Article Text

Abstract
Introduction To analyze the associations of circulating C1q/tumor necrosis factor-related protein-3 (CTRP3) concentrations with several metabolic parameters and to investigate the possible role of CTRP3 in subjects with diabetic peripheral neuropathy (DPN).
Research design and methods A total of 347 participants were recruited in this study, and plasma CTRP3 concentrations were analyzed in subjects with DPN (n=172) and without DPN (non-DPN, n=175). The nerve conduction test and oral glucose tolerance test were performed, and Neuropathy Symptom Score (NSS)/Neuropathy Disability Score (NDS) and biochemical parameters were measured in all participants.
Results Plasma CTRP3 concentrations were significantly lower in patients with DPN compared with those in patients with diabetes without DPN (p<0.01), despite the comparable glucose and lipid metabolism levels in both groups. Groups with a higher plasma CTRP3 level had a faster nerve conduction velocity. In addition, plasma CTRP3 concentrations were negatively correlated with hemoglobin A1c (HbA1c), urea acid (UA), triglyceride, NSS and NDS (p<0.05) after being adjusted for age and sex. Multivariate logistic regression analysis revealed that plasma CTRP3 concentrations were significantly correlated with DPN after being controlled for age, sex, body mass index, HbA1c, blood pressure, lipid profiles, and renal function.
Conclusions Plasma CTRP3 concentrations were significantly lower in patients with DPM and positively correlated with nerve conduction velocity. The relationship between CTRP3 levels and DPN is independent of the glucose and lipid status. Therefore, circulating CTRP3 might serve as a predictor of impairment of nerve conduction in patients with DPN.
- diabetes complications
- diabetic neuropathies
- glucose
- lipids
Data availability statement
Data sharing not applicable as no datasets generated and/or analyzed for this study.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
According to previous reports, more than half of patients with diabetic peripheral neuropathy (DPN) were underdiagnosed because the diagnostic tools are relatively time-consuming and costly.
The development of DPN is deeply associated with an increased inflammation burden.
What are the new findings?
Plasma C1q/tumor necrosis factor-related protein-3 (CTRP3) concentrations were significantly lower in patients with DPN and positively correlated with nerve conduction velocity.
The relationship between CTRP3 levels and DPN is independent of glucose and lipid status.
How might these results change the focus of research or clinical practice?
Circulating CTRP3 might serve as a predictor of impairment of nerve conduction in patients with DPN.
Introduction
Diabetes mellitus is a pandemic disease worldwide, and the prevalence of it is rising rapidly. It is anticipated that more than 700 million patients with diabetes would be diagnosed by the year 2045.1 More importantly, the incidence of several chronic diabetes complications is increasing as well.2 Among these complications, diabetic peripheral neuropathy (DPN) is the major one.3 DPN not only induces series of symptoms of sensory and motor neuropathy but also contributes to the pathology of diabetic foot, the most common cause of amputations.3 4 It is strongly associated with increased mortality, lower-limb amputations and distressing painful neuropathic symptoms in diabetes.5 Epidemic data showed that the prevalence of DPN is estimated to be 28.0% in the type 2 diabetes mellitus (T2DM) group, much higher than that in normal glucose tolerance population, which is 7.4%.5 6 Currently, the diagnosis of DPN mainly depends on neuronal conduction velocity (NCV) testing, as it is time-consuming and costly, and thus more than half of patients with DPN were underdiagnosed according to previous reports.7 8 Moreover, the therapeutic options for DPN are limited due to a poor understanding of its mechanisms.
The structural or functional abnormity of the axon and its associated Schwann cells, neuron perikarya, are the dominant sites injured in DPN.9 Polyol pathway, hexosamine and protein kinase C pathway, accumulation of advanced glycation end products (AGEs) in the diabetic nerve, excess glucose and/or fatty acid flux, insulin resistance are now regarded as the possible mechanisms involved in DNP, which cause vasoconstriction, hypoxia, loss of neurotrophic support, increasing oxidative stress and inflammation, decreasing gene expression of essential proteins, blocked protein synthesis and finally lead to the presentation and development of DPN.10 However, although more and more glucose-lowering agents have been used in clinical therapy, patients with diabetes still presented substantially high cumulative incidence of DPN,6 suggesting that there must be other mechanisms involved in its pathology.
Abundant pieces of evidence showed that both type 2 diabetes11 12 and its chronic complications were deeply associated with increased inflammation burden.13–15 Inflammation is involved in the development of DPN too. Therefore, anti-inflammatory factors are predicted to be inversely correlated with the development of DPN. C1q/tumor necrosis factor-related protein-3 (CTRP3), also name as CORS26 (collagenous repeat-containing sequence of 26 kDa protein), is identified as an anti-inflammatory factor and belongs to the CTRPs family.16 CTRP3 is expressed at a similar level in solid organs and tissues such as the lungs, kidneys and colon and even stronger in the aorta, bone marrow, thyroid gland, and urinary bladder.17 Previous studies have demonstrated that CTRP3 exerts roles in lipid metabolism, insulin resistance, and energy expenditure.16 18 Specifically, CTRP3 can reduce the release of proinflammatory monocyte chemoattractant protein-1 and exhibit anti-inflammatory effects on Lipopolysaccharide (LPS)-induced inflammatory reaction in mature 3T3-L1 adipocytes;19 the circulating concentration of CTRP3 was decreased in obese patients and with diabetes,20 and its deficiency significantly upregulated the expression of adipogenesis and gluconeogenic genes.20 These findings suggest a critical regulatory effect of CTRP3 in metabolic diseases. Recently, several studies revealed its effects on neuroprotection. Wang et al21 found that CTRP3 alleviated brain edema, protected against disruption of the blood–brain barrier, improved neurological functions via Adenosine 5‘-monophosphate (AMP)-activated protein kinase (AMPK)/hypoxia inducible factor-1/vascular endothelial growth factor-dependent pathway in intracerebral hemorrhage rats; another study demonstrate that CTRP3 enhanced the axon growth rate of spinal muscular atrophy motor neurons via the mammalian target of rapamycin signaling.22 According to studies above, we deduce that CTRP3 might have a potential role in DPN.
In this report, we conducted a cross-sectional trial in patients with diabetes to evaluate the relationship between circulating CTRP3 and DPN-related parameters, and attempt to identify if serum CTRP3 has a role in patients with DPN.
Methods
Subjects and exclusion criteria
A total of 347 patients with T2DM were recruited in our study (175 without DPN, 173 with DPN). T2DM was diagnosed according to the American Diabetes Association (ADA) guidelines.23 All patients accepted oral anti-diabetic agent and/or insulin therapies according to their physician’s prescription.
The overall exclusion criteria are as follows: (1) acute complications of diabetes; (2) stage 2 or above hypertension (resting blood pressure ≥160/100 mm Hg); (3) history of cardiovascular and cerebrovascular diseases (myocardial infarction, cardiovascular revascularization, unstable angina, or stroke); (4) acute inflammatory diseases as determined by clinical symptom of infection, or blood leukocyte >7 ×109/L; (5) active renal or hepatic disease, and systemic corticosteroid treatment within the past 6 months; (6) currently pregnant and breastfeeding.
Study measurements
Clinical parameter evaluations of participants
Clinical parameters were assessed according to previous studies.24 In detail, height, weight, and blood pressure were evaluated using standard protocols by trained investigators. Height was measured to minimum recorded unit of 0.1 cm, body weight was measured to an accuracy of ±0.2 kg, blood pressure was measured twice by a standard mercury manometer. Then, the body mass index (BMI) was calculated according to standardized formula.
Blood samples were collected after an overnight fasting for assessment of hemoglobin A1c (HbA1c), triglyceride (TG), total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), high-sensitive C reactive protein (hsCRP), blood urea nitrogen (urea), creatinine (Cr), uric acid (UA), alanine aminotransferase (ALT), and aspartate aminotransferase (AST). All of the blood samples were separated within 30 min, stored at – 20°C before used, and tested within 1 month. All biochemical indicators were detected by biochemical auto analyzer (Beckman CX-7 Biochemical Autoanalyzer, Brea, California, USA).
Oral glucose tolerance test (OGTT)
OGTT was performed according to previous studies. Briefly, after an 8-hour overnight fasting, a glucose solution (contain 75 g glucose) was ingested within 5 min by each subject and blood samples were obtained at 0 and 120 min for glucose concentration assessment.
Neuropathy Symptom Score/Neuropathy Disability Score (NSS/NDS) evaluation
NSS/NDS was assessed in each participant according to previous studies. Generally, NSS was used to evaluate symptoms of neuropathy including unsteadiness in walking, numbness, burning or tingling, fatigue, cramping, aching, prickling sensations, and its values ranged from 0 to 9, and a value ≥5 was defined as neuropathy. The NDS includes ankle reflex, vibration, temperature and pinprick, and its values ranged from 0 to 10, and a value ≥6 was defined as neuropathy.
Nerve conduction testing
Nerve conduction testing was performed by electromyography/evoked potential equipment (NDI-092, Shanghai, China) according to manufacturer’s instructions. The tests were conducted by one neurologist on the same equipment for all participants. The results were processed according to reference values accepted by our electromyogram laboratory and were used to verify the diagnosis of DPN.
Confirmation of DPN
DPN was diagnosed according to the criteria issued by Toronto diabetic neuropathy expert group.25 In brief, confirmed DPN was defined as the presence of abnormalities of nerve conduction and NSS or NDS scores.
Assessment of plasma CTRP3 levels
The plasma CTRP3 concentrations were determined by ELISA with specific antibody against CTRP3 (Proteintech, Wuhan, China) according to standard protocols. All samples were run in duplicate and repeated if there was a >15% difference between duplicates. No significant cross-reactivity or interference was observed.
Related calculation formula
BMI formula is weight in kilograms divided by height in meters squared.
Statistical analysis
All analyses were performed by SPSS V.21 (IBM). Data were expressed as mean values±SD. Before statistical analysis, non-normally distributed parameters were logarithmically transformed to an approximate normal distribution. An independent-sample t-test was used to compare continuous variables between the two groups. Differences among multiple groups were tested by analysis of variance for continuous variables. Interrelationships between variables were analyzed by Spearman’s correlation test and partial correlation test (adjusted by age and sex). The associations of CTRP3 and DPN were examined by multivariate logistic regression analysis, respectively. P values <0.05 were considered to be statistically significant.
Results
Clinical characteristics of all participants
As shown in table 1, a total of 347 participants were recruited in our study, including 202 (58.2%) male and 145 (41.8%) female (p=0.051). All subjects were divided into two groups (non-DPN and DPN). The average age was older and the duration of diabetes was longer in the DPN group than that in the non-DPN group (table 1). BMI, HbA1c, FPG and 2-hour post challenge plasma glucose (2hPG), TC, TG, HDL-c and LDL-c, acute inflammatory marker and hepatic function were comparable between non-DPN and DPN groups (table 1). While blood pressure, urea and Cr were significantly increased in the DPN group compared with the non-DPN group (table 1). Moreover, scores of nerve symptoms assessed by NSS and NDS were higher in patients with DPN as supposed (table 1).
Clinical and laboratory characteristics of study participants
Circulating CTPR3 levels were decreased in DPN and positively correlated with nerve conduction velocity
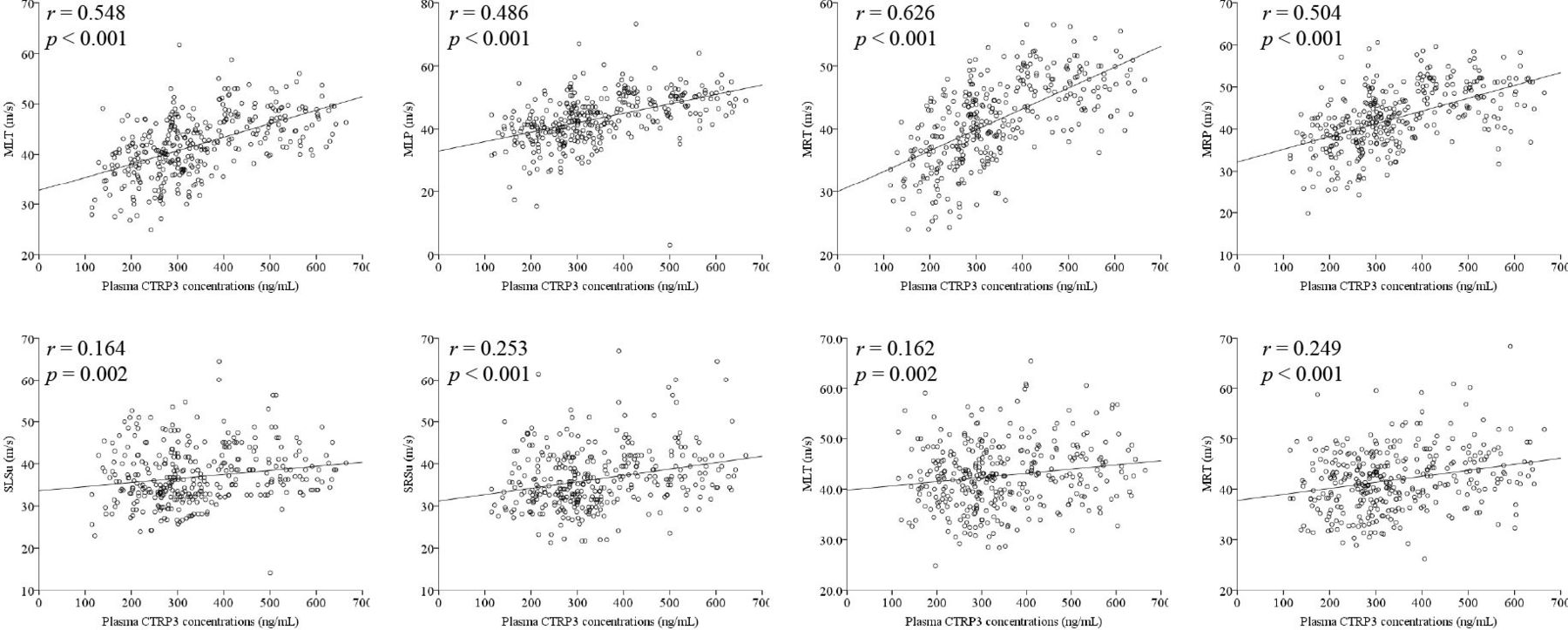
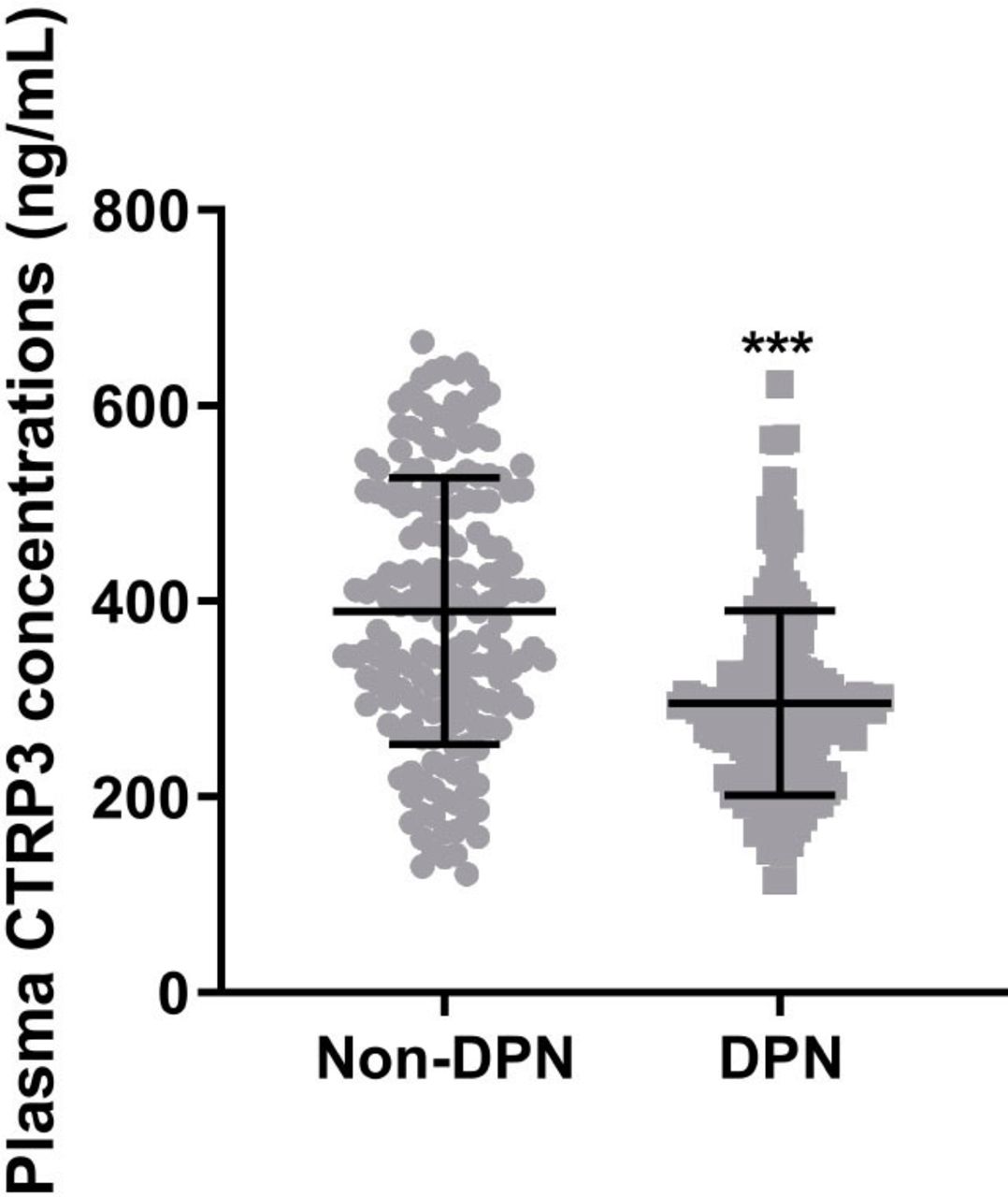
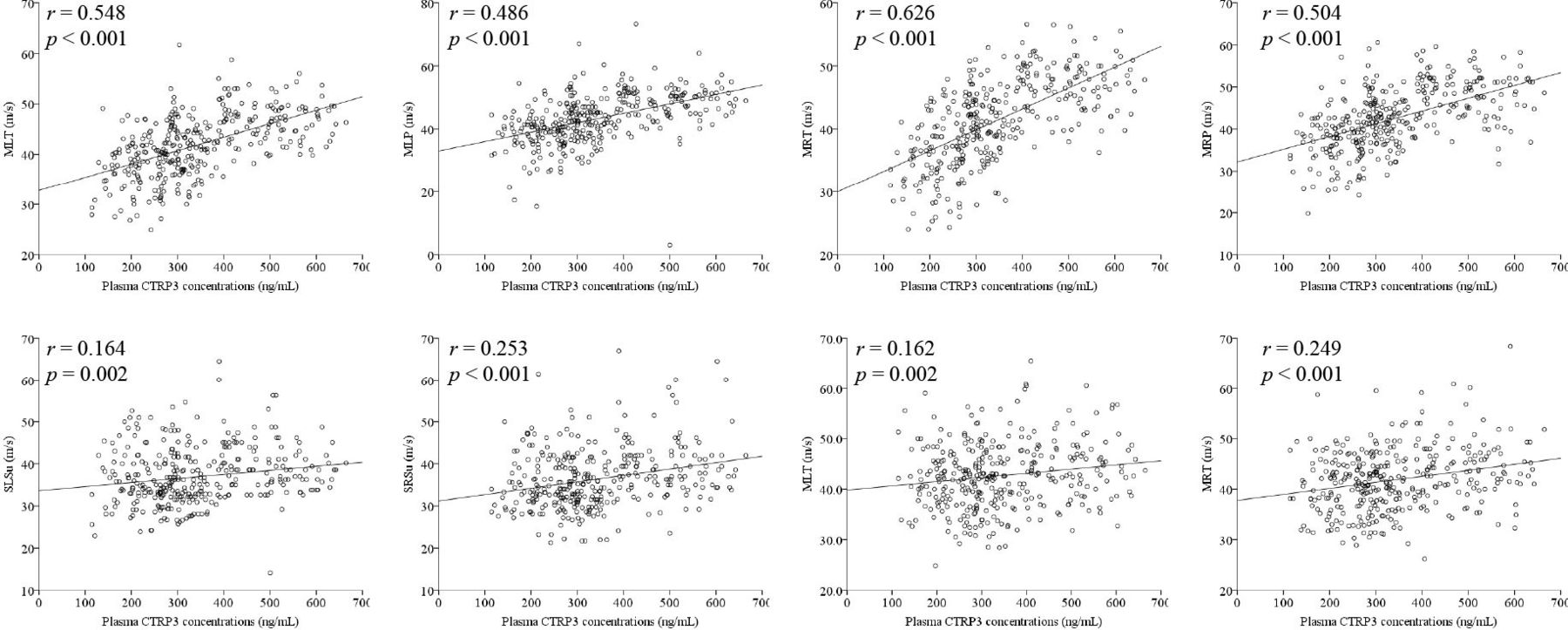
We measured the levels of plasma CTRP3 in both groups. The average concentration of plasma CTRP3 in the DPN group is 295.8±94.2 ng/mL, which was markedly lower than that of 389.8±136.2 in the non-DPN group (p<0.001, figure 1). Next, we conducted subgroup analysis by dividing all participants into four groups, that is, G1: non-DPN; G2: probable DPN (only clinical abnormalities); G3 subclinical DPN (only abnormal NCV); G4: confirmed DPN (both clinical and NCV abnormalities), and CTRP3 concentrations were assessed in these groups. Our results revealed that CTRP3 levels were lowest in G4, followed by G3 and G2, which have comparable CTRP3 concentrations. Subjects in G1 showed the highest level of CTRP3 (online supplemental figure 1). To further assess the association between CTRP3 levels and nerve conduction impairment, we divided all participants into three groups according to tertiles of plasma CTRP3 concentrations (tertile 1: <274.6; tertile 2: 274.6–385.5; tertile 3: >385.5 ng/mL). We found that both motor and sensory nerve conduction velocity of tibia and peroneal nerve increased in the second and (or) third tertiles of CTRP3 levels (table 2), whereas sensory nerve conduction of sural nerve and right tibia nerve did not apparently alter in all tertiles (p>0.05, table 2). Moreover, Pearson’s correlation analyses showed that CTRP3 concentrations were positively correlated with both motor and sensory nerve conduction velocity (figure 2). These results indicated that CTRP3 might play a role in diabetes-related nerve conduction impairments.
Supplemental material
The results of the nerve conduction testing from groups divided according to plasma CTRP3 tertiles

Plasma C1q/tumor necrosis factor-related protein-3 (CTRP3) concentrations in patients without diabetic peripheral neuropathy (non-DPN) and with DPN. Data are presented as means±SD; ***p<0.001 compared with non-DPN.
{kind=link}
{kind=link}
Scatter plots showing the correlations of plasma C1q/tumor necrosis factor-related protein-3 (CTRP3) concentrations with nerve conduction parameters. The correlations were assessed by Pearson’s correlation test. M represents motor, S represents sensory, L represents left, R represents right, T represents tibia, P represents peroneal and Su represents sural.
Association of plasma CTRP3 levels with anthropometric and biochemical parameters in DPN
Further, we investigated the association of circulating CTRP3 concentrations with anthropometric and biochemical parameters. Plasma CTRP3 concentrations were negatively correlated with HbA1c, NSS and NDS (table 3). Intriguingly, after adjusting for age and sex, we found that the negative correlations of CTRP3 with TG and UA became meaningful too (table 3); besides, the relationships with three other factors mentioned above remain significant.
Spearman and partial correlation of variables associated with circulating CTRP3
Multivariate logistic regression analysis revealed that plasma CTRP3 concentrations were inversely correlated with DPN after being controlled for age, sex, BMI, blood pressure, HbA1c, lipid profiles and renal functions (online supplemental table 1).
Discussion
The main findings of the present study indicated that CTRP3 could be a useful marker in evaluation of DPN in subjects with diabetes. Its concentrations were obviously reduced in patients with DPN compared with non-DPN diabetic patients. Further subgroup and association analysis showed that circulating CTRP3 concentration was related to glucose, and more importantly, firmly related to nerve symptoms and conduction velocity. Our findings suggested that CTRP3 maybe a possible solution to inverse the situation of DPN and then prevent it from diabetic foot ulcer, amputation or other secondary complications.
CTRP3 is a widely studied adipokine recently for its functions in many diseases. By injecting CTRP3 into the mice with fracture, the researchers found that CTRP3 promoted the recovery of fracture via altering callus maturation and remodeling.26 In severe acute pancreatitis mouse model, CTRP attenuated pathological lesion, inhibited inflammatory mediator and repressed acinar cell apoptosis.27 Within coronary artery disease (CAD), CTRP3 alters both development and progression of CAD by modulating metabolic pathways, influencing immuno-inflammatory response, and regulating cardiovascular functions.28 Further, many studies identified that CTRP3 functions in metabolic diseases, especially in diabetes mellitus and its complications. Cross-sectional human studies, animal models, cell biological experiments support that CTRP3 have a significant role in diabetic retinopathy,29 30 diabetic cardiomyopathy,31 diabetic nephropathy32 33 via various mechanisms; overexpression of CTRP3 may improve the prognosis of these diabetes complications in multiple ways. However, the relationship of CTRP3 with DPN is not fully understand. CTRP3 was previously revealed to be an anti-inflammatory adipokine that inhibits proinflammatory pathways mediated by LPS-like and Toll-like receptor in monocytes and adipocyte.34 Recent study also found that CTRP3 may exert vasculoprotective effects via the adiponectin receptor 1/AMPK/eNOS-dependent/NO pathway.35 All these data suggest that CTRP3 may have a role in the progress of DPN as its positive functions identified in other tissues or organs. In the current study, we identified that CTRP3 concentration was inversely associated with DPN and its symptoms, while positively related to the nerve conduction velocity. Therefore, these findings supported the possible clinical utility of CTRP3, as a potential index for early diagnosis and severity classification of DPN. Then, patients can get a timely and effective treatment before DPN gets worse, which may not only reduce the disability rate and mortality but also lighten the economic burden of the countries and families with diabetes.
In fact, several previous studies tried to find biomarkers for the early diagnosis of DPN and other microvascular complications of diabetes. Qiao et al36 showed that serum phosphorylated neurofilament-heavy chain level was higher in type 2 diabetic patients with DPN compare with non-DPN subjects. Li et al37 reported serum neuron-specific enolas (NSE) levels were closely associated with DPN. Jakob et al7 demonstrated that myelin protein zero cmRNA and neurofilament light chain protein may have a diagnostic value in DPN. In addition, brown adipose tissue-released cytokine neuregulin and visceral adipose tissue-released cytokine omentin were revealed as predictors of both type 2 diabetes and its microvascular complications.38–41 Our results may provide a new biomarker to predict DPN and a new way to explore the mechanism of DPN. Further studies are warranted to further clarify their diagnostic effectiveness and roles in DPN or other complications of diabetes.
There are several limitations to be stated. First, the causal relationship between circulating CTRP3 concentration and DPN could not be concluded due to the cross-sectional design, and further animal models and cell biological experiments are needed to identify the concrete character of CTRP3 in DPN. Second, the prevalence of both nephropathy and retinopathy were not evaluated in the current study. While CTRP3 plasma concentrations might be affected by various factors, including renal functions, which were decreased in the DPN group. Nevertheless, after adjusting age and sex in our correlational analysis, urea and creatinine were not associated with circulating CTRP3 concentration in the current population.
In conclusion, our study identified plasma CTRP3 concentration as a potential indicator for DPN and its severity, although further studies are needed to demonstrate the effects and mechanism that underlie CTRP3 and DPN.
Data availability statement
Data sharing not applicable as no datasets generated and/or analyzed for this study.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Ethics Committee of Chongqing University Central Hospital (no. 2021-55). Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
KL, LY and YX contributed equally.
Contributors KL, LY, WZ, and KF acquired data, analyzed data and made statistical analysis. BD and KL wrote and edited the manuscript. LY, YX and KL did the interpretation of data and revised the manuscript. BD and KL researched data, drafted and revised the manuscript, obtained study funding, and supervised the study. KL and BD are the guarantors of this work and, as such, take full responsibility for the work and had access to the data, and controlled the decision to publish. All authors have read and approved the manuscript for publication.
Funding This work was supported by grants from basic research and frontier exploration project of Yuzhong District, Chongqing (No. 20200143).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.