Article Text

Abstract
Introduction Women are generally perceived to have a lower risk of cardiovascular events than men, despite a lack of data, particularly among patients with diabetes. Here, we investigated gender differences in the risk of heart failure (HF) events in patients with type 2 diabetes and coronary artery disease (CAD). We also assessed the association between cardiovascular risk factor management and HF events.
Research design and methods This retrospective registry study enrolled consecutive patients with both type 2 diabetes and CAD, based on angiography records and medical charts at 70 teaching hospitals in Japan, from January 2005 to December 2015.
Results The registry included 7785 patients with a mean follow-up period of 1328 days. The mean age of the patients was 67.6 years. The risk of hospitalization for HF in patients with both type 2 diabetes and CAD was significantly higher among women than among men (HR, 1.26, 95% CI 1.06 to 1.50). The relationship between HF risk and achieved low-density lipoprotein cholesterol (LDL-c) and systolic blood pressure, but not hemoglobin A1c, differed between women and men, with statistically significant interactions (p=0.009 and p=0.043, respectively).
Conclusions Women with type 2 diabetes and CAD have a higher risk of HF than men. A significant gender interaction was observed in the association between HF risk and risk factor management, particularly regarding LDL-c and systolic blood pressure. The effectiveness of risk factor management may differ between men and women regarding HF prevention among patients with type 2 diabetes and CAD.
- Diabetes Mellitus, Type 2
- Heart Failure
- Sex Characteristics
Data availability statement
Data are available upon reasonable request. Deidentified data are available from the PI upon request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Women without diabetes have fewer cardiovascular events than men of the same age without diabetes, but this advantage appears to be lost in the context of type 2 diabetes.
Particularly, the Framingham study showed higher incidence of heart failure in women than in men aged >55 years among patients with diabetes and prior coronary or rheumatic heart disease.
What are the new findings?
Under the current evidence-based optimized medical therapy and coronary intervention, women with type 2 diabetes and established coronary artery disease have a higher risk of heart failure than men.
A significant gender interaction was observed in the association between heart failure risk and risk factor management, particularly regarding low-density lipoprotein cholesterol and systolic blood pressure.
How might these results change the focus of research or clinical practice?
A strategy for risk reduction of heart failure specifically for women with type 2 diabetes and coronary artery disease should be established.
Introduction
The incidence of myocardial infarction (MI) and mortality due to coronary artery disease (CAD) is lower in women than in men, which is a common phenomenon worldwide.1 2 However, this may not be true for patients with type 2 diabetes. Although women without diabetes certainly have fewer cardiovascular (CV) events than men of the same age without diabetes, this advantage appears to be lost in the context of type 2 diabetes.3–5 In a Finnish cohort, Juutilainen et al5 showed a marked male excess CAD risk among individuals without diabetes, whereas among patients with diabetes the gap between men and women was almost eliminated. Moreover, the Framingham study showed no gender difference in CAD risk among patients with diabetes.4 A meta-analysis of 37 cohort studies revealed a greater excess risk of CAD associated with diabetes in women than in men.6
Patients with diabetes are reportedly much more likely to develop heart failure (HF) than individuals without diabetes.7 8 Notably, this risk has a gender dependence, as first demonstrated in the Framingham Heart Study.4 9 While the risk of HF was twofold higher in men with diabetes than in respective individuals without diabetes, the risk was fivefold higher in women with diabetes. The underlying reason for the increased risk of women with diabetes developing HF is not entirely clear. Therefore, a practical multiple risk factor management strategy for women to reduce CV events, including HF, has not been well discussed. Furthermore, few studies have found possible gender differences in the prognostic impact of risk factor modification in high-risk patients with type 2 diabetes.
This study aimed to investigate a possible gender difference in the risk of hospitalization for HF in consecutively registered patients with type 2 diabetes and CAD and investigate gender differences in the association between HF events and CV risk factor management.
Methods
Study design and setting
This retrospective registry study enrolled consecutive patients with type 2 diabetes and CAD, based on the evaluation of coronary artery angiography (CAG) records and medical charts by trained clinical research coordinators at 70 teaching hospitals in Japan, from January 1, 2005 to December 31, 2015.
Patients
The following patients were included in this study: those aged >20 years with type 2 diabetes and established CAD. Type 2 diabetes was diagnosed according to the Japanese Diabetes Care Guidelines 2016,10 that is, a fasting plasma glucose level of ≥126 mg/dL and a plasma glucose level of ≥200 mg/dL at any sampling point, or ≥200 mg/dL at 2 hours after a 75 g oral glucose tolerance test, with glycosylated hemoglobin A1c (HbA1c) ≥6.5%. Before enrollment, participants diagnosed as having type 2 diabetes were included when their medical history and medication were consistent with the diagnosis.
CAD was defined as at least 75% stenosis in at least one branch of the coronary artery, a history of an acute coronary syndrome (ACS) as defined by the 2003 guidelines of the American Heart Association11 and the Japanese Circulation Society,12 percutaneous coronary intervention (PCI), or coronary artery bypass grafting (CABG) before enrollment. Patients with malignant neoplasms with a disease-free period of <3 years were excluded.
Data collection and variables
The date of registration was the date of CAG or the date of outpatient visit within 3–6 months after CAG for ACS. Data at registration included age, gender, height, weight, blood pressure, heart rate, medical history, treatment history, laboratory information, concomitant medications (such as diabetic, antihypertensive, antiplatelet, hyperlipidemic, and diuretic drugs), and smoking status as a lifestyle. Follow-up involved the collection of data on blood pressure, heart rate, laboratory test results, concomitant medication information, and CV events every 6 months from the date of enrollment until the death of the patient or the end of the study.
We used the following three variables to represent risk factor management during the observation period: averaged systolic blood pressure (SBP), low-density lipoprotein cholesterol (LDL-c), and HbA1c.
Outcome measures
Hospitalization for HF was defined as hospitalization for worsening HF requiring intravenous treatments, such as diuretics or vasodilators. HF in our study was principally diagnosed according to the diagnostic criteria of the Framingham Heart Study13 and based on information on medical records, that is, response to treatments with diuretics and vasodilators. HF events were reported to the study office and subsequently adjudicated by the event evaluation committee.14
Statistical analyses
Continuous variables measured at registration are expressed as mean±SD unless otherwise indicated. Categorical variables are presented as numbers and percentages. Gender differences in continuous variables were assessed using Student’s t-test or Wilcoxon rank-sum test. Differences in categorical variables were assessed using χ2 test or Fisher’s exact test.
The cumulative incidence of hospitalization for HF was estimated using the Kaplan-Meier method and gender differences were assessed using the log-rank test. The number of hospitalizations for HF and person-years at risk were calculated to estimate gender-specific incidence per 100 person-years. Cox proportional hazard models were used to calculate the HR and 95% CI of the risk of hospitalization for HF in women and men, which was adjusted for age, HbA1c, SBP, LDL-c, ejection fraction, estimated glomerular filtration rate (eGFR), body mass index, smoking status, history of MI, stroke, PCI, CABG, and malignancy, and use of ACE inhibitor, angiotensin II receptor blocker, beta-blocker, biguanide, aspirin, statin, and hemodialysis. The continuous variables among these covariates were dichotomized according to clinically meaningful reference or median values. Although we did not adjust for diabetes duration as a variable in our main analysis because the diabetes durations obtained from the memory of patients were considered less accurate, we conducted sensitivity analysis using diabetes duration dichotomized according to the median value (8 years) as an adjuster in the Cox proportional hazard model because these dichotomized variables were more stable. We also calculated the incidence of HF per 100 person-years, stratified by age and gender.
To exclude possible confounding effects of renal function on the diagnosis of HF, we constructed the same multivariable Cox proportional hazard model to estimate the risk of HF after excluding patients with hemodialysis or an eGFR <15 mL/min.
Averaged values of SBP, LDL-c, and HbA1c during the observation period were used as variables representing risk factor management. We calculated the HR of the risk of HF of each stratified value, as stratified by the reference value, that is, 6%–7% (42–52 mmol/mol) for HbA1c, 130–140 mm Hg for SBP, and 80–100 mg/dL for LDL-c, using Cox proportional hazard models with an interaction term between gender and the stratified variables in each model.
All analyses were performed using JMP V.15.1 (SAS Institute, Cary, North Carolina, USA) and SAS V.9.4. For all tests, p values <0.05 were considered statistically significant.
Results
Among 46 658 patients who underwent CAG at 70 hospitals, 7896 patients with type 2 diabetes and coronary artery stenosis were enrolled, of whom 111 were excluded due to lack of follow-up. The final study population was 7785 patients (28% women), of whom 7454 had significant (>75%) stenosis, 2470 had a history of acute MI, 3503 had a history of PCI, and 875 had a history of CABG (online supplemental figure 1). The mean follow-up period was 1328 days.
Supplemental material
Characteristics of patients
The baseline clinical characteristics are shown in table 1. Women were significantly older, had a long history of diabetes, had poorer glycemic control, and a higher prevalence of hypertension than men. Regular smoking was less prevalent among women than men (p<0.0001) and fewer women had a history of MI or PCI (p<0.0001). Both groups received aspirin equally. Women had more prescriptions for statins (p=0.0003), calcium blockers (p<0.0001), angiotensin receptor blockers (p=0.001), insulin (p<0.0001), and diuretics (p=0.0058). Men had more prescriptions for clopidogrel (p=0.02), beta-blockers (p<0.0001), and ACE inhibitors (p<0.0001).
Baseline characteristics of patients grouped by gender
Incidence of hospitalization for HF
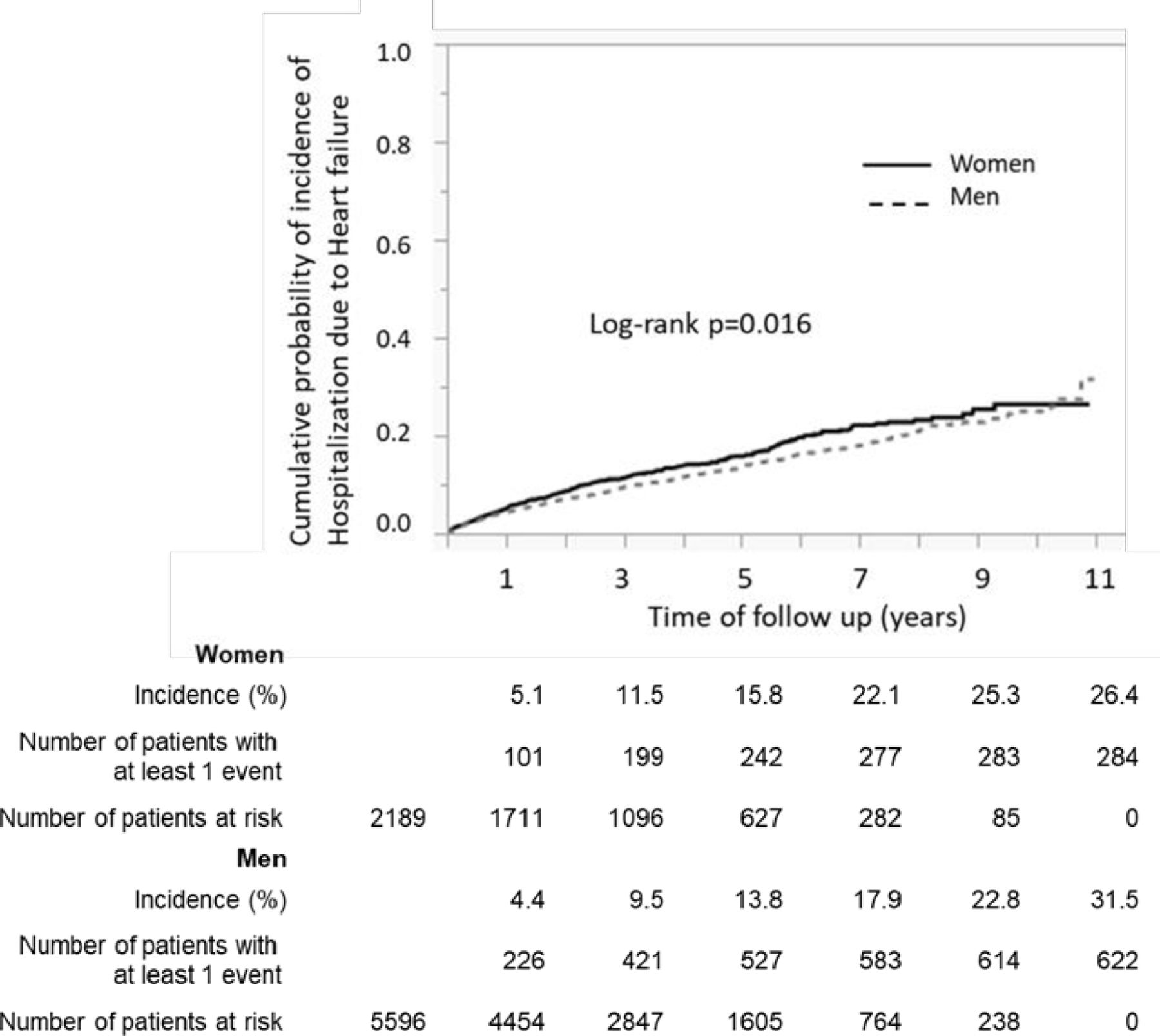
In total, 284 women (13.0 %) and 622 men (11.1 %) were hospitalized for HF, with incidence rates of 3.70 and 3.12 per 100 patients per year in women and men, respectively (log-rank p=0.016) (figure 1, online supplemental table 1). The adjusted risk of hospitalization for HF in women was significantly higher than in men (HR, 1.26 (95% CI 1.06 to 1.50), p=0.008). Although the incidence of HF increased with age in both genders, a higher incidence was found in women than in men aged <65 years (table 2).
Supplemental material
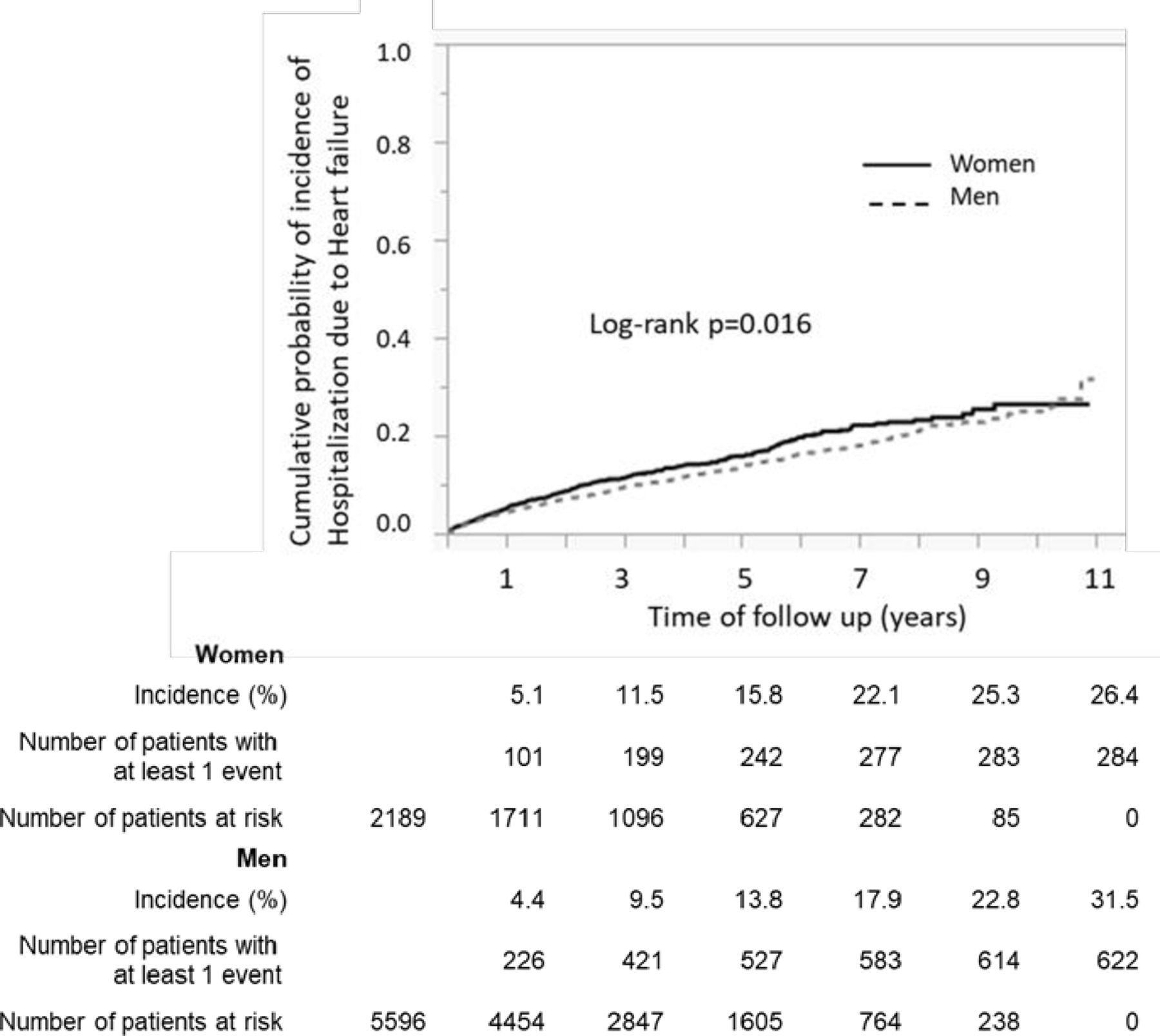
Incidence of hospitalization for heart failure. Kaplan-Meier curves showing the cumulative incidence of heart failure. Men: solid line; women: dashed line; both were with type 2 diabetes and established coronary artery disease.
Incidence of hospitalization for heart failure per 100 person-years, by age group
Sensitivity analysis
The incidence of hospitalization for HF and the adjusted HR for risk, calculated after excluding patients with either hemodialysis or an eGFR <15 mL/min, are shown in online supplemental table 2. After excluding patients with hemodialysis, the risk of hospitalization for HF was significantly higher in women than in men (HR, 1.22 (95% CI 1.02 to 1.47), p=0.0324). Furthermore, even after excluding patients with hemodialysis and an eGFR <15 mL/min, the risk of HF continued to be significantly higher in women than in men (HR, 1.21 (95% CI 1.00 to 1.46), p=0.0469). In terms of diabetes history, analysis using diabetes duration as an adjuster also showed a significantly higher risk of hospitalization for HF in women than in men (HR, 1.24 (95% CI 1.05 to 1.48), p=0.0138).
Risk factor management and hospitalization for HF
Figure 2 shows the association between stratified SBP (figure 2A), HbA1c (figure 2B), and LDL-c (figure 2C) and the risk of hospitalization for HF in women and men during the observation period. While the relationship between HbA1c and risk was almost identical in men and women, we found significant interaction p values for average LDL-c and SBP, showing that women and men were differently affected by these factors (p=0.009 for LDL-c and p=0.043 for SBP).

{kind=link}
{kind=link}
Risk factor management and HR of hospitalization for HF. The relationship between the stratified SBP (mm Hg) (A), HbA1c (% and mmol/mol) (B), and LDL-c (mg/dL) (C) during the observation period and risk of HF in women and men, stratified by the corresponding reference value. HbA1c, glycosylated hemoglobin A1c; HF, heart failure; HR, heart rate; LDL-c, low-density lipoprotein cholesterol; SBP, systolic blood pressure.
In terms of LDL-c, while a direct linear relationship was observed in men with LDL-c >80 mg/dL, the relationship in women was almost constant irrespective of stratified LDL-c levels. SBP seemed to be inversely correlated with HF risk in men, but almost constant irrespective of stratified SBP levels in women with an SBP >110 mm Hg.
Discussion
We found that the risk of hospitalization for HF was significantly higher in women than in men in our cohort of patients with type 2 diabetes and CAD. This result is consistent with that of a report by the Framingham Heart Study,9 which showed that the incidence of HF was significantly higher in women than in men aged >55 years among patients with diabetes and prior coronary or rheumatic heart disease. A more recent hospital-based cohort study in Italy, which included patients with diabetes without CAD, showed that women with diabetes of perimenopausal age had a higher risk of HF than men; however, there was no significant gender difference in the overall HF risk.15 In contrast to the Framingham study, our study showed that women aged <55 years had a higher risk of HF than men. This inconsistency among study results may be attributable to the extent to which patients with diabetes have comorbid CAD, the impact of modern medications, and the practice of PCI; however, there appears to be some consensus regarding the higher risk of HF in women with diabetes.16
A few possible explanations for the higher risk of HF in women than men are available. Although men still have higher rates of cardiovascular diseases (CVDs) than women, if they do not have CAD,17 it has been recognized that women with diabetes lose their relative protection against CVDs.1 18 Therefore, it is possible that higher risks of HF reflect higher risks of CAD progression in women with diabetes, based on the assumption that HF is the manifestation of ischemic heart diseases in patients with diabetes.7 Gender disparities in risk factor management may also contribute to gender differences in HF risk in patients with diabetes and CVDs. Gouni-Berthold et al19 showed that women with diabetes and CVDs have poorer control of important modifiable risk factors than men and receive less intensive lipid-lowering treatments. Similarly, Wexler et al20 reported that women with diabetes and CAD were less likely to be prescribed aspirin than men, or when treated for hypertension or hyperlipidemia women with diabetes and CAD were less likely to have blood pressures <130/80 mm Hg or LDL-c levels <100 mg/dL. Consistent with these reports, women in our registry also had significantly higher SBP, LDL-c, and HbA1c values at baseline. Concerning drugs for CVDs, statins were more prescribed and beta-blockers were less prescribed to women than men. In this study, patients were enrolled from a continuous CAG record and the number of women enrolled in this study was one-third of the number of men. This reflects real-world CAD practice, although it may also reflect gender disparity. Women may be more likely to miss the chance to undergo CAG at the appropriate time.21
If any of these explanations for the gender difference in HF risk are correct, a more intensive risk factor management strategy for women, equivalent to that for men, is recommended to improve HF outcomes. However, this may only be justified if there is no gender difference in the effects of risk factor management on CV outcomes. Therefore, we examined the interaction between gender and the risk factor management–outcome association.
Low-density lipoprotein cholesterol
A recent large-scale meta-analysis of randomized controlled trials of statins for primary and secondary prevention of HF events reported a modest (10%) reduction in first non-fatal HF hospitalizations with statin treatment.22 These results support LDL-c as a modest predictor of HF. However, gender-specific effects on HF risk have not been analyzed. In this study, we found a statistically significant interaction between gender and HF risk, as predicted from the stratified level of achieved LDL-c. We found a direct linear relationship between HF and LDL-c in men, but HF risk was not associated with LDL-c and was almost constant in women. This suggests that LDL-c could be a predictor of HF in men but not in women. Interestingly, this result is partially consistent with the Framingham Heart Study, which showed that total cholesterol is a weak predictor of HF in men but not in women, although not with statistically significant gender interaction.23 These results, although speculative, suggest that HF in women with diabetes may be more likely to result from diabetes itself rather than CAD progression, which is strongly associated with LDL-c. In fact, the history of diabetes in women was significantly longer than that in men; however, our sensitivity analysis using diabetes duration as an adjuster showed a similar HR.
Glycosylated hemoglobin A1c
We could rule out a gender difference in the association between HbA1c levels and HF risk. Poor glycemic control predicts macrovascular and microvascular complications in patients with type 2 diabetes.24 25 A previous cohort study by Iribarren et al,26 which enrolled nearly 50 000 patients, showed that poor glycemic control could also be associated with an increased risk of HF among patients with diabetes which is consistent with the results of the UK Prospective Diabetes Study.27 Unlike our result, these researchers found that the association was stronger in men than in women, with a significant gender interaction.
Systolic blood pressure
In our analysis of blood pressure, we found a significant interaction with respect to gender. While there was a nearly negative correlation between blood pressure and HF risk among men, women with the lowest SBP had an increased risk and those with an SBP >110 mm Hg had a constant risk, irrespective of SBP. These results, although somewhat presumptive, might be interpreted as follows: low blood pressure, whether achieved by strict blood pressure reduction or a decline in cardiac function without intervention, is associated with HF risk; this is linearly associated with an increased risk in men, but in women the association exists only if the SBP is <110 mm Hg.
Strengths and limitations
The strengths of this study were that, unlike analysis of an existing database, patient information was obtained directly from medical records. The large number of patients recruited from a high number of hospitals and the large number of hospitalizations due to HF may provide sufficient power to analyze the association between outcomes and variables. Conversely, a major limitation of our study may result from collecting data retrospectively. The non-rigorous assessment of risk factors, other variables, and outcomes are weaknesses inherent in any retrospective registry study. Particularly, similar to other studies, it is often difficult to accurately diagnose HF. To exclude patients presenting signs and symptoms similar to HF, such as pneumonia and chronic obstructive pulmonary disease, HF was diagnosed based on information available at admission, relevant to the Framingham criteria, and information available after hospitalization, such as improvements in symptoms and signs after specific treatments, including diuretics and nitrovasodilators, as recommended by the Atherosclerosis Risk in Communities study investigators28 and used in the A randomized trial of intensive versus standard blood-pressure control (SPRINT) study.29 We also performed sensitivity analysis after excluding patients with hemodialysis or severe renal dysfunction to exclude those whose renal dysfunction was likely to contribute to HF-like symptoms and signs.
Although the time period of our registry limits further discussion regarding the possible effects of gender on the development of HF with a preserved or reduced ejection fraction and newly developed antidiabetic drugs, such as sodium glucose cotransporter 2 inhibitors, for the prevention of HF in patients with diabetes, our continuous enrollment of patients may provide some evidence in the near future.
In conclusion, our registry-based cohort study indicated that Japanese women with type 2 diabetes and CAD had a higher risk of HF than men. Significant gender effects were found in the association between HF risk and risk factor management, particularly regarding LDL-c and SBP. This result suggests that a strategy for HF risk reduction specific to women should be established.
Data availability statement
Data are available upon reasonable request. Deidentified data are available from the PI upon request.
Ethics statements
Patient consent for publication
Ethics approval
This study was conducted following approval by the Ethics Committee of the University of the Ryukyus, Okinawa, Japan (study ID: 104). Informed consent was obtained in the form of opt-out in each hospital.
Acknowledgments
All authors are grateful to Ms Kaori Une for data management; Ms Mayumi Higa, Ms Sayumi Mekaru, Ms Akane Kikuchi, Ms Hitomi Zukeran, Ms Hitomi Arakaki, Ms Hiromi Yamane, and Ms Ayaku Tsuha for data collection; Ms Makiko Oohorii, Ms Kaori Yamamoto, Ms Ai Sunagawa, Ms Sachiko Kitamura, Ms Hirono Saito, and Ms Saeko Nagano, of the Institute for Clinical Effectiveness, for data management and statistical analyses; and Mr Susumu Seki for statistical analysis. The authors are also grateful to Ms Kayo Chinen and Ms Takako Okumura for study management.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors YF contributed to study design, conception of the analysis, data collection, management plans, statistical analysis, and writing the manuscript. TM supervised the study design, data management, and statistical analysis, and contributed to discussion and revision of the manuscript. AT contributed to data analysis and discussion and revision of the manuscript. MI contributed to the development of the study concept and discussion and revision of the manuscript. MS contributed to the development of the study concept and discussion and revision of the manuscript as a diabetologist. KN contributed to the development of the study concept, management of the registry (with SU), and discussion and revision of the manuscript as a cardiologist. SU acted as gurantor and contributed to the full supervision and development of the study concept, management of the registry, discussion of results, and writing and revision of the manuscript. SU is responsible for the overall content as the guarantor.
Funding This study was funded by the Japan Agency for Medical Research and Development (AMED) (grant numbers JP16ek0210022h and JP191k0201068h).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.