Article Text

Abstract
Introduction Peptide markers of inflammation have been associated with the development of type 2 diabetes. The role of upstream, lipid-derived mediators of inflammation such as eicosanoids, remains less clear. The aim of this study was to examine whether eicosanoids are associated with incident type 2 diabetes.
Research design & methods In the FINRISK (Finnish Cardiovascular Risk Study) 2002 study, a population-based sample of Finnish men and women aged 25–74 years, we used directed, non-targeted liquid chromatography-mass spectrometry to identify 545 eicosanoids and related oxylipins in the participants’ plasma samples (n=8292). We used multivariable-adjusted Cox regression to examine associations between eicosanoids and incident type 2 diabetes. The significant independent findings were replicated in the Framingham Heart Study (FHS, n=2886) and DIetary, Lifestyle and Genetic determinants of Obesity and Metabolic syndrome (DILGOM) 2007 (n=3905). Together, these three cohorts had 1070 cases of incident type 2 diabetes.
Results In the FINRISK 2002 cohort, 76 eicosanoids were associated individually with incident type 2 diabetes. We identified three eicosanoids independently associated with incident type 2 diabetes using stepwise Cox regression with forward selection and a Bonferroni-corrected inclusion threshold. A three-eicosanoid risk score produced an HR of 1.56 (95% CI 1.41 to 1.72) per 1 SD increment for risk of incident diabetes. The HR for comparing the top quartile with the lowest was 2.80 (95% CI 2.53 to 3.07). In the replication analyses, the three-eicosanoid risk score was significant in FHS (HR 1.24 (95% CI 1.10 to 1.39, p<0.001)) and directionally consistent in DILGOM (HR 1.12 (95% CI 0.99 to 1.27, p=0.07)). Meta-analysis of the three cohorts yielded a pooled HR of 1.31 (95% CI 1.05 to 1.56).
Conclusions Plasma eicosanoid profiles predict incident type 2 diabetes and the clearest signals replicate in three independent cohorts. Our findings give new information on the biology underlying type 2 diabetes and suggest opportunities for early identification of people at risk.
- eicosanoids
- inflammation
- diabetes mellitus, type 2
- epidemiology
Data availability statement
Data are available on reasonable request. The FINRISK and DILGOM data used in this article are available from the THL Biobank, based on a written application and relevant Finnish legislation as described on the website of the Biobank https://thl-biobank.elixir-finland.org/.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Type 2 diabetes is a complex disease involving interactions of both environmental risk factors and genetics, and, at an undetermined scale, of inflammation.
Biomarkers of systemic inflammation, such as cytokines, adiponectin and high-sensitivity C reactive protein, have been associated with the development of type 2 diabetes.
Eicosanoids mediate inflammatory processes directly at local level as well as systemically, including through modulation of cytokines and other inflammatory mediators but their role in the development of diabetes is not known.
A recent cross-sectional analysis found several eicosanoids associated with blood pressure traits.
What are the new findings?
Altogether 76 eicosanoid metabolites were associated with incident diabetes in our discovery cohort, FINRISK 2002, independent of traditional risk factors of type 2 diabetes.
These eicosanoids were correlated with each other but three eicosanoids representing independent signals were identified.
An eicosanoid risk score, constructed of the three independent eicosanoids, was associated with incident diabetes risk in two replication cohorts as well as in the meta-analysis of all three cohorts.
One of the eicosanoids associated with incident type 2 diabetes in the present study was also associated with blood pressure in our earlier study.
How might these results change the focus of research or clinical practice?
A targeted analysis of eicosanoids may help to identify individuals at elevated risk of diabetes.
Further research on eicosanoids may uncover novel therapeutic targets for the prevention and treatment of diabetes and reveal new links between diabetes and elevated blood pressure.
Introduction
Diabetes and its complications contribute significantly to the global burden of disease: in 2017, it was the third leading cause of global years lost due to disability for men and the fifth for women.1 It is estimated that its global costs (US$1.3 trillion in 2015) will continue to rise by 2030, even if Sustainable Development Goals related to the disease are met.2
The prevention of complications, such as cardiovascular disease, diabetic nephropathy, neuropathy and retinopathy, lie at the heart of diabetes care. However, clinical trials have shown that the onset of type 2 diabetes can be postponed, and even prevented, by lifestyle changes, such as changes in the intake of fats and fibers, and increasing physical activity, and medical treatment, such as metformin medication.3 4 Therefore, better understanding of factors involved in the development of type 2 diabetes, together with earlier identification of people at risk, are important for optimal targeting of right preventive measures to right people.
Type 2 diabetes is a complex disease involving interactions of both environmental risk factors and genetics, and, at an undetermined scale, of inflammation. Type 2 diabetes is closely linked to cardiovascular and kidney diseases, obesity and metabolic syndrome, all of which are known to be associated with low-grade inflammation. Biomarkers of systemic inflammation, such as cytokines, adiponectin and high-sensitivity C reactive protein (hs-CRP), have been associated with the development of type 2 diabetes in large population-based studies and randomized controlled trials.5–9
Situated proximally (upstream) in the inflammation pathways is a large group of bioactive lipids known as eicosanoids and related oxylipins. These chemical factors are derived from arachidonic acid and other polyunsaturated fatty acids by enzymatic mechanisms, notably via cyclooxygenase (COX), lipoxygenase (LOX) and cytochrome P450 enzymes, as well as by non-enzymatic mechanisms. Eicosanoids mediate inflammatory processes directly at local level as well as systemically, including through modulation of cytokines and other inflammatory mediators.10 With recent advances in mass spectrometry-based metabolomics, hundreds of eicosanoid and oxylipin species can now be detected and quantified in human plasma.11 12
The aim of this study was to examine whether plasma eicosanoid profiles are associated with risk of incident type 2 diabetes in a prospective follow-up of a population-based Finnish cohort. The significant independent signals were replicated using multivariate models in two other cohorts. Together, these cohorts included 1070 cases of incident type 2 diabetes. A secondary aim was to investigate whether the eicosanoid effect is mediated by inflammation or insulin resistance.
Methods
Population, data collection and design
FINRISK 2002
FINRISK (Finnish Cardiovascular Risk Study) 2002 study is a population-based random sample of individuals aged 25–74 years living in Finland (n=8798, participation rate 65.2%). Sampling included stratification by sex, region and 10-year age groups. Participants responded to questionnaires, underwent physical examination by trained nurses and gave blood samples. Detailed study protocols have been previously described.13 Plasma samples from 8292 participants were successfully analyzed with directed non-targeted liquid chromatography-mass spectrometry (LC-MS), as described in previous publications.11 12 In addition, an oral glucose tolerance test (OGTT) was carried out in 3767 participants (45 years of age and older) and data on glucose tolerance status were obtained for 3092 participants without prior history of diabetes. A panel of cytokines was quantified from blood samples of 2951 participants.
For the FINRISK 2002 cohort, prevalent diabetes cases at baseline and incident cases during follow-up were identified combining information from the National Hospital Discharge Register (NHDR), Causes of Death Register (CDR) and the Drug Reimbursement and Drug Purchase Registers (DPR), using the Finnish personal identification number, up to December 31, 2017. Diagnostic codes for extracting information from NHDR and CDR were E10-E14 (International Classification of Diseases (ICD)-10) or 250*B (ICD-9). Diabetes medication purchase ATC code A10 or a special reimbursement code for diabetes medications were used for identifying diabetes cases from the drug purchase register. If medicine purchase was the only fulfilled criterion, ≥3 purchases were required, and diagnosis codes were used to exclude gestational diabetes. To determine the type of diabetes, we used a proxy variable: all participants under 30 years of age and treated with insulin only, or in combination with metformin, and those aged 30–40 years when insulin only was started, were categorized as type 1 diabetes. All other persons with diabetes were considered to have type 2 diabetes. Thanks to the country-wide electronic healthcare registers, the follow-up was virtually 100% complete.
Participants with prevalent or incident type 1 diabetes were excluded from the analysis (n=79). Record linkages based on the personal identification code to NHDR, CDR and DPR were also used to identify subjects to be excluded from the analysis, due to cancer (excluding ICD-10 category C44, n=1085). Participants pregnant at baseline (n=44) were also excluded from the final analyses. Finally, after excluding further participants with missing values of variables relevant for our analyses, the total study population consisted of 6548 participants. Online supplemental figure 1 presents a flow chart formulating the final study sample.
Supplemental material
Framingham Heart Study Offspring
Framingham Heart Study (FHS) Offspring study is a cohort of 5124 participants that were first examined in 1971 and consecutively re-examined every 4–8 years. The cohort consists of the children of the FHS first-generation cohort, and their spouses. Participants of the original cohort were enrolled in a longitudinal community-based cohort study in 1948, including a random sample of two-thirds of the adult population of Framingham, Massachusetts, USA. Detailed study protocols have been previously published.14 For this study, we considered individuals who participated in the eighth examination cycle of FHS Offspring in 2005–2008 and whose samples were successfully analyzed with LC-MS (n=2886). After excluding 771 participants with diabetes at baseline or missing covariates, we included n=2115 participants as the replication cohort. Diabetes mellitus in FHS Offspring cohort was diagnosed either by fasting plasma glucose ≥126 mg/dL (7.0 mmol/L), non-fasting plasma glucose ≥200 mg/dL (11.0 mmol/L) or treatment with insulin or an oral hypoglycemic agent as ascertained at routine FHS examinations or based on annual medical health history updates.
DILGOM 2007
The DIetary, Lifestyle and Genetic determinants of Obesity and Metabolic syndrome (DILGOM) study is an extension of the FINRISK 2007 survey, which included a random population-based sample of individuals aged 25–75 years living in Finland. All participants of the FINRISK 2007 survey were invited to take part in the more focused DILGOM study and 5024 participated (participation rate 80%).
Participants responded to self-administered questionnaires, underwent a physical examination by trained nurses and gave blood samples. Detailed study protocols have been previously described.15 Plasma samples from n=4903 participants were successfully analyzed with LC-MS. Cases of diabetes were identified and information from registries combined in an identical way to the FINRISK 2002 cohort, as described above. Similarly, participants with prevalent type 1 diabetes, pregnancy, cancers (excluding ICD-10-C44) and missing values were excluded from the final replication cohort. Finally, 3905 individuals were included in the analyses.
Laboratory methods and plasma eicosanoid profiling
Plasma eicosanoid profiling for all three cohorts was carried out in the same laboratory at the University of California San Diego, USA. The profiling methodology is described in more detail elsewhere.11 12 In short, we used directed, non-targeted LC-MS combined with computational chemical networking to identify eicosanoids in participants’ plasma samples. In the discovery sample, FINRISK 2002, a total of 545 eicosanoids and related oxylipins were validated using methodologies such as spectral fragmentation pattern networking and manual annotation.
The OGTT was carried out according to WHO recommendations, and the testing and measurement methodologies have previously been described in detail.16 Fasting plasma glucose and insulin concentrations were used to calculate the homeostasis model assessment for insulin resistance (HOMA-IR) and for beta-cell function (HOMA-B) indices.17
We quantified well-known inflammatory markers often hypothesized to associate with diabetes. hs-CRP was quantified with the Architect ci8200 Chemistry Analyser (Abbott Laboratories, USA) from FINRISK 2002 serum samples and with Architect c8000 analyzer (Abbott Laboratories, USA) from DILGOM 2007 serum samples, using an immunoturbidimetric method (Sentinel Diagnostics, Italy). Interleukin-1 receptor antagonist (IL-1Ra), interleukin-6 (IL-6) and tumor necrosis factor alpha (TNF-α) were quantified from previously unthawed heparin plasma samples using Bio-Rad’s premixed Bio-Plex Pro Human Cytokine 27-plex Assay and 21-plex Assay, and Bio-Plex 200 reader with Bio-Plex V.6.0 software (Bio-Rad Laboratories, USA). The detailed methodology has been previously published.18 19
Statistical methods
The eicosanoid profiling data were normalized using plate medians corrected for plate deviation: plate medians were subtracted from each feature and then divided by the median absolute deviation.20
We used means, or where relevant due to skewed distributions, geometrical means and IQRs to summarize baseline characteristics of continuous variables and frequencies for categorical variables. For subsequent analyses, participants with prevalent type 2 diabetes (n=167) were excluded from the FINRISK study population resulting in n=6381 (with n=586 of incident type 2 diabetes cases).
To test the association of eicosanoids with incident type 2 diabetes in our discovery cohort FINRISK 2002, we used Cox proportional hazards regression and a nested modeling approach, adjusting for well-established risk factors for type 2 diabetes, and other confounding factors, in three different models. The first model adjusted for age, sex, region of residence and mass spectrometry plate. The second model (model 2) added adjustments for body mass index (BMI), physical activity, parental history of diabetes, prevalent cardiovascular disease (CVD), systolic blood pressure, antihypertensive medication, triglycerides and lipid-lowering medication. We also ran a third model that was further adjusted for hs-CRP. Furthermore, we ran the sensitivity analyses where BMI was replaced with waist-to-hip ratio or waist circumference and also a model where persons with prevalent CVD at baseline were excluded from the analysis. The proportional hazards assumption was tested using Schoenfeld residuals.21 We used the false discovery rate (FDR) correction method for type I error control in multiple comparisons.22 We also produced a correlation heatmap for eicosanoids significantly associated with incident type 2 diabetes, ordered using the complete linkage clustering method. Correlations with hs-CRP were also added to the heatmap.
Eicosanoids with significant associations in any of the three longitudinal analysis models (described above) were then included in a stepwise Cox regression analysis with forward selection, applying a Bonferroni-corrected inclusion threshold of p<0.05/545=0.00009.23 We constructed an eicosanoid risk score for the three remaining eicosanoids using their respective regression coefficients as weights in the prediction model.
We examined type 2 diabetes-free survival across quartiles of the risk score using Cox models and Kaplan-Meier survival curves. We compared survival distributions using the log rank test.24 Using Cox regression, we calculated the risk per SD change in the eicosanoid risk score for the different models.
We calculated medians of fP-Glucose (fP-Gluc), fP-Insulin (fP-Ins), HOMA-IR and HOMA-B for the eicosanoid score quartiles and tested the linear trends across the quartiles adjusting for age, sex and BMI. We explored the correlations between fP-Gluc, fP-Ins, HOMA-IR, HOMA-B and three eicosanoids from the risk score using Spearman’s correlation. Correlations were also calculated between a panel of cytokines, namely IL-1Ra, IL-6, TNF-α and the same three eicosanoids.
Replication analyses for the three eicosanoids exceeding the Bonferroni-corrected inclusion threshold (p<0.05/545=0.00009) in FINRISK were performed in the FHS Offspring cohort with Cox regression adjusted for age, sex, BMI, systolic blood pressure, hypertension treatment and triglycerides. Participants with baseline diabetes (n=302) and missing values in the covariates were excluded from the analysis, resulting in n=236 incident diabetes cases out of a total of 2115 individuals included.
In the DILGOM 2007 cohort, we excluded participants with prevalent type 2 diabetes (n=144), and thus 3761 individuals (out of which n=248 with incident type 2 diabetes) were included in the replication analysis. The analysis was performed for the three eicosanoids with Cox regression adjusting for the same covariates as in the FINRISK cohort.
Meta-analysis of the risk scores in the three cohorts was performed using a random-effects model (metafor package in R). We used R, V.3.6.1, for all analyses and the source code for analyses is available at https://doiorg/105281/zenodo3968712.
Results
Baseline characteristics of the FINRISK 2002, DILGOM 2007 and FHS Offspring cohort participants (women and men) are presented in table 1. Hemoglobin A1c (HbA1c) values were only available for FINRISK participants older than 50 years (n=3586).
Baseline characteristics of FINRISK 2002 discovery cohort (n=6548) and FHS Offspring (n=2886) and DILGOM 2007 (n=3905) replication cohorts
Longitudinal analyses: independent eicosanoids
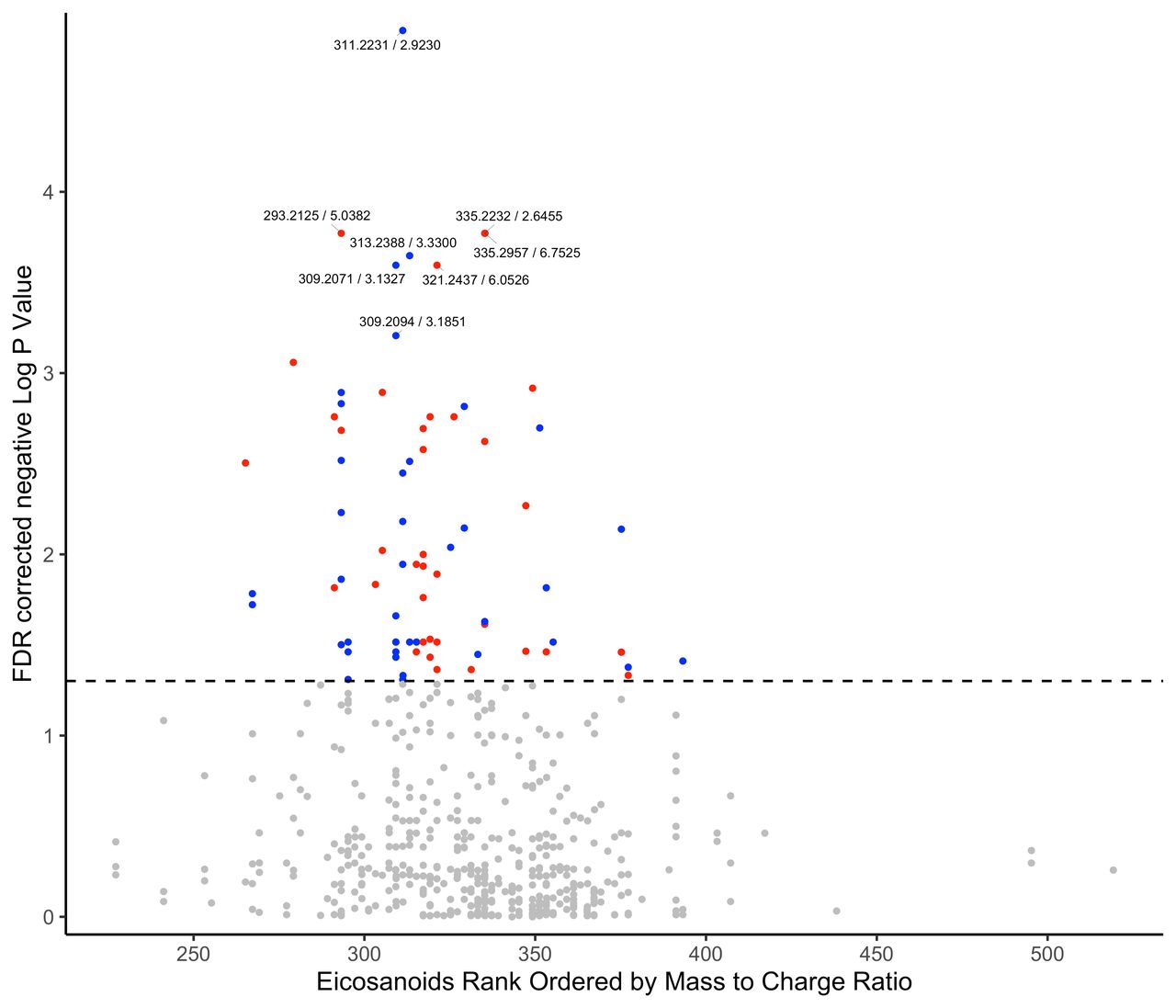
When we tested eicosanoids one by one in the FINRISK 2002 cohort using the multivariate models described in the ‘Methods’ section, we observed altogether 76 significant associations between eicosanoids and incident type 2 diabetes. Eicosanoids, their FDR-corrected levels of significance and the direction of the association with type 2 diabetes, are visualized in figure 1. The heatmap of pairwise correlations for the 76 eicosanoids with significant associations, and hs-CRP, is shown in online supplemental figure 2. Overall, the eicosanoids correlated with each other, with some clusters of strong positive correlations.
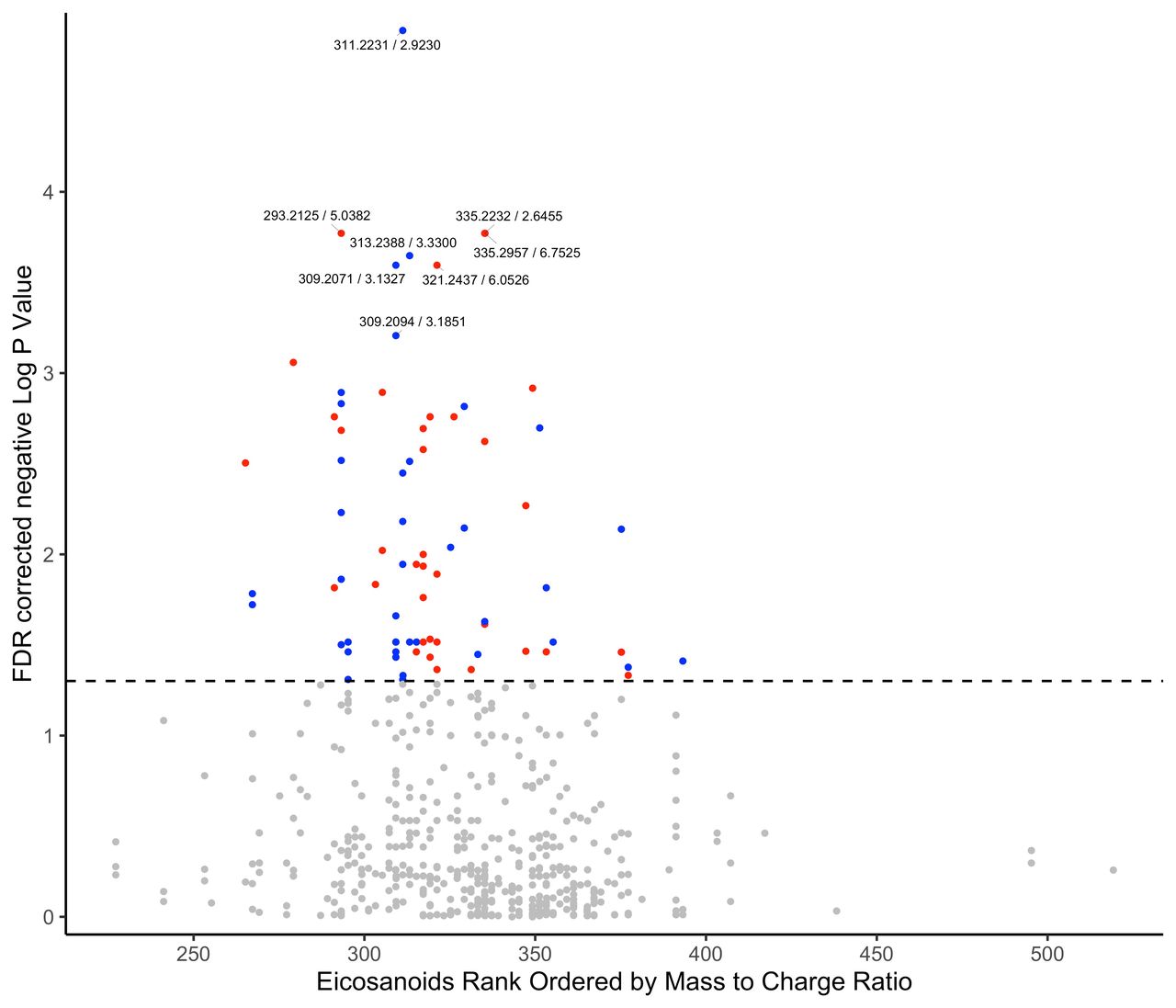
Associations between eicosanoids and incident type 2 diabetes in FINRISK 2002. A statistically significant association was found for 76 eicosanoids and incident type 2 diabetes: red is for positive associations, blue is for negative associations and grey is for non-significant associations. Dashed line represents the false discovery rate (FDR)-corrected level of significance. Eicosanoids analysed one by one, adjusted for age, sex, body mass index, physical activity, parental history of diabetes, prevalent cardiovascular disease, systolic blood pressure, antihypertensive medication, triglycerides, lipid-lowering medication, geographical area and mass spectrometry plate.
We included 76 eicosanoids that showed significant associations with incident type 2 diabetes in the stepwise Cox regression analysis using model 2. Three eicosanoids remained in the model, notably an unknown eicosanoid (EIC 62), 8-iso-prostaglandin A1 (8-iso-PGA1) and 12-hydroxy-5,8,10-heptadecatrienoic acid (12-HHTrE). The forest plot (figure 2) presents HRs and 95% CIs for the individual eicosanoids remaining in the model. The unknown eicosanoid was inversely associated with incident type 2 diabetes, whereas 8-iso-PGA1 and 12-HHTrE were positively associated with the disease risk. Neither these HRs nor their statistical significances changed substantially in the sensitivity analyses where BMI was replaced with indicators of central obesity, that is, waist-to-hip ratio or waist circumference, or in the analyses where persons with prevalent CVD at baseline were excluded.
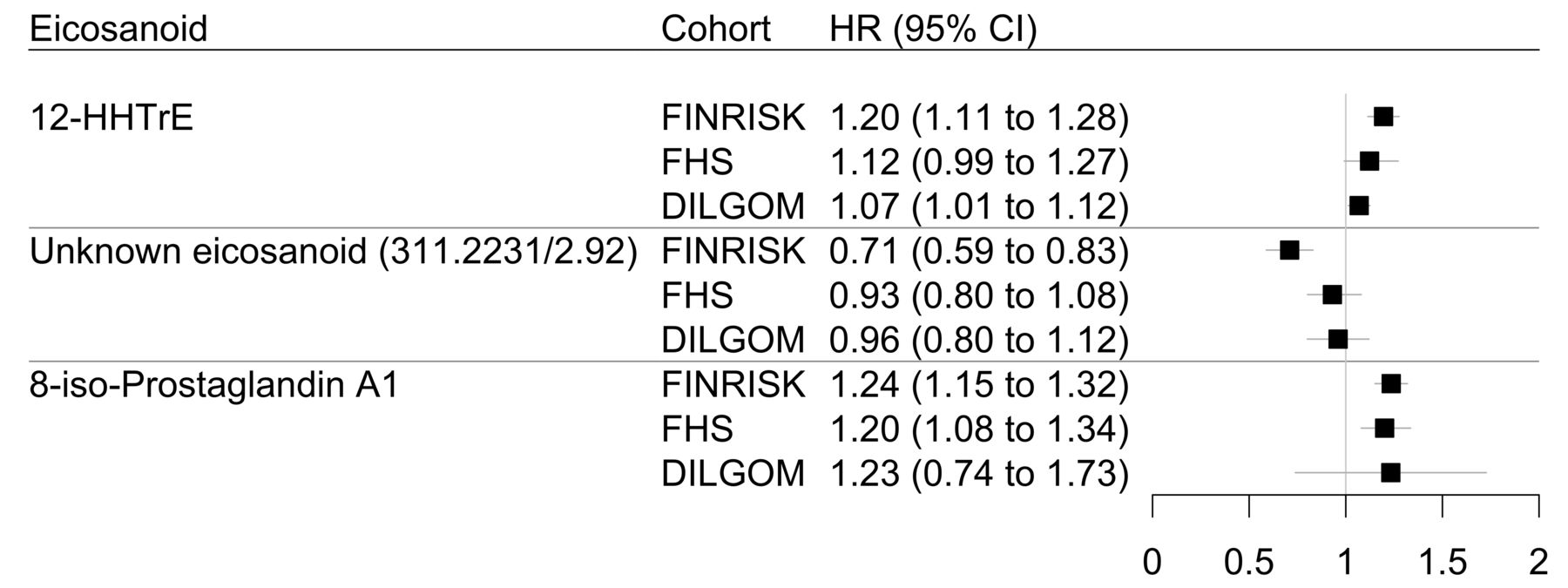
Forest plot showing HRs and 95% CIs for three eicosanoids independently associated with incident type 2 diabetes. Each eicosanoid was analysed separately. Cox proportional hazards regression analyses for the FINRISK and DILGOM cohorts are adjusted for age, sex, body mass index (BMI), physical activity, parental history of diabetes, prevalent cardiovascular disease, systolic blood pressure, antihypertensive medication, triglycerides, lipid-lowering medication, geographical area and mass spectrometry plate. For the Framingham Heart Study (FHS) cohort, Cox proportional hazards regression analyses are adjusted for age, sex, BMI, systolic blood pressure, hypertension treatment and triglycerides. DILGOM, DIetary, Lifestyle and Genetic determinants of Obesity and Metabolic syndrome; 12-HHTrE, 12-hydroxy-5,8,10-heptadecatrienoic acid; 8-iso-PGA1, 8-iso-prostaglandin A1.
Cox regression on the three eicosanoids was performed in the replication cohorts (figure 2). The eicosanoid 8-iso-PGA1 was replicated in FHS (p<0.001) and 12-HHTrE in DILGOM (p=0.025) cohort, and the other two were directionally consistent.
Longitudinal analyses: eicosanoid risk score
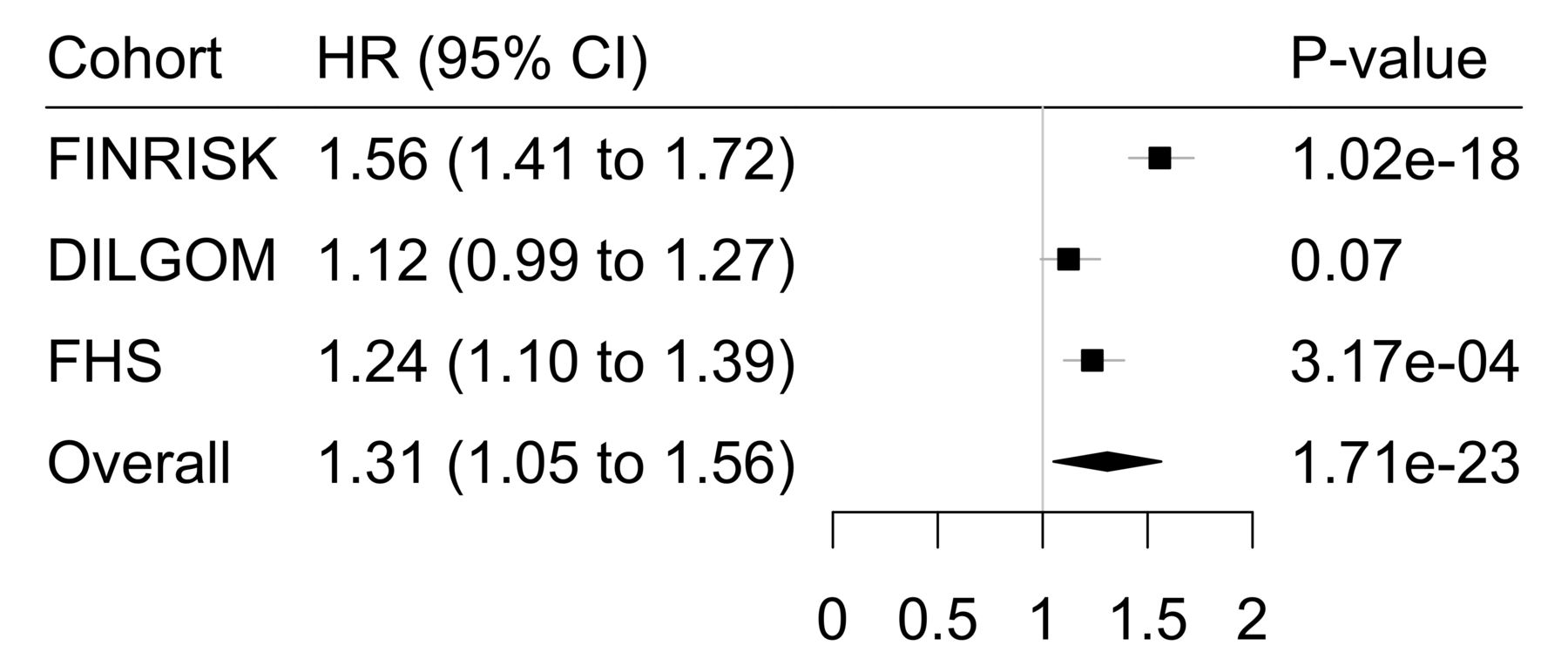
Using these three eicosanoids, we established an eicosanoid risk score. Results are presented for women and men combined as testing revealed no interaction with sex and the eicosanoid risk score. The multivariate adjusted HRs per SD for the three different cohorts are presented in figure 3, together with the random-effects meta-analysis, which gave a pooled HR of 1.31 (95% CI 1.05 to 1.56, p<001).
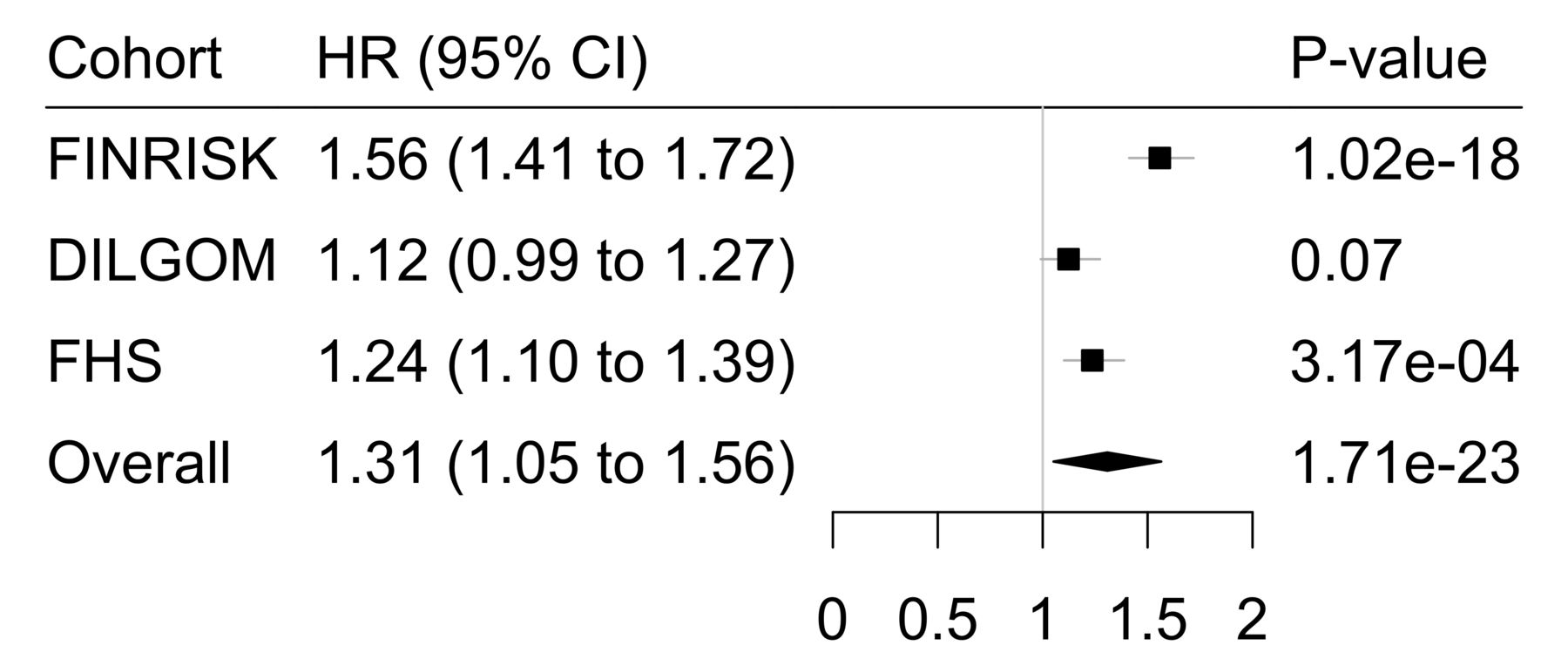
Forest plot showing HRs and 95% CIs for the eicosanoid risk score and its independent association with incident type 2 diabetes in the FINRISK cohort, FHS and DILGOM replication cohorts and their meta-analysis. Cox proportional hazards regression analyses for the FINRISK and DILGOM cohorts are adjusted for age, sex, body mass index (BMI), physical activity, parental history of diabetes, prevalent cardiovascular disease, systolic blood pressure, antihypertensive medication, triglycerides, lipid-lowering medication, geographical area and mass spectrometry plate. For the FHS cohort, Cox proportional hazards regression analyses are adjusted for age, sex, BMI, systolic blood pressure, hypertension treatment and triglycerides. Meta-analysis was calculated using the random-effects model. DILGOM, DIetary, Lifestyle and Genetic determinants of Obesity and Metabolic syndrome; FHS, Framingham Heart Study.
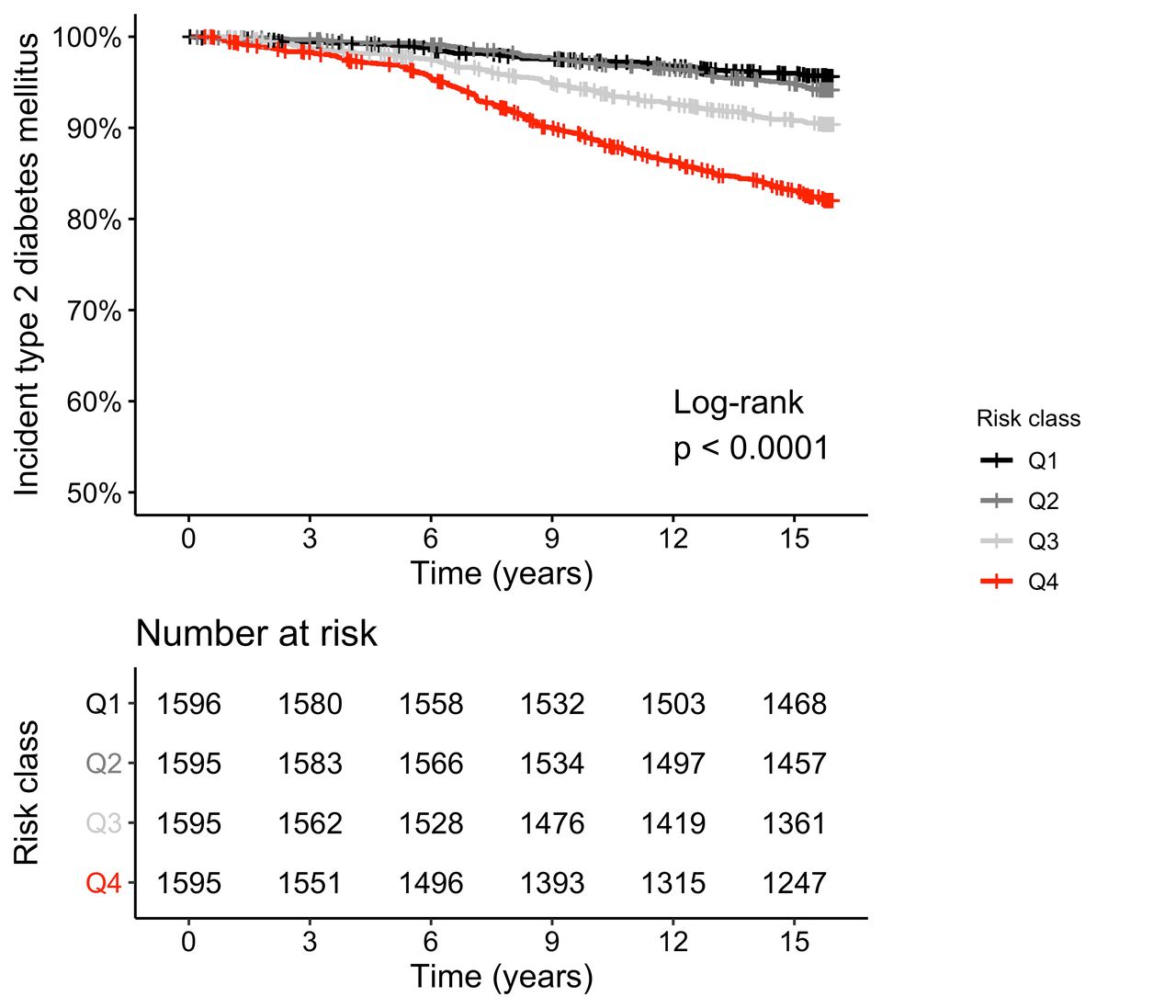
In the top risk score quartile of participants, compared with the lowest quartile, the HR was 2.80 (95% CI 2.53 to 3.07) in FINRISK, 1.74 (95% CI 1.31 to 2.31) in FHS and 1.37 (95% CI 1.00 to 1.74) in DILGOM (online supplemental table 1). The respective HRs for quartiles 2 and 3 demonstrated a dose-response type relationship of the eicosanoid score with the risk of incident type 2 diabetes in all three cohorts. Furthermore, Kaplan-Meier curves for the risk score quartiles in FINRISK are presented in figure 4. Disease-free survival in the lowest quartile was 95.7% and 82.6% in the top quartile.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier curves for the three-eicosanoid risk score and incident type 2 diabetes in FINRISK 2002. Diabetes-free survival analysis for the different risk classes/quartiles (Q1–Q4). Analyses adjusted for age, sex, body mass index, physical activity, parental history of diabetes, prevalent cardiovascular disease, systolic blood pressure, antihypertensive medication, triglycerides, lipid-lowering medication, geographical area and mass spectrometry plate.
Eicosanoid associations with glucose and insulin levels and commonly known cytokines
The medians of fP-Gluc, fP-Ins, HbA1c and HOMA-IR increased across the eicosanoid risk score quartiles, and the increasing trend remained statistically significant (p<0.0001) after adjusting the analyses for age, sex and BMI. For HOMA-B, the increase was less significant (p=0.014) (online supplemental table 2).
The eicosanoid identified as 12-HHTrE was quite strongly correlated with fP-Gluc, fP-Ins, HbA1c, HOMA-IR, HOMA-B and hs-CRP (online supplemental table 3). The other eicosanoids showed some statistically significant correlations with these glucose metabolism indicators but the magnitudes of the correlation coefficients were modest.
None of the three eicosanoids correlated with the blood concentrations of inflammatory cytokines. In addition, Cox proportional hazards regression analysis for the multivariable model, further adjusted for the inflammatory cytokines, remained significant for both the continuous three-eicosanoid risk score as well as the third and fourth risk quartiles of the score.
Discussion
Downstream mediators of inflammation such as CRP and other peptide mediators of inflammation such as cytokines, have received a lot of attention in the study of the development of type 2 diabetes.25 Previous studies have pointed to adiponectin, apolipoprotein B, CRP, IL1-Ra and ferritin playing a role in type 2 diabetes prediction.6 7 The Whitehall II study examining MR/CRP haplotypes suggested non-causal associations between CRP, insulin resistance, glycemia and diabetes, and that upstream effectors of inflammation may play a more causal role in the development of diabetes.26
Combined with advanced metabolomics methodologies, our statistically cogent survival analysis using a three-eicosanoid risk score suggests a significant independent role for lipid-derived, upstream mediators of inflammation in the prediction of incident type 2 diabetes. One of the three eicosanoids showed an independent inverse association with incident type 2 diabetes, suggesting potential protective characteristics for some plasma eicosanoids. However, this negative association was not statistically significant in the replication cohorts.
In 2011, Luo and Wang examined the role of eicosanoids from the different arachidonic acid metabolism pathways in pathogenesis of diabetes: they proposed that eicosanoids metabolized by the COX pathway are active participants in the function of beta-cells, those metabolized by the LOX pathway act as mediators in the beta-cell inflammation whereas the role of eicosanoids metabolized via the cytochrome P450 enzymes was still unclear.27 More recently, metabolites have been suggested to act as regulators of insulin sensitivity and further hypothesized to play a role in the pathogenesis of insulin resistance and type 2 diabetes.28
Out of the individual eicosanoids identified for our three-eicosanoid risk score, two are metabolites with known bioactivity. 8-iso-PGA1 is part of isoprostanes, which are stereoisomers of prostaglandins formed independent of COX enzymes, through peroxidation of arachidonic acid. They are considered as markers of oxidative stress, which may lead to chronic inflammation.29 30 Studies have suggested a causal role for isoprostanes in the development of different disease states, such as incident type 2 diabetes.30 31
Oxidative stress has also been implicated in the development of complications of diabetes such as nephropathy and neuropathy.32 33 A recent study found that individuals with heredity of type 2 diabetes have an increased susceptibility to oxidative stress and inflammation following a high carbohydrate meal.34
The second known eicosanoid demonstrating a positive independent association with incident type 2 diabetes is 12-HHTrE. Different enantiomers of 12-HHTrE are metabolites of non-enzymatic activity as well as of COX and LOX pathways, and they have been implicated in conditions such as breast cancer, hypertension, endothelial prostacyclin formation, response to acute exercise and high carbohydrate intake.35–38
A study using the same mass spectrometry platform recently found 12-HHTrE to be robustly associated with blood pressure.36 None of the eicosanoids associated with blood pressure were correlated with 8-iso-PGA1, however one of them (Tetranor-12(R)-HETE) strongly correlated with 12-HHTrE. Furthermore, the unknown eicosanoid from our risk score showed strong correlation with all but one of the eicosanoids associated with blood pressure.
The Cox regression models using the eicosanoid risk score replicated in the FHS cohort but did not quite reach statistical significance in DILGOM. However, a meta-analysis of the risk scores in the three cohorts produced a statistically significant result. These results support our hypothesis of an eicosanoid risk score predicting incident type 2 diabetes.
Pathogenetic mechanisms for the effects of these eicosanoids on the risk of incident type 2 diabetes are not known. 12-HHTrE was moderately associated with HOMA-IR and other indicators of insulin resistance, even after adjustment for age, sex and obesity. Interestingly, the eicosanoid 8-iso-PGA1 that replicated strongly in the FHS cohort did not correlate with glucose levels and only weakly with the insulin indicators.
Our study showed very little correlation between a panel of cytokines and the three eicosanoids significantly associated with type 2 diabetes. In addition, the Cox models further adjusted for cytokines in the FINRISK cohort, remained statistically significant both for the continuous eicosanoid risk score as well as the upper risk quartiles. This suggests that the peptide markers of inflammation, hs-CRP, IL-6, IL-1Ra and TNF-alpha, may not comprehensively reflect all aspects of subclinical inflammation that play a role in risk of type 2 diabetes and can be identified by using eicosanoids as more proximal markers of inflammatory activity. Alternatively, the eicosanoid score may increase the risk of type 2 diabetes through mechanisms other than traditional inflammatory pathways.
Recently, it has been suggested that inflammation should be targeted with novel therapeutics, as part of treatment and prevention of type 2 diabetes and its complications, especially because some antidiabetic agents have direct and secondary anti-inflammatory properties.39 40 Biological and pharmacological characteristics of upstream mediators of inflammation, such as of the two eicosanoids positively associated with incident type 2 diabetes (8-iso-PGA1 and 12-HHTrE), need to be further investigated in order to establish potential eicosanoid-targeting anti-inflammatory therapeutic measures.
Our study suggests potential windows of opportunity for intervention in terms of both prevention and treatment of type 2 diabetes. We speculate that 8-iso-PGA1 and 12-HHTrE could be used as personalized biomarkers in the identification of people at risk of developing type 2 diabetes. Interestingly, the latter metabolite was also associated with hypertension in our recent analysis.36 Better understanding of determinants and functions of these two eicosanoids may allow for a more targeted approach in the preventive measures such as lifestyle and medical interventions.3 4 These two eicosanoids, the three-eicosanoid risk score and their novel biomarker potential should be examined with closer detail in order to establish their roles in the early development of insulin resistance and type 2 diabetes.
Strengths and limitations
Our study is a large population-based random sample of adults aged 25–74 years with a high participation rate, prospective design and negligible loss to follow-up. Analyses were controlled for traditional risk factors for incident type 2 diabetes, other factors that may affect inflammation levels and hs-CRP. Versatile sensitivity analyses replacing BMI with indicators of central obesity or excluding persons with prevalent CVD at baseline confirmed the robustness of the findings. The partial replication of our results in FHS and DILGOM datasets further strengthens the study. 8-iso-PGA1 replicated robustly in the FHS cohort. The other two were directionally consistent but the lack of statistical significance may be due to the limited statistical power in both FHS and DILGOM. Also, the FHS participants were on average 20 years older than FINRISK participants, which may have had an effect on replication. The eicosanoid profiling for all three cohorts was done in the same laboratory with the same methods. We used a sophisticated, directed, non-targeted LC-MS combined with computational chemical networking to identify hundreds of known and putative eicosanoids from the majority of the study participants.
Our study design is observational which cannot establish causality. The study included mainly white participants of European ancestry and, therefore, the findings may not be generalizable to all ethnic groups. Limitations of our study include possible bias due to self-reported smoking status and the level of physical activity as well as lack of information on the use of over-the-counter drugs such as acetylsalicylic acid, non-steroidal anti-inflammatory analgesics and omega-3 fatty acids. Using family history of type 2 diabetes as our only consideration of genetic risk factors instead of, for example, a polygenic risk score, is a further limitation. In addition, we could only detect known and putative eicosanoids that circulate in human plasma. And finally, the identity of several eicosanoids, including one of the eicosanoids with a significant inverse association with our outcome, remains unknown.
Conclusions
Plasma eicosanoids are associated with incident type 2 diabetes and our three-eicosanoid risk score was an independent predictor of future type 2 diabetes in the general population. Of individual eicosanoids, 8-iso-PGA1 clearly replicated in two independent populations. Furthermore, 12-HHTrE which has been associated with hypertension earlier, predicted type 2 diabetes in the two Finnish cohorts and was close to statistical significance in FHS as well. Finally, our findings provide novel biological information on the development of type 2 diabetes suggesting opportunities for early identification of individuals at risk and potential therapeutic targets for more precise prevention and treatment of type 2 diabetes.
Data availability statement
Data are available on reasonable request. The FINRISK and DILGOM data used in this article are available from the THL Biobank, based on a written application and relevant Finnish legislation as described on the website of the Biobank https://thl-biobank.elixir-finland.org/.
Ethics statements
Patient consent for publication
Ethics approval
The FINRISK 2002 study was approved by the Ethical Committee for Epidemiology and Public Health of the Helsinki University Hospital District on December 19, 2001 (Ref 558/E3/2001). The DILGOM 2007 study was approved by the Coordinating Ethical Committee of the Helsinki and Uusimaa Hospital District on April 3, 2007 (Ref 229/E0/2006). The research protocols of the FHS are reviewed annually by the Institutional Review Board of the Boston University Medical Center. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We would like to thank the FINRISK 2002 cohort participants as well as participants in the FHS who have contributed to this research for decades.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
KT and JP are joint first authors.
Contributors KT, JP, VS, MJ, SC, TJN, PJ and ASH designed the study. JP and TL performed the statistical analyses and KT drafted the manuscript. JDW, KM, KAL, AA and MJ performed eicosanoid measurements. JT was responsible for the substudy where the oral glucose tolerance test was carried out and other measurements related to glucose metabolism were done. MS and SJ performed the cytokine analyses. All authors contributed to the revision of the manuscript with important intellectual content. VS is the guarantor of the study.
Funding This work was supported by Paavo Nurmi, Aarne Koskelo, Emil Aaltonen and Finnish Medical Foundations, and Academy of Finland (#141136 to MS and SJ; #321356 to ASH; #321351 to TJN; #46558 to JT). VS was supported by the Finnish Foundation for Cardiovascular Research. MJ and JDW were supported by grants from the US National Institutes of Health, including NIH S10OD020025 and R01ES027595 to MJ and K01DK116917 to JDW. This work was partially supported by the National Heart, Lung and Blood Institute’s Framingham Heart Study (contracts N01-HC-25195, HHSN268201500001I and 75N92019D00031). RSV is supported by an Evans Scholar award and Jay and Louis Coffman Foundation from the Department of Medicine, Boston University School of Medicine. The glucose tolerance testing in this work was supported by the grants to JT from Academy of Finland (grant 46558); the Social Insurance Institution of Finland; the Future Forum, Astra Zeneca and Eli Lilly Finland.
Competing interests VS has received honoraria for consulting from Novo Nordisk and Sanofi. He also has ongoing research collaboration with Bayer (all unrelated to the present study). JT has received research funding from Bayer and owns stocks of Orion Pharma and Aktivolabs. Other authors declare no conflicts of interest.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.