Article Text

Abstract
Introduction Sodium–glucose cotransporter 2 (SGLT2) inhibitors are now recommended in guidelines for persons with type 2 diabetes mellitus (T2DM) and at risk of advanced kidney disease as part of the glucose-lowering regimen.
Research design and methods To explore the optimal threshold at which to initiate SGLT2 inhibitor therapy, we conducted an observational study analyzed under a counterfactual framework. This study used the electronic healthcare database in Japan, comprising data from approximately 20 million patients at approximately 160 medical institutions. Persons with T2DM with an estimated glomerular filtration rate (eGFR) ≥ 30 mL/min/1.73 m2 in April 2014 were eligible. The primary end point was the composite of renal deterioration (>40% decline in eGFR) and the development of eGFR<30 mL/min/1.73 m2. We estimated the risk of the composite end point occurring over 77 months in different scenarios, such as early or delayed intervention with SGLT2 inhibitors for uncontrolled diabetes at different hemoglobin A1c (HbA1c) thresholds. The parametric g-formula was used to estimate the risk of the composite end point, adjusting for time-fixed and time-varying confounders.
Results We analyzed data from 36 237 persons (149 346 person-years observation), of whom 4679 started SGLT2 inhibitor therapy (9470 person-years observation). Overall, initiating SGLT2 inhibitor therapy was associated with a 77-month risk reduction in the end point by 1.3–3.7%. The largest risk reduction was observed within 3 months of initiation once the HbA1c level exceeded 6.5% (risk reduction of 3.7% (95% CI 1.6% to 6.7%)) compared with a threshold of 7.0% or higher.
Conclusions Our analyses favored early intervention with SGLT2 inhibitors to reduce the renal end point, even for persons with moderately controlled HbA1c levels. Our findings also suggest caution against clinical inertia in the care of diabetes.
- Pharmacoepidemiology
- Nephrology
Data availability statement
Data may be obtained from a third party and are not publicly available. Data sharing is not allowed by the data provider. For inquiries regarding our data set, please contact the Real World Data Co., Ltd. (Kyoto, Japan).
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Sodium–glucose cotransporter 2 (SGLT2) inhibitors are currently recommended in guidelines for persons with type 2 diabetes mellitus who are at risk of advanced kidney disease as part of the glucose-lowering regimen.
The optimal threshold for introducing SGLT2 inhibitors for patients with diabetes to maximize the renoprotective effect is unknown.
WHAT THIS STUDY ADDS
In this hypothetical intervention using retrospective observational data of 36 237 patients in Japan, early introduction of SGLT2 inhibitors at a hemoglobin A1c level ≥6.5% yielded the largest risk reduction of renal disease progression among 12 different strategies investigated.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
Our analyses favored early intervention with SGLT2 inhibitors to reduce renal worsening and suggest caution against clinical inertia in the care of diabetes.
Introduction
The advent of sodium–glucose cotransporter 2 (SGLT2) inhibitors mirrors a major advance for persons with type 2 diabetes mellitus (T2DM) who are at risk of advanced kidney disease.1,2 The renal benefit of SGLT2 inhibitors has been consistently shown in clinical trials and observational studies using real world data. 3–8 In clinical guidelines, SGLT2 inhibitors are now listed as the second-line therapy for persons with T2DM, and an estimated glomerular filtration rate (eGFR) >30 mL/min/1.73 m2 is considered secondary prevention for diabetic kidney disease.9
In a recent placebo-controlled trial, dapagliflozin showed a favorable effect on kidney outcomes among patients with chronic kidney disease, regardless of the presence or absence of T2DM.10 Another trial, EMPA-KIDNEY, is ongoing to examine whether empagliflozin prevents worsening of kidney disease among persons who have chronic kidney disease with or without T2DM.11 These results indicate that, in the future, the SGLT2 inhibitor class could be used for persons with T2DM, regardless of glycemic control (or even for persons without diabetes); as of September 2021, dapagliflozin already had the authorized indication for non-diabetic persons with kidney disease.12–14 Until the expanded indication is approved for other agents, persons with poorly controlled T2DM were most likely to be candidates for add-on SGLT2 inhibitor therapy. However, it is uncertain at what glycemic level SGLT2 inhibitors should be initiated to optimize renal outcomes for persons with T2DM or whether renal outcomes differ depending on the timing of SGLT2 inhibitor introduction. This topic is clinically relevant, given that glycemic control is one of the key components in preventing progression towards end-stage renal disease.7
This study aimed to explore the optimal threshold of hemoglobin A1c (HbA1c) for intervention with SGLT2 inhibitor therapy for persons with T2DM under several hypothetical scenarios using observational data.
Research design and methods
Data source
This study used the RWD database, an electronic healthcare database in Japan, the details of which are reported elsewhere.6 15 This database collects the records of ~20 million patients from ~160 medical institutions in Japan. The stored information includes demographic data, diagnoses, prescriptions, and laboratory results from both outpatient and inpatient encounters. The data were automatically extracted from electronic health records at each medical institution. Patient records are maintained by assigning unique identifiers for each patient, which are valid only within the same institution. The diagnoses were recorded as International Statistical Classification of Diseases and Related Health Problems, 10th Revision (ICD-10) codes, and the prescription records were kept in Anatomical Therapeutic Chemical codes.
The last available date of patient records varied across institutions, with a rapid decline in the number of records after September 2020; this was largely due to an administrative reason of the database holder, such as the COVID-19 pandemic.
Patient criteria
Eligible patients were prevalent users of diabetic medication with a diagnosis of diabetes in April 2014 (the index date), when the first SGLT2 inhibitor was available in Japan. We defined prevalent users as patients with at least one prescription record of a glucose-lowering agent (except for SGLT2 inhibitors) within 180 days of the index date. As disease coding practices in Japan were not sensitive enough to capture T2DM cases,6 we used a broader case definition by ICD-10 codes including both E11 (‘diabetes mellitus, type 2’) and E14 (‘diabetes, unspecified’), unless other specific types of diabetes were concurrently coded (eg, E10 representing type 1 diabetes). Other inclusion criteria were persons aged ≥20 years at the index date; persons whose laboratory data were available both within 90 days prior to the index date and after the index date; and eGFR >30 mL/min/1.73 m2 at the index date. To identify prescriptions for diabetic medication, the Anatomical Therapeutic Chemical code A10 was used. No specific exclusion criteria were prepared.
Hypothetical intervention
We conducted several hypothetical interventions under a potential outcome framework, also known as the counterfactual framework (figure 1).16 17 This framework requires three assumptions—positivity, conditional exchangeability, and consistency—for computation of the probability of an outcome occurring (Supplemental Methods in online supplemental file 1). These assumptions were statistically untestable,17 and whether such assumptions would hold depends on the clinical context. For example, this study assumed that at each medical encounter, individuals who did and did not initiate SGLT2 inhibitors were exchangeable conditional on the variables of age, sex, HbA1c, and medication history other than SGLT2 inhibitors. Intuitively explained, if the outcomes differed between two exchangeable populations, the difference likely resulted from SGLT2 inhibitor use. As a per-protocol effect,18 we assume that all persons who meet the criteria for initiating SGLT2 inhibitor therapy did start pharmacologic treatment and that SGLT2 inhibitors were sustained once they were started except for censoring. The estimated effect was analogous to that obtained from per-protocol analysis in a clinical trial.
Supplemental material
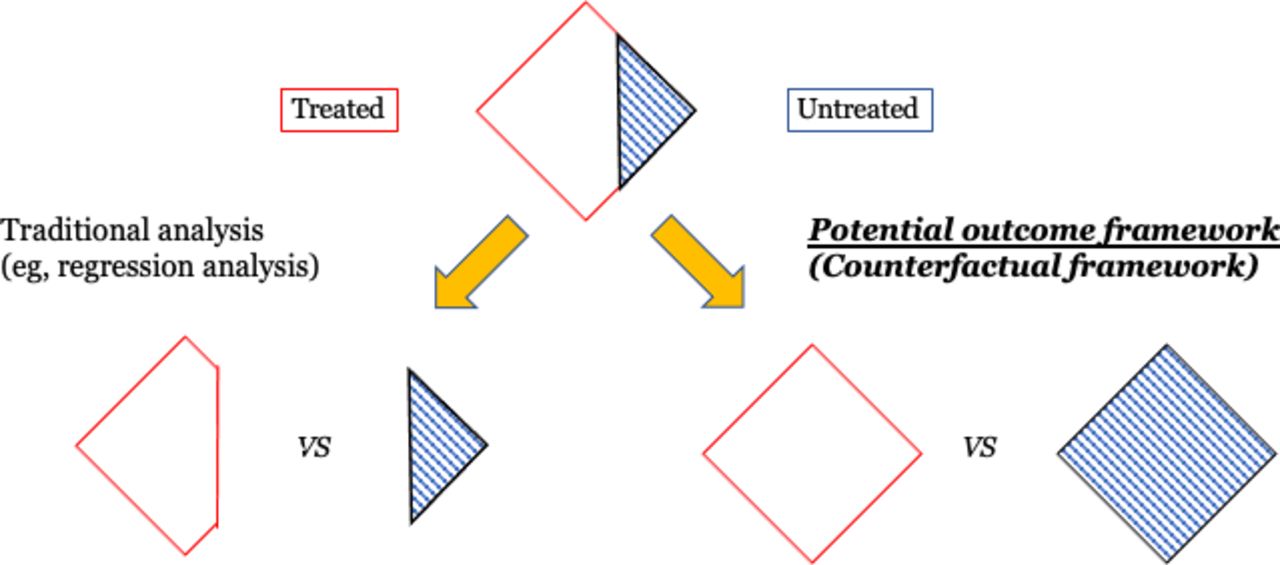
Illustrative scheme of the counterfactual framework.
Our de novo research question was ‘If the timing of introducing SGLT2 inhibitors differed in people with T2DM, what would have been observed with respect to worsening renal risk?’. As such, we prepared the primary hypothetical intervention to introduce SGLT2 inhibitors for all persons once their HbA1c level exceeded 7.0%. The probability of a hypothetical outcome occurring was compared with that of the natural course, a model-based simulation of observed data. The interval between HbA1c measurement and SGLT2 inhibitor initiation was primarily set at 3 months, which was changed to 6 months, 9 months and 12 months in the sensitivity analysis. This mirrors the scenario of initiating SGLT2 inhibitors within 3 months (or 6 months, 9 months and 12 months) after HbA1c exceeds ≥7.0%. In addition, the threshold of HbA1c was changed to 6.5% and 7.5% in the sensitivity analyses; the same four intervals were tested.
Outcome
The outcome of interest was the incidence of sustained renal worsening, defined as either1 a >40% decline in eGFR from the baseline value19 or2 eGFR <30 mL/min/1.73 m2. For both measures, at least two measurements ≥30 days apart were required to define sustained deterioration. The value of eGFR was calculated with the following equation using the serum creatine value at the visit: eGFR (mL/min/1.73 m2)=194 × creatine –1.094 (mg/dl)×age–0.287 (years) (×0.739 for women).
This formula was modified from the original Modification of Diet in Renal Disease equation, given the body composition of the Japanese population.20
Statistical analysis
Descriptive statistics were used to summarize patient characteristics. The crude annual eGFR slope was estimated by a mixed-effects linear model accounting for within-person clustering.
Under the potential outcome framework, the parametric g-formula was used to estimate the probability of outcome occurrence for each hypothetical intervention.21–23 In daily clinical practice, patient conditions, namely, glycemic control and medications, can vary over time. The parametric g-formula is among the procedures accounting for such time-varying confounders.24 We modeled age, sex and the grade of renal function at the index date as time-fixed covariates, whereas HbA1c at each visit and exposure histories to other diabetic medications were accounted for as time-varying covariates. The estimates obtained using the parametric g-formula should be viewed as the population-level effect.
The observation started in April 2014, and all patients were assumed to be followed through September 2020 except for censoring due to death. Unlike traditional survival analysis, loss to follow-up is not treated as censoring in the parametric g-formula; data after loss to follow-up are modeled from the data of patients who remain in the cohort.22 However, in the preliminary analysis, we noticed model instability when incorporating data after September 2020, when the patient population size rapidly declined. For this reason, we truncated patient data as of September 30, 2020. In this study, death was the competing event for the renal outcome; thus, data were censored at the time of death (if it occurred). The follow-up was monthly; if visit records were missing, the data, including medication and laboratory results, were carried forward from the last visit (until the next visit).
All statistical analyses were conducted using the R statistical environment (V.4.10). We also relied on the gfoRmula R package (V.0.32) for g-formula estimation.25 Non-parametric bootstrapping with 200 samples was used to compute the 95% CI. The 95% CI did not cross a null effect; it was considered statistically significant.
Sensitivity analysis
Our study primarily included persons whose baseline eGFR was ≥30 mL/min/1.73 m2. We added a sensitivity analysis that included persons with a baseline eGFR of ≥45 mL/min/1.73 m2. This was because there was caution—though not contraindicated—against SGLT2 inhibitor use for persons with an eGFR of <45 mL/min/1.73 m2 in the package insert of some SGLT2 inhibitors.26 27 This means that persons whose eGFR was <45 mL/min/1.73 m2 were less likely to receive SGLT2 inhibitor therapy, and this situation might correspond to the near violation of the positivity assumption. This was a post hoc analysis, reflecting the discussion among the authors.
Furthermore, four sensitivity analyses were added as recommended by the journal reviewers. First, the outcome was changed to the eGFR change (ie, a continuous variable) at the end of follow-up. Second, the inclusion criteria were expanded to persons whose baseline eGFR was ≥20 mL/min/1.73 m2. These criteria were modified because SGLT2 inhibitors are not necessarily contraindicated to persons with an eGFR <30 mL/min/1.73 m2 in Japan, and it is possible that such persons can use the SGLT2 inhibitors. The lower threshold of 20 mL/min/1.73 m2 was determined by the authors to be compatible with the inclusion criteria of a previous randomized controlled trial28 and the package insert of empagliflozin in Japan.29 Third, the model was further adjusted by antihypertensive drug use and ACE inhibitor/angiotensin II receptor blocker use as time-varying confounders. Because blood pressure records for each person were lacking, this analysis was performed as a sensitivity analysis because of the concern for potential model misspecification. Finally, we conducted benchmark analyses to illustrate how the g-formula worked in the case examples of dipeptidyl peptidase-4 (DPP-4) inhibitors and glucagon-like peptide-1 (GLP-1) receptor agonists, instead of SGLT2 inhibitors. A similar analytic framework to that of the primary analysis was adopted in these sensitivity analyses.
Results
Characteristics of the cohort
A total of 36 237 persons were included in the analysis. The median age at the index date of April 2014 was 70 (IQR: 63–78) years, and men accounted for 62.7% (22 713/36 237) of the cohort. The baseline eGFR was 67.3 (median, IQR: 54.2–80.9) mL/min/1.73 m2. The baseline data of quantitative urinary albumin-creatinine ratio was available in 11 165 persons, of which the median value was 20.6 (IQR: 8.6–73.0) mg/gCr. There were 4315 recorded deaths at a median of 27 months after the index date. Overall, the study cohort contributed 149 346 person-years of observation, with the longest observation being 77 months. The most commonly used glucose-lowering drug at the index date was DPP-4 inhibitors (55.5%), followed by biguanides (37.2%) and sulfonylureas (34.1%). The median HbA1c value was 7.0%, with an IQR of 6.4%–7.7%. During the study period, 4679 persons (12.9%) started SGLT2 inhibitor treatment, and they contributed 9470 person-years of observation. Regarding the renal outcome, the crude overall decline in the eGFR was 0.80 (SE: 0.011) mL/min/1.73 m2 annually, and one patient developed end-stage renal disease.
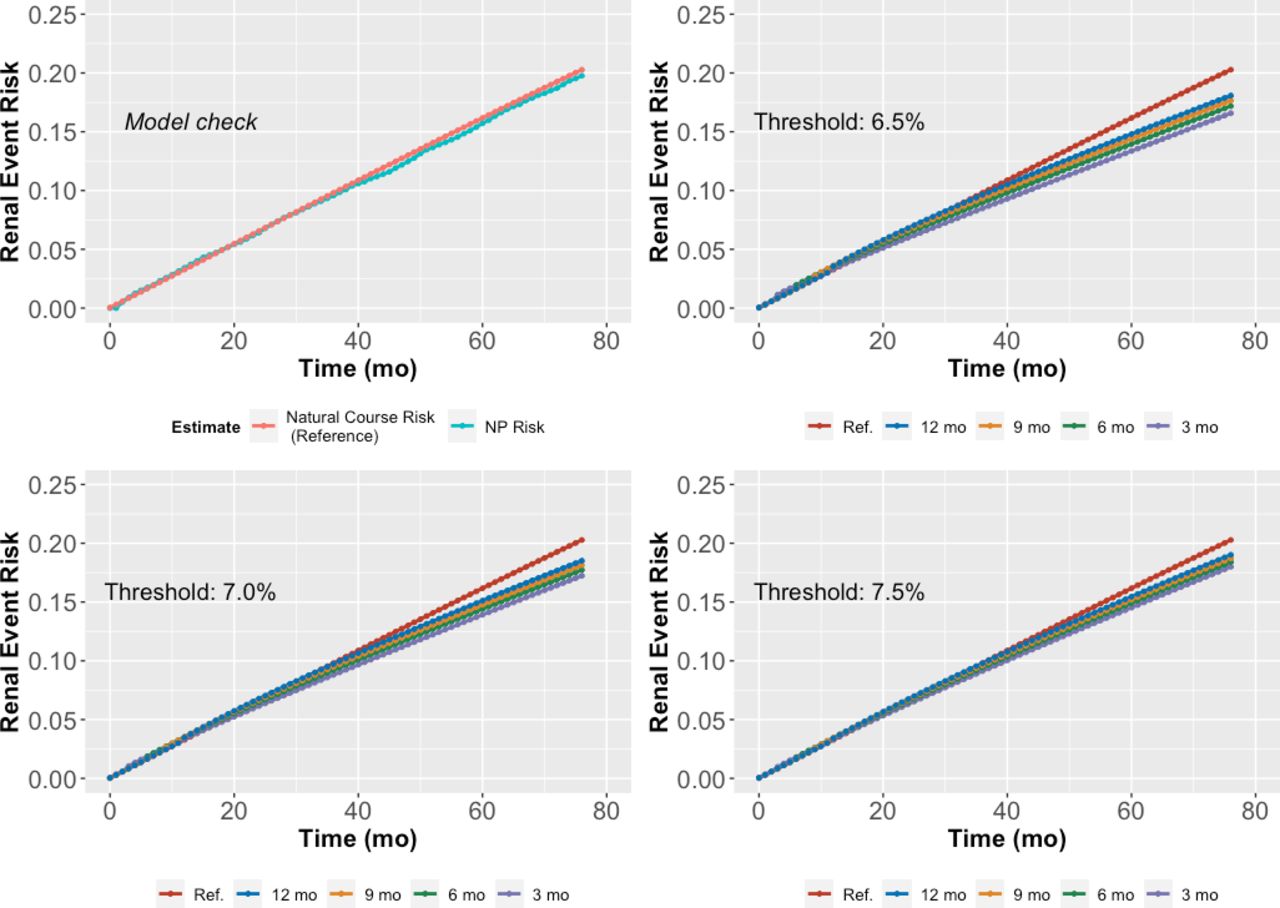
In the natural course scenario, 20.0% of persons experienced the renal composite end point, and this estimate was very close to the observed data (figure 2: upper left). This result means that the chance of our model misspecification was limited, although this is not guaranteed.25

Renal outcome stratified by the threshold hemoglobin A1c (HbA1c). mo, month(s); NP, non-parametric.
Main analysis
In the hypothetical intervention involving initiation of SGLT2 inhibitors within 3 months of HbA1c ≥7.0%, the 77-month risk of the composite end point was 17.2% of the study population, with a 3.1% lower risk relative to that of the natural course (table 1, figure 2). When initiation of SGLT2 inhibitors was deferred until 6 months, 9 months and 12 months, a beneficial effect of SGLT2 inhibitors was also observed, but the risk reduction was smaller than that observed with the ‘within 3 months’ strategy (table 1, figure 2: lower left).
Renal risk in different treatment strategies
In the sensitivity analyses using different thresholds of HbA1c levels—6.5% and 7.5%—the most beneficial effects were observed in the ‘within 3 months’ intervention for people whose HbA1c exceeded 6.5% (table 1, figure 2: right).
By stratifying the timing of intervention, we reaffirmed that the intervention, even at the lower HbA1c threshold, could reduce renal worsening (figure 3).

{kind=link}
{kind=link}
{kind=link}
Renal outcome stratified by the lag time. mo, month(s).
Sensitivity analysis
In the analysis limited to persons with a baseline eGFR of ≥45 mL/min/1.73 m2, data from 32 356 persons (138 540 person-years observation) were analyzed. Although the outcome occurrence was less frequent than that in the primary analysis, the results were essentially similar (online supplemental table 1). This sensitivity analysis also favored the earlier introduction of SGLT2 inhibitors for renoprotection among persons with T2DM.
Similarly, earlier introduction of SGLT2 inhibitors was associated with better renal outcomes in other sensitivity analyses in which1 the outcome was the continuous eGFR value;2 persons with a low eGFR were involved (data of 36 937 persons analyzed); and3 an additional adjustment by antihypertensive drug and ACE inhibitor/angiotensin II receptor blocker use was conducted (online supplemental tables 2-4). In the analysis in which continuous eGFR change was the outcome, however, statistical significance was noted only for very early introduction of SGLT2 inhibitors (online supplemental table 2). Unlike SGLT2 inhibitors, there were no benefits observed in DPP-4 inhibitors and GLP-1 receptor agonists (online supplemental tables 5 and 6).
Discussion
We estimated the 77-month risks of renal events among the T2DM population under different HbA1c-guided strategies regarding the initiation of SGLT2 inhibitor therapy. Overall, the initiation of SGLT2 inhibitors was associated with a lowered risk of reaching the renal end point. For example, the strategy of starting SGLT2 inhibitors within 3 months of HbA1c ≥7.0% could lower the risk by 3.1% at 77 months. The largest benefit was found with the strategy of initiating SGLT2 inhibitors within 3 months of HbA1c ≥6.5% (risk reduction by 3.7%) compared with deferred initiation (vs within 6 months, within 9 months or within 12 months) or initiation at a higher HbA1c threshold (vs 7.0% or 7.5%). The results were essentially similar in the sensitivity analysis that changed the inclusion criteria regarding baseline eGFR.
It is difficult to choose a single cut-off of HbA1c to define ‘uncontrolled’ diabetes or when to start add-on therapy. In this study, the threshold of 7.0% was primarily selected to accord with the American Diabetes Association guidelines that recommend a target HbA1c<7.0%.30 As higher or lower target levels are also acceptable if taking into account individualized risk or preference, we also prepared two different thresholds: 6.5% and 7.5%. Somewhat unexpectedly, the largest benefit was observed with the strategy with a threshold of 6.5% for uncontrolled T2DM. This could be explained in two ways. First, tight glucose control was better for preventing renal worsening,31 even for persons whose HbA1c level exceeded 6.5%. The benefit of stricter glucose control is not clearly shown in T2DM, particularly with regard to renal protection. For example, earlier randomized trials of intensive glucose control often employed progression of albuminuria as a renal end point.32 33 Future studies regarding intensive glucose control might support our explanation, but safety concerns for such trials remain.34 An alternative explanation is that the number of persons receiving SGLT2 inhibitors was expected to increase as the thresholds for initiating therapy lowered. Thus, it is also possible that the largest benefit in the 6.5% threshold strategy was simply reflected by the largest sample size exposed to SGLT2 therapy, whose effect could be introduced via either glucose-lowering or non-glycemic pathways of SGLT2 inhibitors.2
We also found that the earlier introduction of SGLT2 inhibitors led to better renal outcome, irrespective of all the thresholds of HbA1c examined (figure 2). The interpretation of this finding might be complicated because the period of exposure to SGLT2 inhibitors varied among different strategies; persons with early introduction (eg, within 3 months) were anticipated to receive SGLT2 inhibitor therapy longer than those with deferred introduction by the end of follow-up at 77 months (Supplemental Discussion in online supplemental file 1). It is intuitively difficult to understand whether—and to what extent, if any—these different exposure periods affected the estimated results among different strategies. With respect to this point, given the irreversible nature of the eGFR trajectory, we assumed that the estimated benefit of early initiation cannot be biased upward or overestimated (details in Supplemental Discussion in online supplemental file 1).
The parametric g-formula is a statistical method that can answer questions such as ‘when to treat’.24 Although this method is unfamiliar (or may be difficult to understand) to clinicians, it has recently been applied in clinical research to investigate when to initiate antiretroviral drugs35 or to examine lifestyle modifications and the subsequent risk of stroke 36 37 in which the effect of a ‘hypothetical’ intervention was evaluated. The statistical advantage of the parametric g-formula is that it can account for time-varying confounders and treatment-confounder feedback, the complex situation where the confounder affects the treatment and the treatment affects the confounder; it is known that traditional regression methods may fail in the presence of treatment-confounder feedback.38 In the care of diabetes, drug regimens and patient characteristics (eg, HbA1c) change over time, and both interact with each other so that the presence of treatment-confounder feedback is likely in diabetes care. As such, we applied the parametric g-formula to explore when to best initiate SGLT2 inhibitors, a question that is difficult to answer with other study designs.
Since our results are premature to be translated directly into clinical practice at this moment, the implications of our study need discussion. First, it could provide a rationale for future research, including randomized controlled trials, to seek the optimal timing of SGLT2 inhibitor treatment to achieve its renal benefit. From a clinical perspective, we may quantify the negative effect of clinical inertia by comparing the scenarios between early versus deferred initiation or those between lower or higher thresholds to initiate intervention.39 40 Our findings might also support the grade E recommendation of the American Diabetes Association that the medication regimen should be re-evaluated every 3–6 months.28
As the indication for SGLT2 inhibitors is expected to expand to non-diabetic persons at risk of renal disease, it may be interesting to explore whether our findings would be applicable to persons without diabetes. However, during the study period, SGLT2 inhibitors were only indicated for persons with T2DM, and thus, we did not have data on people without diabetes who used SGLT2 inhibitors. This research topic is the future agenda, when real-world data of non-diabetic persons are available.
Although the parametric g-formula is a sophisticated statistical approach, the model relies on several assumptions that cannot be tested. Moreover, whether findings obtained from this novel approach will change the clinical practice is yet to be certain. For transparency, we showed how the g-formula worked using DPP-4 inhibitors and GLP-1 receptor agonists as case examples (online supplemental tables 5 and 6). In the supplemental file, we have also provided the sample R codes.
There are several limitations in our study. First, there were unmeasured confounders, including dietary habits or duration of T2DM, in each person, which may have affected the results. Second, as we could not model the extent to which SGLT2 inhibitor therapy lowered HbA1c with each strategy, we could not explore the relationship between lowering HbA1c levels and the downstream renal effect. Third, Asian populations are known to be more susceptible to diabetic renal disease, and thus, the generalizability of the findings to other populations is uncertain.41 Fourth, we did not evaluate the harms of SGLT2 inhibitor therapy or its benefits other than kidney function protection. Potential adverse events associated with SGLT2 inhibitors include hypoglycemia, euglycemic diabetic ketoacidosis, genitourinary tract infection, volume depletion and bone fracture.30 Although there were claims records for these conditions in our data set, we could not specify which events were due to SGLT2 inhibitor use. Furthermore, even if identification of such events was possible, events that did not require medical attention (eg, non-severe hypoglycemia) or instances when patients were treated by other facilities outside the RWD database could not be captured. Therefore, we could not fully evaluate whether our therapeutic strategy of SGLT2 inhibitor administration might increase drug-related adverse events. Finally, our estimates were population-level effects, meaning that it is uncertain whether the benefit of SGLT2 inhibitors was delivered equally, regardless of individualized risk.
In summary, using observational data of persons with T2DM with the parametric g-formula, we compared the effect of different strategies of SGLT2 inhibitor initiation on the renal end point using different HbA1c thresholds and timings. Overall, our analysis favored the early introduction of SGLT2 inhibitors at a lower HbA1c threshold to reduce renal worsening. Future studies may be warranted to assess whether this strategy could be implemented in clinical practice. Our findings also suggest caution against clinical inertia in the care of diabetes.
Data availability statement
Data may be obtained from a third party and are not publicly available. Data sharing is not allowed by the data provider. For inquiries regarding our data set, please contact the Real World Data Co., Ltd. (Kyoto, Japan).
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Kyoto University Graduate School and Faculty of Medicine Ethics Committee (#R2927). We used anonymized data, which were exempted from informed consent of each participant according to Japanese law.This study was conducted under the approval of our institutional review board (R2927).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors MT and KK designed the study. MT conducted the data analyses and wrote the first draft of the manuscript. MO and NI provided critical comments from the viewpoint of a diabetologist, and the draft was substantially revised in response to their comments. All authors read the final version of the submitted manuscript.
Funding The study is supported by Japan Society for the Promotion of Science (grant number: 20H03941).
Competing interests MT received a consultation fee from Eisai Co., Ltd. MO received research support from Takeda Pharmaceutical Co., Ltd. and speaker honoraria from Takeda Pharmaceutical Co., Ltd., Nippon Boehringer Ingelheim Co., Ltd., Daiichi Sankyo Co., Ltd., Ono Pharmaceutical Co., Ltd, AstraZeneca, MSD K.K., Novo Nordisk Pharma Ltd., Eli Lilly Japan K.K., Sanofi K.K., Mitsubishi Tanabe Pharma Co., Kyowa Hakko Kirin Co., Ltd, Kowa Co., Ltd., Astellas Pharma Inc., Sumitomo Dainippon Pharma Co., Ltd., and Taisho Toyama Pharmaceutical. NI received research funds from Terumo Corp., Drawbridge, Inc., and asken Inc; speaker honoraria from Kowa Co., Ltd., MSD K.K., Astellas Pharma Inc., Novo Nordisk Pharma Ltd., Ono Pharmaceutical Co., Ltd., Nippon Boehringer Ingelheim Co., Ltd., Takeda Pharmaceutical Co., Ltd., Mitsubishi Tanabe Pharma Corp., Sumitomo Dainippon Pharma Co., Ltd., Sanofi K.K., Eli Lilly Japan K.K.; and scholarship grants from Kissei Pharmaceutical Co., Ltd., Sanofi K.K., Daiichi-Sankyo Co., Ltd., Mitsubishi Tanabe Pharma Corp., Takeda Pharmaceutical Co., Ltd., Japan Tobacco Inc., Kyowa Kirin Co., Ltd., Sumitomo Dainippon Pharma Co., Ltd., Astellas Pharma Inc., MSD K.K., Ono Pharmaceutical Co., Ltd., Sanwa Kagaku Kenkyusho Co., Ltd., Nippon Boehringer Ingelheim Co., Ltd., Novo Nordisk Pharma Ltd., Novartis Pharma K.K., and Life Scan Japan K.K. KK received research funds from Eisai Co., Ltd., Kyowa Kirin Co., Ltd., Sumitomo Dainippon Pharma Co., Ltd., Pfizer Inc., Stella Pharma Corporation, CMIC Co., Ltd., Suntory Beverage & Food Ltd., Mitsubishi Corporation, and Real World Data Co., Ltd.; consulting fees from LEBER Inc., JMDC Inc., Shin Nippon Biomedical Laboratories Ltd., Kaken Pharmaceutical Co., Ltd., and Advanced Medical Care Inc.; executive compensation from Cancer Intelligence Care Systems Inc.; and honoraria from Mitsubishi Chemical Holdings Corporation, Mitsubishi Corporation, and Pharma Business Academy; and holds stock in Real World Data Co., Ltd. KK declares no competing interests.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.