Article Text

Abstract
Introduction The incidence of atrial fibrillation (AF), a significant risk factor for cardiovascular disease (CVD), is increasing worldwide. Type 2 diabetes mellitus (T2D) and advanced age are recognized as major risk factors for AF, but herein, we evaluated the incidence of AF in elderly patients with T2D and compared the prognosis between these patients with/without AF.
Research design and methods The Japanese Primary Prevention of Atherosclerosis with Aspirin for Diabetes (JPAD2) study is a follow-up cohort study of the JPAD trial, a randomized controlled clinical trial initiated in 2002 in 2535 Japanese patients with T2D, to examine whether low-dose aspirin prevents CVD. After completion of that trial, we followed up the patients until 2019 and evaluated the incidence of AF. We also compared the incidence of cerebral cardiovascular events in elderly patients with T2D with/without AF.
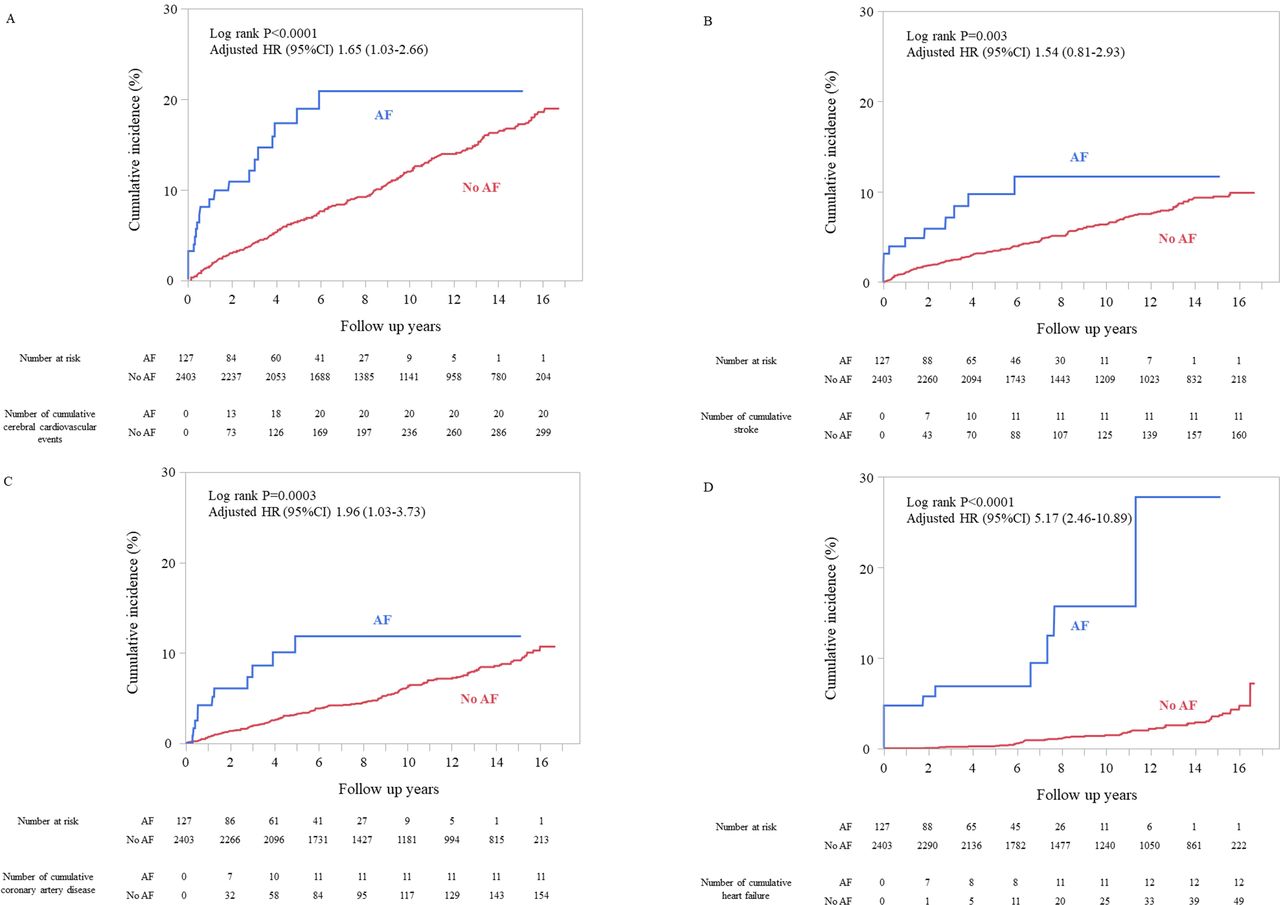
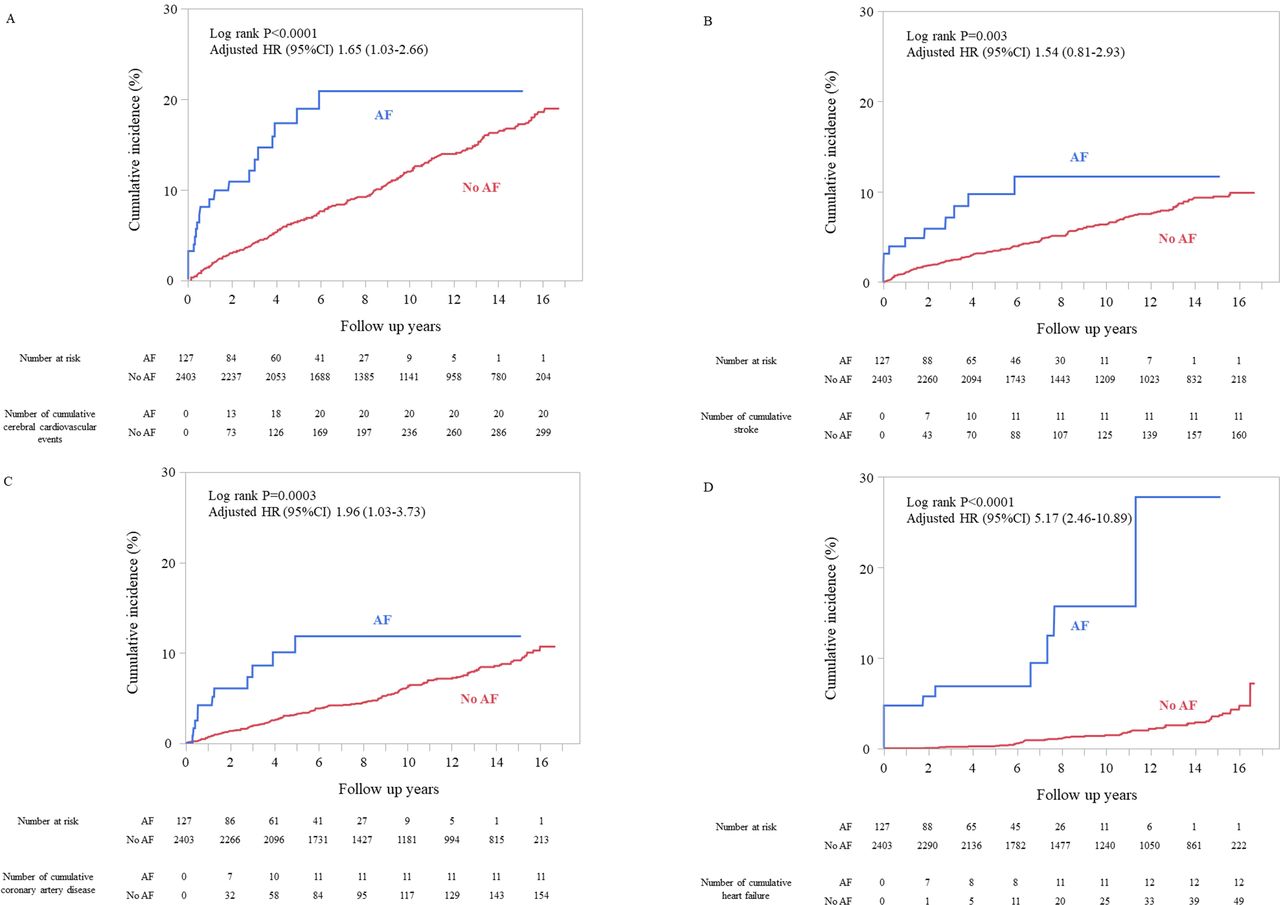
Results During the median follow-up period of 10.9 years, 132 patients developed AF (incidence rate: 5.14/1000 person-years). The adjusted HRs for cerebral cardiovascular events, stroke, coronary artery disease, heart failure, and all-cause death in elderly patients with T2D with versus without AF were 1.65 (95% CI 1.03 to 2.66), 1.54 (95% CI 0.81 to 2.93), 1.96 (95% CI 1.03 to 3.73), 5.17 (95% CI 2.46 to 10.89), and 1.82 (95% CI 1.24 to 2.67), respectively.
Conclusions Annually, 1 in 200 elderly Japanese patients with T2D are estimated to develop AF. Because elderly patients with T2D with AF are at an elevated risk for CVD, careful follow-up of this patient subgroup is necessary.
Trial registration number NCT00110448.
- atrial fibrillation
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Atrial fibrillation (AF), which is known as a major risk factor for cerebral cardiovascular disease, is dramatically increasing along with the ageing of the population and pandemic of type 2 diabetes mellitus (T2D) worldwide, as both ageing and T2D are major risk factors for AF.
The reports of the incidence and the prognosis of AF in patients with T2D are sparse.
What are the new findings?
Annually, 1 in 200 elderly Japanese patients with T2D were estimated to develop AF.
Among elderly patients with T2D with AF, almost 1 in 20 patients die every year, and almost 1 in 30 patients annually develop cerebral cardiovascular events.
The risk of cardiovascular disease in elderly patients with T2D with AF is twofold to fivefold higher than that in these patients without AF.
How might these results change the focus of research or clinical practice?
The poor prognosis of elderly patients with T2D with AF supports the need for development of effective preventive methods of AF among elderly patients with T2D.
Very careful follow-up of elderly patients with T2D is necessary for detection of new-onset AF.
Introduction
Atrial fibrillation (AF) is one of the most frequently encountered cardiac arrhythmias in daily clinical practice, and at present, with the ageing of the population and pandemic of type 2 diabetes mellitus (T2D) worldwide, the incidence of AF is increasing, as both advanced age and T2D are well-known major risk factors for AF.1 It is estimated that 10–16 million people in the USA and 72 million people in Asia will suffer from AF by the year 2050,2 3 and 17.9 million people in Europe will suffer from AF by the year 2060.4 AF is known as a major risk factor for cardiovascular disease (CVD), which shortens healthy life expectancy and imposes a tremendous economic burden.5 While it is crucial to establish countermeasures to prevent the development of AF, especially in elderly patients with T2D who are at an elevated risk for both AF and CVD, no precise estimation of the incidence of AF has been conducted in elderly patients with T2D so far. Furthermore, there are almost no reports on the risk for CVD in elderly patients with T2D with AF, especially from Asia, in spite of the potential differences in the risk of AF related to ethnicity.6
The objectives of the present study, conducted in the same cohort of patients with T2D as the study cohort for another large study, the Japanese Primary Prevention of Atherosclerosis with Aspirin for Diabetes (JPAD2) study, were to evaluate (1) the incidence of AF and risk factors for AF in elderly patients with T2D, and (2) the mortality and morbidity (cerebral cardiovascular events, stroke, coronary artery disease, heart failure, and hemorrhagic events) rates in elderly patients with T2D with and without AF.
Methods
Study design
The JPAD2 study is a prospective study conducted in the same study cohort as the 2535 Japanese patients with T2D enrolled in the JPAD trial, which was a randomized, open-label, standard care-controlled clinical trial conducted to examine the preventive efficacy of low-dose aspirin against cardiovascular events. After the completion of the JPAD trial, we followed up the patients enrolled in that trial and constructed the study cohort for the JPAD2 study. Detailed descriptions of both studies have been published previously.7 8 In brief, patient enrollment for the JPAD trial was started at 163 institutions throughout Japan in December 2002 and completed in May 2005. After completion of the JPAD trial in April 2008, we continued to follow-up all the patients until 2019 and designed the JPAD2 study in the same study cohort. Patients were followed up until July 2019 or occurrence of any fatal events at an earlier date, regardless of the development of any cardiovascular events (online supplemental figure S1). The mean age (SD) of the patients at the study baseline was 65 (10) years, and we consider that this patient cohort represented a real-world cohort of elderly Japanese patients with T2D, and the ideal cohort to evaluate the trends in the incidence of AF in elderly patients with T2D.
Supplemental material
Study patients
The inclusion and exclusion criteria for the JPAD trial have been published earlier.7 8 In brief, the patient inclusion criteria were as follows: (a) diagnosis of T2D; (b) 30–85 years of age; and (c) ability to provide informed consent. The exclusion criteria included a history of CVD, including cerebrovascular disease, and history of antiplatelet/antithrombotic therapy. Because the JPAD trial was a primary prevention trial, none of the participant patients had a history of AF at the time of recruitment for that trial.
Ascertainment of the outcomes
Diagnosis of AF was based on a 12-lead ECG or 24-hour Holter ECG monitoring, and the AF was ascertained as non-valvular AF by echocardiography. The ECG findings were validated by independent reviewers (two certified cardiologists) in conjunction with the findings of echocardiography. The primary outcome was the incidence of cerebral cardiovascular event, defined as a composite of stroke and coronary artery disease, in the patients with AF versus those without AF. Stroke was a composite of ischemic stroke (fatal and non-fatal ischemic stroke and transient ischemic attack), hemorrhagic stroke (fatal and non-fatal), and subarachnoid hemorrhage (fatal and non-fatal). Hemorrhagic stroke was also included in hemorrhagic events. Ascertainment of coronary artery disease was based on death from coronary causes, non-fatal acute myocardial infarction, unstable angina, new onset of exertional angina, and asymptomatic ischemic heart disease, percutaneous coronary intervention, and coronary artery bypass grafting. Heart failure was defined as heart failure requiring admission to a hospital. Death was classified as all-cause death, death from stroke, and cardiac death. Hemorrhagic events consisted of gastrointestinal bleeding, hemorrhagic stroke, and bleeding from any other sites. All the potential endpoints and hemorrhagic events were adjudicated by a central independent committee in both the JPAD trial and JPAD2 study.
Statistical analysis
The patient characteristics at the study baseline are expressed as means±SD or median (IQR) values for continuous variables, and in numbers and percentages for categorical variables. Comparison between the two groups was conducted by the Student’s t-test or Wilcoxon rank-sum test, as appropriate, for continuous variables and by the χ2 test for categorical variables.
To determine the incidence of AF, the follow-up time was computed from the baseline until the occurrence of AF, death, or the date of last known contact with the patient. A multivariable Cox proportional hazards model was used to identify the risk factors for AF. The variables included in the model for assessment of the risk factors for AF were age, sex (men), systolic blood pressure, body mass index (BMI), HbA1c, smoking history (current or past), use of antidiabetic drugs, antihypertensive drugs, statins, aspirin, and duration of diabetes. For evaluation of the mortality and morbidity rates in the patients with AF, we excluded five patients with AF who had not been followed up immediately after the onset of AF. In the patients with AF, the follow-up time was computed from the onset of AF until death/occurrence of any cardiovascular events and hemorrhagic events/date of last known contact with the patient. In the patients without AF, the follow-up time was computed from the baseline. The cumulative incidences of each event in the patients with T2D with and without AF were estimated using the Kaplan-Meier method, and differences between groups were assessed by the log-rank test. Furthermore, we compared the incidences of cerebral cardiovascular events, stroke, coronary artery disease, heart failure, all-cause death, and hemorrhagic events between patient groups with and without AF using the multivariable Cox proportional hazards model, with adjustments for the age, sex (men), BMI, HbA1c, smoking history (current or past), presence/absence of hypertension and/or dyslipidemia, use of aspirin, and duration of diabetes. As secondary analysis, we compared the mortality and morbidity rates between the study patients with and without AF over a follow-up period of 6 years, as the majority of patients with AF were censored after 6 years of follow-up.
All the statistical analyses were conducted using SAS V.9.4 (SAS Institute). All the statistical tests were two sided, and p<0.05 was set as being indicative of statistical significance.
Results
The mean age±SD of the patients at the baseline was 65±10 years, and the median duration of diabetes was 7.0 years (IQR: 2.9–12.3). Over the course of the median follow-up period of 10.9 years, 132 patients developed AF (incidence rate of AF: 5.14/1000 person-years (PY), figure 1). The mean age±SD at onset of AF was 75±9 years, and the median duration of diabetes was 14.5 years (IQR: 9.8–19.6). When we compared the baseline characteristics of the patient groups with T2D with and without AF, the mean age was higher and the mean HbA1c was lower in the patient group with AF as compared with the patient group without AF (online supplemental table S1).

Cumulative incidence of atrial fibrillation (AF).
In regard to the risk factors for AF, multivariable Cox proportional hazards model identified only advanced age as a significant factor associated with a higher risk of AF, while none of the other established risk factors for cerebral cardiovascular events (eg, male sex, systolic blood pressure, BMI, HbA1c, smoking, duration of diabetes, and use of antihypertensive drugs, antidiabetic drugs, statins, and aspirin) were shown to be associated with the risk of AF in the elderly patients with T2D enrolled in the study (table 1).
Risk factors for atrial fibrillation in elderly patients with type 2 diabetes mellitus
The incidences of cerebral cardiovascular events, stroke, coronary artery disease, and heart failure were higher in the patient group with AF than in the patient group without AF (table 2, figure 2A–D). Also, the patient group with AF showed significantly elevated risk for the development of cerebral cardiovascular events, coronary artery disease, and heart failure than the patient group without AF, even after the adjustments for the conventional risk factors for cerebral cardiovascular events (figure 2A,C,D, table 2). However, after adjustments for the conventional risk factors for cerebral cardiovascular events, no significant difference in the risk of stroke was observed between the patient groups with and without AF (table 2, figure 2B).
Mortality and morbidity rates in the patient groups with and without atrial fibrillation
{kind=link}
{kind=link}
Risk of cardiovascular disease in the patient groups with and without atrial fibrillation (AF). (A) Cerebral cardiovascular events. (B) Stroke. (C) Coronary artery disease. (D) Heart failure. Adjusted HRs (95% CIs) were obtained using a multivariable Cox proportional hazards model with adjustments for age, sex (men), body mass index (BMI), HbA1c, smoking history (current or past), presence/absence of hypertension and/or dyslipidemia, use of aspirin, and duration of diabetes.
As the etiologies of stroke differ by the type of stroke (ischemic stroke, hemorrhagic stroke), we compared the risk factors for each subtype of stroke between the patient groups with and without AF. The results revealed no significant difference in the risk of ischemic stroke between the patient groups with and without AF (table 2, online supplemental figure S2).
The mortality rate in the patient group with AF was significantly higher than that in the patient group without AF. The mortality rates in the patient groups with and without AF were 49.34/1000 PY and 17.80/1000 PY, respectively, and the adjusted HR of all-cause death in the patient group with AF as compared with the group without AF was 1.82 (95% CI 1.24 to 2.67) (table 2, online supplemental figure S3).
In regard to the risk for hemorrhagic events also, there was no significant difference between the patient groups with and without AF (table 2, online supplemental figure S4). Furthermore, secondary analysis restricted to a 6-year follow-up period did not alter the main results (online supplemental figures S5−S11).
Conclusion
The findings of this study revealed that annually, 1 in 200 elderly Japanese patients with T2D develop AF. Elderly patients with T2D with AF showed a marked increase in the risk of mortality and absolute risk of cerebral cardiovascular events. Almost 1 in 20 patients die every year, and almost 1 in 30 patients annually develop cerebral cardiovascular events. In particular, the risk of coronary artery disease and heart failure in elderly patients with T2D with AF was twofold to fivefold higher than that in these patients without AF.
Our study is the first report of evaluation of the risk of AF in elderly Japanese patients with T2D and of the mortality and morbidity rates in these patients with AF using real-world data. Multiple large-scale cohort studies have reported a higher risk of AF in elderly patients and patients with T2D.9 10 One study from the USA using a large-scale claim database reported an age-adjusted and sex-adjusted incidence rate of AF of 9.1/1000 PY (95% CI 8.6 to 9.7).11 As compared with this figure, the incidence rate of AF in our study was relatively low. However, several studies suggested the existence of racial differences in the risk of AF. For example, one previous report from Japan suggested a lower incidence of AF in Japanese people as compared with western populations.12 Consistent with this notion, it has been reported that a single screening of subjects over 65 years of age from western countries was likely to yield 1.44% persons with new- onset AF,13 whereas a study from Japan reported identifying new-onset AF in only 0.45% (95% CI 0.30% to 0.64%) of persons with a mean age of 65 years and above.12 Considering that previous studies consistently reported a 1.3-fold to 1.6-fold higher risk of AF in patients with T2D,9 10 the incidence rate of AF in our elderly patients with T2D (5.14/1000 PY) seemed quite consistent with previous reports. In regard to the risk factors for AF, we could not identify any significant risk factors other than advanced age in our study; however, in view of the markedly increased risk of mortality and morbidity in elderly patients with T2D with AF, a careful follow-up of elderly patients with T2D for timely detection of AF and adoption of countermeasures for prevention of AF are definitely warranted.
The other important findings of our study are the markedly increased risk of death, coronary artery disease, and heart failure in elderly patients with T2D with AF. These results were also consistent with the results of the Action to Control Cardiovascular Risk in Diabetes study (ACCORD) study, a previously reported large-scale randomized controlled trial (RCT) from the USA. They reported that patients with T2D and new-onset AF had an HR of 2.65 for all-cause mortality (95% CI 1.8 to 3.86), an HR of 2.1 for myocardial infarction (95% CI 1.33 to 3.31), and an HR of 3.80 (95% CI 2.48 to 5.84) for the development of heart failure.14 As AF induces thrombosis and impairment of cardiac function and vice versa, it is quite conceivable that patients with AF are at an elevated risk for coronary artery disease and heart failure. On the other hand, our study did not reveal any statistically significant increase in the risk of ischemic stroke in elderly patients with T2D with AF, after adjustments for established risk factors for cerebral cardiovascular events. We are unable to explain this result, as AF is one of the major causes of ischemic stroke. It is possible that the small number of stroke events in our subjects masked any statistically significant increase of the risk. However, in view of the high incidence of stroke in patients with AF (17.93/1000 PY), very careful follow-up of elderly patients with T2D with AF is obviously necessary. Our study also revealed no significant difference in the risk for hemorrhagic events between the patient groups with and without AF. On the other hand, both T2D and advanced age are risk factors for bleeding in association with anticoagulant therapy, which is an established therapy for the prevention of stroke in patients with AF.15 However, in our study, only 44% of patients with AF had been prescribed an oral anticoagulant, in spite of the high stroke risk profile (data not shown). The low prescription rate of oral anticoagulants in our study is consistent with the report from the Japanese AF registry study, which also revealed a low prescription rate (64%) of oral anticoagulants among Japanese patients with AF (mean age: 74 years±11; underlying T2D: 23%).16 The low prescription rate of oral anticoagulants in our study cohort could be one of the reasons for the unexpected result of our study mentioned above.
Our study has several strengths, including the large sample size and long duration of follow-up. However, it also has potential limitations. First, for the diagnosis of AF, some patients with paroxysmal AF could be undiagnosed. Thus, there is the possibility that the risk of AF in elderly patients with T2D was underestimated. Second, the JPAD trial was designed as an RCT to evaluate the efficacy of low-dose aspirin in preventing CVD, but not in preventing AF; our sample size was probably insufficient for evaluation of the latter. Third, we did not measure some potential risk factor variables. For examples, carotid intima media thickness, pulse wave velocity, and ankle brachial index, indices of arteriosclerosis and arterial stiffness, were reported to be risk factors for CVD including AF, and these factors could be attested in our study.17 However, the additive predictive value of these indices for CVD is still under discussion and the addition of these arterial indices may modestly influence our results.18–20 Also, as we have comprehensively controlled for other risk factors for CVD including AF, the effects of such indices on our findings should be small if any. Fourth, new types of antidiabetic drugs (dipeptidyl peptidase 4 (DPP4) inhibitors or sodium-glucose cotransporter-2 (SGLT2) inhibitors) have been developed in the last decade, and the change of antidiabetic treatment may influence the risk of AF and other CVD. Especially, SGLT2 inhibitors are reported to have preventive effects of AF and other CVD.21 22 However, we could not evaluate the influence of these new types of antidiabetic drugs on the risk of AF and other CVD, as those drugs have been available since almost 10 years after the initiation of the JPAD2 cohort and a limited number of incident AFs were observed after these drugs were available in Japan. Therefore, it is possible that the incidence of AF and other CVD in patients with T2D will decrease in the future. However, due to the global ageing of the society and the pandemic of T2D, we need to pay relentless effort to prevent AF and other CVD in patients with T2D.
Nevertheless, no large-scale real-world data of the risk of AF and the mortality and morbidity rates in elderly patients with T2D with AF have been reported from Asia until now. Our study could, therefore, provide some important guidance to physicians to plan countermeasures for prevention of AF in elderly patients with T2D.
In conclusion, elderly patients with T2D with AF, as compared with the same patients without AF, appear to be at a significantly higher risk of development of CVD. Therefore, a careful follow-up of elderly patients with T2D is necessary for timely detection of new-onset AF and CVD.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Both the JPAD trial and the JPAD2 study were carried out in compliance with the Declaration of Helsinki, with the approval of the institutional review boards of the Graduate School of Medical Science, Kumamoto University (Ethics Board approval number: 1749) and Nara Medical University (Ethics Board approval number: 2212). All the study participants gave written informed consent for enrollment in the JPAD trial as well as the JPAD2 study. The JPAD trial is registered in ClinicalTrials.gov (identifier: NCT00110448).
Acknowledgments
We are indebted to the participants of the JPAD trial and JPAD2 study for their outstanding commitment and cooperation. We thank M Ohtorii (Institute for Clinical Effectiveness, Kyoto, Japan) for her role in the data management and statistical analyses. The authors also wish to thank M Nagahiro, M Okamoto, and M Aoyama (Kumamoto University, Kumamoto, Japan), and Y Wada, Y Kamada, and M Miyagawa (Nara Medical University, Kashihara, Japan) for their excellent secretarial assistance.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors TM accepts full responsibility for the work and/or the conduct of the study, had access to the data, and controlled the decision to publish. Guarantor: TM. Study design and conception: HO, YS, TM. Acquisition of data: SO, HS, MS, MN, ND, HJ, MW, IM. Data analysis: CM, TM. Interpretation of analysis: CM, HO, YS, SO, HS, MS, MN, ND, HJ, MW, IM, TM. Drafting of the manuscript: CM, TM. Manuscript review for scientific content: HO, YS, SO, HS, MS, MN, ND, HJ, MW, IM. Supervision: HO, YS, TM.
Funding This study was supported by JRISTA, The BMS/Pfizer Japan Thrombosis Investigator Initiated Research Program (CV185-729). The JPAD trial was supported by the Ministry of Health, Labour, and Welfare of Japan (H16-Junkanki-004, H26-Iryo-Ippan-012, H27-Junkanki-Ippan-001, and H28-ICT-Ippan-004). The JPAD2 cohort study was supported by the Japan Heart Foundation, and JSPS KAKENHI grants 26293159, 16H05297, 17K18278, and 18H03032.
Competing interests CM reports research grants from Morinaga. HO reports lecturer’s fees from Bayer, Bristol-Myers Squibb, and Towa; manuscript fee from Novartis. YS reports research grants from Actelion, Astellas, Astellas Amgen Bio Pharma, Bayer, CMIC, Daiichi Sankyo, EP‐CRSU, Japan Lifeline, Kowa, Mebix, Meditrix, Novartis, Ono, Roche Diagnostics, and Terumo; non-purpose research grants from Astellas, Chugai, Daiichi Sankyo, Fuji Yakuhin, Kowa, Kyowa Hakko Kirin, Medtronic, Mitsubishi Tanabe, MSD, Nihon Medi-Physics, Ono, Otsuka, Sanofi, Shionogi, Sumitomo Dainippon, Takeda, and Teijin; lecturer’s fees from Alnylam, Asahi Kasei, AstraZeneca, Bayer, Boehringer Ingelheim, Daiichi Sankyo, Eli Lilly, Janssen, Kowa, Mitsubishi Tanabe, MSD, Novartis, Ono, Otsuka, Pfizer, Taisho Toyama, Takeda, and Toa Eiyo; manuscript fees from Asahi Kasei and Novartis; advisory boards for Amgen, Bayer, Boehringer Ingelheim, Mitsubishi Tanabe, Novartis, Ono, Pfizer, and Roche Diagnostics. SO reports lecturer’s fees from AstraZeneca, Eli Lilly, Mitsubishi Tanabe, Novartis, Ono, Sumitomo Dainippon, and Takeda. HS reports a manuscript fee from Mochida. IM reports lecturer’s fees from Astellas, AstraZeneca, Bayer, Boehringer Ingelheim, Daiichi Sankyo, Kowa, Mitsubishi Tanabe, MSD, Ono, Shionogi, and Takeda. MN reports research grants from Bayer; lecturer’s fees from Astellas, Bayer, Boehringer Ingelheim, Daiichi Sankyo, Eisai, Kowa, Nippon Shinyaku, Ono, Otsuka, Pfizer, Sumitomo Dainippon, and Takeda. ND reports lecturer’s fees from Abbott, Actelion, Astellas, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, Daiichi Sankyo, Kowa, Medtronic, Mitsubishi Tanabe, MSD, Nippon Shinyaku, Novartis, Otsuka, Pfizer, and Takeda. HJ reports research grants from Astellas, AstraZeneca, Bayer, Boehringer Ingelheim, Chugai, Daiichi Sankyo, Eli Lilly, GlaxoSmithKline, MSD, Novo Nordisk, Ono, Pfizer, Sanofi, Sanwa Kagaku Kenkyusho, Shionogi, Taisho Toyama, and Takeda; lecturer’s fees from Abbott, Astellas, AstraZeneca, Bayer, Boehringer Ingelheim, Daiichi Sankyo, Eli Lilly, Kyowa Hakko Kirin, Mitsubishi Tanabe, MSD, Novo Nordisk, Sanofi, Sanwa Kagaku Kenkyusho, Taisho Toyama, Takeda, Teijin, and Terumo; manuscript fees from Novo Nordisk and Taisho Toyama. MW reports research grants from AstraZeneca, Eli Lilly, and Sanofi; lecturer’s fees from Abbott, Astellas, Astellas Amgen Bio Pharma, AstraZeneca, Bayer, Boehringer Ingelheim, Daiichi Sankyo, Eli Lilly, Kowa, Kyowa Hakko Kirin, Mitsubishi Tanabe, MSD, Novartis, Novo Nordisk, Ono, Otsuka, Sanofi, Sanwa Kagaku Kenkyusho, Sumitomo Dainippon, Taisho Toyama, Takeda, and Teijin. TM reports lecturer’s fees from AstraZeneca, Bristol-Myers Squibb, Daiichi Sankyo, Japan Lifeline, Kowa, Toray and Tsumura; manuscript fees from Bristol-Myers Squibb and Kowa; advisory board for Novartis and Teijin.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.