mL, the coefficient of variation was 6%, and there was no stated cross-reactivity with proinsulin. Plasma glucose was measured using the Synchron LX20 analyzer (Beckman-Coulter), using the manufacturer’s recommended protocol. The coefficient of variation for the assay was 1.2% at a mean glucose value of 94.6 mg/dL (5.3 mmol/L) during the study period.
The IR was calculated using the homeostatic model assessment (HOMA) (HOMA-IR=(insulin×glucose)/22.5). A HOMA value above 2.5 was used to indicate IR.5 HOMA is a validated surrogate marker for IR and has good agreement with gold standard hyperinsulinemic euglycemic clamp.6
Serum androstenedione and total testosterone were measured by LC/MS/MS on an Acquity UPLC system coupled to a Quattro Premier XE mass spectrometer (Waters, Manchester, UK). Sex hormone binding globulin (SHBG) was measured by immunometric assay with fluorescence detection on a DPC Immulite 2000 analyzer (Euro/DPC) using the manufacturer's recommended protocol. The FAI was obtained as the total testosterone x 100/SHBG.
All participants underwent a standard long-protocol agonist IVF cycle.1 The treatment cycle was abandoned if the total follicle count was below 5, above 25 or if other signs/symptoms of ovarian hyperstimulation were observed. Abandoned cycles were not excluded from analysis. Fertilization rate was calculated by number of metaphase II oocytes divided by total oocytes collected multiplied by 100. Correlation was done between testosterone levels with IVF parameters including fertilization rates in insulin-resistant women (HOMA >2.5) compared with patients who are non-insulin resistant.
Linear regression analysis was used to assess parameters and the outcomes of IVF cycle. Mann-Whitney U test was used to compare means, as the biological data were not normally distributed. P values are two sided and the values ≤0.05 represent statistical significance. Data are reported as mean+SD. Statistical analysis was performed using SPSS for Windows NT, version 15.0.
Results
Nine patients (18%) had a HOMA level indicating IR (>2.5) (insulin-resistant group). The mean age at the start of the IVF/ICSI cycle was (mean±SD) 33.2±4.0 years (non-insulin-resistant group: 33.6±3.9; insulin-resistant group: 33.1±4.1 years). The mean body mass index was (mean±SD) 25.7±4.7 kg/m2 (non-insulin resistant group: 25.9±4.8; insulin-resistant group: 25.3±4.1 kg/m2) and the mean follicle-stimulating hormone level (taken on day 4) was (mean±SD) 5.8±1.5 mIU/mL (non-insulin-resistant group: 5.7±1.3; insulin-resistant group: 5.9±1.6 mIU/mL).
The mean testosterone levels measured using immunoassay were (mean±SD) 2.5±1.4 nmol/L and 0.97±0.46 nmol/L (non-insulin-resistant group: 0.98±0.47 nmol/L; insulin-resistant group: 0.96±0.44 nmol/L) using LC/MS/MS. The mean SHBG level was 65.2±38.6 nmol/L. The calculated FAI was 6.2±6.1 using testosterone measured by immunoassay and was 1.98±1.4 using LC/MS/MS. The androstenedione level measured using LC/MS/MS was 4.4±1.9 nmol/L (non-insulin-resistant group: 4.3±1.8 nmol/L; insulin-resistant group: 4.6±2.1 nmol/L).
There was a significant negative correlation between testosterone measured by LC/MS/MS and fertilization rates (r=−0.62, p=0.03), total dose of gonadotrophin used (r=−0.55, p=0.04) and days stimulated (r=−0.61, p=0.03) in women who were insulin resistant that was not found in non-insulin-resistant women (r=0.09, p=0.32). However, there was no correlation between LC/MS/MS testosterone and fertilization rates (r=0.12, p=0.33) in the group as a whole.
There was also a significant negative correlation between FAI measured by LC/MS/MS and fertilization rates (r=−0.73, p=0.02), total dose of gonadotrophin used (r=−0.60, p=0.03) and days stimulated (r=−0.52, p=0.02) in women who were insulin resistant. This correlation was not found in non-insulin-resistant women (r=0.11, p=0.44). However, there was no correlation between LC/MS/MS FAI and fertilization rates (r=0.12, p=0.33) in the group as a whole. LC/MS/MS FAI showed a positive linear correlation with ovarian response to hyperstimulation as measured by follicle count (r=0.82, p=0.02) without a threshold effect.
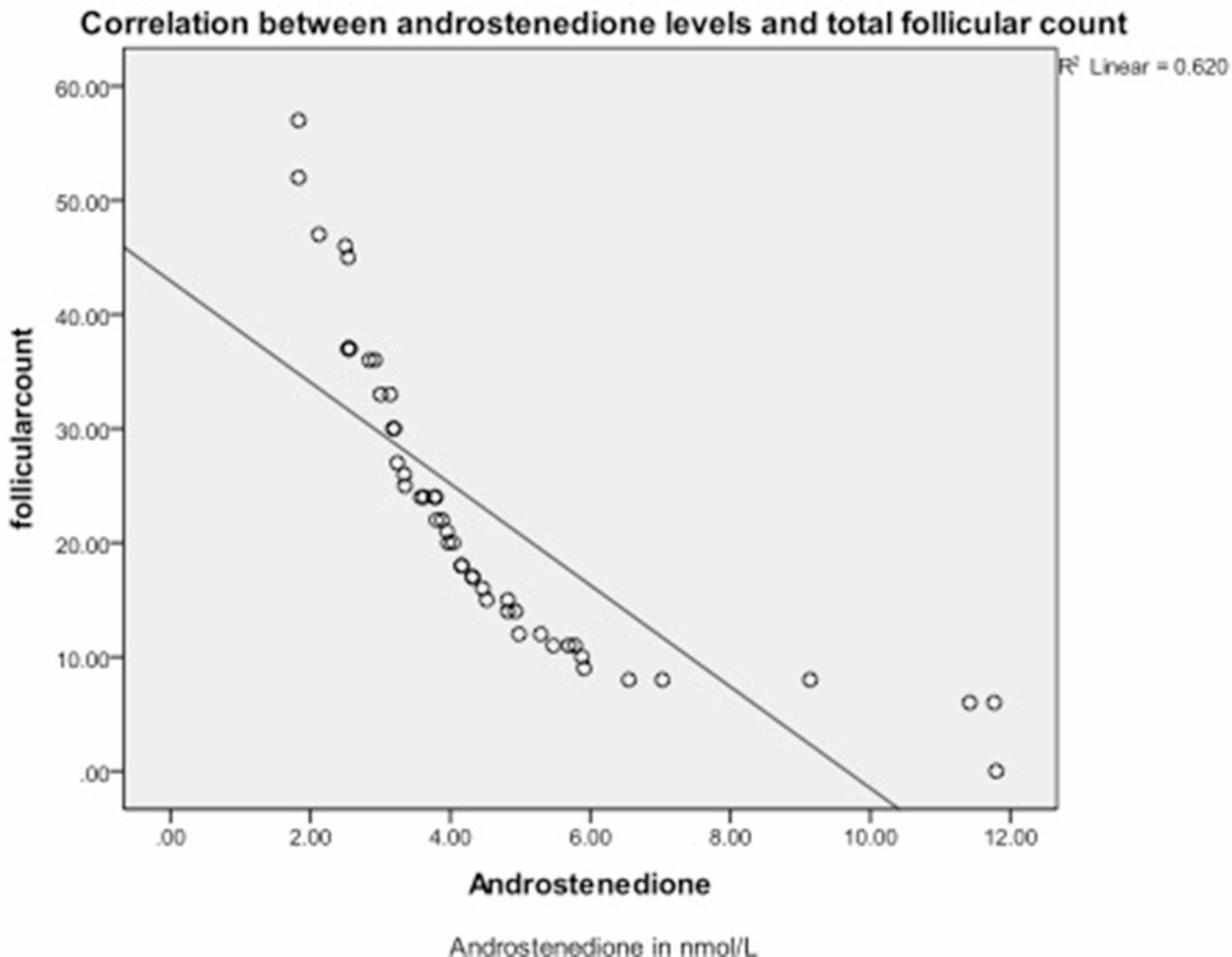
There was a significant positive correlation between LC/MS/MS androstenedione and fertilization rates (r=0.87, p<0.01), total dose of gonadotrophin used (r=0.68, p=0.02) and days stimulated (r=−0.52, p<0.01) in insulin-resistant women. This correlation was not found in non-insulin-resistant women (r=0.11, p=0.44). There was a significant negative correlation of androstenedione with ovarian response to hyperstimulation as measured by follicle count in the group as a whole (r=−0.87, p<0.01) (figure 1).

{kind=link}
Correlation between androstenedione and total follicular count.
Discussion
This study shows that an increase in testosterone and FAI derived from the LC/MS/MS testosterone has a negative impact on oocyte fertilization rates in insulin-resistant women without PCOS undergoing fertility treatment using IVF. This was in contrast to the finding where there was no correlation with oocyte fertilization rates using FAI calculated using testosterone measured by immunoassay.1 Interestingly, in this study, there was a significant positive correlation of androstenedione with various IVF parameters including oocyte fertilization rates in insulin-resistant women, suggesting that the androgen cross-reactivity in the previous immunoassay study may have cancelled out the positive and negative effects of the differing androgens.
This reduction in fertility rates with an increase in FAI in women who have insulin resistance adds to the evidence that insulin resistance augment hyperinsulinemia and vice versa.7 Together this may indicate that that these factors have a negative effect on the ovary and consequently on fertility. In vitro studies have shown that insulin and insulin-like growth factor-1 augment luteinizing hormone stimulation of steroidogenesis in ovary theca-interstitial (thecal) cells.8–11 These data are in accord with the showing that women who have hyperandrogenism and insulin resistance in PCOS have reduced fertilization rates that often require medical intervention to restore fertility.12
FAI in the group as a whole showed a positive linear correlation with ovarian response to hyperstimulation (as measured by follicle count), which was a continuous relationship and was not affected by HOMA. This is in accord with the previous study showing continuous positive linear correlation between the FAI and follicle count.1
There was a negative correlation between testosterone and FAI and total dose of gonadotrophin used for stimulation, which suggests that women with higher testosterone need lower gonadotrophin doses for stimulation. This is in accord with the data showing beneficial effects of testosterone patches in poor responders undergoing IVF to boost ovarian response.13
On the other hand, androstenedione levels had a positive correlation with fertilization rates, total dose of gonadotrophin used and number of days stimulated in women who were insulin resistant. There was also a significant negative correlation of androstenedione with ovarian response to hyperstimulation as measured by follicle count without a threshold effect in the group as a whole. This could be potentially due to the effect of insulin resistance on 17-beta-hydroxysteroid dehydrogenase which converts androstenedione to testosterone.14 15 A recent retrospective analysis using an immunoassay showed a positive correlation of androstenedione levels and a negative correlation with testosterone on IVF parameters in accord with the study reported here.2
The introduction and increase in use of LC/MS/MS into routine practice permits precise and accurate measurements of serum androgens including testosterone and androstenedione. This means that testosterone can be accurately measured in the range of <5 nmol/L that is typically seen in women.16 Measuring testosterone using LC/MS/MS rather than immunoassay will be more helpful in assessing women experiencing subfertility.
These data confirm the finding that there is a threshold effect of insulin resistance below which no clinical effect of androgen levels are seen. Hyperandrogenism with concomitant insulin resistance is a common finding in PCOS, and the use of metformin in these patients to reduce insulin resistance has been widely used. However, this study may explain the discrepant results of the use of metformin in PCOS when after the initial optimistic reports of metformin improving ovulatory rates, a large randomized study in comparison with clomiphene showed that metformin was ineffective.17 Hypothetically, if insulin resistance was reduced though still greater than a HOMA value of 2.5 with metformin, then these data would suggest that the hyperandrogenism would still have a negative impact on fertility and a therapeutic effect of metformin may not be seen.
In conclusion, this study shows that total testosterone and FAI derived from LC/MS/MS measured testosterone showed a reduction in fertilization rates, while LC/MS/MS androstenedione correlated with an increase in fertilization rates in women with insulin resistance but not those without.
References
Footnotes
Contributors TS, EHD, YHZD, SMM and SLA were involved in protocol development, patient recruitment, data analysis and first draft of the manuscript. JR and EHD were involved in sample analysis. TS, EHD, YHZD, SMM and SLA reviewed and edited the manuscript. All authors approved the final version of the manuscript.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Humber Research Ethics Committee, UK.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Sample set and data are available at the Diabetes Centre, Hull Royal Infirmary by contacting the corresponding author.