Article Text

Abstract
Introduction The effects of lifestyle interventions in persons with type 2 diabetes (T2D) on health-related quality of life (HRQoL) and subjective well-being are ambiguous, and no studies have explored the effect of exercise interventions that meet or exceed current recommended exercise levels. We investigated whether a 1-year intensive lifestyle intervention is superior in improving HRQoL compared with standard care in T2D persons.
Research design and methods We performed secondary analyses of a previously conducted randomized controlled trial (April 2015 to August 2016). Persons with non-insulin-dependent T2D (duration ≤10 years) were randomized to 1-year supervised exercise and individualized dietary counseling (ie, ‘U-TURN’), or standard care. The primary HRQoL outcome was change in the 36-item Short Form Health Survey (SF-36) physical component score (PCS) from baseline to 12 months of follow-up, and a key secondary outcome was changes in the SF-36 mental component score (MCS).
Results We included 98 participants (U-TURN group=64, standard care group=34) with a mean age of 54.6 years (SD 8.9). Between-group analyses at 12-month follow-up showed SF-36 PCS change of 0.8 (95% CI −0.7 to 2.3) in the U-TURN group and deterioration of 2.4 (95% CI −4.6 to −0.1) in the standard care group (difference of 3.2, 95% CI 0.5 to 5.9, p=0.02) while no changes were detected in SF-36 MCS. At 12 months, 19 participants (30%) in the U-TURN group and 6 participants (18%) in the standard care group achieved clinically significant improvement in SF-36 PCS score (adjusted risk ratio 2.6, 95% CI 1.0 to 4.5 corresponding to number needed to treat of 4, 95% CI 1.6 to infinite).
Conclusion In persons with T2D diagnosed for less than 10 years, intensive lifestyle intervention improved the physical component of HRQoL, but not the mental component of HRQoL after 1 year, compared with standard care.
Trial registration number NCT02417012.
- diabetes mellitus
- type 2
- exercise
- life style
- quality of life
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
The effects of lifestyle intervention in persons with type 2 diabetes (T2D) on mental health-related quality of life (HRQoL) and subjective well-being (SWB) are not clear, and little is known about the effects of longer term lifestyle interventions with high volumes of exercise (at or greater than current recommended levels) on HRQoL and SWB.
No long-term randomized control studies exploring HRQoL and SWB have used objectively measured levels of exercise or adherence.
What are the new findings?
Lifestyle intervention with high volumes of exercise results in modest improvements in physical HRQoL compared with standard care, partly due to a deterioration in the standard care group.
Lifestyle intervention with high volumes of exercise has no significant effect on either mental HRQoL or SWB, potentially due to relatively high baseline scores.
How might these results change the focus of research or clinical practice?
Persons with short-standing T2D and no diabetes-related complications will likely not experience any major improvements in mental HRQoL or SWB via lifestyle intervention, even when significant reductions in the need for glucose-lowering medications are achieved; potentially reducing chances for long-term adherence.
Future studies should explore the effects of lifestyle intervention on HRQoL and SWB in persons with T2D with diabetes-related complications and/or compromised levels of HRQoL and SWB.
Background
Improving health-related quality of life (HRQoL) and subjective well-being (SWB) should be a central aspect in the care of persons with type 2 diabetes (T2D) given that persons with poor mental health show lower adherence to treatment and lower glycemic control1–3 leading to increased risk of long-term complications.4
The recommended management strategies of T2D include lifestyle changes (diet, exercise, and weight loss) prior to or in parallel with the initiation of pharmacological therapy.5 Lifestyle changes, specifically exercise, have shown to improve mental health especially in people with overt depression and anxiety.6 7 Various psychosocial (eg, self-efficacy) or biological (eg, neuroplasticity) hypotheses have been suggested to explain the positive effects of exercise on mental health.6 However, the effects of exercise on persons’ reported well-being in persons with T2D have been mixed.8 The Look AHEAD (Action for Health in Diabetes) study is the largest and longest running study in persons with T2D designed to determine if weight loss achieved through lifestyle reduces the risk of cardiovascular mortality and morbidity.9 A 1-year follow-up study reported reduced symptoms of depression,10 as well as improved HRQoL,11 specifically in relation to the physical component of HRQoL12 in the intervention group of the Look AHEAD study. A recent systematic review involving persons with T2D found that 15 out of 20 studies showed a positive effect of aerobic exercise on QoL, whereas the effect of resistance training was mixed.13 Analyses of the Italian Diabetes and Exercise Study (IDES) reported that to achieve significant improvement in physical HRQoL, the exercise volume had to be at least 17.5 MET hours/week (corresponding to approximately 210 min of moderate exercise per week).14 This exercise volume exceeds current minimum exercise recommendations of 150 min of moderate to vigorous aerobic exercise, and two to three strength training sessions per week.15 A limited number of studies have specifically explored if exercise and HRQoL are associated in a dose-dependent manner. These studies indicate that higher exercise levels are associated with higher HRQoL.16 17
However, methodological issues in relation to design, exercise adherence, and study duration make the interpretation of earlier studies challenging. The vast majority of studies have prescribed exercise volumes that are lower, or near current minimum exercise recommendations. Thus, very little is known about the potential benefits (or harms) of exercise volumes exceeding current recommendations. Therefore, the mixed results so far relating the effects of exercise on HRQoL could be a result of few studies exploring the effects of exercise levels exceeding the current minimum recommendation. Recently, we reported the results from a 12-month intensive lifestyle intervention (ie, ‘U-TURN’ intervention), which employed exercise volumes two times greater than current recommendations. The results showed that T2D persons had a higher likelihood of achieving discontinuation of glucose-lowering medications while maintaining optimal HbA1c levels, compared with persons receiving standard care.18 However, the effect on HRQoL was not reported. Using protocolized HRQoL data obtained in U-TURN, the aim of the present study was to investigate whether the ‘U-TURN’ intervention may be superior in improving HRQoL and/or mental health compared with standard care in persons with T2D.
Methods
Study design
The original trial (U-TURN) is registered at ClinicalTrials.gov, and a detailed description of the study protocol19 and primary results18 have been published previously. In brief, the U-TURN study was a single-center, assessor-blinded, two-arm, parallel-group trial designed to test whether an intensive lifestyle intervention was equally effective in maintaining glycemic control compared with standard care in persons with T2D in the Capital Region of Denmark.18 Participants were randomized in a 2:1 ratio in permuted blocks of 3 and 6, stratified by sex. The 12-month follow-up was finalized in August 2016 and the primary results were published in 2017.18 For this study, a prespecified statistical analysis plan was developed prior to conducting any of the secondary analyses (online supplemental material 1).
Supplemental material
Participants and eligibility
In brief (see ref 18 19 for details), 98 participants were included in the U-TURN study. Participants recruited to the study were diagnosed with T2D within the last 10 years, aged ≥18 years, and had a body mass index of ≥25 but ≤40 kg/m2. Exclusion criteria were severe comorbidities and/or insulin usage or HbA1c >9% (75 mmol/mol).
Prior to baseline measurements, participants had their glucose-lowering, lipid-lowering, and blood pressure-lowering medications titrated by the study endocrinologist according to prespecified treatment targets.
Intervention
The U-TURN intervention has previously been described in detail.19 In brief, both groups received standard care, consisting of medical counseling, lifestyle advice, and education in T2D provided by a study nurse at baseline and every third month during the 12-month intervention period.
In addition, the U-TURN group received two primary interventions: increased levels of structured exercise and individualized meal plans. The recommended training volume in the intervention was prescribed to reach 240–300 min of aerobic training/week and two or three resistance training sessions/week. All training was performed in groups and supervised across the study period. Supervision was gradually reduced and supported by online supervision. A clinical dietician prepared individual meal plans and the implementation was continuously discussed during group sessions (same groups as the training groups) and during individual counseling. In addition, four supportive interventions were applied: support of increased sleep duration, support of increased levels of daily physical activity, self-monitoring of behaviors related to the other interventions, and diabetes management and education.
Measurements
HRQoL was assessed using the 36-item Short Form Health Survey (SF-36), version 1. This 36-item generic questionnaire consists of eight subscales (physical functioning, role physical, bodily pain, general health, vitality, social functioning, role emotional, mental health), which can be further aggregated into a physical component score (PCS) and mental component score (MCS).20 The scores have a mean of 50 and an SD of 10 in the US general population with higher scores indicating better health. In Denmark, general population studies have found slightly better mean scores: PCS=52 and MCS=54.21 The SF-36 has been used in many studies with persons with diabetes and has shown good reliability, known groups validity, predictive validity, and responsiveness to change.22–24
Well-being was assessed using the Mental Health Continuum-Short Form (MHC-SF) and the Warwick-Edinburgh Mental Well-Being Scale (WEMWBS). The MHC-SF is a 14-item generic questionnaire measuring emotional, social, and psychological well-being. Each item is scored on a 6-point Likert scale with higher scores indicating better well-being and mental health.25 The MHC-SF has shown high internal consistency, discriminant validity, and has been shown to be highly reliable over time.25–27 The MHC-SF categorizes three levels of positive mental health: flourishing, moderate, or languishing. A diagnosis of flourishing mental health requires that the participant experience ‘every day’ or ‘almost every day’ at least 1 out of 3 signs of hedonic well-being and in addition 6 of 11 possible signs of positive functioning during the past 4 weeks. A diagnosis of languishing requires the participant to experience ‘never’ or ‘once or twice’ at least one of the measures of hedonic well-being and low levels on at least 6 of the 11 signs of positive functioning. Participants that are neither flourishing nor languishing are diagnosed as having moderate mental health. The WEMWBS is a 14-item generic scale measuring mental health and mental well-being with Likert scale response options for each item ranging from 1 (none of the time) to 5 (all of the time). Total scores can range from 14 to 70, with higher scores indicating better mental well-being and health.28 The WEMWBS has shown high internal consistency and has been found appropriate to use in the Danish population.29 Mood was assessed using the Global Mood Scale (GMS). The scale consists of positive (eg, active) and negative terms (eg, helpless) that each is rated on a 5-point Likert scale from 0 (not at all) to 4 (extremely). Scores on both the negative affect and positive affect scales range from 0 to 40. Both the negative affect and positive affect scales of the GMS are internally consistent.30 31
All measurements (ie, SF-36, MHC-SF, WEMWBS, GMS) were self-reported and assessed at baseline, and at 6, 8, 10, and 12-month follow-up, except for WEMWBS, which was assessed only at baseline and at 12-month follow-up. All assessments were carried out in parallel to collection of physiological data in the parent trial (U-TURN) (ie, same time points except for 8 and 10-month follow-up). All exercise and physical activity data were registered via a Polar V800 watch (Finland). Participants were instructed to wear the watch 24 hours/day throughout the intervention. Details of exercise volume measurement methods were described in the prepublished protocol.19 Assessments were performed in one laboratory and the biochemical analyses were completed at the central laboratory (Rigshospitalet, Denmark) using standard procedures.
Outcomes
The primary outcome was change in the PCS from baseline to 12-month follow-up. Key secondary outcomes include change in MCS from baseline to 12-month follow-up and the proportion of responders, that is, participants achieving a clinically significant improvement from baseline to 12-month follow-up in PCS: defined as a component score ≥3.4 point change,15 and MCS: defined as a component score ≥4.6 point change.32 Exploratory outcomes include change in the SF-36 subscales, MHC-SF total score, MHC-SF categorical score, change in WEMWBS, and change from baseline in the positive and negative affect scores derived from the GMS, all at 12 months of follow-up.
Sample size and power considerations
No formal power or sample size analyses were performed for the present secondary analysis study. However, for a two-sample pooled t-test of a normal mean difference with a two-sided significance level of 0.05, a total sample size of 96 (allocation ratio of 2:1) has a 95.5% likelihood to detect a statistically significant standardized mean difference (SMD) of 0.8 (36). An SMD is the ratio between the group difference and the pooled SD, and an SMD of 0.8 is considered a large effect.33 Also, the study would have a power of approximately 80% to detect SMD of 0.6 (moderate effect size).33 Thus, assuming that 98 participants will be available from the intention-to-treat (ITT) population (64 vs 34), we should have sufficient statistical power (>80%) to detect a statistically significant difference between the groups corresponding to a moderate to large effect size.
Statistical analysis
The primary analysis was based on the ITT population34 including all randomized participants with available data at baseline. Missing data were handled indirectly using mixed models that provide valid statistical inference assuming that data are ‘Missing At Random’.35 A repeated measures linear mixed model was used including the participant as a random effect factor; fixed effects were treatment group (two levels), time (five levels), the interaction between treatment group and time, and the value of the outcome at baseline. A gatekeeping procedure using serial testing was applied to adjust multiplicity.36 The analyses were performed in sequence until one of the analyses failed to show a significant difference or all analyses had been completed at a statistical significance level of 0.05 (two tailed).
Categorical changes for dichotomous endpoints as well as categorical endpoints were analyzed with the use of logistic regression with participant as a random effect, and treatment group, time, the interaction between treatment group and time, and the value of the outcome (on a continuous scale) at baseline as fixed effects (similar to the analyses of continuous outcomes). From the logistic regression models, the resulting OR values and 95% CIs were converted into approximate risk ratios (RR).37 From the RRs, we estimated the absolute risk difference (RD), which was used to estimate the number needed to treat (NNT) by taking the reciprocal of the RD. The NNT communicates the effect size in absolute terms38 by indicating how many persons with diabetes that on average must be managed with the U-TURN intervention rather than standard care to achieve one additional good outcome.
Sensitivity analyses included non-responder imputation of missing data (ie, ‘Baseline Observation Carried Forward’) and crude analysis of the potentially biased per-protocol population.39 The per-protocol population was defined specifically by adherence to medication and attendance to medical consultations, and for the U-TURN group, specifically, attendance to 70% or more of the prescribed exercise sessions. Further details are available in the statistical analysis plan (online supplemental material 1). All analyses were performed in the statistical program R (V.3.5.1),40 with the packages lme441 and nlme.42
Results
A total of 98 participants were included, 64 in the U-TURN group and 34 in standard care (figure 1). At baseline, participants had a mean age of 54.6 years (SD 8.9) and SF-36 PCS median score of 55.1 points (IQR 49.7–57.7) (table 1). In total, three participants had depression at baseline: two in the standard care group and one in the U-TURN group. Of these, only the participant in the U-TURN group reported receiving antidepressant medical treatment at baseline.
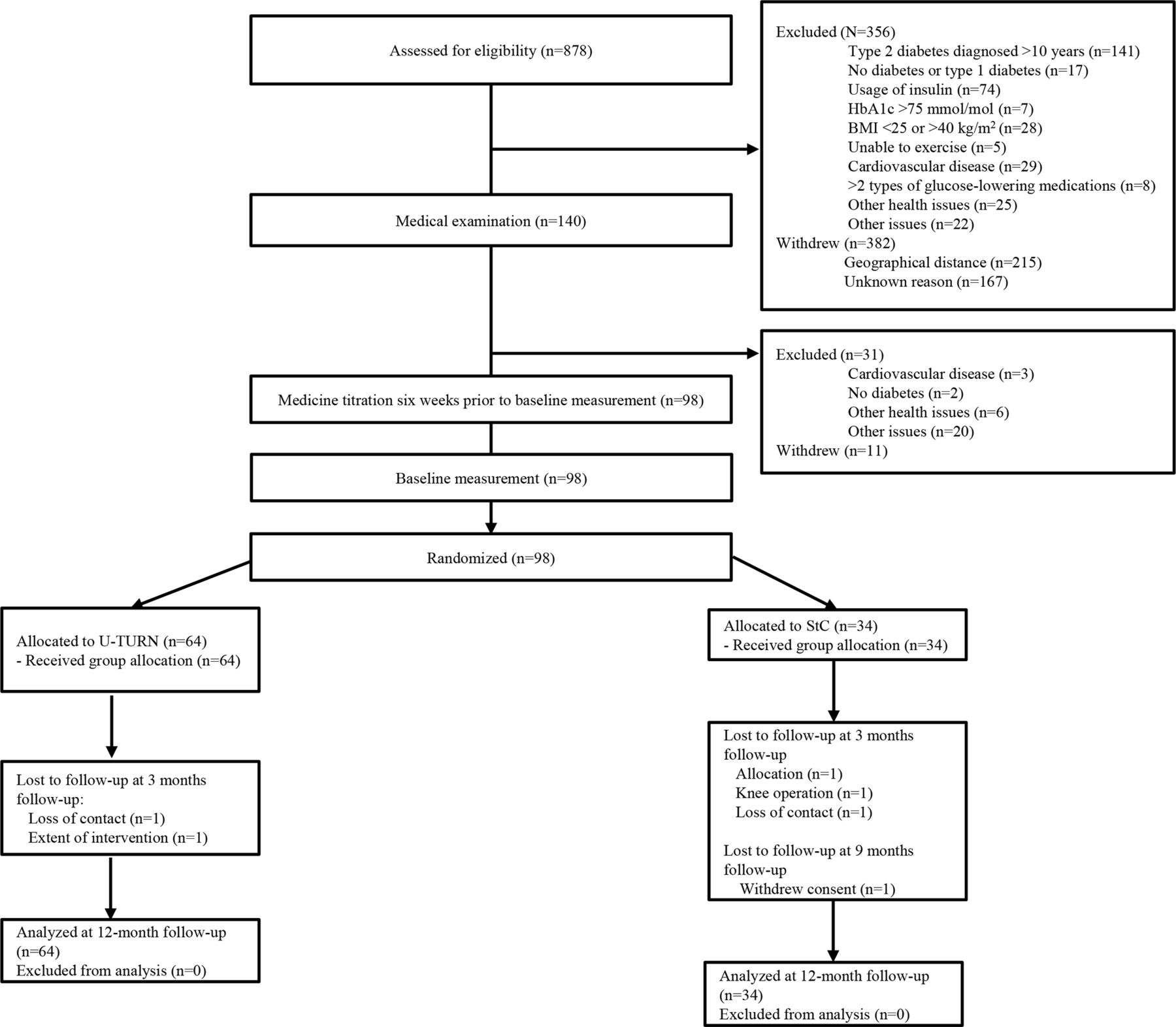
Flow of participants through the study. BMI, body mass index; HbA1c, glycated hemoglobin A1c; StC, standard care.
Baseline characteristics for the intention-to-treat population
From baseline to 12-month follow-up, the U-TURN group reported a mean change of 0.8 (95% CI −0.7 to 2.3) in PCS scale, while the standard care group reported a mean decline in PCS score of 2.4 (95% CI −4.6 to −0.1). The corresponding difference between groups was 3.2 (95% CI 0.5 to 5.9, p=0.020) in favor of the U-TURN intervention (table 2).
Between-group comparisons of the changes in the primary, key secondary and exploratory outcomes from baseline to 12-month follow-up
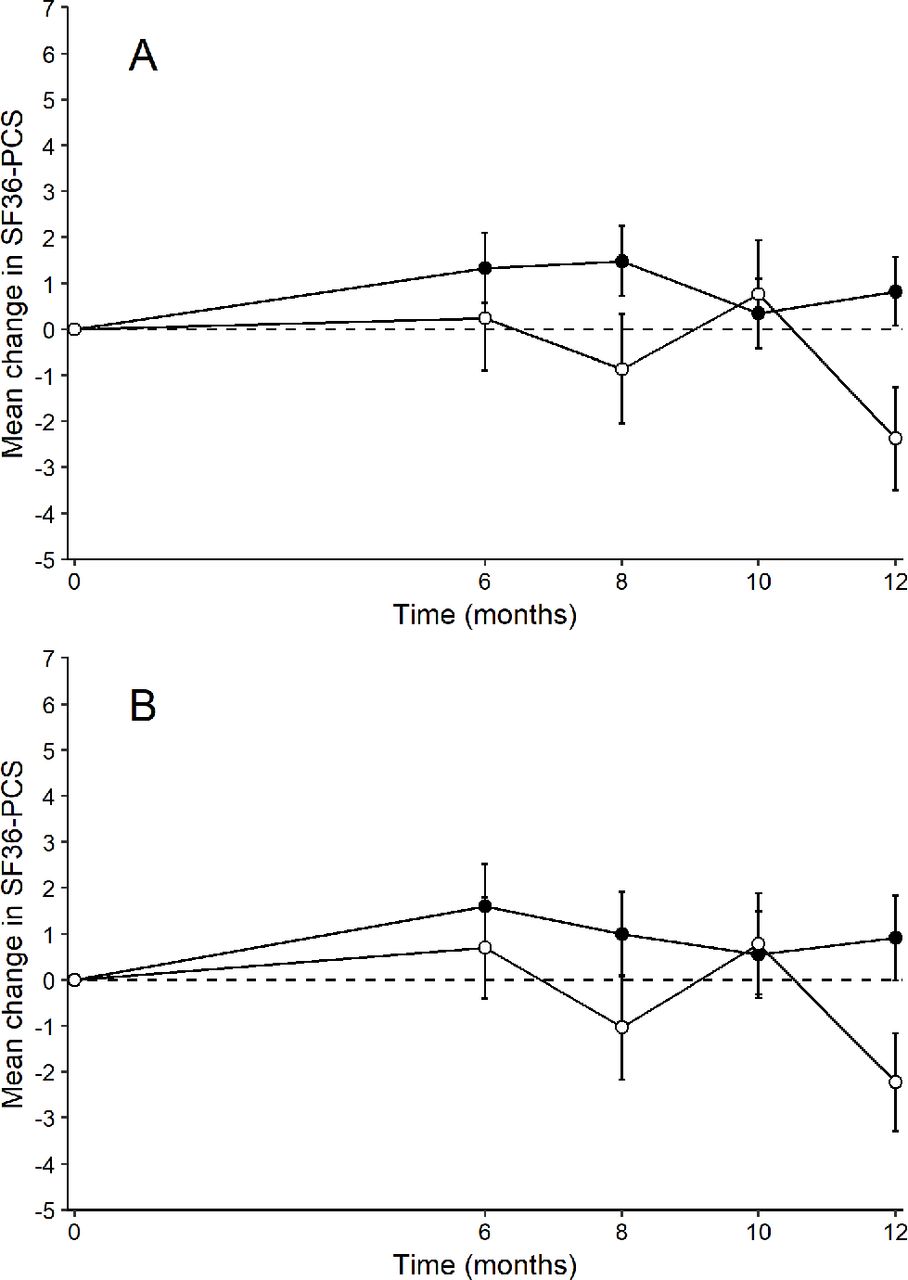
According to the trajectories, the difference between groups mainly appeared at 12-month follow-up (figure 2).

{kind=link}
{kind=link}
Time-course data of the mean changes in SF-36 PCS for the intention-to-treat (ITT) population (A) and the per-protocol population (B). Solid points indicate the intervention group whereas open points indicate the standard care group. The error bars indicate SEs. Least squares means estimates are from repeated measures mixed models with no imputations of missing data. PCS, physical component score; SF-36, 36-item short form health survey.
In the U-TURN group, 19 (30%) participants reported a clinically significant improvement in the PCS score (ie, responders) at 12-month follow-up compared with 6 (18%) participants in the standard care group, with an OR of 4.04 (95% CI 0.94 to 17.43, p=0.061) adjusted for baseline PCS. This means that the participants in the U-TURN group have four times the odds of responding compared with the participants in the standard care group, but the CI is very wide and includes 1 (ie, no statistically significant difference between the groups). The estimated OR corresponds to an adjusted RR of 2.6 (95% CI 1.0 to 4.5) and an NNT was accordingly 4 (95% CI 1.6 to infinite). No difference was observed for the change in MCS, nor for the proportion achieving clinically significant improvements in the PCS score. The sensitivity analyses using the per-protocol population (table 3) and the single-imputation non-responder technique of missing data confirmed the robustness of these findings (online supplemental table 1).
Supplemental material
Between-group comparisons of the changes in the primary, key secondary and exploratory outcomes from baseline to 12-month follow-up for the per-protocol population*
For the exploratory outcomes, changes in SWB and mood were not significantly different in the U-TURN group compared with the standard care group.
Discussion
The main finding in this study was that a 12-month lifestyle intervention, including high levels of exercise, significantly improved physical HRQoL in persons with T2D (diagnosis <10 years) compared with standard care. Specifically, 30% of the participants in the U-TURN group compared with 18% in standard care group achieved a change in score considered to represent a clinically significant improvement in regard to physical HRQoL. Despite the improvement in physical HRQoL, mental HRQoL, SWB, and mood were not significantly improved by the intervention.
We hypothesized that the U-TURN intervention would improve HRQoL and SWB. We based this hypothesis on the fact that the U-TURN participants achieved significant reductions in the need for glucose-lowering medications, with more than half of participants being discontinued from medications during the intervention.18 In addition, participants also managed to maintain glycemic control, improve fitness, and reduce several cardiovascular risk factors.18 43 These improvements are potentially important in relation to mental health for several reasons. First, glucose-lowering mediation has been shown to interfere with normal life44 because it is associated with discomfort45 and decreased QoL.46 Second, depression is prevalent in persons with T2D,47 and lifestyle interventions have been shown to improve signs of depression in persons with T2D10 and the healthy population.48 49 Third, epidemiological evidence suggests that an increased level of physical activity and a healthier diet are associated with better mental health; however, the (causal) effect is likely being bidirectional.50 However, the failure of the U-TURN intervention to improve mental outcomes is in line with several previous studies that have demonstrated that lifestyle interventions positively influence physical HRQoL in persons with T2D but do not provide improvements in the mental component of HRQoL. In the Diabetes Aerobic and Resistance Exercise trial, a combined exercise group did not show improvements in physical HRQoL compared with controls. The mental HRQoL was not significantly altered; however, due to deterioration in the controls the between-group difference was significant.51 Also, in the Health Benefits of Aerobic and Resistance Training in Individuals with Type 2 Diabetes study, a randomized 9-month exercise intervention with a control and three different exercise groups (aerobic, resistance and aerobic plus resistance training), it was reported that every intervention group demonstrated greater improvements in physical HRQoL compared with controls, but that the changes in mental HRQoL did not differ significantly between any of the intervention groups and controls at 9-month follow-up.52
The longest running study to date, the Look AHEAD study, evaluated the effect of a lifestyle intervention including healthy eating and physical activity aimed at achieving weight loss. During the 8-year follow-up period, physical HRQoL declined in the intervention group as well as in the control group. However, the decline was significantly greater in controls who received standard care.10 These results align with our findings. In our study, the between-group difference in the PCS was partly due to the decline in the PCS in the standard care group, contrasting with the positive change observed in the intervention group. In support of our results, the Look AHEAD study did not find significant differences between the groups in mental HRQoL at any time during the 8-year follow-up period.10 The IDES study demonstrated that higher levels of exercise volume increased physical HRQoL; however, the levels of physical activity had to exceed current recommended levels to reach significance.14 In contrast to our results as well as previous studies, the IDES study also showed an improvement in mental HRQoL at every level of physical activity in the intervention group after 12 months of intervention.14 This discrepancy could be explained by the fact that the IDES study included participants treated with insulin, and persons with a longer average duration of disease, both of which are indicative of more severe disease states. Both factors have been associated with worse HRQoL.53 In addition, the baseline levels of mental HRQoL in the IDES study are the lowest of all the studies discussed thus far, and these low baseline scores could explain why the IDES study found improvements in the mental HRQoL, while other studies did not. In other words, the low baseline scores could offer greater room for improvement. In contrast, our study participants had relatively high baseline mental HRQoL scores, the highest among studies discussed here. This difference may reflect a healthier volunteer bias, which would result in the inclusion of a selected subgroup of persons with good mental health at baseline. Although this possible explanation is speculative, the U-TURN intervention was intensive and required participants to allocate significant amounts of time and effort to the program. In addition, participants in the present study had relatively well-regulated glycemic control at baseline and had no severe diabetes-related complications known to be associated with a strong negative impact on HRQoL.54 55 Interestingly, while T2D has been associated with lower levels of HRQoL compared with the background population,56 57 persons without macrovascular complications appear to have an HRQoL that is relatively unaffected by the disease, and even persons with macrovascular complications appear to experience only small decreases in HRQoL.54 Another explanation for why mental health did not improve in this study could be that the intensive nature of the intervention blunted potential positive effects on mental health, as the efforts required to comply with the intervention may have resulted in a reduction in the mental HRQoL. The real-world acceptance and adherence to the intensive exercise program may differ across countries, as, for example, in Denmark, 29% are not adherent to the recommendations for physical activity for health compared with 37% in other high-income Western countries.58 However, since our results align with similar studies discussed here that prescribed lower levels of exercise and less intensive interventions, it is unlikely that the intensive training level obscured an otherwise positive effect on mental HRQoL.
Although speculative, it is possible that lifestyle interventions, in particular increased levels of physical activity and exercise, are effective in improving low affective states, but as our study and the other high-quality studies discussed here show, mental HRQoL and SWB may be relatively resistant to improvement in persons with T2D without major diabetes-related complications or depression.
In healthy populations, lifestyle interventions have demonstrated no or only modest effects on HRQoL.48 59 It can be hypothesized that unless an individual is starting with suboptimal mental health, mental health improvements are difficult to achieve due to ceiling effects. This hypothesis is supported by the theory that SWB is under the control of a homeostatic-like mechanism, fitness,60 that is resistant to long-term changes both in a positive and negative direction.61 SWB is characterized by two unique features: it has a natural positive offset and is highly stable over time.60 It has been proposed that individuals have a set-point range for SWB that is maintained through a psychological homeostasis system that draws on internal and external factors to maintain a stable level of SWB when challenges arise and overtime.60 This theory implies that in the absence of pathologies such as depression, long-term positive effects of lifestyle interventions on mental health are likely going to be absent.
There are some limitations to our study. First, the measurement instruments used to assess mental health are generic, and these scales may not be sensitive enough to detect and quantify small changes that are important to persons with T2D or subjective changes specifically related to exercise behavior. Second, exploring mental health was not the primary outcome of the U-TURN study and all findings have explorative character. Furthermore, participants in the present study had high baseline HRQoL which may have limited our ability to measure improvements in mental health. Third, the sample size might be underpowered to detect lower effect sizes. Fourth, the diversity in our trial population is limited, so further research should confirm our findings in populations of other ethnicities and/or socioeconomic backgrounds. Finally, due to the medical titration before baseline, participants were well controlled, making generalizability to less well-regulated persons questionable.
Conclusion
In persons with T2D diagnosed for less than 10 years without significant diabetes-related complications, lifestyle intervention including high volumes of exercise leads to modest improvement of physical HRQoL compared with standard care whereas effects on mental health were limited. Even with high volumes of exercise, significant reductions in the need for diabetes medications, increased fitness, and reduced cardiovascular risk factors appear to be unable to mediate this phenomenon. Because this is an explorative study, further studies specifically designed to investigate whether and how a lifestyle intervention can improve HRQoL are needed to infer causality.
Acknowledgments
The authors thank all the patients for their participation in the study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors CSM is the main author of the paper and contributed to the design of the study, the analysis and interpretation of data, and the drafting and revision of the manuscript. SMN performed the statistical analysis in R and contributed to interpretation of data and writing of the manuscript. MYJ and RC contributed to the design of the study, interpretation of data, and writing of the manuscript. MRL is the principal investigator of the U-TURN study and contributed to the conception and design of the study, the interpretation of data, and writing of the manuscript. RC, JM, JB, HL, AV, DEL, and BKP contributed to the conception and design of the study and gave final approval of the published version of the manuscript. CSM is the guarantor of this work and as such had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Funding This project was funded by TrygFonden. The Centre for Physical Activity Research (CFAS) is supported by a grant from TrygFonden. The Centre for Inflammation and Metabolism/CFAS is a member of the Danish Center for Strategic Research in Type 2 Diabetes (the Danish Council for Strategic Research, grants 09-067009 and 09-075724). The Contour Next glucose monitors were provided by Bayer, Copenhagen, Denmark. This work was also supported by a grant from the Danish Diabetes Academy, which is supported by the Novo Nordisk Foundation (MRL). In addition, MYJ received funding from Rigshospitalet. RC and SMN's employer, the Parker Institute, Bispebjerg and Frederiksberg Hospital, is supported by core grant (OCAY-18-774-OFIL) from the Oak Foundation.
Disclaimer The funders had no role in design and conduct of the study; collection, analysis, and interpretation of data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Competing interests AV was appointed vice-president for AstraZeneca’s Translational Research and Early Clinical Development during the completion of the study, but remained in the scientific steering committee of this study. RC and SMN’s employer, the Parker Institute, Bispebjerg and Frederiksberg Hospital, is supported by core grant OCAY-13-309 from the Oak Foundation. RC reports receiving personal fees from Abbott, AbbVie, Amgen, Axellus, Bayer HealthCare Pharmaceuticals, Biogen Idec, Bristol-Myers Squibb, Cambridge Weight Plan, Celgene, Eli Lilly, Hospira, Ipsen, Janssen, Laboratoires Expanscience, and Merck Sharp; personal fees from employment from Research Unit for Musculoskeletal Function and Physiotherapy, Institute of Sports Science and Clinical Biomechanics, and the University of Southern Denmark; grants pending and grant funding from Axellus, AbbVie, Cambridge Weight Plan, Janssen, and Merck Sharp; and being involved in many healthcare initiatives and research that could benefit from wide uptake of this publication, including Cochrane, Outcome Measures in Rheumatology, International Dermatology Outcome Measures, RADS, and the Grading of Recommendations Assessment, Development and Evaluation Working Group. MRL received personal speaker fees from Novo Nordisk.
Patient consent for publication Not required.
Ethics approval Guidelines from the Helsinki Declaration were followed and the study was approved by the Scientific Ethical Committee at the Capital Region of Denmark. All participants provided oral and written informed consent.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. Proposals should be directed to MRL (mathias.ried-larsen@regionh.dk). To gain access, data requestors will need to sign a data access agreement.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.