Article Text

Abstract
Introduction Sarcopenia index (SI), calculated by (serum creatinine/cystatin C)×100, is reported to be associated with sarcopenia. Few studies reported the association between SI and subclinical atherosclerosis. We evaluated the association between SI and subclinical atherosclerosis, assessed by brachial-ankle pulse wave velocity (baPWV).
Research design and methods One hundred seventy-four patients with type 2 diabetes were included in this cross-sectional study. The relationship between SI and baPWV was assessed by Pearson’s correlation coefficient. To calculate area under the receiver operator characteristic (ROC) curve (AUC) of SI for the presence of subclinical atherosclerosis, which was defined as baPWV >1800 cm/s, ROC analysis was performed. Logistic regression analyses were performed to assess the effect of SI on the prevalence of subclinical atherosclerosis adjusting for covariates.
Results Mean age, duration of diabetes, baPWV, and SI were 66.9 (10.1) years, 17.7 (11.6) years, 1802 (372) cm/s, and 77.6 (15.8), respectively. There was an association between SI and baPWV (men; r=−0.25, p=0.001, and women; r=−0.37, p=0.015). The optimal cut-off point of SI for the presence of subclinical atherosclerosis was 77.4 (sensitivity=0.72, specificity=0.58, p<0.001, AUC 0.66 (95% CI: 0.57 to 0.74)). In addition, SI was associated with the prevalence of subclinical atherosclerosis (adjusted OR 0.95, 95% CI: 0.91 to 0.99, p=0.015).
Conclusions SI is associated with the prevalence of subclinical atherosclerosis in patients with type 2 diabetes.
- renal function
- atherosclerosis
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Sarcopenia is reported to be associated with risk of cardiovascular disease and mortality.
Serum creatinine/serum cystatin C ratio, called as sarcopenia index, is used as a surrogate marker for sarcopenia.
WHAT THIS STUDY ADDS
There was an association between sarcopenia index and brachial-ankle pulse wave velocity.
Sarcopenia index is associated with the prevalence of subclinical atherosclerosis.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
Since sarcopenia index can be evaluated by serum sample, the physicians should pay attention to the patients with low sarcopenia index as the having risk of the presence of subclinical atherosclerosis.
Introduction
Among patients with diabetes, cardiovascular disease (CVD) is an important cause of morbidity and mortality;1 2 it is reported that one of the major risk factor for CVD is atherosclerosis, which is a risk for peripheral arterial disease (PAD) and non-embolic ischemic stroke.3 Type 2 diabetes (T2D) is known to cause atherosclerosis.4 Subclinical atherosclerosis has been reported to be a risk for cardiovascular events in patients with diabetes.5 6 Therefore, screening for subclinical atherosclerosis is a useful for identifying high-risk patients including patients with diabetes.7
Sarcopenia is becoming an important consideration in older patients with T2D, because the number of older patients with diabetes is increasing.8 Sarcopenia is reported to be associated with risk of CVD9 and mortality.10–12 Serum creatinine (Cre)/serum cystatin C (CysC) ratio, the so-called sarcopenia index (SI), is used as a surrogate marker for sarcopenia.13–16 Previous studies show that there is an association SI with incident CVD events and mortality.17 18
Pulse wave velocity (PWV) is developed as a marker of arterial stiffness19 and is expressed as the severity of vascular damage;20 it is a useful tool to detect subclinical atherosclerosis.21 In particular, brachial-ankle PWV (baPWV) is useful to detect subclinical atherosclerosis.22 23 However, few studies revealed the association between SI and subclinical atherosclerosis. Therefore, in this cross-sectional study, we used baPWW to evaluate the relationship between SI and subclinical atherosclerosis.
Materials and methods
Study participants
In this cross-sectional study, we extracted the data from the KAMOGAWA-DM cohort study, which is an ongoing prospective cohort study.24 To clarify the natural history of patients with diabetes, we invited all patients with diabetes who were outpatients of Department of Endocrinology and Diabetes of Kyoto Prefectural University of Medicine Hospital (Kyoto, Japan) or Department of Diabetes of Kameoka Municipal Hospital (Kameoka, Japan) to participate in the KAMOGAWA-DM cohort study and enrolled those who agreed to participate. In this study, we extracted the data of patients who were registered from November 2016 to December 2017.25 Exclusion criteria were as follows: non-T2D, no data of baPWV, no data of CysC, renal dysfunction (defined as serum Cre >2.0 mg/dL),26 missing data of body weight, history of CVD, including heart failure, unstable angina, myocardial infarction, stroke, and peripheral artery disease (defined as ankle-brachial index <0.9).27
Data collection and measurements
Body mass index (BMI) was assessed as weight (kg) divided by height2 (m2). Using a standardized self-administered questionnaire, the data of habitual alcohol consumption (consuming alcohol daily or not), smoking status (current smoker or not), and exercise habit (exercise of some kind at least once a week or not) were obtained. Usage of medications for hypertension and diabetes, including insulin, sulfonylurea, glinide, dipeptidyl peptidase-4 inhibitors, biguanide, thiazolidine, alpha-glucosidase inhibitors, sodium glucose co-transporter 2 inhibitors (SGLT2i), glucagon-like peptide-1 receptor agonist (GLP-1RA), and dyslipidemia, including statin, were obtained from medical records.
Serum was collected after an overnight fast. Serum Cre and CysC levels were measured. SI was calculated as (serum Cre divided by serum CysC)×100.
After at least 5 min of rest in the supine position, the baPWV was measured using a Colin Waveform analyser (PWV/ABI, Colin Medical Technology, Komaki, Japan) as well as both arm and ankle blood pressure. The details of this method have been described elsewhere.28 The Pearson’s correlation coefficients of interobserver and intraobserver reproducibility were r=0.98 and r=0.87, respectively.28 The higher baPWV, with both sides measured, was used as representative for each patient. At same time, the lower ABI, with both sides measured, was used as representative for each patient. A baPWV >1800 cm/s was defined as subclinical atherosclerosis.22
Statistical analysis
The statistical analyses were carried out using the JMP V.13.2.1 software (SAS Institute, Cary, North Carolina, USA). Statistical significance was set at p value <0.05.
Continuous variables were expressed as mean (SD) and categorical variables were expressed as percentage (%) (number). The relationships between CysC, Cre, or SI and baPWV were evaluated by Pearson’s correlation coefficient. The receiver operating characteristic (ROC) analysis was used to calculate area under the ROC curve (AUC) of CysC, Cre, or SI for the presence of subclinical atherosclerosis. Then, logistic regression analyses were performed to evaluate the effect of CysC, Cre, or SI on the presence of subclinical atherosclerosis, adjusting for age, sex, BMI, smoking status, exercise habit, systolic blood pressure, hemoglobin A1c (HbA1c), antihypertensive medication, insulin, SGLT2i, GLP-1RA, and statin usage. Furthermore, subanalyses were performed for patients aged ≥65 years.
Results
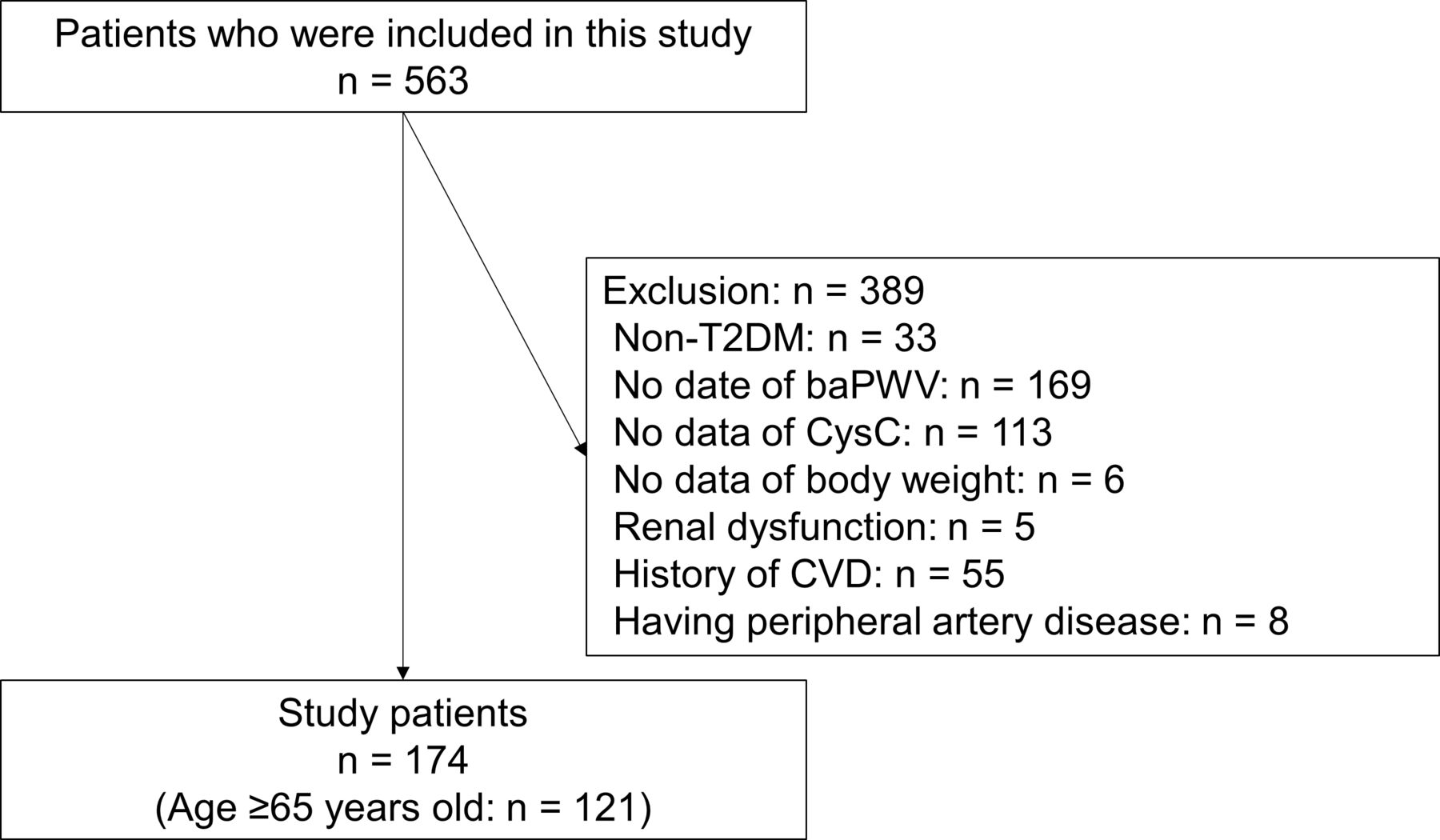
Five hundred sixty-three patients were included in this cross-sectional study. After excluding 389 patients, 174 patients were selected for this study (figure 1). The clinical characteristics of this study patients are shown in table 1. Mean age, duration of diabetes, and baPWV were 66.9 (10.1) years, 17.7 (11.6) years, and 1802 (372) cm/s, respectively. The proportion of subclinical atherosclerosis was 43.7% (n=76).
Clinical characteristics of study participants

Inclusion and exclusion flow. baPWV, brachial-ankle pulse wave velocity; CVD, cardiovascular disease; CyC, cystatin C; T2DM, type 2 diabetes.
Data were expressed as mean (SD) or number (%). SI was calculated as (serum Cre divided by serum cystatin C)×100.
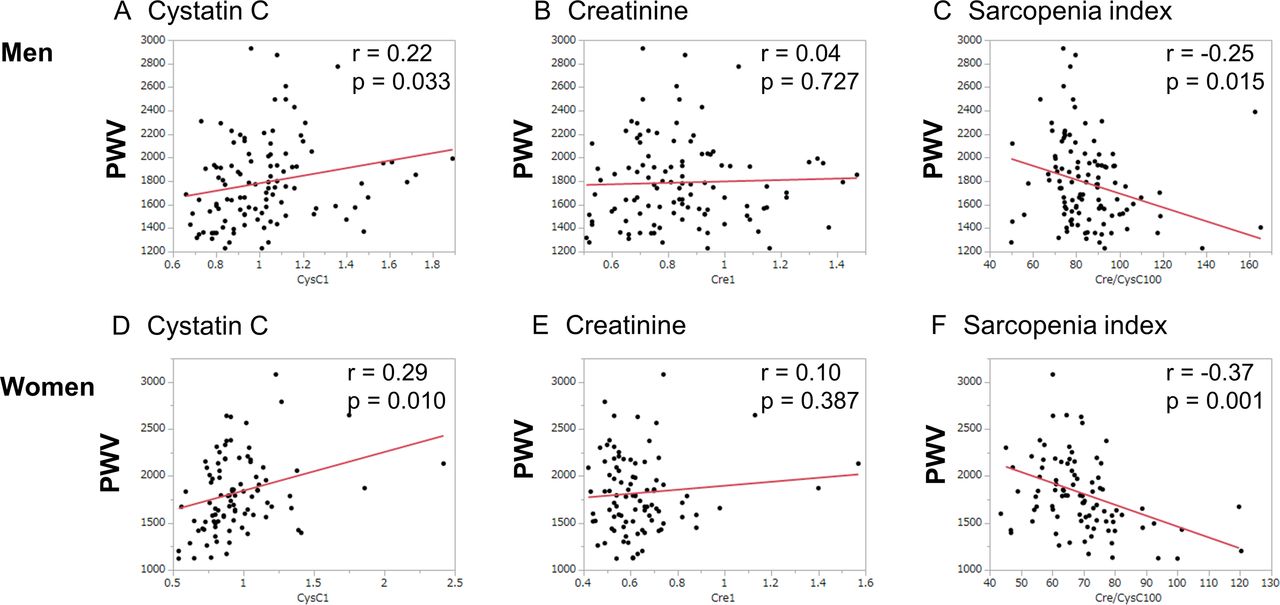
Figure 2 represents the association between CysC, Cre, or SI and baPWV. CysC and SI were related to baPWV, whereas Cre was not related to baPWV in both sexes (figure 2).

Correlation between cysteine C (CysC), creatinine (Cre), or sarcopenia index and brachial-ankle pulse wave velocity (PWV). (A–C) Correlation between cysteine C, creatinine, or sarcopenia index and brachial-ankle PWV among men. (D–F) Correlation between cysteine C, creatinine, or sarcopenia index and brachial-ankle PWV among women.
The AUC of SI for the prevalence of subclinical atherosclerosis (0.66 (95% CI: 0.57 to 0.74)) was superior for that of Cre (0.49 (95% CI: 0.40 to 0.57), p=0.023). Furthermore, the optimal cut-off point of SI for the prevalence of subclinical atherosclerosis was 77.4 (sensitivity=0.72, specificity=0.58, p<0.001) (figure 3A).

Receiver operating characteristic (ROC) curve and area under the ROC curve (AUC) of cysteine C, creatinine, or sarcopenia index for subclinical atherosclerosis. (A) All patients. Red line represents cysteine C (AUC 0.62, 95% CI 0.53 to 0.70), green line represents creatinine (AUC 0.49, 95% CI 0.40 to 0.57), and blue line represents sarcopenia index (AUC 0.66, 95% CI 0.57 to 0.74). The p values of difference of AUC of cysteine C and creatinine, cysteine C and sarcopenia index, and creatinine and sarcopenia index were <0.001, 0.449, and 0.023, respectively. (B) Patients aged ≥65 years. Red line represents cysteine C (AUC 0.53, 95% CI 0.43 to 0.64, p=0.071), green line represents creatinine (AUC 0.53, 95% CI 0.43 to 0.64), and blue line represents sarcopenia index (AUC 0.61, 95% CI 0.51 to 0.71). The p values of difference of AUC of cysteine C and creatinine, cysteine C and sarcopenia index, and creatinine and sarcopenia index were 0.992, 0.272, and 0.071, respectively.
Table 2 shows the ORs of CysC, Cre, and SI for the presence of subclinical atherosclerosis. After adjusting for covariates, SI was related to the prevalence of subclinical atherosclerosis (OR 0.95, 95% CI: 0.91 to 0.99, p=0.015), whereas CysC (OR 1.51, 95% CI: 0.24 to 9.60, p=0.658) or Cre (OR 0.26, 95% CI: 0.02 to 2.80, p=0.263) was not.
Logistic regression analyses for the presence of subclinical atherosclerosis
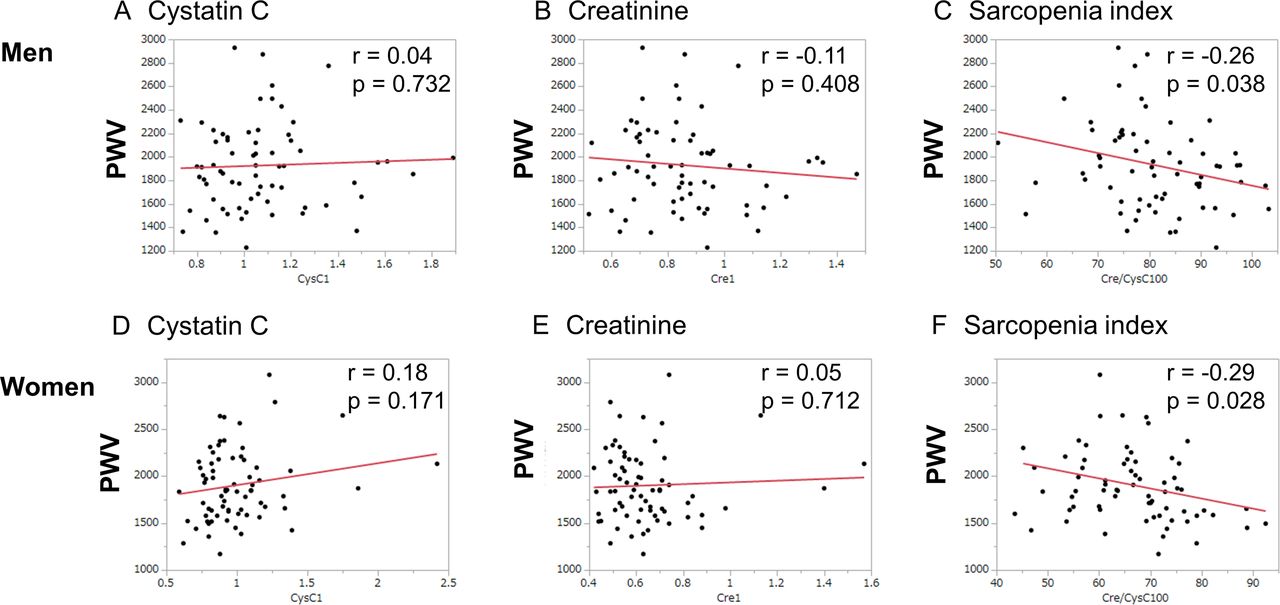
Subanalyses of patients aged ≥65 years were also performed. SI was associated with baPWV, whereas CysC or Cre was not associated with baPWV in both sexes (figure 4). In addition, the AUC of SI for the prevalence of subclinical atherosclerosis (0.61 (95% CI: 0.51 to 0.71)) tended to be superior to that of Cre (0.53 (95% CI: 0.43 to 0.64), p=0.071). Furthermore, the optimal cut-off point of SI for the prevalence of subclinical atherosclerosis was 77.2 (sensitivity=0.70, specificity=0.54, p=0.044) (figure 3B). SI was related to the prevalence of subclinical atherosclerosis (OR 0.94, 95% CI: 0.89 to 0.99, p=0.017), whereas CysC (OR 2.45, 95% CI: 0.27 to 21.9, p=0.424) or Cre (OR 0.43, 95% CI: 0.03 to 5.96, p=0.531) was not, after adjusting for covariates (table 2).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Correlation between cysteine C (CysC), creatinine (Cre), or sarcopenia index and brachial-ankle pulse wave velocity (PWV) among patients aged ≥65 years. (A–C) Correlation between cysteine C, creatinine, or sarcopenia index and brachial-ankle PWV among men. (D–F) Correlation between cysteine C, creatinine, or sarcopenia index and brachial-ankle PWV among women.
Discussion
In this study, we investigated the association between SI and subclinical atherosclerosis in patients with type 2 diabetes mellitus (T2DM) and clarified that there is an association of SI with baPWV and the prevalence of subclinical atherosclerosis.
A recent meta-analysis showed that the proportion of sarcopenia in patients with T2DM was higher than that in people without T2DM.29 Sarcopenia is reported to be associated with a risk of atherosclerosis,30–34 CVD9 35–38 and mortality.10–12 Recent studies showed that SI is useful marker for sarcopenia and physical activity levels.13–15 39 In addition, SI is reported to be associated with incident CVD17 18 and mortality.17 40–42 However, little is known about the association between SI and subclinical atherosclerosis. Recently, Shin43 revealed that there was an association between SI and carotid plaque score in patients with T2DM.
A possible explanation for the association between SI and subclinical atherosclerosis is discussed below. In sarcopenia, the balance between muscle catabolism and synthesis is disrupted due to suppression of the proliferative signaling pathway of skeletal muscle cells and overactivation of the apoptotic signaling pathway.44 Malnutrition, physical inactivity, oxidative stress, hormonal changes, inflammation, insulin resistance, autophagy, and apoptosis and have been implicated in the development of both CVD and sarcopenia.45 Sarcopenia and CVD are closely related through insulin resistance, inflammation, and oxidative stress.44 For example, increased interleukin (IL)-6, which is associated with the degree of atherosclerosis in older patients,46 encourages the catabolism of skeletal muscle and muscle atrophy.47 Increased reactive oxygen species (ROS) causes vasoconstriction and encourages arterial hypertension, promotes the formation of atherosclerotic plaques, and causes vascular endothelial dysfunction.44 The accumulation of ROS leads to sarcopenia by promoting muscle hydrolysis; at the same time, it affects muscle protein synthesis via nitrification.48 In addition, high palmitic acid intake leads to muscle atrophy49 and CVD50 through increasing ROS. These mechanisms are involved in SI and subclinical atherosclerosis.
The limitations of our study should be mentioned. First, since our study is a cross-sectional study, casual nexus is unknown and further follow-up study is needed to clarify this relationship. Second, relatively small number of participants, so there is a possibility that it may not accurately represent the study population. The characteristics, including sex, smoking, BMI, and HbA1c, were not different between analysis group and exclusion group (men, 56.3% vs 60.9%, p=0.304; smoker, 14.4% vs 13.3%, p=0.741; BMI, 23.5 (3.5) vs 24.1 (4.3) kg/m2, p=0.304; and HbA1c, 7.3 (0.9) vs 7.2 (0.9) %, p=0.163), although age of the analysis group was lower than that of exclusion group (66.9 (10.1) vs 70.4 (10.2) years, p<0.001). Third, measurement of markers of inflammation and oxidative stress, such as serum IL-6, 4-hydroxynonenal, and urinary 8-OH-dG may support our hypothesis. Unfortunately, however, we did not measure these markers. Lastly, we only included Japanese patients, thus, it is uncertain that the results of this study generalized to non-Japanese populations, especially non-Asian populations.
In conclusion, SI is associated with the presence of subclinical atherosclerosis in patients with T2DM and this has implications for the management of these patients. Further large-scale prospective studies are needed to clarify the causal nexus.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The Ethical Committee of Kyoto Prefectural University of Medicine approved this study (No. RBMR-E-466-5) and written informed consent was obtained from all participants.
References
Footnotes
Contributors YH designed the study, researched, analyzed, and interpreted data and wrote manuscript; FT researched and interpreted data and contributed to discussion; TOk, TOs, TS, HO, SM, EU, NN, and MA researched data and contributed to discussion; MH conceptualized the study, researched data, and contributed to discussion; MY researched data and contributed to discussion; MF conceptualized the study, researched data, and contributed to discussion. All authors have contributed significantly, and that all authors are in agreement with the content of the manuscript. YH is responsible for the overall content as guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer Direct COI did not exist, however, several potential COI, expressed in supplement manuscript, existed.
Competing interests YH has received honoraria from Kowa Company, Sanofi, Takeda Pharmaceutical, Terumo, and Chugai Pharmaceutical, outside the submitted work. TOs has received honoraria from MSD, Sumitomo Dainippon Pharma, Novo Nordisk Pharma, Daiichi Sankyo, Eli Lilly Japan, Takeda Pharmaceutical, Nippon Boehringer Ingelheim, Mitsubishi Tanabe Pharma Corporation, Kyowa Kirin, Kowa Company, Ono Pharmaceutical, Toa Eiyo, and AstraZeneca, grants from Combi Corporation, outside the submitted work. HO received grant support from the Japan Society for the Promotion of Science and received personal fees from MSD, Mitsubishi Tanabe Pharma Corporation, Sumitomo Dainippon Pharma, Novo Nordisk Pharma, Daiichi Sankyo, Eli Lilly Japan, Kyowa Hakko Kirin Company, Kissei Pharmaceutical, Takeda Pharmaceutical, Kowa Pharmaceutical, Ono Pharmaceutical, and Sanofi, outside the submitted work. TS has received personal fees from Eli Lilly Japan, Mitsubishi Tanabe Pharma, Kowa Pharmaceutical, Astellas Pharma, Takeda Pharmaceutical, Sanofi, Taisho Toyama Pharma, Kyowa Hakko Kirin, Kissei Pharma, MSD, Novo Nordisk Pharma, Ono Pharmaceutical, outside the submitted work. EU received grant support from the Japanese Study Group for Physiology and Management of Blood Pressure, the Astellas Foundation for Research on Metabolic Disorders, the Japan Society for the Promotion of Science, Mishima Kaiun Memorial Foundation and received personal fees from Nippon Boehringer Ingelheim, Mitsubishi Tanabe Pharma Corporation, Daiichi Sankyo, Takeda Pharmaceutical, MSD, Kyowa Hakko Kirin, Sumitomo Dainippon Pharma, Kowa Pharmaceutical, Novo Nordisk Pharma, Ono Pharmaceutical, Taisho Pharmaceutical, AstraZeneca, and Sanofi, outside the submitted work. Donated Fund Laboratory of Diabetes therapeutics is an endowment department, supported with an unrestricted grant from Ono Pharmaceutical, Taiyo Kagaku, and Taisho Pharmaceutical, outside the submitted work. NN received grant support from Japan Society for the Promotion of Science and The Japan Food Chemical Research Foundation, and received personal fees from Kowa Pharmaceutical, and Novo Nordisk Pharma, outside the submitted work. MA received personal fees from Takeda Pharmaceutical Abbott Japan, Sumitomo Dainippon Pharma, Kowa Pharmaceutical, Novo Nordisk Pharma, Ono Pharmaceutical, AstraZeneca, and Chugai Pharmaceutical, outside the submitted work. MH received grants from AstraZeneca, Ono Pharmaceutical, Oishi Kenko, Yamada Bee Farm, Nippon Boehringer Ingelheim and received personal fees from AstraZeneca, Ono Pharmaceutical, Eli Lilly Japan, Sumitomo Dainippon Pharma, Daiichi Sankyo, Mitsubishi Tanabe Pharma, Sanofi, and Kowa Pharmaceutical, outside the submitted work. MY received personal fees from MSD, Sumitomo Dainippon Pharma, Kowa Company, AstraZeneca, Takeda Pharmaceutical, Kyowa Hakko Kirin, Daiichi Sankyo, Kowa Pharmaceutical, and Ono Pharmaceutical, outside the submitted work. MF received grants from Ono Pharmaceutical, Oishi Kenko, Yamada Bee Farm, Nippon Boehringer Ingelheim, Kissei Pharma, Mitsubishi Tanabe Pharma, Daiichi Sankyo, Sanofi, Takeda Pharma, Astellas Pharma, MSD, Kyowa Kirin, Sumitomo Dainippon Pharma, Kowa Pharmaceutical, Novo Nordisk Pharma, Sanwa Kagagu Kenkyusho, Eli Lilly Japan, Taisho Pharma, Terumo, Tejin Pharma, Nippon Chemiphar, Abbott Japan and Johnson & Johnson, Terumo and received personal fees from Nippon Boehringer Ingelheim, Kissei Pharma, Mitsubishi Tanabe Pharma, Daiichi Sankyo, Sanofi, Takeda Pharma, Astellas Pharma, MSD, Kyowa Kirin, Sumitomo Dainippon Pharma, Kowa Pharmaceutical, Novo Nordisk Pharma, Ono Pharmaceutical, Sanwa Kagaku Kenkyusho, Eli Lilly Japan, Taisho Pharma, Bayer Yakuhin, AstraZeneca, Mochida Pharma, Abbott Japan, Teijin Pharma, Arkray, Medtronic Japan and Nipro, Terumo, outside the submitted work. These sponsors were not involved in the study design, in the collection, analysis, or interpretation of data, in the writing of this manuscript or in the decision to submit the article for publication. The other authors have nothing to disclose.
Provenance and peer review Not commissioned; externally peer reviewed.