Article Text

Abstract
Introduction Healing time for neuropathic planter foot ulcers (NPFUs) in persons with diabetes may be reduced through use of non-removable fiberglass total contact casting (F-TCC) compared with removable cast walkers (RCWs), although the evidence base is still growing.
Research design and methods We conducted a rapid review and systematically searched for, and critically assessed, randomized controlled trials (RCTs) that compared the efficacy of F-TCC versus RCW, focusing on the time to ulcer healing in adult persons (18+ years) with NPFUs and type 1 or type 2 diabetes. We meta-analysed the mean differences and associated 95% CIs using an inverse variance, random-effects model. We also conducted a trial sequential analysis (TSA) to assess if the available evidence is up to the required information size for a robust conclusion. We assessed and quantified statistical heterogeneity between the included studies using the I2 statistic.
Results Out of 102 retrieved citations, five RCTs met the eligibility criteria. Participants’ inclusion in relation to stage of ulcer was highly variable as was peripheral neuropathy complicating comparisons. F-TCC appeared to present a shorter ulcer healing time (−5.42 days, 95% CI −9.66 days to −1.17 days; I2 9.9%; 5 RCTs; 169 participants) compared with RCW. This finding was supported by the TSA.
Conclusions There is limited evidence from RCTs to suggest that F-TCC has a shorter ulcer healing time compared with RCW among adults with diabetic NPFUs. Properly designed and conducted RCTs are still required for a stronger evidence base.
- Meta-Analysis
- Diabetic Foot
- Wound Healing
- Clinical Medicine
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Previous systematic reviews with broader inclusion criteria reported reduced ulcer healing time for total contact casting (TCC) compared with removable devices.
WHAT THIS STUDY ADDS
Five randomized controlled trials specifically compared time to ulcer healing between non-removable fiberglass TCC (F-TCC) and removable cast walkers (RCWs) in adult persons with neuropathic planter foot ulcers and type 1 or type 2 diabetes.
There was a significantly shorter ulcer healing time with the non-removable F-TCC compared with RCWs.
Trial sequential analysis suggested that the required information size was not reached but indicated that the current sample size has power to achieve significant evidence without any error.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
This study confirms clinical perception that non-removable F-TCC is a more effective technique than RCW.
Introduction
Persons with diabetes (PWD) are at risk of developing nerve injury (eg, diabetic neuropathy) due to elevated blood glucose levels. Symptoms of diabetic neuropathy range from reduced or complete loss of sensations in the leg/foot, to skin ulcerations, and infections of the skin that can progress to the deeper soft tissues and bone, and in severe cases, lower extremity amputations (LEAs). Prevention of diabetic neuropathy is of utmost importance as it affects an estimated 15% of all PWD during their lifetime; with 15%–20% of these persons potentially progressing to LEAs.1 While thorough assessments for peripheral neuropathy can be quite involved, the use of the 10 gm monofilament test has become the accepted clinical screening tool.2 3 Thankfully, advances in technology such as the Corneal Confocal Microscopy test may prove to be an effective alternative to traditional approaches, including being able to identify PWD who are likely to develop future diabetic neuropathy.4 5
For PWD who have developed complications, adequate treatment and effective management strategies are critical. Among those who developed neuropathic planter foot ulcers (NPFUs), a shorter ulcer healing time has been suggested with the use of the fiberglass total contact casting (F-TCC) compared with the traditional removable cast walkers (RCW), owing to compliance with use of the device (removable vs non-removable devices).6 TCC suggestively improves ulcer healing, with higher ulcer healing rates recorded with their use compared with use of the traditional RCW.7 8 The evidence regarding these offloading devices is still growing and their comparative effectiveness is not yet fully established. In view of the accumulating evidence and still many unanswered clinical questions, we aimed to systematically identify, critically appraise, and summarize the findings from randomized controlled trials (RCTs) that compared the efficacy of F-TCC against RCW in adult persons (18+ years) with NPFUs and type 1 or type 2 diabetes.
Methods
This rapid systematic review was part of a Systematic Prospective Assessment of Rapid Knowledge Synthesis project (https://osf.io/fnx36/). The review was registered with the Open Science Framework (registration: osf.io/xhcr6) and was conducted in accordance with the WHO guidelines for rapid reviews,9 and the findings reported following the Preferred Reporting Items for Systematic Reviews and Meta-analysis guidelines.10
Search strategy
We first conducted the literature search in May 2020, limiting our searches to articles published since 2010 in the English language (online supplemental appendix 1). However, we updated the searches in July 2021 to include all eligible articles irrespective of year of publication. A knowledge synthesis librarian (NA) designed a literature search strategy for Medline (Ovid) and another librarian peer reviewed the search strategy using the Peer Review of Electronic Search Strategies (PRESS) checklist.11 The revised search strategy was adapted for Embase (Ovid) and Cochrane Central (Ovid).
Supplemental material
Population, Intervention, Comparator, Outcome & Study design (PICOS) framework
In summary, we assessed the efficacy of F-TCC compared with RCW in adult persons with NPFUs and type 1 or type 2 diabetes, focusing on RCTs published in the English language. The ulcer must have involved the foot (below the ankle and on the plantar surface). Ulcers involving the ankle or above, ulcers other than neuropathic plantar ulcers (including ischemic ulcers or venous stasis ulcers) and ulcers due to other types of diabetes (eg, gestational) were excluded. The primary outcome was time to ulcer healing.
Study selection, data extraction and risk of bias assessment
One reviewer screened the citations retrieved from the literature searches and documented the number of ineligible citations at the title/abstract screening stage, and both the number and reasons for ineligibility at the full-text article screening stage. The reviewer scanned references of all included full-text articles for potential trials for inclusion, extracted data from the included trials and assessed risk of bias in included trials using the Cochrane tool for risk of bias assessment in RCTs.12 Another reviewer checked the extracted data and risk of bias assessments for errors. The two reviewers resolved any disagreements with the extracted data and risk of bias assessments through discussions or involvement of another reviewer.
Data analysis
We summarized the characteristics of the included RCTs and the risk of bias assessments, and presented data in tabular form. We meta-analysed mean differences and associated 95% CIs using an inverse variance, random-effects model. We assessed and quantified statistical heterogeneity between pooled results from the included studies using the I 2 statistic.13 We conducted a trial sequential analysis (TSA) to assess if the available evidence is up to the required information size (total sample size) for robust conclusion. For this analysis, we followed the methods outlined by Wetterslev and colleagues14 and used the TSA software (V.0.9.5.5 beta Copenhagen Trial Unit, Center for Clinical Intervention Research, Rigsospitalet, Copenhagen, Denmark (www.ctu.dk/tsa)). We calculated the required information size using a random-effects model with a minimum mean difference of −5.42 days, and a heterogeneity level (I2 ) of 10%. We assumed two-sided tests of significance, a power level of 80%, and alpha <0.05.
Results
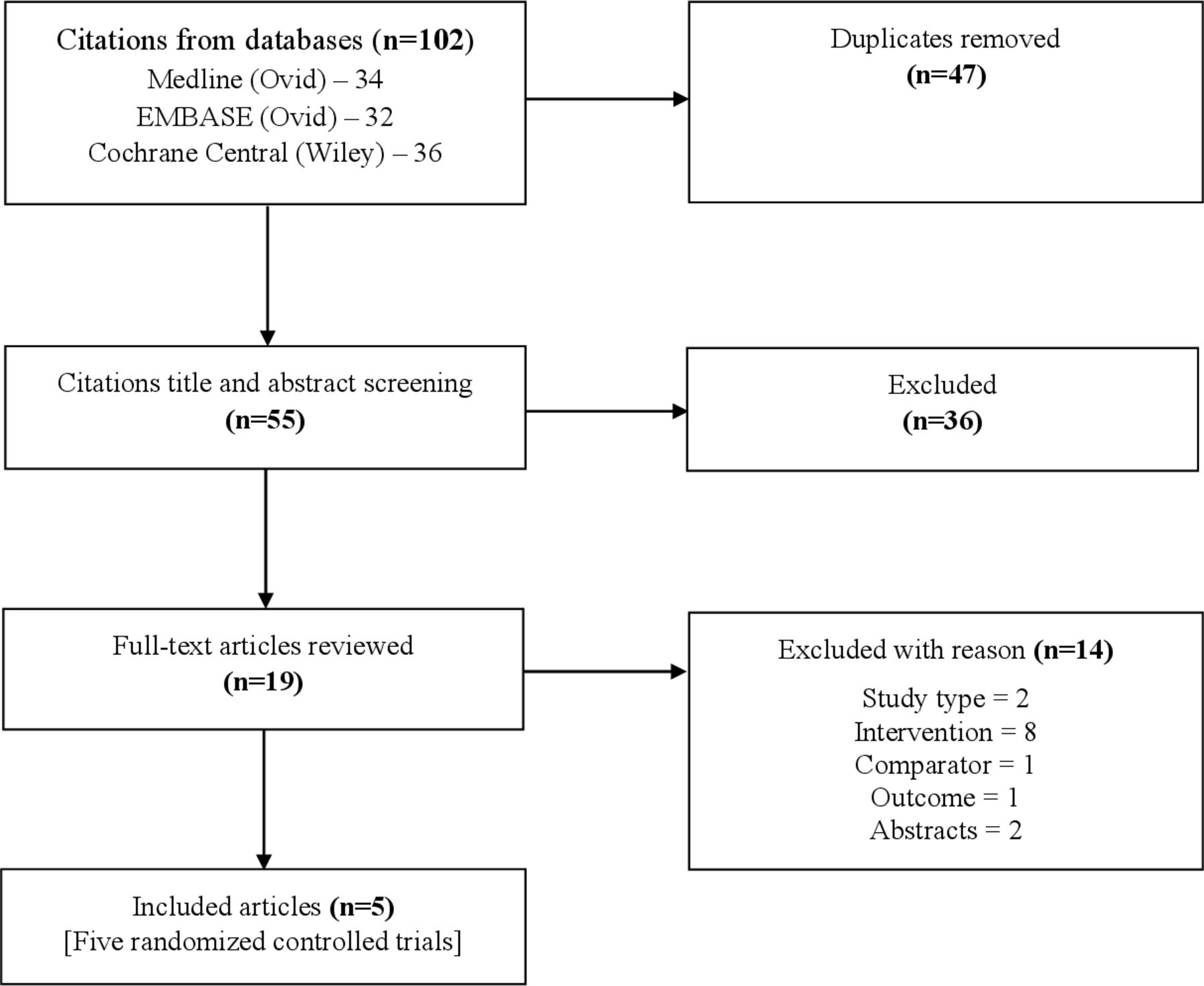
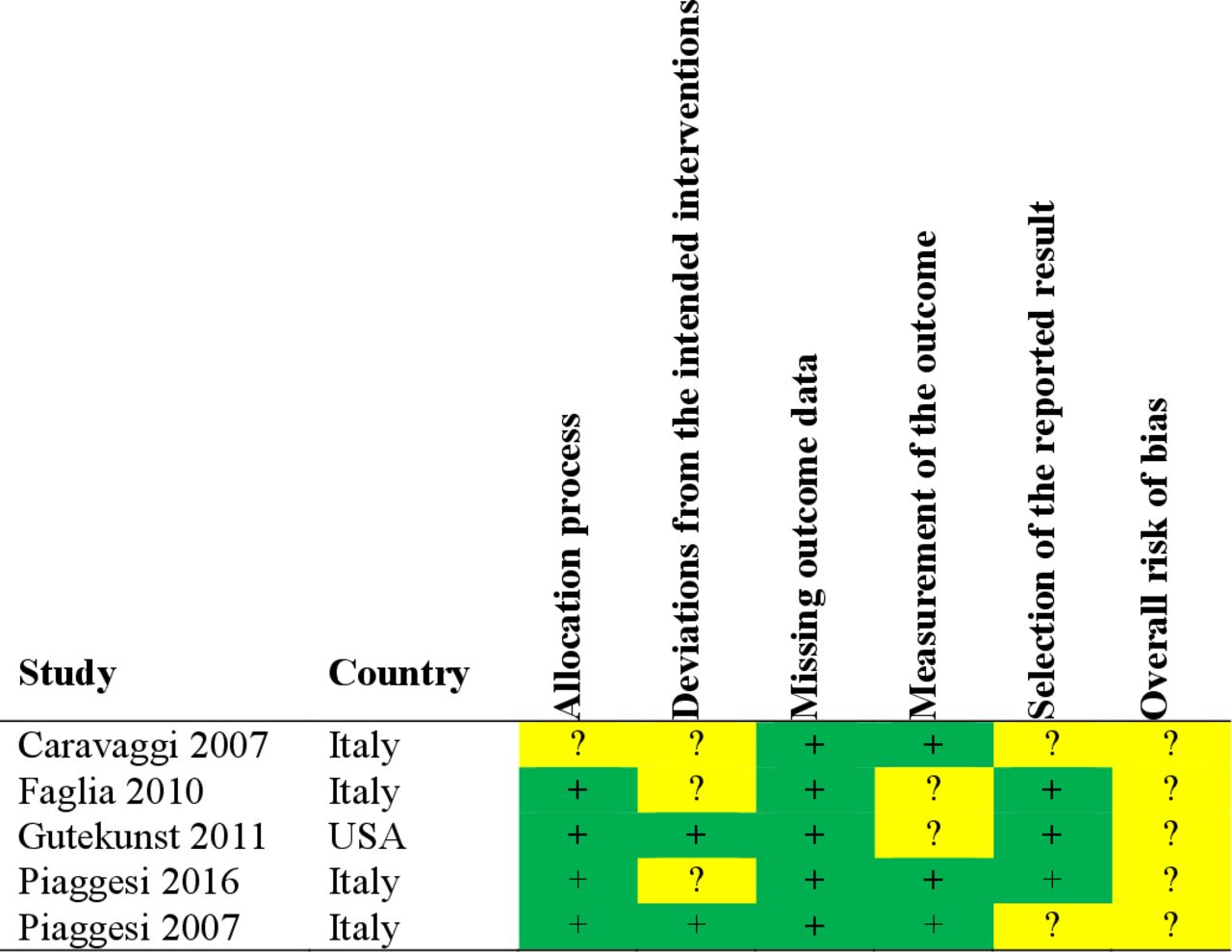
From 102 retrieved citations, we included five RCTs representing 211 participants (figure 1).15–19 The characteristics of the trials are summarized in table 1. There were four trials from Italy,15 16 18 19 and one trial from the USA.17 These trials varied in participants’ inclusion criteria with regard to ulcer stages and definition of peripheral neuropathy. There was also substantial variability in the method of application of the F-TCC and in the characteristics of the RCW. It is important to note, however, that the mean hemoglobin A1c was largely comparable across intervention groups within and across trials, and the duration of follow-up was similar across trials. Two trials were industry-funded,16 19 one was not industry-funded,17 one trial was not funded,18 and one trial did not report on funding.15 One of the trials was judged to have an unclear risk of bias for allocation process, three trials were judged to have an unclear risk of bias for deviations from the intended interventions, and two trials were judged to be of unclear risk of bias for each measurement of the outcome, and for selection of the reported result, with all the trials judged to be of overall unclear risk of bias (figure 2).
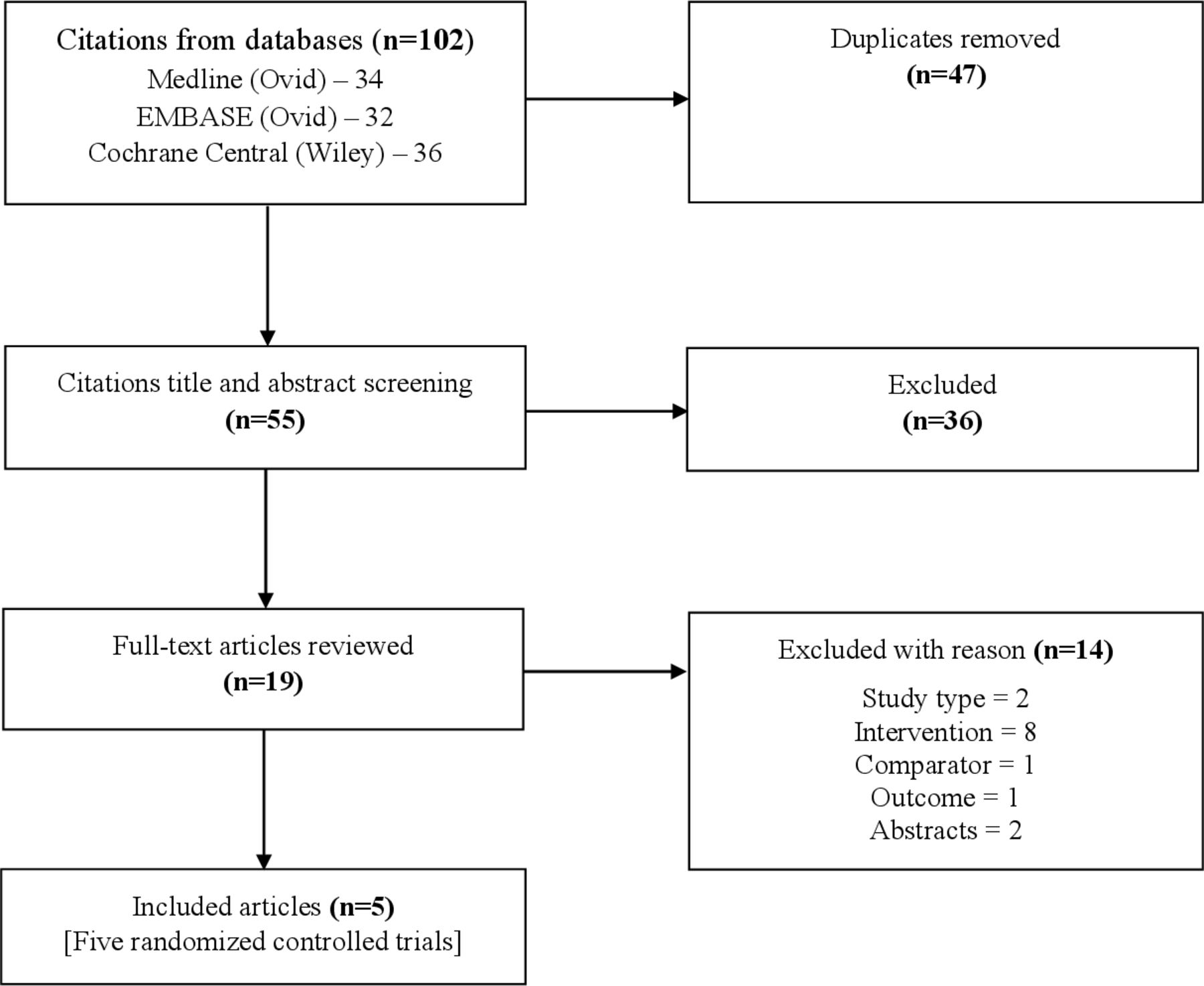
Summary of literature search and screening process (modified Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) flow chart).
Summary characteristics of the included randomized controlled trials
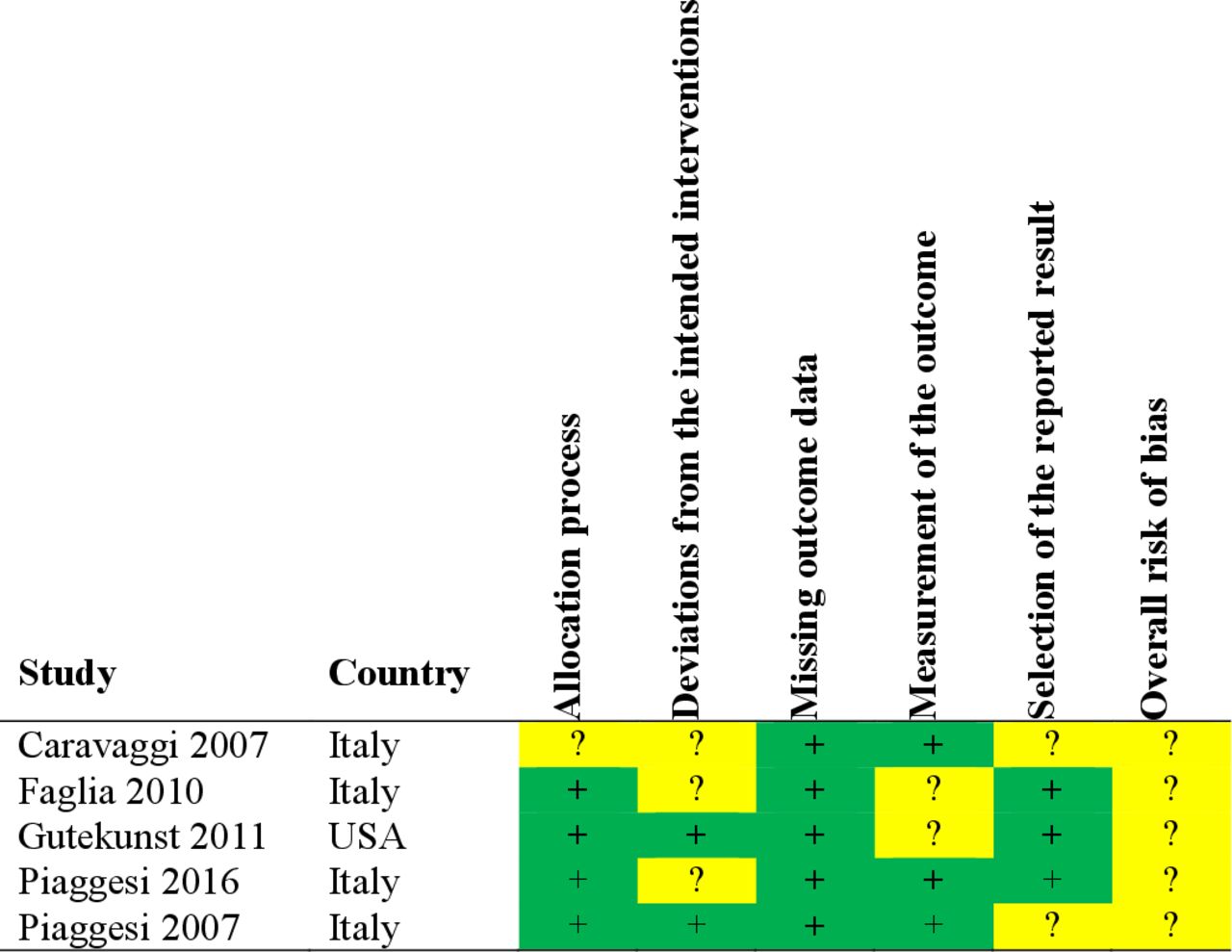
Risk of bias assessment of the included randomized controlled trials.
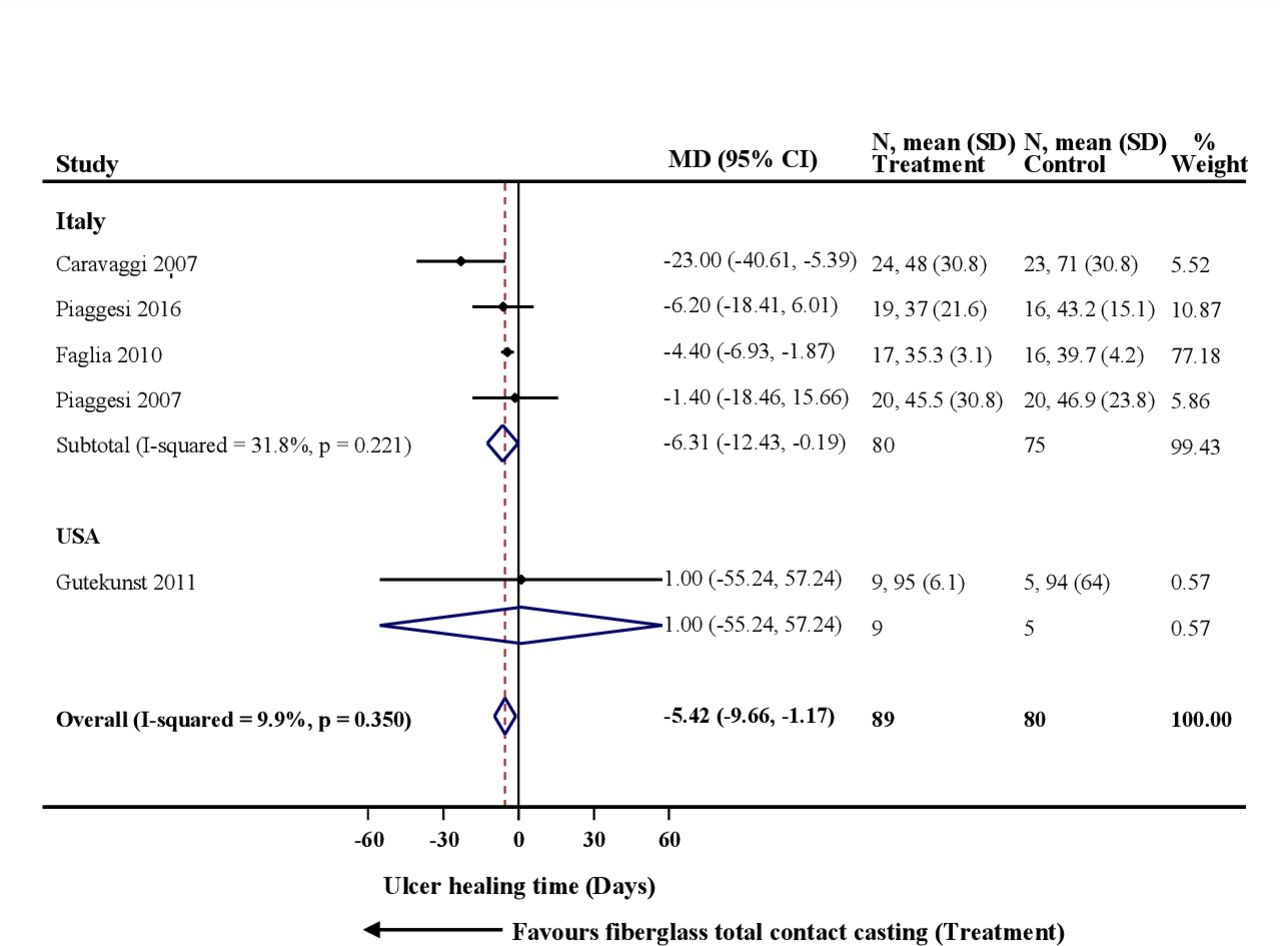
F-TCC was found to have a shorter ulcer healing time (−5.42 days, 95% CI −9.66 days to −1.17 days; I 2 9.9%; 5 RCTs; 169 participants) compared with RCW (figure 3). We conducted sensitivity analysis excluding one trial for which standard deviation (SD) for mean ulcer healing times was not reported (we used the largest SD from the other trials).15 F-TCC was found to still have a shorter ulcer healing time compared with RCW, although with a slightly lower point estimate, reduced heterogeneity and more precise effect estimates (−4.40 days, 95% CI −6.85 days to −1.95 days; I 2 0%; 4 RCTs; 122 participants). In subgroup analysis limiting to the trials from Italy, which have similar trial and participants’ characteristics, a shorter ulcer healing time with F-TCC compared with RCW was observed; with (−6.31 days, 95% CI −12.43 days to −0.19 days; I 2 31.8%; 4 RCTs; 155 participants) and without inclusion of the study that did not report SD (−4.41 days, 95% CI −6.86 days to −1.96 days; I 2 0%; 3 RCTs; 108 participants). These findings however appeared driven by one large, industry-funded trial.16 There was insufficient data to assess the influence of trial characteristics on the pooled estimates.

Forest plot for time to ulcer healing.
Trial sequential analysis
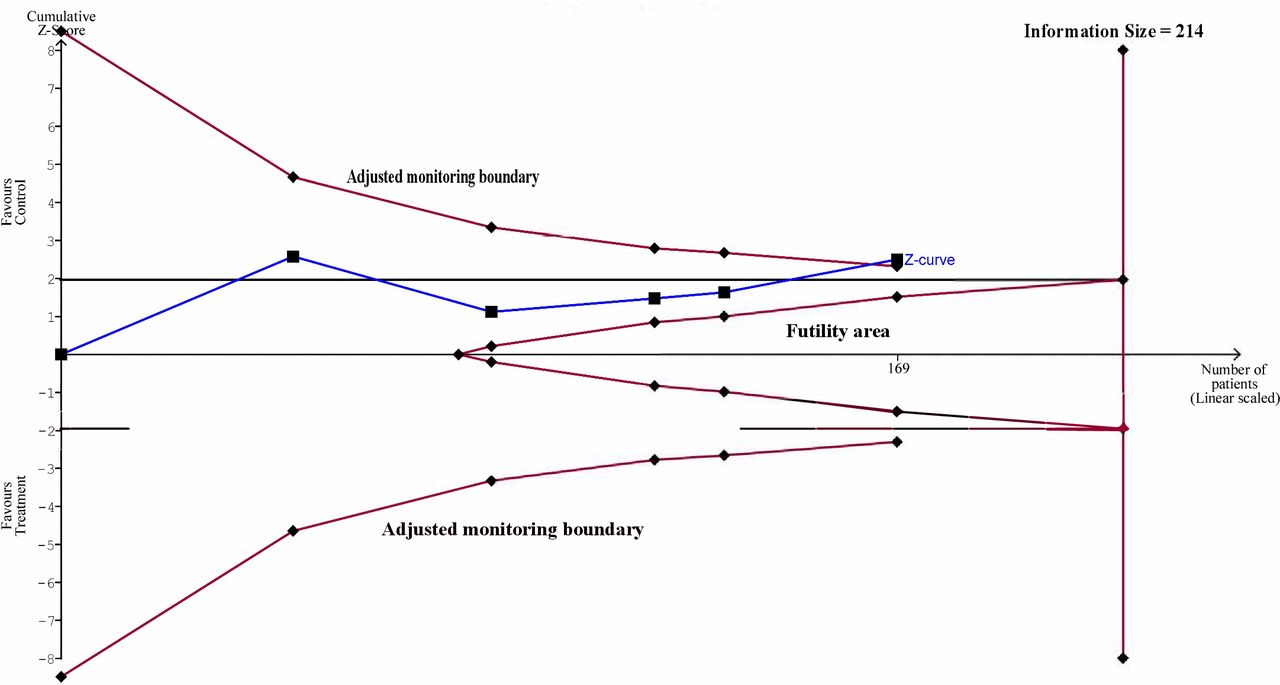
As shown in figure 4, the required information size (214 participants) was not reached but the cumulative Z-curve (blue line) crossed the adjusted trial sequential monitoring boundary for benefit (red line) enabling conclusion of a significant decrease in time to healing among participants undergoing F-TCC. The pooled estimate is therefore less likely to be a random finding due to a lack of power or multiple testing if bias could be ignored.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Trial sequential analysis for time to ulcer healing.
Discussion
This rapid systematic review summarized the evidence from a small number of trials but the findings provide considerable insight into the comparative benefits of F-TCC for shorter ulcer healing time compared with RCW among adult PWD with NPFUs. We found F-TCC to have a shorter ulcer healing time compared with RCW. However, we advise cautious interpretation of our finding as participants in the trials may have in fact differed with respect to the general management of diabetes, including medication use and adherence, and effective management/control of other chronic diseases from which a PWD may also be suffering. Most of the trials excluded persons whose ulcer(s) did not heal by the end of the follow-up periods from the analysis and there were potential issues concerning risk of bias in the included trials. We were unable to compare the efficacy of F-TCC and RCW in subpopulations, nor were we able to explore the influence of characteristics of the included trials on the pooled-effect estimates.
Notwithstanding the observed variability in the included trial characteristics, the results from this review may be due to adherence (compliance) associated with the use of F-TCC which is an irremovable device compared with the RCW which is removable. To the best of our knowledge, this is the first meta-analysis that compares ulcer healing time specifically between F-TCC and RCW among adult PWD and NPFUs; hence, there are no available reviews for direct comparison with our findings. A health technology assessment of evidence from RCTs did, however, find that, compared with RCW, NPFU healing was improved with TCC (0.17 days, 95% CI 0.00 days to 0.33 days) when compared with RCW (0.21 days, 95% CI 0.01 days to 0.40 days), but found no difference in ulcer healing between TCC and non-RCW.7 Another systematic review of RCTs found higher healing rates of 74%–95% among participants treated with TCC compared with 52%–85% among those treated with the RCW.8 Morona and colleagues reported reduced ulcer healing time for TCC compared with removable devices.20 However, they included randomized and non-randomized trials in their meta-analysis and compared both total TCC and instant TCC with all types of removable devices (therapeutic shoes and RCW). Elraiyah and colleagues also reported reduced ulcer healing time for TCC compared with removable devices.21 However, they included comparison with custom-made temporary footwear and was therefore not limited to comparison with RCWs. Further, a systematic review by Lazzarini and colleagues investigated effectiveness of offloading interventions in diabetic foot ulcer healing, including both controlled and non-controlled studies.22 They found TCCs and non-removable knee-high walkers to be equally effective, and concluded that the evidence supports use of non-removable knee-high offloading devices as the first-choice offloading intervention for healing plantar neuropathic forefoot and mid-foot ulcers. However, this systematic review did not include meta-analysis and therefore, the conclusions were not based on quantitative analysis. That said, these findings support the perception of better treatment outcomes for TCC and may therefore mean that TCC confers better treatment outcomes for NPFUs in PWD compared with RCW due to its non-removable nature, which potentially ensures compliant use of the device. A recent rapid qualitative review evaluated participants’ experiences using offloading devices.23 The review found that adherence to offloading devices depended on the participants’ assumed self image with using an offloading device every day and that the participants needed time to reflect on using these devices in their daily lives so they are better prepared to accept a new self image that incorporated the device use, which helps increase adherence in the long term. The review, however, also found that when expectation of healing was unmet, participants’ adherence to offloading devices appear to decrease.
Review limitations and merits
Given that this was a rapid review, we carefully negotiated efficiencies into our approach. For example, we did not search clinical trial registries or conference abstracts so may have missed potentially relevant RCTs and that we included only English language publications so may have missed any relevant non-English publication. In keeping with rapid review expectations, only one reviewer selected studies for inclusion, which could introduce bias and potential omission. This review only considered time to healing and did not consider longevity of the healed wound or other relevant outcomes. Despite these potential limitations, this review is strengthened by the inclusion of highly skilled knowledge synthesis librarians, who developed and peer reviewed the literature search strategies, using the PRESS checklist. Further, the conduct and reporting of the review were according to known rapid review standards. The review findings answer important clinical questions that would be of help to clinicians and policy makers in decision-making regarding the management of diabetic NPFUs.
Conclusions
Among adults with diabetic NPFUs, there is limited evidence from RCTs to suggest that F-TCC has a shorter ulcer healing time compared with RCW; however, clinically, the perception is that F-TCC is a more effective technique than RCW. TSA indicated that the current sample size has power to achieve significant evidence without any error. The risk of bias in the available evidence warrants a cautious interpretation of the finding. More properly designed and conducted RCTs are still required for a stronger evidence base.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
The authors thank Dr. Andrea C. Tricco and Ms. Nazia Darvesh of the Knowledge Synthesis Team, Li Ka Shing Knowledge Institute of St. Michael’s Hospital, Toronto, Canada for their support and coordination of the study, Dr. David Sinacore and Dr. Dave Gutekunst for providing them with additional data, and Ms. Angela Osterreicher for peer reviewing their literature search strategy.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Methodology: GNO, RR, NA, TH, LB, IT and AMAS; Data acquisition: GNO, OLTL, NA and AMAS; Formal analysis: GNO and RR; Interpretation: GNO, RR, JME and AMAS; Validation: GNO, RR and AMAS; Draft manuscript: GNO; Manuscript revisions: GNO, RR, OLTL, NA, TH, LB, IT, JME and AMAS; Final approval for submission: GNO, RR, OLTL, NA, TH, LB, IT, JME and AMAS; Guarantors: GNO and AMAS.
Funding The Canadian Institutes of Health Research (CIHR) Project Grant for Systematic Prospective Assessment of Rapid Knowledge Synthesis (SPARKS).
Disclaimer The authors do not have any relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties. JME is a member of working groups for the management of the diabetic foot for the Canadian Diabetes Association, International Working Group for the Diabetic Foot and the Infectious Disease Society of America, and has been involved in the drafting of guidelines for all of these organizations.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.