Article Text

Abstract
Introduction Hypoglycemia is often recurrent and severe in patients with congenital hyperinsulinism (CHI). However, there is little information regarding frequency or patterns of episodes to inform clinical management and future trial design.
Research design and methods We aimed to describe frequency and patterns of hypoglycemia by varying thresholds through a large continuous glucose monitoring (CGM) dataset. Through the UK CHI centers of excellence, data were analyzed from patients with CHI over a 5-year period. Hypoglycemia thresholds of 3.0 (H3.0), 3.5 (H3.5) and 3.9 (H3.9) mmol/L were used to test threshold change on hypoglycemia frequencies.
Results From 63 patients, 3.4 million data points, representing 32 years of monitoring, were analyzed. By UK consensus threshold H3.5, patients experienced a mean 1.3 hypoglycemic episodes per day. Per cent time hypoglycemic increased from 1.2% to 3.3% to 6.9% when threshold changed from H3.0 to H3.5 and H3.9. Merged data showed periodicity of hypoglycemia risk in 24-hour periods in all patients.
Conclusions We have evaluated a large dataset to provide a comprehensive picture of the frequency and patterns of hypoglycemia for patients with CHI in the UK. These data establish a baseline risk of hypoglycemia by CGM and provide a framework for clinical management and clinical trial design.
- hypoglycemia
- hyperinsulinism
- blood glucose self-monitoring
Data availability statement
Data are available upon reasonable request. Data were used as part of a service evaluation and thus are not freely available for research purposes. If data were required to be shared, this could be organized with the appropriate legalities and ethical approval.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Little information is available regarding frequency or patterns of hypoglycemic episodes for patients with congenital hyperinsulinism (CHI).
Clinical management and future trial design are severely hampered by this lack of data.
Small CHI datasets suggest periodicity to hypoglycemia patterns.
WHAT THIS STUDY ADDS
Based on 32 years of continuous glucose monitoring data, patients with CHI experience 1.3 hypoglycemic episodes per day.
Percentage time hypoglycemic increases from 3.3% to 6.9% when hypoglycemia threshold is increased from 3.5 mmol/L to 3.9 mmol/L.
Periodicity of hypoglycemia risk in 24-hour periods is confirmed by a large, heterogeneous dataset.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
This baseline hypoglycemia risk provides a framework for clinical management and clinical trial design.
Confirmation of 24-hour periodicity of hypoglycemia risk provides vital information for the targeting of future interventions.
Introduction
Congenital hyperinsulinism (CHI) is the most common cause of recurrent and severe hypoglycemia in early childhood but knowledge about the frequency of hypoglycemia is absent. This is, in part, due to a lack of agreement regarding hypoglycemia thresholds, with no conclusive evidence of a definitive cut-off above which neurological impact is minimized. In the UK, and most of Europe, 3.5 mmol/L (63 mg/dL) is felt to offer a safe and pragmatic level at which neuroglycopenia is minimized and treatment burden is manageable.1
While glucose ranges in CHI have been described by low frequency self-monitoring of blood glucose (SMBG) with glucometer,2 very few studies have described hypoglycemia frequency using the high granularity data available from continuous glucose monitoring (CGM) and these have only been on a small scale.3 4 Incidence of hypoglycemia is, unsurprisingly, higher when measured by CGM over SMBG5 and thus it is important to use CGM to estimate the true incidence as SMBG will report a significant underestimate, more so overnight.4
The interest in novel therapies for the treatment of CHI has increased significantly over the last few years6 7 and many of these will be coming to trial in the near future. In order to ensure that expensive and burdensome trials address therapy outcomes robustly, it is essential for trial design to be based on credible data. To this end, we aimed to provide a description of the frequency and pattern of hypoglycemia by CGM in patients from a large and heterogeneous dataset, representative of the UK CHI population and upon which future trials can be based. Furthermore, we aimed to describe the relative frequencies and daily patterns of hypoglycemia by varying thresholds to demonstrate how threshold changes affect the frequency of recorded hypoglycemia.
Research design and methods
This study was performed as a national service evaluation project collating anonymized datasets derived from children with CHI under the care of the two highly specialized CHI services in the UK: Northern Congenital Hyperinsulinism Service based at Royal Manchester Children’s Hospital and Alder Hey Children’s Hospital; and Great Ormond Street Hospital Congenital Hyperinsulinism Service. All patients with confirmed CHI under the care of the two centers, who had undergone monitoring with CGM, were eligible for inclusion. CHI was confirmed by the finding of detectable serum insulin at the time of hypoglycemia (glucose <3.0 mmol/L) in patients with a glucose infusion rate exceeding 8 mg/kg/min, consistent with a diagnosis of CHI. Patients with transient CHI (resolution at <12 months of age) or diabetes secondary to subtotal/near total pancreatectomy were excluded. Retrospective CGM data were downloaded from the Dexcom Clarity website in .csv file format and anonymized by each hospital team. Anonymized files were collated by the study team along with minimal clinical data including genetic mutation status (positive mutation identified on 13-gene CHI panel (R144 in National Genomic Test Directory) vs negative/not tested), and medication status (on or off disease-modifying medications for CHI) but excluding patient-identifiable information.
CGM data were processed as per American Diabetes Association (ADA) guidelines for definition of CGM hypoglycemia:8 three values (≥15 min) below a threshold to commence a hypoglycemic episode and three values (≥15 min) above a threshold to terminate an episode. These guidelines were used as a practical way to exclude short-lived hypoglycemic episodes detected by CGM that were unlikely to represent true hypoglycemia, thereby enhancing data confidence. Therefore, use of the ADA hypoglycemia criteria was agnostic of the underlying disease. Data were analyzed using purpose-built scripts in Python V.3.8.8. Scripts were designed to assess the number of hypoglycemic episodes per day as well as percentage time spent hypoglycemic as defined by varying glucose cut-offs (H3.0, H3.5, H3.9 for 3.0, 3.5, 3.9 mmol/L). Differences in percentage time hypoglycemic between subgroups were analyzed using Χ2 tests. The study aim was to evaluate the incidence of hypoglycemia in the UK CHI population and investigate change in hypoglycemia frequency with variable thresholds.
Results
Data were obtained from 63 patients with CHI over a period of 5 years (2017–2021). Mean age (range) was 6 years 3 months (1 month–18 years) with 54 patients (86%) over 12 months of age. The mean (range) number of days of data per patient was 182 (1–1490), resulting in 3.4 million data points representing almost 17 million minutes (over 32 years) of glycemic monitoring. All patients used a Dexcom CGM device, either a G4 or a G6 depending on the year of insertion. Prior to 2019, 14 patients used the G4 device while in all other patients the later generation G6 device was used. Indications for the use of CGM were at the discretion of the clinical teams and were not evaluated as part of this study. Patients who met eligibility criteria but in whom CGM data were not accessible via Dexcom Clarity were not included. For hypoglycemia by UK consensus H3.5 criteria, a mean of 1.3 hypoglycemic episodes per day were observed, for mean duration of 36 min with patients spending 3.3% of their time in hypoglycemia (table 1). For more severe hypoglycemia by H3.0 criteria, there were 0.5 hypoglycemic episodes per day, for mean duration of 35 min and resulting in 1.2% of the time below threshold (table 1). In contrast, by a higher threshold (H3.9), the mean number of hypoglycemic episodes increased to 2.4 per day, for mean duration of 42.4 min and 6.9% time below threshold. Therefore, the use of a higher or lower hypoglycemia threshold than the UK consensus H3.5 threshold led to a significantly increased or decreased percentage time in hypoglycemia. As the analyses of varying thresholds were performed on identical data, the differences in percentage time hypoglycemic are not subject to any likelihood of being caused by chance and thus a test for statistical significance is not required.
Hypoglycemia values as per varying thresholds for hypoglycemia
As a point of comparison, we analyzed CGM data point by point (single values below a hypoglycemia threshold) rather than using the ADA criteria. By non-ADA criteria and using the H3.5 threshold, patients had 2.4 hypoglycemic episodes per day, lasting 22 min with 3.6% time below threshold. Data for alternative hypoglycemia thresholds are presented in table 1.
Subgroup analysis revealed small but statistically significant differences between those with and without pathological genetic mutations causing CHI. Those without mutations (n=20) spent marginally greater time below all thresholds of hypoglycemia than those with mutations (n=43) (for H3.5: 3.58% vs 3.01%, Χ2 statistic=1970, p<0.001) as well as having more hypoglycemic episodes per day (table 1). Those patients not receiving treatment for CHI at the time of glycemic monitoring (n=14) spent significantly more time below all thresholds of hypoglycemia than those receiving medications (n=49) (for H3.5: 6.74% vs 2.54%, Χ2 statistic=58 698, p<0.001).
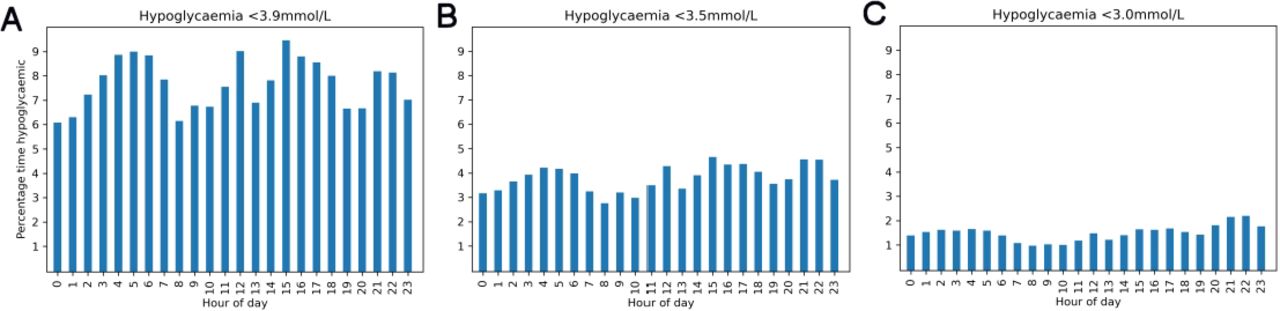
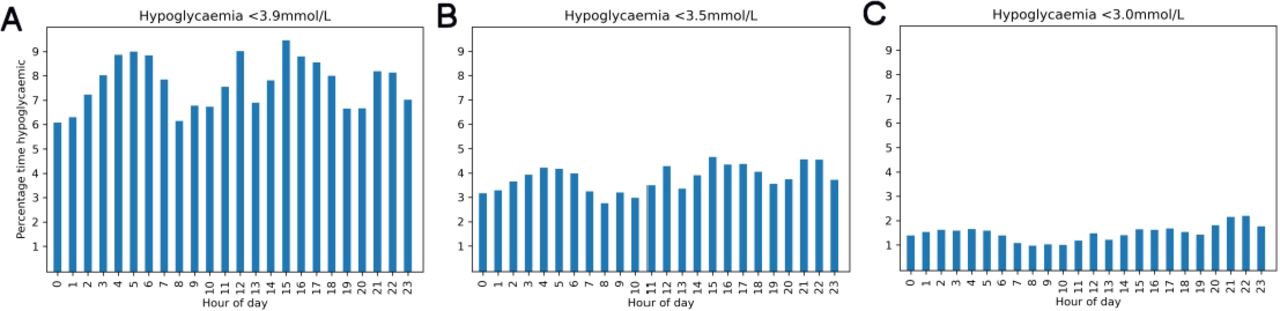
Analysis of glucose trends in merged data over 24-hour periods showed hypoglycemia periodicity with increased risk before traditional mealtimes and around 21:00–22:00 (figure 1). This pattern varied as hypoglycemia cut-offs were changed between H3.9, H3.5 and H3.0 but risk was lowest at 08:00 for all thresholds.
{kind=link}
Distribution of hypoglycemia over 24-hour periods showing periodicity with three peaks (03:00–06:00, 15:00–18:00 and 21:00–22:00) with relatively low risk at 08:00 and a small, short-lived but consistent peak in risk at midday. As hypoglycemia thresholds are reduced from H3.9 (A) to H3.5 (B) and subsequently to H3.0 (C), the % time in hypoglycemia reduced although periodicity is retained.
Discussion
We have evaluated a large database comprising 3.4 million data points by CGM to demonstrate variable frequency of hypoglycemia at different thresholds. While the range of glucose levels has been described in observational studies,2 9 the majority have reported low frequency blood/plasma glucose levels with only a few reporting glucose levels by CGM3 4 outside of studies analyzing CGM accuracy.5 Our study is the first major analysis of real-world CGM profiles describing the frequency of hypoglycemia in patients with CHI and, given the size of the combined dataset, presents a comprehensive picture, over-riding anomalies related to skewed recruitment, data quality and other biases inherent in an observational cohort. Given that the use of CGM is not routine in the management of CHI, there is a possible bias towards severity affecting the generalizability of results.
Hypoglycemia cut-offs for CHI are arbitrary and artificial. Traditional cut-off glucose levels of 2.6 mmol/L had been derived from studies that are not relevant to CHI10 and most medium-term to long-term studies reporting neurodevelopment either exclude patients with CHI11 or do not specify CHI inclusion.12 While hypoglycemia may not be attributable to a single glucose test and is probably individualized for the risk of neuroglycopenia, the definition of hypoglycemia is a pivotal starting point that guides further investigation and treatment. Therefore, it is important to compare different thresholds of hypoglycemia to quantify relative frequencies at each threshold.
At present, the treatment threshold of hypoglycemia in CHI is pragmatic and based on the need to minimise the risk of neuroglycopenia with the least intensity of treatment support.1 In CHI, this threshold is chosen by UK consensus at 3.5 mmol/L.6 However, there are no baseline data on treated or untreated patients with CHI. It is unknown if a hypoglycemia cut-off of 3.5 mmol/L corresponds to different frequencies of hypoglycemia than higher (3.9 mmol/L) or lower (3.0 mmol/L) thresholds. At present, there are no data on long-term neurodevelopmental impact of various CGM-derived hypoglycemia thresholds. However, there is an immediate need to use CGM in clinical practice and to determine clinical trial design for novel therapies in CHI. In the absence of long-range robust outcome markers, our study provides a comparative evaluation of differential thresholds to establish baseline hypoglycemia. We have shown that the frequency of hypoglycemia by ADA criteria is 3.3% at 3.5 mmol/L but rising significantly (112% increase) at 3.9 mmol/L.
While we did not set out to describe the level of glycemic control between CHI subgroups, the large difference in percentage time hypoglycemic between those patients on and off treatment for CHI is apparent. The latter group represented those non-responsive to diazoxide, those being weaned off medications or undergoing pancreatic surgery and those receiving non-disease-modifying medications such as acarbose, contributing to the heterogeneity of hypoglycemia phenotypes. Because this project was a service evaluation, minimal clinical details were obtained and thus no clear conclusions can be drawn. However, the increase in hypoglycemia seen in the off medication group may be due to several factors beyond the remit of our study design; these could include persistent unrecognized hypoglycemia in post-pancreatectomy CHI and relative improved glycemic control in those on medications.
We have demonstrated a replication of the characteristic risk profile of hypoglycemia throughout the day that has previously been described in patients with CHI.4 The risk of hypoglycemia is not static throughout the day and shows periodicity with increased risk through overnight fasting in almost all patients. Further peaks throughout the day are likely to represent pre-meal times for patients. Variations in the risk of hypoglycemia throughout the day provide a further focus for those designing interventions to reduce hypoglycemia in a clinical trial setting.
Our study establishes baseline risk of hypoglycemia at different thresholds that are likely to be used in the design of clinical trials based on CGM output. A strength of our study is the size and heterogeneity of the sample population drawn from the entire UK, providing a representative sample of the populations for future clinical trials. While SMBG remains standard of practice,13 the higher frequency and the propensity for CGM to identify nocturnal hypoglycemia4 clearly demonstrates the superiority of CGM in clinical trial application even in the presence of suboptimal error rates. Therefore, our study outcomes provide valuable baseline data in order to test for risk and benefit with novel therapies.
Our study does not test accuracy of CGM in relation to paired SMBG values; this has been described elsewhere by other groups and is the current focus of a separate study by our group. We accept that diversity of the patient profile and different management styles may impact on the glucose profile, thereby introducing centre-specific bias. However, such bias reflects real-world scenarios that permeate into clinical practice as well as research studies and will be a consideration for any future clinical trials.
Conclusions
We have described hypoglycemia frequency in CHI in a large dataset derived from a national cohort. Using CGM, we have demonstrated large variations in hypoglycemia frequency when thresholds are altered from H3.5 to H3.0 or H3.9 mmol/L. We have also demonstrated periodicity of risk of hypoglycemia through the day. Such factors should be considered in routine clinical management and influence the design of interventional trials in CHI.
Data availability statement
Data are available upon reasonable request. Data were used as part of a service evaluation and thus are not freely available for research purposes. If data were required to be shared, this could be organized with the appropriate legalities and ethical approval.
Ethics statements
Patient consent for publication
Ethics approval
As the study was designed as a service evaluation, ethical approval was not sought. Exemption from an ethical review board was not sought as the study was a service evaluation and thus does not require ethical approval.
Footnotes
Contributors CW collected the CGM data for RMCH patients and then collated and analysed the complete dataset and wrote the first draft of the manuscript. CW is the guarantor. YT collected the CGM data for GOSH patients and reviewed and approved the final manuscript. PRG contributed to the write up of the manuscript and reviewed and approved the final version. KEC contributed to the write up of the first manuscript and provided basic science input as well as reviewing and approving the final draft. MS-E was co-lead consultant for the RMCH patients, contributed to the manuscript write up and approved the final version. SS was lead consultant for the AHCH patients, provided CGM data from this patient group and approved the final manuscript. AD was lead consultant for the GOSH patients, contributed to the collection of CGM data from these patients and approved the final version of the manuscript. IB was co-lead consultant for RMCH patients, helped draft the first version of the manuscript and approved the final version.
Funding Some of the CGM devices for the RMCH patients were funded by a Momentum grant from Health Innovation Manchester.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.