Article Text

Abstract
Introduction To determine the relative contributions of various amounts and intensities of exercise alone to a combined lifestyle intervention on health-related quality of life (HrQoL) measures.
Research design and methods Participants (n=162) were sedentary, overweight/obese, with pre-diabetes, and randomized to one of four 6-month interventions: (1) high amount/moderate intensity exercise–energy expenditure of 16 kcal/kg of body weight/week (KKW) at 50% oxygen consumption (V̇O2) reserve; (2) high/vigorous–16 KKW at 75% V̇O2 reserve; (3) low/moderate–10 KKW at 50% V̇O2 reserve; (4) low/moderate plus diet–10 KKW at 50% V̇O2 reserve plus a calorically restricted diet. The 36-Item Short-Form Survey (SF-36) and Satisfaction with Physical Function and Appearance (SPF/SPA) survey were assessed at baseline and post-intervention. Analyses of covariance determined differences in change scores among groups (p<0.05). Paired t-tests determined significant pre-intervention versus post-intervention scores within groups (p<0.05).
Results Across the intervention, all groups (p<0.05) improved the physical component, SPF, and SPA scores. Only the low/moderate/diet group (p<0.001) significantly improved the mental component score. The high/vigorous group achieved 84.5% of the low/moderate/diet group effect for change in physical component score, and the low/moderate group achieved 83.7% of the low/moderate/diet group effect for change in mental component score.
Conclusions In general, a low amount of moderate intensity exercise combined with diet was the most effective intervention for improving HrQoL. Of the exercise-only interventions, vigorous intensity exercise provided the greatest impact on changes in physical function. On the other hand, low amounts of moderate intensity exercise provided the greatest impact on mental well-being, potentially being a more attainable exercise dose for previously sedentary individuals with pre-diabetes to achieve.
- diabetes mellitus
- type 2
- caloric restriction
- exercise
- quality of life
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
There is a well-established relationship between lifestyle interventions—similar to the Diabetes Prevention Program—and improvement in self-rated health-related quality of life, among various populations.
What are the new findings?
Of exercise-only interventions, low amounts of moderate intensity exercise provided the greatest impact on mental well-being among individuals with pre-diabetes.
Of exercise-only interventions, vigorous intensity exercise provided the greatest impact on changes in physical function among individuals with pre-diabetes.
Low amounts of moderate intensity exercise may be a more attainable exercise dose for previously sedentary individuals with pre-diabetes to achieve.
How might these results change the focus of research or clinical practice?
Among individuals with pre-diabetes, clinicians may want to encourage low amounts of moderate intensity exercise to improve mental well-being.
Introduction
Type 2 diabetes impacts nearly 10.5% of the US population over the age of 18 years old.1 Moreover, the increased prevalence of adults with pre-diabetes has placed individuals at a 4%–6% increased risk of developing type 2 diabetes and cardiovascular disease.2 Due to the negative health outcomes associated with pre-diabetes and type 2 diabetes, the Diabetes Prevention Program (DPP) was developed. The DPP is a landmark program establishing lifestyle changes (diet, exercise, and weight loss) to be the ‘gold standard’ therapy for prevention of diabetes, successfully reducing the incidence of diabetes by 58% in those at risk over 3 years of follow-up.3 4 Exercise alone is effective in reducing the risk of cardiovascular disease, type 2 diabetes, adverse blood lipid profile, certain cancers, and all-cause mortality.5 Moreover, among individuals with diabetes, exercise alone provides notable benefits for disease management, and is typically used in conjunction with pharmacotherapy regimens for optimal efficacy.6 Among individuals with impaired glucose tolerance, reduction of type 2 diabetes incidence appears comparable for exercise alone, diet alone, and combined exercise and diet interventions.7
Along with increased risk of cardiometabolic disease, pre-diabetes can reduce self-rated health-related quality of life (HrQoL).8–17 In addition to HrQoL being an important outcome for lifestyle intervention studies, improvements in HrQoL may serve to reinforce the benefits of and adherence to lifestyle changes made to improve negative health outcome responses. There is a well-established relationship between lifestyle interventions—similar to DPP—and improvement in self-rated HrQoL, among various populations.5 18–21 While successful in improving self-rated HrQoL, a combined lifestyle intervention approach makes it challenging to distinguish differences between the impact of diet and exercise components on changes in health-related outcomes (eg, glucose, HrQoL, body composition, etc). Therefore, the relative contribution of varying amounts and intensities of exercise alone to the overall diet plus exercise effect of DPP on changes in self-rated HrQoL is poorly understood. Moreover, the most efficacious amount and intensity of exercise for improvement in self-rated HrQoL among individuals with pre-diabetes is important to understand in order to better tailor treatment.
The Studies of Targeted Risk Reduction Interventions through Defined Exercise among individuals with Prediabetes (STRRIDE-PD) aimed to better understand the benefit of aerobic exercise relative to a combined exercise and diet program—similar to DPP—and explored the independent influence of exercise amount and intensity for improving glucose metabolism among individuals at risk of developing type 2 diabetes. The STRRIDE-PD Trial provided a distinct opportunity to investigate changes in self-rated HrQoL among individuals with pre-diabetes—the population of interest in the DPP. Thus, the objective of this secondary analysis was to determine the relative contribution of aerobic exercise alone at various amounts and intensities in comparison with a DPP-like lifestyle intervention (exercise, calorie restriction, and weight loss) on self-rated HrQoL measures.
Research design and methods
Study design
In the STRRIDE-PD randomized trial (NCT00962962; conducted from 2009 to 2012), participants completed physical fitness, body composition, and HrQoL assessments prior to and following a 6-month supervised exercise intervention.22 Participants were recruited continuously between 2009 and 2012 from Durham, North Carolina, USA, and the surrounding area. Randomization was performed with a standard computer-based random number generator using a randomized design, blocked by gender and race.
Participants
Potential participants (n=3052) responded to local advertisements and were screened by phone. Of these, 288 met inclusion criteria and were enrolled in the study. Inclusion criteria were as follows: age 45–75 years, body mass index (BMI) 25–35 kg/m2, resting blood pressure <160/90 mm Hg, fasting plasma glucose ≥95–<126 mg/dL (readings from two separate days, both being ≥95 mg/dL and the first being <126 mg/dL), and low density lipoprotein cholesterol <190 mg/dL. Exclusion criteria included smoking, diabetes, uncontrolled hypertension, musculoskeletal disorders, and cardiovascular disease. After obtaining written informed consent, participants were asked to maintain their current lifestyle during a 3-month run-in period, followed by randomization into one of four exercise or exercise plus diet and weight loss groups. The purpose of the run-in period was to discourage individuals who were not serious about the study commitment and thus reduce the dropout rate that could occur after randomization. Demographic data were collected prior to the 3-month run-in period. All other measures in this analysis—HrQoL surveys, anthropometrics, and physical fitness—were assessed at baseline (pre-intervention) and post-intervention (16–24 hours following the final exercise bout). Participants were compensated for participation in the STRRIDE-PD trial.
Exercise training and dietary intervention
Participants were randomized into one of four 6-month intervention groups. Oxygen consumption (V̇O2) reserve was chosen for exercise prescription and calculated as previously described.22 The intervention groups were as follows: (1) high amount/moderate intensity exercise (High/Mod)–16 kcal/kg of body weight/week (KKW) at 50% V̇O2 reserve; (2) high amount/vigorous intensity exercise (High/Vig)–16 KKW at 75% V̇O2 reserve; (3) low amount/moderate intensity exercise (Low/Mod)–energy expenditure of 10 KKW at 50% V̇O2 reserve; (4) low amount/moderate intensity exercise plus diet (Low/Mod/Diet)–10 KKW at 50% V̇O2 reserve plus a calorically restricted diet designed to reduce body weight by 7% over 6 months. The Low/Mod/Diet group design was based on the DPP.3 22
Following baseline, a ramp period (~10 weeks) gradually increased exercise amount to the prescribed level. Exercise mode was predominantly treadmills and included elliptical trainers, rowing, and bicycle ergometers. A recommended exercise frequency with the goal of a 60 min maximum for a single exercise session was provided by the research team, but the actual exercise frequency was up to the participant. Participants were asked to exercise under supervision at least 2 days per week; at these sessions, heart rate monitor data were downloaded and training progress was discussed. Participants were allowed to exercise at our fitness center without supervision on the other days. Exercise intensity was maintained by using a target heart rate range confirmed by a submaximal oxygen consumption test at the midpoint of the exercise program. Thus, as fitness increased, participants worked harder to achieve a similar heart rate, which required reducing weekly exercise time to maintain constant weekly energy expenditure. All exercise was verified by Polar Electro (Kempele, Finland) downloadable heart rate monitors. Maximal exercise duration was capped at 6 hours per week to limit participant burden. Participants in the Low/Mod/Diet group attended four initial counseling sessions, followed by 12 biweekly intensive group sessions adapted from the DPP manual.
The 36-Item Short-Form Survey
The 36-Item Short-Form Survey (SF-36) was assessed before and following the intervention period as a measure self-perceived physical and mental health over the prior 4 weeks. The SF-36 is scored into eight domains: (1) physical functioning, (2) role-physical, (3) bodily pain, (4) general health, (5) vitality, (6) social functioning, (7) role-emotional, and (8) mental health. The physical component score is comprised of the following four domains: physical functioning, role-physical, bodily pain, and general health. The mental component score is comprised of the following four domains: role-emotional, social functioning, vitality, and mental health. The SF-36 is valid and reliable, and there are standardized norms available for comparative purposes.23 24 Participants’ raw scores were converted into scale scores ranging from 0 to 100, with greater scores representing better HrQoL or greater functioning for all scales.25 The SF-36 was scored by assessors blinded to subject group assignment.
Satisfaction with Physical Function and Appearance Survey
The Satisfaction with Physical Function and Appearance Survey (SPF/SPA) was used to measure participant-perceived satisfaction with physical function and appearance before and following the intervention period. This survey has been validated in several randomized controlled trials assessing HrQoL and physical activity participation.26 27 This nine-question survey contains five questions on physical function and four questions on physical appearance. Participants answered the following questions (question number in parentheses) regarding physical function: ‘Over the past 4 weeks, how satisfied have you been with (1) your overall level of physical fitness? (2) the muscle strength in your legs? (3) your level of endurance or stamina? (5) your overall level of energy? (6) your physical ability to do what you want or need to do?’ The following questions were asked regarding physical appearance: ‘Over the past 4 weeks, how satisfied have you been with (4) your muscle tone? (7) your weight? (8) your shape? (9) your overall physical appearance?’ Each item was rated on a 7-point Likert scale ranging from −3 to 3 with the following terms: (−3) very dissatisfied, (−2) somewhat dissatisfied, (−1) a little dissatisfied, (0) neither, (+1) a little satisfied, (+2) somewhat satisfied, and (+3) very satisfied. Questions 1, 2, 3, 5, and 6 were averaged together to generate an SPF score. Similarly, questions 4, 7, 8, and 9 were averaged together to generate an SPA score. Greater scores indicate greater satisfaction with physical function and/or appearance. The SPF/SPA Survey was also scored by blinded assessors.
Physical fitness and anthropometrics
All physical fitness and anthropometric measures were assessed by trained study staff and evaluated at baseline and following the 6 months of prescribed exercise training. Peak V̇O2 was determined via maximal cardiopulmonary exercise tests with a 12-lead ECG and expired gas analysis on a treadmill using the TrueMax 2400 Metabolic Cart (ParvoMedics, Salt Lake City, Utah, USA) as previously described.22 The two greatest, consecutive, 15-second readings within the final 90 s of the test were averaged to determine peak V̇O2. Exercise tests were performed under medical supervision and were conducted by clinical exercise physiologists.
Height and body weight were assessed with the participant in light weight clothing without shoes. Height was assessed using a stadiometer (Seca-220, Hamburg, Germany) to the 0.1 cm, measured one time. Body weight was assessed using a calibrated digital scale to the nearest 0.1 kg, measured one time prior to a muscle biopsy visit. Waist circumference around the minimal waist (the lowest circumference measurement above the umbilicus and below the xiphoid) and hip circumference were measured to the nearest 0.1 cm. Body composition measures were assessed using the BOD POD air displacement plethysmography method (COSMED, Chicago, Illinois, USA).
Statistical analyses
Data were analyzed using JMP V.15.0 (SAS Institute, Cary, North Carolina, USA). Prior to data analysis, all assumptions for each statistical test were assessed. A p value of <0.05 was considered significant. To determine between group differences, analysis of covariance (ANCOVA), with baseline values used as covariates, was conducted. If an ANCOVA p value was <0.10, we then conducted the following three prespecified independent t-tests comparisons to reduce the number of post hoc tests and increase power: (1) to assess for a diet effect (Low/Mod vs Low/Mod/Diet); (2) to assess for an amount effect (Low/Mod vs High/Mod); and (3) to assess for an intensity effect (High/Mod vs High/Vig). A p value of <0.05 was considered significant in post hoc testing. Two-tailed, paired t-tests were used to determine whether the pre-intervention versus post-intervention scores for changes within each group were significant. Because the variables in the present article were not the primary outcome variables for the STRRIDE-PD Trial, there were no a priori power calculations. ‘Per protocol’ analyses are presented.
Results
Of the 237 participants randomized, 162 individuals had complete data for either the SF-36 (n=160) or the SPF/SPA (n=158) surveys. Figure 1 describes the flow of participants from recruitment to post-intervention testing. Baseline demographic characteristics and the prescribed exercise interventions are presented for each group in table 1. Participants were on average 59.3±7.5 years old, obese (BMI: 30.4±2.7 kg/m2), predominantly, female (60.2%) and white (78.9%). Baseline and change scores for SF-36 individual domains, physical component score, mental component score, SPF, SPA, physical fitness, and anthropometrics are presented for each group in table 1.
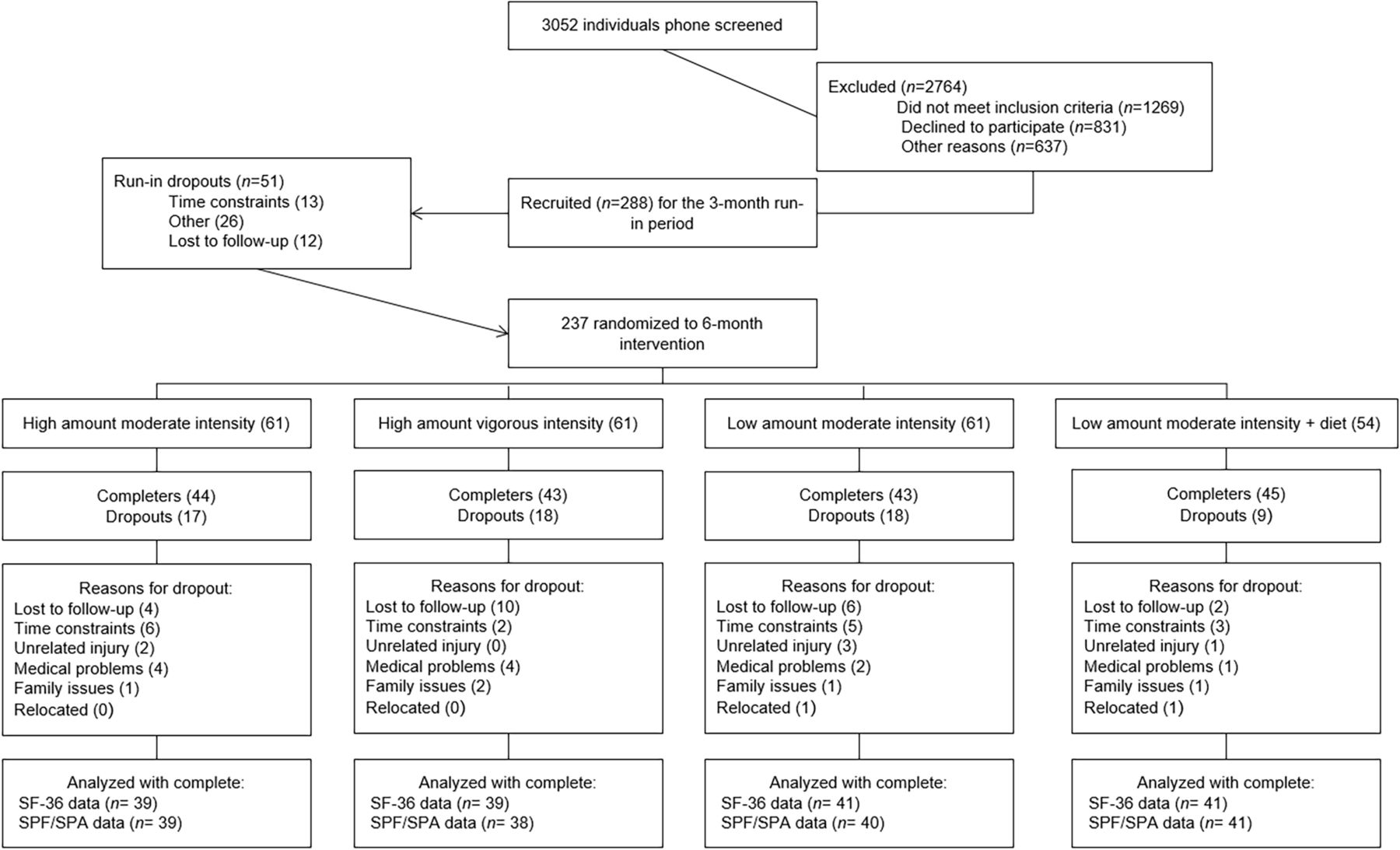
Flow chart of screening, randomization, inclusion and exclusion. SF-36, 36-Item Short-Form Survey; SPF/SPA, Satisfaction with Physical Function and Appearance.
Demographic characteristics, exercise intervention prescription, and adherence, as well as baseline and change values for satisfaction with physical function and appearance, SF-36, anthropometric, and physical fitness variables by intervention group
Exercise effects on physical fitness and anthropometrics
Following the intervention, all groups significantly improved peak V̇O2, ranging from 1.3±2.4 to 2.8±2.8 mL/kg/min (p<0.05 for all groups). For anthropometric measures, all groups experienced a reduction in weight (ranging from −1.1±3.4 to −6.2±4.9 kg; p<0.05 for all groups) and fat mass (ranging from −1.2±3.0 to −6.1±5.8 kg; p<0.05 for all groups). High/Vig was the only group to significantly increase lean body mass (0.7±1.7 kg; p<0.05). High/Mod, High/Vig, and Low/Mod/Diet decreased both minimal waist circumference (ranging from −1.2±4.0 to −3.8±6.0 cm; p<0.10 for groups) and hip circumference (ranging from −1.3±2.6 to −4.0±3.7 cm; p<0.05 for groups). Table 2 displays significant differences among groups for each physical fitness and anthropometric measure.
ANCOVA and post-hoc comparison values for SF-36 domains, physical fitness, and anthropometric variables
Effects on SF-36
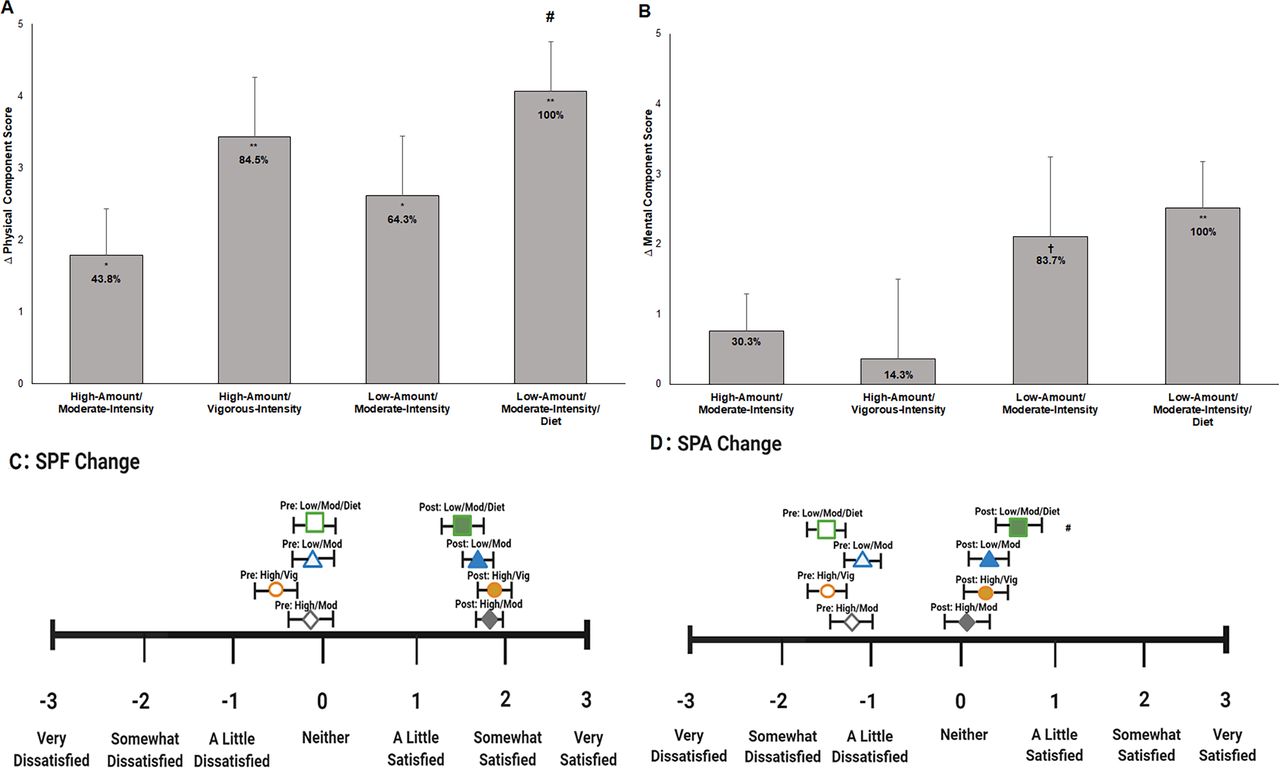
Across the 6-month intervention, there was a significant diet effect (p=0.037), with Low/Mod/Diet having a greater improvement in physical component score compared with Low/Mod (group effect: F=2.201; p=0.030). All groups significantly improved their physical component score, ranging from 1.8±4.1 to 4.1±4.4 points (p<0.05 for all groups; table 1, figure 2A). The High/Vig group was able to achieve 84.5%, the Low/Mod group achieved 64.3%, and the High/Mod group achieved 43.8% of the effect for change in physical component score compared with the ‘gold standard’ Low/Mod/Diet group. There was no significant between group effects for change in mental component score (group effect: F=0.711; p=0.182). Only the Low/Mod/Diet group experienced a significant increase in mental component score following the intervention (2.5±4.2; p<0.001) and the Low/Mod group trended toward a significant increase (2.1±7.3; p=0.072; table 1, figure 2B). The Low/Mod group was able to achieve 83.7%, the High/Mod group achieved 30.3%, and the High/Vig group achieved 14.3% of the effect for change in mental component score compared with the ‘gold standard’ Low/Mod/Diet group.

{kind=link}
{kind=link}
(A) Change in physical component score by group. (B) Change in mental component score by group. (C) Satisfaction with physical function pre-intervention and post-intervention scores by intervention group. (D) Satisfaction with physical appearance pre/post-scores by intervention group. Empty green square=Low/Mod/Diet pre-intervention score. Filled green square=Low/Mod/Diet post-intervention score. Empty blue triangle=Low/Mod pre-intervention score. Filled blue triangle=Low/Mod post-intervention score. Empty orange circle=High/Vig pre-intervention score. Filled orange circle=High/Vig post-intervention score. Empty gray diamond=High/Mod pre-intervention score. Filled gray diamond=High/Mod post-intervention score. Error bars indicate SE. Significant within-group change: †p<0.1; *p<0.05; **p<0.01. Significant or trending diet effect: #p<0.05. SPF/SPA, Satisfaction with Physical Function and Appearance.
When evaluating changes in each of the domain scores, Low/Mod/Diet achieved significant or trending toward significant improvements in ‘physical functioning’ (p=0.008), ‘role-physical’ (p=0.001), ‘bodily pain’ (p=0.069), ‘general health’ (p<0.001), ‘vitality’ (p=0.003), ‘role-emotional’ (p=0.003), and ‘mental health’ (p=0.030). Low/Mod achieved significant or trending toward significant improvements in ‘physical functioning’ (p<0.001), ’general health’ (p=0.081), ‘vitality’ (p=0.023), and ‘role-emotional’ (p=0.022). High/Vig achieved significant or trending toward significant improvements in ‘physical functioning’ (p<0.001) and ‘role-physical’ (p<0.001). High/Mod achieved significant or trending toward significant improvements in ‘physical functioning’ (p=0.002), ‘general health’ (p=0.003), and ‘vitality’ (p=0.018). Table 2 displays significant differences among groups for each SF-36 domain.
Effects on SPF/SPA
Following the intervention, there was a trending diet effect (p=0.092), with Low/Mod/Diet experiencing a slightly greater improvement in SPA score compared with Low/Mod (group effect: F=1.97; p=0.040). There were no significant between-group effects for change in SPF score (group effect: F=0.98; p=0.135). Prior to the intervention, all intervention groups reported overall negative average SPF and SPA scores, indicating overall dissatisfaction with both physical function and physical appearance (figure 2). Following the intervention, all groups significantly increased average SPF (p<0.001 for all groups; figure 2C) and SPA (p<0.05 for all groups; figure 2D) scores. Following the intervention, both average SPF and SPA scores were positive for all intervention groups, indicating overall satisfaction with physical function and physical appearance.
Discussion
Though the impact of participation in aerobic exercise on measures of self-rated HrQoL is well established,28–30 little research has compared a DPP-like intervention with an exercise-only intervention at various amounts and intensities. The STRRIDE-PD Trial provided the opportunity to determine what percentage of a DPP-like intervention effect can be achieved with aerobic exercise alone at varying levels on self-rated HrQoL measures, as well as determine the independent effect of exercise amount and intensity on self-rated HrQoL among individuals with pre-diabetes.
In this secondary analysis, the Low/Mod/Diet group, in general, had the greatest improvement in self-rated HrQoL measures, except for change in SPF score. When assessing the independent effects of exercise amount and intensity on self-rated HrQoL, vigorous intensity exercise alone provided the greatest improvement in self-rated physical function, observed in both the physical component score and the SPF score. However, low amount, moderate intensity exercise alone (Low/Mod) and in conjunction with diet (Low/Mod/Diet) provided the greatest improvement in self-rated mental function, observed in both the mental component score and the SPA score. Thus, when the goal of an exercise intervention is to improve how a person physically feels and functions, prescribing vigorous intensity exercise alone, especially in high amounts (High/Vig), is likely to have the greatest impact on individuals with pre-diabetes. Conversely, performing the minimum recommended amount of exercise as suggested by the 2018 Physical Activity Guidelines for Americans5 –150 min/week of moderate intensity–provides the greatest improvement on perceived mental health and appearance. While we did not test the reasons for this observed difference, there are likely reasons we can speculate on. For example, (1) low amounts of any intensity of aerobic exercise may be perceived as easier to attain; and/or (2) the addition of calorie restriction and weight loss to low amount, moderate intensity exercise typically may result in greater improvements in self-confidence and body image—more so than vigorous intensity exercise alone—especially for previously sedentary individuals who are at risk of diabetes.
There is a well-established relationship between combined lifestyle interventions and measures of HrQoL among individuals with pre-diabetes and type 2 diabetes.8–17 The DPP followed (n=3234) individuals without diabetes, but who had elevated fasting and post-load plasma glucose for an average of 3.2 years. Participants were randomized to either an intensive lifestyle program, metformin program, or placebo.8 Their intensive lifestyle program aimed to induce ≥7% weight loss and prescribed 150 min/week of moderate intensity exercise. The DPP intensive lifestyle program showed improvement in physical component score, which was not found in the metformin or placebo groups. However, they did not observe a significant change in mental component score in any of the three groups.8 In our intervention arm mimicking the first 6 months of the DPP lifestyle program, we observed a significant improvement among our Low/Mod/Diet group in both physical and mental component scores.
Similarly, the Look AHEAD trial (n=5145) randomized individuals with overweight or obesity and type 2 diabetes to either an intensive lifestyle intervention or diabetes support and education group for up to 8 years of follow-up.9 The intensive lifestyle intervention was designed to induce ≥7% weight loss in the first year and encouraged participation in ≥175 min/week of moderate intensity physical activity. The Look AHEAD results demonstrate that enrollment in a weight management program yielding significant weight loss and improvement in physical fitness also improves HrQoL via physical component score.9 Yet, we found among individuals with pre-diabetes, participation in aerobic exercise alone and the addition of diet plus weight loss significantly improves not only the physical component score, but also SPF and SPA scores. Furthermore, our DPP-like intervention was the only group to significantly improve the mental component score. This observed difference may be due to study population, likely meaning once an individual has diabetes, improving mental well-being is a more challenging task.
This is one of the first studies to explore the independent effects of exercise amount and intensity to a DPP-like intervention on self-rated HrQoL measures. In addition, our study employed two different measures of self-rated HrQoL, allowing us to assess the effects of our exercise interventions on different dimensions of HrQoL. Further, showing the desired physical efficacy of the intervention, the 6-month duration of the intervention resulted in significant changes among objective measures of cardiorespiratory fitness and anthropometrics.
Limitations of this study include the use of questionnaires to capture perceived HrQoL measures. Randomization should have helped to equalize the groups with reference to this limitation, and quality of life measures are by definition perceptual. Nonetheless, use of questionnaires can result in the inclusion of false answers, differences in understanding and interpretation of questions, lack of personalization, and unanswered questions. Also, this study was designed as an efficacy study, not an intention-to-treat study. Moreover, obtaining a high amount of moderate intensity exercise among individuals with low fitness levels is challenging. On average, the High/Mod group participants in this study required, on average, 4.8 hours of moderate intensity exercise (more for women) to expend 16 KKW. The diet component of the Low/Mod/Diet group was more intensive compared with the exercise-only groups, and included many additional one-on-one and small group interactions; the additional time and attention resulted in the lowest dropout rate of all the groups. Since we did not control for the greater amount of personal contact time received by Low/Mod/Diet relative to the exercise-only groups, it is possible that the interpersonal contact contributed to the differential improvement in mental well-being. Further, the data collected in this study were collected between the years of 2009 and 2012, therefore it is unclear if the outcomes measured here would be the same if the data had been collected more recently today as obesity continues to become visually normalized.
Conclusions
In general, a low amount of moderate intensity exercise in conjunction with diet was the most effective intervention for improving multiple measures of self-rated HrQoL. While vigorous intensity exercise provided the greatest impact on changes in self-rated physical function, a low amount of moderate intensity exercise provided the greatest impact on changes in self-rated mental health and appearance. Further research is needed to clarify why low amounts of moderate intensity exercise produced the greatest impact on mental well-being. Low amounts of moderate intensity exercise may be more attainable for previously sedentary individuals with pre-diabetes and provide greater quality of life benefits. This may lead to greater long-term adherence to lifestyle change.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Duke University Institutional Review Board (Pro00012628). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors would like to thank the research volunteers for their dedication and effort, and the staff who helped with the implementation of the study and assisted with data collection.
References
Footnotes
Contributors WEK, CAS, and CWB contributed to the study conception and design. Data collection was performed by LWP, LAB, LHW, and CAS. Data analysis and manuscript conception were conducted by KAC, LMR, LBF, ICS, RQW and KMH. The first draft of the manuscript was written by KAC and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript. KAC is the guarantor and accepts full responsibility for the work and/or the conduct of the study, had access to the data, and controlled the decision to publish.
Funding This study was funded by the National Institute of Diabetes and Digestive and Kidney Diseases (R01DK081559). KAC is supported by the National Human Genome Research Institute (1T32HG008955-01). LMR was supported by the National Heart, Lung, and Blood Institute (T32-HL-007101). Support for CW was provided in part by the US Department of Veterans Affairs Rehabilitation Research and Development Service Program (I01RX002843).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.