Article Text

Abstract
Introduction This study aimed to evaluate the test utilization and intraindividual changes of anti-glutamic acid decarboxylase antibody (GADA), a biomarker for autoimmune diabetes in Korean adults.
Research design and methods We retrospectively investigated longitudinally measured GADA test results to assess test utilization and intraindividual changes through a laboratory information system.
Results During the 3-year study period, 11 668 GADA tests were performed in 11 184 Korean adults. The overall rate of GADA positivity at initial measurement was 7.8%. Among the 11 668 test results, 871 GADA test results from 401 Korean patients (228 men and 173 women) requested by 54 hospitals were analyzed for intraindividual changes. Among these 401 patients, 80 (20.0%) had positive (≥2.0 U/mL) and 35 (8.7%) had gray zone GADA (1.0–1.9 U/mL) level at initial measurement. The prevalence of GADA-positive patients based on initial measurement was significantly different by type of medical institution. Among 80 patients with initial positive results, 5 (6.3%) experienced qualitative GADA changes during follow-up. Among the 321 patients with initially negative or gray zone GADA, 9 (2.8%) changed to GADA positive at least once during follow-up.
Conclusions Although most patients had stable GADA results, some exhibited qualitative changes during follow-up. This study can help to understand the variation in GADA positivity in the monitored patients.
- antibodies
- ethnic groups
- health services
Data availability statement
Data are available upon reasonable request. The datasets generated and analyzed during the current study are available from the corresponding authors upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Anti-glutamic acid decarboxylase antibody (GADA) is the most prevalent autoantibody at the onset of type 1 diabetes and is a hallmark of latent autoimmune diabetes in adults. Previous studies regarding GADA positivity in adult Korean patients were conducted from 1990s to 2017 and included data from patients visiting university hospitals.
WHAT THIS STUDY ADDS
GADA test utilization and intraindividual changes in a Korean adult population visiting different types of medical institutions were assessed from longitudinally measured data.
The prevalence of GADA-positive patients based on initial measurement was significantly different by type of medical institution.
Some patients who were initially GADA negative or gray zone changed to GADA positive at least once during a 3-year follow-up.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
An assessment of GADA test utilization and intraindividual changes can improve understanding of the characteristics of the patient population and the prevalence of disease, and these data can be used in evaluating the clinical performance of laboratory tests and improve the quality of the clinical test service.
Introduction
Autoantibodies against glutamic acid decarboxylase (GADA) are used as a biomarker for several neurological and endocrine autoimmune diseases.1 2 In particular, GADA is the most prevalent autoantibody at the onset of type 1 diabetes and is a hallmark of latent autoimmune diabetes in adults, a slowly progressing form of pancreatic endocrine autoimmunity affecting up to 5% of patients with type 2 diabetes and known for its association with insulin dependency.1 Measurement of GADA is an important screening and management tool for patients with diabetes because of its use in diabetes classification and insulin prescription.3
Although the prevalence and incidence of type 1 diabetes in Korea are reported to be lower than in Western populations, the overall incidence has increased by 3%–4% every year from 2007 to 2017.4 5 Moreover, diabetes mellitus in Asian populations has etiological heterogeneity, such that early diagnosis and management of diabetes rely on clinical findings including measurement of islet autoantibodies such as GADA, which is an important diagnostic that could improve patient outcomes.3 6 Previous studies on GADA positivity in adult Korean patients were conducted from the 1990s to 2017 and have included data from patients visiting university hospitals.4 7–15
In clinical laboratories, understanding the utilization and intraindividual changes of a test can improve the understanding of patient characteristics, including the prevalence of diseases, and these data can be used in evaluating the clinical performance of laboratory tests and to improve the quality of clinical test service.16 17 For example, prevalence of test results in a patient population is important in statistical analysis of comparability in clinical tests, including whether the number of specimens and predictive value of a negative or positive result are affected by prevalence.18 19 Furthermore, because the Green Cross Laboratories is one of the biggest clinical laboratories providing a GADA testing service throughout South Korea, analysis of test utilization using large population data through a laboratory information system can have important implications in Korea. For instance, understanding of population characteristics is a basic step in various clinical studies to improve clinical outcomes.18–20 Therefore, in this study, we aimed to investigate the test utilization of GADA in the adult Korean population visiting local clinics and hospitals and to assess intraindividual changes based on longitudinally measured data.
Research design and methods
Study populations
Longitudinally measured GADA test results in Korean adults were retrospectively investigated to assess test utilization and intraindividual changes through the laboratory information system in Green Cross Laboratories from July 19, 2018 to July 18, 2021. Information on subject age, sex, type of medical institution that requested GADA test, number of GADA test measurements, and quantitative and qualitative GADA test results of each measure was obtained. Types of medical institutions were categorized into three groups: university hospitals, hospitals, and others (local clinics, referral clinical laboratories, armed forces hospitals, and public medical centers). Results were excluded for subjects with missing data on age or sex. All data were anonymized before statistical analysis. Green Cross Laboratories is one of the biggest referral clinical laboratories in Korea, providing clinical services for GADA tests throughout Korea. Nationwide utilization of the GADA test is available from Healthcare Bigdata Hub by Health Insurance Review & Assessment Service (HIRA) in Korea (https://opendata.hira.or.kr/, accessed on March 4, 2022), with the test code D8031. Between August 2018 and July 2021, 68 727 GADA tests were performed in 62 794 Korean subjects. In this study period, GADA tests were performed in 11 184 Korean subjects in Green Cross Laboratories (about 17.8% of 62 794 Korean subjects during the same period).
Analysis of GADA
GADA was measured with a radioimmunoassay using an anti-GAD65 RIA kit (DIAsource, Nivelles, Belgium) on an r-counter (Cobra 5010 Quantum, Packard, Meriden, USA). The analytical measurement range of GADA was 0.7–120.0 U/mL. Samples were judged positive when the GADA level was ≥2.0 U/mL, negative when the GADA level was <1.0 U/mL, and in the gray zone when the GADA level was 1.0–1.9 U/mL according to the manufacturer’s instructions.
Statistical analysis
The Χ2 test was used to investigate the difference in GADA positivity by sex, age group by decade, and type of medical institution. The Mann-Whitney U test was adopted when appropriate for non-normally distributed continuous variables to compare age and quantitative GADA results by sex and type of medical institution. To investigate GADA positivity by type of medical institution, a weight-adjustment factor was calculated based on data from Healthcare Bigdata Hub by HIRA (online supplemental table S1). Sankey diagram visualization was performed using SankeyMATIC (https://sankeymatic.com/, accessed on March 4, 2022).
Supplemental material
Results
Baseline characteristics of study subjects
The study design and results are summarized in the online supplemental figure S1. During the 3-year study period, 11 654 GADA tests were performed for 11 184 Korean adults. Among these subjects, 10 783 (96.4%) had GADA level measured only once. After exclusion of 10 783 test results, 871 GADA test results from 401 Korean patients (228 men and 173 women) requested by 54 hospitals were included in the analysis of intraindividual changes. Baseline characteristics of study subjects are summarized in table 1. The median (IQR) age of patients who had undergone follow-up GADA tests was 50.9 (35.4–63.5) years. Most (89.0%) patients underwent two GADA tests during follow-up (range, two to eight measurements). Age, number of follow-up measurements, follow-up duration, quantitative and qualitative GADA test results, and type of medical institution requesting GADA tests were not significantly different between men and women.

Anti-glutamic acid decarboxylase antibody (GADA) test results by age in subjects who had follow-up GADA test results (at initial baseline measurement). The y-axis on the left of the graph represents the number of GADA test results (numbers presented in the stack bars), and the y-axis on the right of the graph represents the percentage of positive GADA tests results. The red line represents the percentage of positive GADA test results (with gray lines pointing toward the percentages from the red line, corresponding values are in the y-axis on the right).
Baseline characteristics of study subjects who underwent anti-glutamic acid decarboxylase antibody (GADA) tests
GADA test results and utilization
Qualitative GADA results and the rate of GADA-positive results at initial measurement are shown in figure 1. In this population, the rate of GADA-positive results was not significantly different by age group. Among the 401 patients, 80 (20.0%) had positive (≥2.0 U/mL) and 35 (8.7%) had gray zone GADA (1.0–1.9 U/mL) level at the initial measurement. The prevalence of GADA-positive patients based on initial measurement was significantly different by type of medical institution (table 2). Although 67.6% of the 401 patients visited university hospitals, and the number of GADA-positive patients was highest in patients visiting university hospitals (46 patients, 11.5%), the prevalence of GADA-positive patients visiting other types of medical institutions was highest (9 of 22, 40.9%). Patient characteristics of age and sex were not statistically different by type of medical institution.
Prevalence of positive anti-glutamic acid decarboxylase antibody (GADA) results among 401 followed-up patients by medical institution (based on initial measurement)
Samples were judged positive when the GADA level was ≥2.0 U/mL, negative when the GADA level was <1.0 U/mL, and gray zone when the GADA level was 1.0–1.9 U/mL.
Intraindividual change in GADA
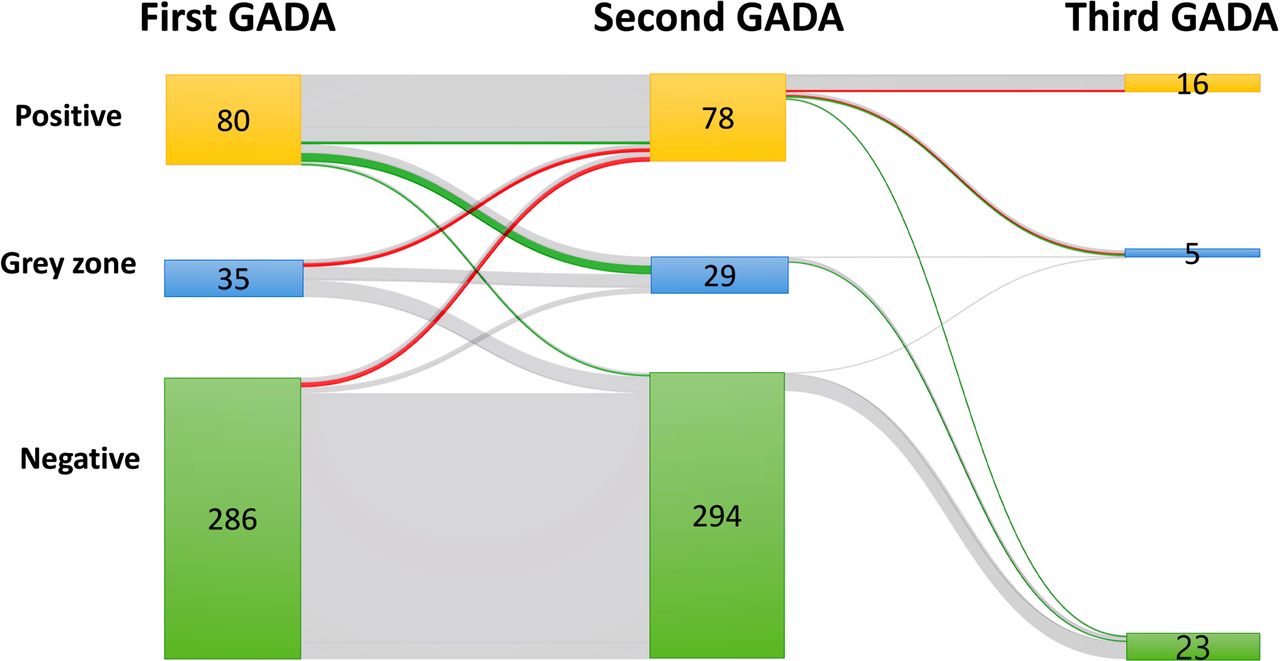
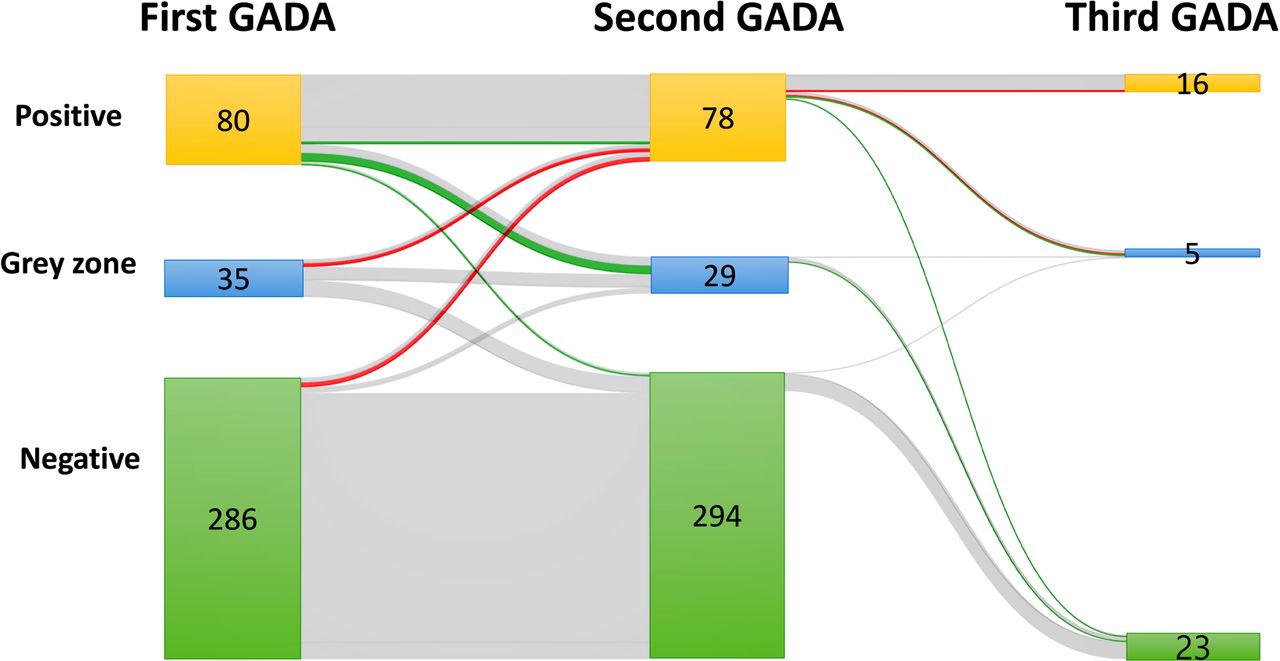
Among the 80 patients with initial GADA-positive results, 5 (6.3%) experienced qualitative changes of GADA to negative or gray zone results during the follow-up period. Among 321 patients with initially negative or gray zone GADA level, 9 (2.8%) changed to a positive GADA result at least once during the follow-up period. Intraindividual changes of GADA results are shown in figure 2. The number of subjects who attended more than three follow-up visits was small (n=11), and the results of the first to third measurements are shown in figure 2. Among these 11 patients, 8 did not experience qualitative change of GADA results, while the other 3 experienced qualitative change from positive to not positive (negative or gray zone) during the first to third follow-up measurements. The maximum difference between GADA results at the initial and follow-up measurements ranged from −23.6 to 15.3 U/mL. Five patients who experienced qualitative changes from positive to gray zone or negative GADA had low quantitative value (range, 2.3–7.0 U/mL) at initial measurement. There was no statistical difference in prevalence of qualitative GADA changes and by type of medical institution.
{kind=link}
{kind=link}
Intraindividual changes in anti-glutamic acid decarboxylase antibody (GADA) using a Sankey diagram (created using SankeyMATIC, https://sankeymatic.com/). Gray flows indicate cases without qualitative GADA changes and colored flows indicate cases that experienced qualitative GADA changes during follow-up; green flows indicate cases that experienced qualitative GADA result change from initially positive to not positive (negative or gray zone), red flows indicate cases that experienced qualitative GADA result change from initially not positive (negative or gray zone) to positive. Number of subject is available in the bar of each measurement.
Discussion
In this study, we evaluated the utilization of GADA tests and intraindividual changes in results in Korean adults using retrospective data from tests requested by 54 hospitals during the 3-year study period.
Persistence of positive islet cell autoantibodies is a risk factor for clinical diabetes.3 Studies on the clinical implications of GADA in diabetes, including persistence and timing of seroconversion in association with development of insulin dependency, are ongoing.2 3 21–25 In Korea, the seroprevalence of GADA has been reported to be 4%–25% in type 2 diabetes in different settings.26 In the present study, GADA prevalence is comparable with that of previous studies performed in Korean adults with diabetes. In the present study, the highest prevalence of GADA positivity was observed in subjects visiting other types of medical institutions (local clinics, referral clinical laboratories, armed forces hospitals, and public medical centers) compared with those visiting university hospitals or general hospitals. However, the number of subjects with follow-up GADA tests at other types of medical institutions was small (22 subjects); therefore, this result should be interpreted with caution. According to the data from Healthcare Bigdata Hub, more patients (50.3%) with type 1 diabetes mellitus (Korean disease code E10) visited other types of medical institutions than university hospitals (24.4%) and general hospitals (26.3%). Because previous studies on the seroprevalence of GADA were performed in university hospitals in Korea, the reason for the high seroprevalence in this group should be clarified through future studies.
Previous studies performed in adult patients with type 2 diabetes reported that GADA levels fluctuated during the 6-year follow-up period but persisted in most (93.0%) patients.27 It has been reported that quantitative and qualitative changes in GADA were found in up to 18.6% of children with type 1 diabetes,28 which is comparable with previous studies performed in adult subjects. A limited number of studies focus on the fluctuation of GADA in Korean populations. Future studies are needed to clarify the significance of these changes in clinical diabetes care.
According to recent clinical practice guidelines for diabetes by the Korean Diabetes Association and the American Diabetes Association, it is recommended that islet cell autoantibodies be monitored in patients with diabetes because of the clinical heterogeneity of the complex phenotype, in which clinical presentation and disease progression can vary considerably between patients.3 26 In the present study, most GADA tests were performed once. Although most patients had stable GADA results during follow-up, some experienced qualitative changes. Since January 18, 2018, the reimbursable conditions for GADA tests by HIRA require that the first measured tests are performed to determine the prognosis for future treatment when it is difficult to distinguish type 1 and type 2 diabetes at the time of diagnosis, under clinical suspicion of type 1 diabetes (patient age younger than mid-30s, family history of type 1 diabetes, autoimmune diseases, thin body type), or patients with type 2 diabetes taking oral hypoglycemic agents who have findings suggestive of type 1 diabetes, such as inability to control blood glucose with requirement of insulin treatment within a relatively short period of time (3–5 years). According to the Diabetes Fact Sheets in Korea, 6.4%–8.9% of patients diagnosed with diabetes are treated with insulin therapy.29 In this study, about 3.6% (401 of 11 184) of patients underwent follow-up GADA tests. Considering that qualitative GADA change from initially negative to positive can be a clinical concern of diabetes and insulin dependency, GADA test monitoring may be helpful for patients with diabetes who need to initiate insulin treatment.3
The strength of this study was the use of a large amount of GADA test data, which were requested from 54 hospitals throughout Korea to investigate the utilization of GADA testing. This study using longitudinally measured GADA results from patients visiting local clinics in Korea will help to fill the knowledge gaps on intraindividual changes in Korean patients. A limitation of this study was the lack of detailed clinical information and other related biomarkers (such as hemoglobin A1c, c-peptide, and insulin) and other autoantibodies associated with diabetes and beta-cell destruction, such as islet or insulinoma-associated antigen, zinc transporter 8, and islet cell autoantigen. The descriptive nature of the study, small number of cases (power), limited number of variables, information of clinical diagnosis, such as newly diagnosed diabetes, undiagnosed type 2 diabetes, and non-diabetes-related testing can affect the results and also are limitations. Because this study aimed to investigate the utilization of GADA testing including the prevalence of GADA test results, how many tests were repeatedly measured in the same individuals, and intraindividual changes in repeatedly measured GADA tests, the present study has a descriptive nature and subjects had at least two data points. Therefore, specific statistical methods for longitudinal studies using at least three data points and a multilevel model of change framework testing the non-dependency of the observation were not applied. This study might be susceptible to selection bias due to missing values in population characteristics, because this study focused on results from patients with available follow-up GADA results. The proportions of specimens from patients visiting different types of medical institutions might limit the generalizability of this study. However, the large number of test results of this study (17.8% of all Koreans tested GADA) is a strength and increases understanding of the utilization of GADA tests in Korea. These results on intraindividual changes in GADA will increase knowledge on GADA tests in Korea.
Conclusions
In conclusion, we evaluated the utilization of GADA tests and intraindividual changes GADA levels in Korean patients. Considering that some patients have qualitative changes during follow-up, monitoring of GADA level in the management of patients with diabetes is suggested. Future well-designed studies using clinical samples, detailed clinical findings, and other related biomarkers in association with disease progression are needed to clarify the clinical implications of changes in GADA levels and the prognostic value of GADA tests.
Data availability statement
Data are available upon reasonable request. The datasets generated and analyzed during the current study are available from the corresponding authors upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study was conducted according to the guidelines outlined in the Declaration of Helsinki, and all procedures involving human subjects were approved by the Institutional Review Board (IRB) of Green Cross Laboratories (GCL-2021-1045-01). A waiver of informed consent was approved by the IRB since the waiver would not adversely affect the rights and welfare of the subjects because the study was retrospective and involved no more than minimal risk to the subjects.
Acknowledgments
We thank Yeon Woo Jo at Green Cross Laboratories for her administrative support.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Conceptualization—RC and SGL. Methodology—RC, WP, GC and JL. Software—RC, WP and GC. Validation—RC, WP, GC and SGL. Formal analysis—RC, WP and GC. Investigation—RC, WP, GC, JL and SGL. Resources—RC. Data curation—RC. Writing (original draft preparation)—RC. Writing (review and editing)—RC, WP, GC, JL, SGL and EHL. Visualization—RC, WP and GC. Supervision—SGL and EHL. Project administration—RC. Funding acquisition—SGL and EHL. SGL and EHL are the guarantors and take responsibilities for the conduct and the contents of the article. All authors have read and agreed to the published version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.