Article Text

Abstract
The number of patients with diabetes is increasing among older adults in the USA, and it is expected to reach 26.7 million by 2050. In parallel, the percentage of older patients with diabetes in long-term care facilities (LTCFs) will also rise. Currently, the majority of LTCF residents are older adults and one-third of them have diabetes. Management of diabetes in LTCF is challenging due to multiple comorbidities and altered nutrition. Few randomized clinical trials have been conducted to determine optimal treatment for diabetes management in older adults in LTCF. The geriatric populations are at risk of hypoglycemia since the majority are treated with insulin and have different levels of functionality and nutritional needs. Effective approaches to avoid hypoglycemia should be implemented in these settings to improve outcome and reduce the economic burden. Newer medication classes might carry less risk of developing hypoglycemia along with the appropriate use of technology, such as the use of continuous glucose monitoring. Practical clinical guidelines for diabetes management including recommendations for prevention and treatment of hypoglycemia are needed to appropriately implement resources in the transition of care plans in this vulnerable population.
- hypoglycemia
- diabetes mellitus, type 1
- diabetes mellitus, type 2
- geriatrics
Data availability statement
All data relevant to the study are included in the article.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Diabetes mellitus (DM) prevalence is high among older adults, with more than 25% of individuals between 65–75 years and 40% older than 80 years of age are diagnosed with diabetes.1 According to a 2015 analysis of claims from the Centers for Medicare & Medicaid Services (CMS) chronic conditions database, a diabetes diagnosis was listed in nearly one in three Medicare beneficiaries.2 In the US, the majority of older adults with diabetes having type 2, and less than 10% of this population having type 1 DM.3 4 Furthermore, nearly half of adults over 65 years of age meet the criteria for impaired glucose tolerance or pre-diabetes.3 4 From 2000–2018, the percentage of individuals with diabetes who were 65 years or older increased from ~14% to 21.8%.5 In fact, the number of older adults diagnosed with diabetes has increased from 4.7 million in 2000 to 11 million in 2018. This number is projected to double to nearly 26.7 million by 2050.6
The prevalence of diabetes in long-term care facilities (LTCFs) is estimated to be between 20% and 34% in the USA7–13 and around 21.8% across seven different healthcare systems in Europe.14 15 According to the National Center for Health Statistics in 2016, there were 15 600 nursing homes in the USA housing 1.3 million residents,16 with 86% of residents being 65 years of age or older.17 This population of older adults with diabetes residing in LTCF requires individualized approaches to therapy due to higher risk of complications primarily from iatrogenic hypoglycemia and multiple comorbidities.18 In this article, we address the management of diabetes in older adults in long-term care (LTC) settings and discuss approaches to minimize the risk of hypoglycemia.
Challenges of diabetes management in older adults
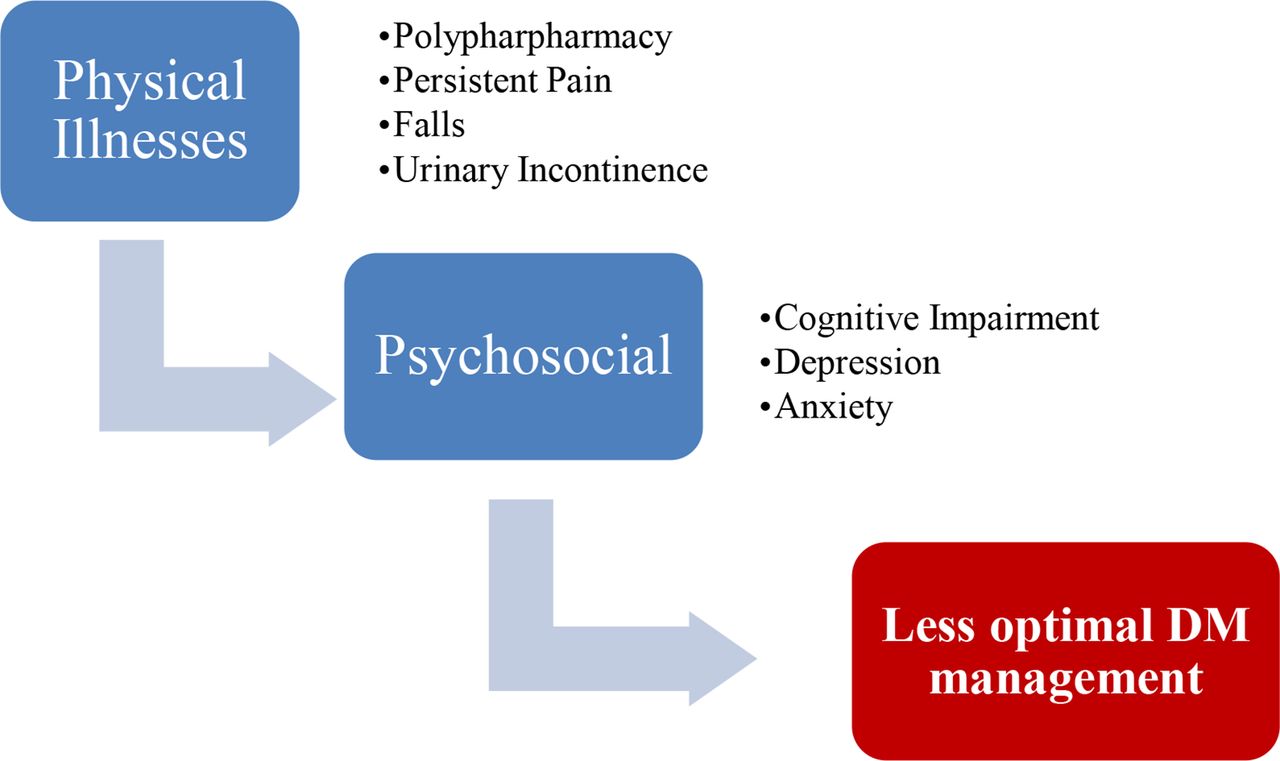
Older adults with diabetes are at higher risk of complications including cardiovascular disease and stroke compared with patients without diabetes.19 In the outpatient settings, more than half of adults with diabetes are codiagnosed with other chronic diseases, and two out of five individuals have more than four comorbid conditions.20–23 In addition, diabetic nephropathy is highly prevalent among older adults with diabetes as nearly half of this population has impaired glomerular filtration rate (GFR), albuminuria or end-stage kidney disease.24 Many other comorbidities occur at high rate among older adults including lower extremity amputations related to diabetic neuropathy, β-amyloid variant Alzheimer disease,25 dyslipidemia,26 falls that lead to fractures,27 28 and hypoglycemia unawareness.29 30 Therefore, older adults are at higher risk of disability and premature death compared with patients without diabetes31 (figure 1). In addition, older adults with diabetes are at greater risk than persons without diabetes for several common geriatric syndromes,32 which make the older adults in LTC settings more vulnerable to hypoglycemia and other complications30 (figure 2). Screening and appropriate management of diabetes and comorbidities can improve outcomes in LTCF residents with diabetes.32

Common diabetes-related comorbidities and frequency of occurrence per age. The incidence of diabetes complications divided by age groups among patients with diabetes (per 1000).204 This figure was reproduced from the CDC data (http://www.cdc.gov/diabetes, accessed 2021). No permission was needed since these data were in the public domain and may be reproduced or copied without permission from CDC. CDC, Centers for Disease Control and Prevention; CHF, congestive heart failure; ESRD, end-stage renal disease; IHD, ischemic heart disease.
{kind=link}
{kind=link}
Common geriatric syndromes in patients with diabetes in long-term care facilities. DM, diabetes mellitus.
Economic burden of diabetes when treating older adults
Older adults with diabetes have a threefold increased risk of being admitted to a hospital or to an acute care setting compared with younger patients.33 34 In fact, national data report more than half of all diabetes-related hospital admissions were in older adults in the period of 2007–2014, with an estimated number of 32 million patients with diabetes over the age of 65 being hospitalized during the same period.5 35
The American Diabetes Association (ADA) estimates the total cost of caring for diabetes has sharply increased by 26% from 2012 to 2017, from $245 billion to $327 billion. The majority of these costs were spent on hospital inpatient care (30%) and treating diabetes complications (30%), with the remaining cost being directed to medications and office visits. Adults over 65 years of age use more health resources compared with younger adults regarding hospital admissions (63% vs 37%), long-term facility use (65% vs %35), and medication prescription (70% vs %30) according to the 2017 ADA report.36 Furthermore, the diabetes-attributable nursing home (NH) costs were estimated to equal $10–11 billion for LTCF residents aged 65–84 in 2013.37
One of the major complications of managing diabetes is hypoglycemia, which contributes to the economic burden of diabetes in older adults. Data from several trials revealed that hypoglycemia in older adults is associated with longer length of stay, complications and further increase in hospitalization cost.38–40 In fact, the yearly cost of medication-induced hypoglycemia among older adults was estimated to equal $509 214 473.41
Transitions of care to LTCFs
LTC refers to a wide variety of services for individuals who require assistance with the activities of daily living (ADLs) or medical care services related to age and/or permanent or temporary conditions that affect the patients’ independent abilities.42 LTCFs provide medical and personal care to their residents. They include NHs, skilled nursing facilities, assisted living facilities, or shorter stay rehabilitative services.43
Most patients admitted to LTCFs are channeled from hospitals following Medicare rule of having three consecutive inpatient calendar days prior to acceptance. However, a smaller number of patients can acquire authorization to be admitted directly from the outpatient settings if they meet certain criteria.44 Providers at LTCFs count on the hospital discharge summaries or the primary care professionals’ instruction to deliver the continuum of care. This transition is generally governed by several guidelines to help providers organize and coordinate health information transmitted so the quality of patient care is assured. One of the major clinical practice guidelines on transition of care comes from the American Medical Directors Association, which fails to incorporate detailed diabetes management strategies in their handbook or in the universal transfer form.45
There is a lack of standardized diabetes management in the older population due to the diverse constellation of comorbidities and the lack of clinical trials in this population. Considering the numerous challenges to manage diabetes in older adults (table 1), several societies have published guidelines for the management of diabetes.
Challenges facing diabetes management at long-term care facility from American Diabetes Association guidelines50 128
These recommendations revolve around improving glycemic control and avoidance of hypoglycemia. It is recommended to follow a conservative glycemic target at LTCF aiming for fasting blood glucose of 100–140 mg/dL and 140–180 postprandially while preventing hypoglycemia.30 The ADA recommends, in healthy functional patients with few coexistent chronic conditions, to target a glycated hemoglobin (HbA1c) of less than 7.5% (53–58 mmol/L). This target is raised to 8.0%–8.5% (64–69 mmol/L) in older adults with multiple coexisting chronic illnesses and cognitive impairment or those who are functionally dependent.32 In older adults who are not treated with insulin or insulin secretagogues, the Endocrine Society clinical practice guideline recommends targeting an HbA1c of less than 7.5%, 8.0%, or 8.5% for patients who are in good, intermediate, and poor health, respectively. For patients using drugs that may cause hypoglycemia (insulin and insulin secretagogues), the Endocrine Society recommends increasing the HbA1c target by 0.5%.30 Further recommendations from Japan Diabetes Society/Japan Geriatrics Society joint committee’s clinical practice guidelines,46 European Diabetes Working Party for Older People 2011 Clinical Guidelines for Type 2 Diabetes Mellitus,47 Diabetes Canada,48 and International Diabetes Federation49 are summarized in (table 2).
Guideline recommendations for key clinical outcomes for older people with diabetes
Currently, guidelines for older adults with diabetes in LTCF prioritize the avoidance of hypoglycemia50–52 and the individualization of therapy. The ADA recommends simplifying treatment regimens and avoiding the use of sliding scale insulin alone. Addressing diabetes goals in older adults residing in LTCF should be conducted in an interdisciplinary manner based on individual comorbidities.50
Several studies have confirmed that glucose control is often tight rather than poor at LTCFs with HbA1c that is lower than the goal for this population.53–58 This may indicate overtreatment since more than 50% of older adults being treated with hypoglycemia-associated drugs (insulin and insulin secretagogues) have an HbA1c that is less than 7% as reported from the National Health and Nutrition Examination Survey.59
Recent developments in antidiabetic drugs portfolio provide an opportunity to optimize diabetes care in LTCFs. Currently, there are 12 glucose-lowering agents with different mechanisms of action.60 Some of the newer agents (dipeptidyl peptidase-4 inhibitors, glucagon-like peptide-1 (GLP-1) receptor agonists and sodium–glucose cotransport 2 inhibitors (SGLT-2i)) are associated with a lower risk of hypoglycemia compared with insulin and sulfonylureas (SUs).60–62 In addition, newer long-acting insulin analogs, such as glargine U300 and degludec insulin, are associated with lower rates of hypoglycemia compared with first-generation basal insulins (Neutral Protamine Hagedorn insulin (NPH), glargine U100 and detemir).63
Hypoglycemia among older adults in LTCFs
Hypoglycemia is a major problem in LTC residents with type 2 diabetes (T2D). A retrospective study of over 1400 residents found that 42% of patients in LTCFs had at least one episode of blood glucose (BG) of <70 mg/dL, and 7% experienced BG of <54 mg/dL.8 Hypoglycemia is most common in patients treated with SUs and/or insulin, with SUs accounting for 18.8% of hypoglycemic episodes and insulin responsible for 64%.8 Other studies have documented hypoglycemia rates up to 34% in patients treated with SUs.58
Hypoglycemia is the main limiting factor for optimizing glycemic control in patients with diabetes. Target HbA1c range should be modified on an individual basis and determined by the patient’s history of hypoglycemia, life expectancy, presence of comorbidities and diabetes complications. Dementia and cognitive impairment put residents at higher risk of hypoglycemia due to failure to recognize symptoms or to communicate those symptoms to caregivers. Furthermore, caregivers may be less able to recognize symptoms of hypoglycemia in patients with underlying cognitive impairment.50 Decrease in β-adrenergic function and lack of adrenergic symptoms, such as palpitations, sweating and tremors, have been reported in older adults with hypoglycemia.64 Neuroglycopenic symptoms, such as confusion, delirium, and dizziness, may be the presenting indicator of hypoglycemia, which can be difficult to differentiate from underlying dementia.65 Other physiological changes in the elderly also exacerbate risk of hypoglycemia. Renal and hepatic impairment can interfere with metabolism of medications, specifically SUs and insulin.66 Age-related changes in counter-regulatory responses also increase the risk of hypoglycemia unawareness.67
Significant morbidity and mortality are associated with hypoglycemia in LTCF residents. The prevalence of hypoglycemia is estimated between 28% and 40%.8 58 68 Hypoglycemia has been associated with increased risk of falls and fractures and cardiac arrhythmias.69 70 In addition, patients suffering from hypoglycemia have longer length of stay (52 vs 29 days, p<0.001), higher rates of emergency room visits or hospitalization (44% vs 31%, p=0.005), and greater mortality 20% vs 10% p=0.002) than those without hypoglycemia.8 Moreover, a randomized controlled trial confirmed increased complications and more episodes of acute kidney injury in patients with hypoglycemia compared with those without.58
Polypharmacy was considered one of the major predictors of severe hypoglycemia in LTCF.40 71 One study reported that LTCF residents receive an average of 7.2 medications, and 69.5% of them had at least one error in their medication reconciliation.72 In Europe, The Services and Health for Elderly in Long Term Care study observed polypharmacy (>5 medications) in 50.7% and excessive polypharmacy (≥10 drugs) in 16.9% of older adults with cognitive impairment.73 Other factors that could lead to hypoglycemia in LTCFs include the partial or the full dependently for ADLs, heterogeneity of nutritional needs, and errors on medications administration.50
Clinical guidelines from professional organizations74–76 recommend the use of subcutaneous insulin, as the preferred therapy for glycemic control for most patients with T2D in LTCFs. Although effective in improving glycemic control, observational and prospective randomized studies have reported rates of hypoglycemia between 30% and 37% with insulin administration in LTCF residents with T2D.58 77 Errors in insulin administration can cause severe hypoglycemia that can impact the individual’s cognition and, if not corrected in a timely manner, can be lethal.32
Several strategies have been proposed to minimize risk of hypoglycemia. Recommendations include simplification of medication regimens, avoidance of insulin secretagogues (SUs), and minimization of sole use of sliding scale insulin. Liberalization of diet may improve food and drink intake and minimize risk of unintentional weight loss. Physical activity should be targeted to the individual resident’s functional capability.50
Hypoglycemia treatment in LTCFs
The best approach to minimize hypoglycemia is by preventing its occurrence in the first place. Most hypoglycemia episodes are preventable, and minimizing their duration and frequency has been proven to decrease mortality.78 Hospitals have implemented several strategies to decrease the occurrence of hypoglycemia such as reviewing patients’ treatment regimen when BG is less than <70 mg/dL.79 This includes monitoring glucocorticoids doses, activity level, oral intake, and enteral or parenteral feedings as well. Hospital protocols aim to evaluate root causes to address systemic issues when hypoglycemia occurs rather than treating it as a separate event.80 To improve synchronization of prandial insulin with mealtime, several strategies are executed in the hospital settings. Some methods include alerting the nurse of meals tray delivery by food staff or standardizing the food delivery schedules.81 A remote surveillance system that allows a diabetes specialist to make recommendations in the patient chart has also been tested. It demonstrated decrease in the hypoglycemia frequency and the approach was widely accepted.82 83 Furthermore, novel approaches are also being studied in hospitalized patients to predict hypoglycemia using machine learning or artificial intelligence embedded in the electronic medical record.84 85 Providers at LTCF could implement some of the strategies that are followed in the hospital, but quality improvement projects and research trials are needed to explore the full effects in such environments.
All hospitals and long-term facilities have instituted a hypoglycemia treatment protocol. These are usually executed by nurses when blood glucose falls below 70 mg/dL and providers are ought to alter the diabetes management regimen to decrease the risk of further severe and very severe hypoglycemia.86 If the patient is able to swallow or has an oral access using gastric or nasogastric tubes, 15 g of carbohydrate should be administered. This equals 4 oz of juices or regular soda, 8 oz of skim milk, or one instant glucose of 31 g tube. If the patient is not able or allowed (nil per os (NPO)) to swallow, a half of dextrose 50 ampule should be given intravenousy for a BG between 41 mg/dL and 70 mg/dL, or a full ampule when blood glucose is less than 40 mg/dL. In both cases, blood glucose should be rechecked in 15 min and the approach can be repeated if glucose remains less than 70 mg /dL. Once hypoglycemia is resolved (>70/mg/dL), the treatment plan should be examined carefully for any possible contributors such as the presence of glucose-lowering medications (eg, SUs) or higher than needed insulin dosage.
Use of glucagon
Glucagon is a hormone that is secreted directly from the α cells of the pancreas.87 It raises blood glucose levels through glycogenolysis and gluconeogenesis in the liver.87 88 The administration of glucagon is considered one of the most important approaches in the treatment of hypoglycemia since it is the primary counter-regulatory hormone to insulin.89 90 The available emergency kits contain a dose of 1 mg of glucagon. After intramuscular, subcutaneous, or inhaled administration, plasma blood glucose levels peak at 26–30 min.91–93
The ADA recommends prescribing glucagon for all patients who are at high risk of severe hypoglycemia. Additionally, instruction should be provided to caregivers or family members of these patients about its administration.94 Despite this recommendation, glucagon safety and availability, it is still underused among patients with diabetes.95–97 Several studies of family members and trained caregivers suggest difficulties using available emergency kits which might indicate the lack of user-friendly products.98 In addition, many physicians and patients with diabetes fail to recognize the importance of glucagon injection. Studies from Japan and Croatia report the underuse of glucagon for both type 1 diabetes mellitus (T1DM) and type 2 diabetes mellitus (T2DM).96 99 In Canada, the percentage of glucagon administration to patients being transferred to the hospital for hypoglycemia was only 40% prehospitalization and less than 1% in the emergency department. Furthermore, the lack of discharge protocol was evident from several emergency departments, with instructions being documented in less than half of the patients, and only 20% were referred to diabetes services.100 In fact, patients discharged from the emergency department following hypoglycemic episodes are at a higher risk of being readmitted within 2 days of a recurrent hypoglycemia.101
If a person is unable to swallow or is unresponsive, subcutaneous, intramuscular, or intranasal glucagon or intravenous glucose should be given by a trained family member or medical personnel. Glucagon for injection is available in prefilled forms ready for intramuscular, subcutaneous, or intravenous administration. Two standard Food and Drug Administration (FDA)-approved formulations of standard glucagon are the GlucaGen HypoKit (Novo Nordisk, Copenhagen, Denmark) and the Glucagon Emergency Kit (Eli Lilly, Indianapolis, Indiana, USA). Both formulations are supplied as lyophilized white powder requiring reconstitution prior to injection as 1 mg per vial. New, more stable formulations of glucagon have recently become available for clinical use: intranasal glucagon, dasiglucagon, and non-aqueous soluble glucagon. These new FDA-approved formulations have demonstrated glycemic responses similar to standard glucagon formulations for the treatment of hypoglycemia but without the need for reconstitution.102 Intranasal glucagon is FDA-approved under the trade name Baqsimi (Eli Lilly) comprising 1 mg glucagon per 10 mg dry powder. Absorption of the powder occurs across the nasal mucosa with a 3 mg glucagon having the maximal effect.103–105 Non-aqueous glucagon solutions (trade name GVOKE) was the first glucagon product approved that can be administered via a prefilled syringe (GVOKE PFS) or autoinjector (GVOKE HypoPen), reducing the steps to prepare and administer glucagon in the event of hypoglycemia.106 107 Dasiglucagon is a novel stable peptide analog of human glucagon consisting of 29 amino acids with 7 amino acid substitutions relative to native glucagon (trade name Zegalogue). In clinical trials, the time taken to increase glucose concentration to above 70 mg/dL was 6 min with doses of 0.3 and 0.6 mg of dasiglucagon, which is comparable to standard glucagon at doses of 0.5 and 1.0 mg.106
There is a lack of clinical trials regarding the use and implementation of glucagon in LTCF protocols. One quality improvement project reported no hospital transfer for hypoglycemia episodes after glucagon was implemented in their protocol.108 Such application could decrease the frequency of severe hypoglycemia in LTC populations and would minimize unnecessary healthcare costs related to hypoglycemic episodes and its poor outcome.
Use of technology in LTCFs
Currently, capillary point-of-care (POC) monitoring is the standard of care to measure glucose levels in the LTCF,50 61 68 which is usually done before meals and at bedtime. In recent years, the use of continuous glucose monitoring (CGM) that measures interstitial glucose levels every 5–15 min has been shown to provide a better assessment of glycemic control and hypoglycemia detection compared with POC capillary testing.
Several randomized trials have shown that CGM technology facilitates and improves diabetes care in insulin-treated ambulatory patients,109–111 as well as in hospitalized patients.112–117 Subjects with T2D treated with basal-bolus insulin therapy in the hospital were studied in combination with CGM use. The detection of both hypoglycemic and hyperglycemic events with the use of CGM was increased compared with the standard-of-care POC testing.114 Furthermore, novel technology has been developed to allow CGM glucose values to be transmitted wirelessly from the patient’s bedside to a central monitoring device in the hospital nursing station. This approach, known as glucose telemetry system with Bluetooth technology, allows for early recognition and treatment of hypoglycemia, thereby reducing the frequency of events in insulin-treated patients with T2D.118–120 About half of the hypoglycemic events in older adults are asymptomatic121 and occurred between dinner and breakfast, indicating that these episodes would be missed by standard POC testing as glucose testing is rarely done during night-time. A recent panel of experts in inpatient diabetes care reported that CGM could effectively identify trends toward hypoglycemia and hyperglycemia, allowing for better and safer management of patients with T2D in facilities.122 123 A recent large study evaluated CGM and POC glucose data from hospitalized patients in the general wards. The results demonstrated a very good overall accuracy of CGM despite comorbidities such as CVD, renal dysfunction, mild–moderate anemia, and respiratory diseases. However, CGM accuracy might be lower in hypoglycemia (<70 mg/dL) or in severe anemia. CGM might also have interferences with some molecules in the bloodstream (acetaminophen >4 g/day, vitamin C, and hydroxyurea); and it is not recommended for patients who are planning to have MRI.124 125 Further research is needed to determine the potential benefits of real-time CGM to improve glycemic control and to prevent hypoglycemia in vulnerable population of adult patients admitted to LTCFs particularly in the era of COVID-19 pandemic.
Medical approaches for older adults with diabetes in LTCFs
Several oral and injectable antidiabetic agents are available for the treatment of diabetes in older adults, which can be used as monotherapy or in combination with insulin (table 3). Claims data from the ambulatory settings suggest that older adults were found to use more long-acting insulin and less of the newer DM medication such as GLP-1a.126 The evidence shows that newer oral antidiabetic drugs can be effective for disease control and less likely to cause hypoglycemia.58 127
Oral antidiabetic drugs: pros and cons in older adults
Insulin
Insulin is frequently used in older adults in LTCFs. It is mostly used when diabetes is not controlled with oral medications, as well as during acute illness, preoperative period, or when the person has severe renal or liver disease.128 Basal insulin analogs (glargine, detemir or degludec) administered starting at 0.1 units/kg/day (or 10 units/day) with slower titration increasing once or two times per week until fasting glucose is less than 150–180 mg/dL or HbA1c<7.5%–8.0%. Basal insulin glargine is also available in a concentrated formulation as insulin glargine 300 units/mL (Gla-300; Sanofi, Paris, France) and degludec U-200 (Novo Nordisk). These formulations of insulin have been studied in older adults with comparable glycemic control to insulin glargine 100 units/mL.129 130
Clinical studies have reported that replacing a sliding scale with a lower dose of basal insulin analogs at a total daily dose of 0.1–0.15 units/kg/day might decrease the risk of hypoglycemia in this frail population.131 132 If basal insulin is not sufficient to control hyperglycemia, the basal bolus approach is recommended starting at 0.2–0.3 U/kg/day divided as 50% basal and 50% prandial coverage.133 However, the use of rapid-acting insulin should be individualized since older adults might have different types of day-to-day living behaviors, which correlate with their dining time and location. Practitioners should also consider LTCF policies in reference to mealtime insulin administration since numerous logistical planning need to be in place. For example, the location of administration (resident private room vs dining room) and the timing of insulin injection in reference to food arrival could significantly affect blood glucose control. More data are needed to generate guidelines which are specific to diabetes management in LTCF.
Metformin
Metformin is the most commonly used antidiabetic drug for the management of T2D and acts by decreasing hepatic glucose production through multiple molecular mechanisms.134 Metformin has a low risk of hypoglycemia and is weight neutral, making it an attractive option. Metformin contraindications are limited to impaired renal function with estimated glomerular filtration rate (eGFR) of <30 mL/min/1.73 m2, acute HF or active decompensated liver disease.135 136 In addition to the clinical benefits, metformin is inexpensive, which allows for its use as first oral choice in the treatment of T2D, including institutionalized older adults. Metformin is known to cause gastrointestinal (GI) adverse events such as nausea and diarrhea, complicating the management in older adults who might suffer from decreased oral intake and are at a higher risk of dehydration.137 Metformin has been associated with increased risk of lactic acidosis if used in patients with impaired kidney function.138 Guidelines for diabetes management recommend holding metformin in the hospital. The acute changes during hospitalization such as dehydration and renal or hepatic dysfunction might further exacerbate the possibility of developing lactic acidosis, particularly if they receive contrast media.139 140 However, the environment at LTCF is considered less acute, yet no studies have evaluated the use of metformin in these settings. In summary, more trials are needed to evaluate the benefits and risks of using metformin among LTCF residents. Metformin remains a preferred option for geriatric individuals compared with other agents that could cause hypoglycemia and increase mortality risk.137 Nonetheless, practitioners could prescribe this agent in the older adult population, taking into consideration the risk of lactic acidosis and dehydration from the decrease oral intake. Metformin dosage can be started at 500 mg/day and titrated up as tolerated to a maximum of 2000 mg/day in a normal GFR. Providers could opt for extended-release versions to minimize the risk of intolerance.
Insulin secretagogues
SU stimulates insulin secretion by activating SU receptors on B cells.141 142 The major side effect is hypoglycemia, especially in the case of irregular caloric intake, decreased renal function, and polypharmacy, which are common in older adults in LTCF. Studies have associated SU use with poor outcome and a 7% to 10% mortality rate among patients with SU-induced hypoglycemia.8 143 The use of SU has been associated with higher all-cause mortality compared with metformin144 and an increased risk of fractures in older population with T2DM.145
Metiglinides have a shorter half-life and include nateglinide and repaglinide. They are used preprandially and have a similar mechanism of action as SUs which could lead to hypoglycemia risk.146 It is worth noting, however, the lower rates of severe hypoglycemia with metiglinides when compared with SU in RCTs involving older adults.147–150
Clinical studies on the use of insulin secretagogues in LTCF are lacking. On the other hand, their use in hospital settings is not recommended by professional societies151 152 due to the possible risk of hypoglycemia among older adults who might suffer from renal dysfunction. Providers should probably follow these recommendations in LTCF pending more concrete evidence about their safety and benefits. Nonetheless, if these agents are to be considered in LTCFs, health professionals should elect short-acting insulin secretagogues that have lower risk of hypoglycemia in the settings for renal impairment such as glipizide or metiglinides.153 154 Additionally, metiglinides are usually more expensive than SU, should be adjusted for GFR, and ought not be used in older patients with erratic eating behaviors.
Thiazolidinediones (TZDs)
These drugs work as peroxisome proliferator-activated receptor (PPAR) agonists and regulate carbohydrate and lipid metabolism, enhance tissue response to insulin, and have favorable effects on endothelial function and inflammation.155 TZDs are metabolized by the liver, so they can be used in the setting of impaired renal function. The use of TZDs can cause fluid retention, peripheral edema, weight gain, macular edema and heart failure (HF).156
Prescribing this class of medicine to LTCF residents should be considered after exhausting other options. The prevalence of HF among older adults in LTCF is estimated to equal 20%–37.4%,157 and using TZD might increase the risk of readmission to the hospital for HF exacerbation or even death.157 158 Furthermore, older adults have more prevalence of osteoporosis or osteopenia and TZD has been associated with a higher rate of fractures, particularly in postmenopausal women.159–162
Alpha-1 glucosidase inhibitors
This family of medications include miglitol and acarbose. They are a group of drugs that slow carbohydrates absorption by blocking the action of brush border enzymes (alpha glucosidases) and increasing GLP-1 levels. They primarily work on postprandial hyperglycemia.163 These agents have the advantage of not causing hypoglycemia;156 however, use is limited due to GI side effects such as flatulence, abdominal pain and abdominal cramp.164
Despite their safety, the use of this agent in older adults residing at LTCF is not routinely followed due to the lack of clinical trials in this population and the higher rate of GI side effects. The half-life of this medicine is short and requires frequent administration, which might be challenging in LTCF.163
Dipeptidyl peptidase-4 (DPP-4) Inhibitors
This class of medication acts on dipeptidyl peptidase-4 enzyme that degrades endogenous secretion of GLP-1. Inhibiting this enzyme increases the availability of GLP-1, resulting in increased insulin secretion and reducing glucagon release. This family of drugs improves fasting and postprandial glucose levels; they are well tolerated and can be taken as monotherapy or in combination with other oral antidiabetic medications.165 166 These drugs are convenient to use in older adults because they can be used in the setting of renal dysfunction, have limited side effects, and have a low rate of hypoglycemia.167 A randomized controlled study showed that the DPP-4 inhibitor is as effective as insulin glargine for glucose control with significant lower risk of hypoglycemia in LTCF residents with T2D.77 155 A prospective randomized 6-month open-label randomized controlled trial compared the efficacy and safety of linagliptin versus basal insulin glargine of a total of 140 residents with T2DM in three LTCFs affiliated with community safety-net hospitals. Both groups had similar mean daily glycemic control, but compared with glargine, the group treated with linagliptin had fewer mild hypoglycemic events of <70 mg/dL (3% vs 37%).77
Glucagon-like peptide 1 receptor agonists (GLP1-RAs)
GLP1 is an incretin hormone that stimulate insulin secretion in a glucose-dependent manner. In addition, they promote delayed gastric emptying and inhibit the production of glucagon, which further decrease glucose levels.77 HbA1c can decrease by approximately 1.0%–1.5% when using this drug, along with weight loss of about 2–5 kg.168 Clinical trials have demonstrated that GLP1-RA have cardiovascular benefits among patients with established atherosclerotic cardiovascular disease.169 170 Several studies have demonstrated the renal protection of GLP1-RA171–173 and possible positive effects on cognitive and memory functions.174 175 They may work through blood glucose and blood pressure lowering, reduction of insulin levels and weight loss,176 and lower inflammatory state, which can reduce albuminuria and prevent the decline of renal function in patients with diabetes.177
Healthcare professionals should be aware that most of GLP1-RAs are injectable once per day or per week and require visual, motor, and cognitive skills for administration. Furthermore, the GI side effects such as nausea and diarrhea are reportedly commonly (10%–28%),178–180 whereas vomiting and other adverse effects were noted less frequently (2%–12%), and these add to the limitation of their use in older adults.181 To minimize GI side effects, providers at LTCFs should start with the lower dosage and increase gradually every 1–2 weeks to reach the maximal tolerated dose. The nutrition status of the resident should be also considered since the prevalence of malnutrition is estimated to equal 18%–21% across studies.182 183
Sodium–glucose cotransport 2 inhibitors
SGLT-2is are a group of drugs that lowers the reabsorption of glucose in the proximal convoluted tubule of the nephron by inhibiting the sodium-glucose transport protein 2, therefore promoting the excretion of the glucose in the urine and lowering blood glucose.184 These drugs lower the HbA1c by approximately 1% and contribute to modest weight loss of 1–3 kg.185 186 It can be used as monotherapy or combined with other oral antidiabetic drugs and/or insulin. Apart from the antidiabetic effect, SGLT-2is have been found to have cardiac and renal protection in patients with diabetes.187 SGLT-2is reduced hospitalization for HF by 23% in patients with diabetes and reduced the progression of renal disease by 45%.188 The use of SGLT-2is is now recommended by clinical guidelines for the management of T2D in patients with coexisting HF and diabetic kidney disease.189 190 Nearly 20.0%–37.4% of LTCF residents are diagnosed with HF;157 however, no studies have evaluated SGLT-2i safety and efficacy on decreasing HF admission in these settings.
A meta-analysis on the cardiovascular outcome trial on the use of this drug class showed that the efficacy for older adults reported an OR for major adverse cardiovascular events (MACEs) of 0.95 (95% CI 0.86 to 1.05) in people <65 years old and 0.83 (95% CI 0.71 to 0.96) for people >65 years old.191
Adverse effects reported with the use of SGLT-2is include urinary tract infections (UTIs) and yeasts infections.192 In patients with T1DM, SGLT-2is have been associated with increased risk of euglycemic diabetic ketoacidosis, but this complication is rare in patients with T2D.193 The use of SGLT-2is in LTCF has not been evaluated by RCT, but previous clinical trials have included older adults. This class of medicine was found to be effective, safe, and provided cardiorenal benefits in the geriatric population, but caution should be exercised when initiating in LTCF.194 195 First, UTI is the second most common infection in LTCF,196 and the prevalence of asymptomatic bacteriuria is estimated at 18%–57%.197 Administering SGLT-2is might theoretically increase the risk of developing or worsening UTI if perineal hygiene was not followed in these settings. Second, the osmotic diuresis effects of using this class of medicine might be problematic in older adults who are at risk of dehydration, particularly if they are on loop diuretics.198 Blood pressure and GFR should be monitored if SGLT-2is were to be started or continued in LTCF. A slight decrease in GFR is expected after initiating this medicine, but there is evidence that their use is safe in mild or moderate renal dysfunction.199 Furthermore, almost 70.3% of LTCF residents suffer from urinary incontinence and the use of these medications might impact this issue negatively due to the diuresis effects.200 Third, the scarcity of data in older adults with frailty and these agents might not support using them in this population yet. Therefore, more studies are needed to evaluate the safety and efficacy of using SGLT-2is in LTCF.
Combination therapy
Many diabetes agents are available in combination therapies which might be beneficial in older adults to decrease the burden of polypharmacy. It is possible now to offer different oral agents in one tablet. This will improve compliance and lead to lower HgA1c. The most common agents include combination of metformin with either SGLT-2i, or incretin agents201 202 and a newly approved triple combination therapy of metformin, SGLT-2i, and incretin agents.203 204 Furthermore, new advances have allowed the combination of long-acting insulin and GLP1a therapy in one injection. This approach might be favorable to older adults since it will decrease the number of injections significantly. In addition, long-acting insulin/GLP1a combination might replace insulin-bolus therapy, which will probably lead to a decrease in the risk of hypoglycemia in older adults and possibly improve the quality of life.205–208
Conclusion
Older adults have diverse clinical profiles and their health status undergo rapid and acute changes which can affect glucose control. Thus, the management of diabetes can be affected based on the living environment and the amount of social, physical, and psychological support provided. With the prevalence of older adults with diabetes increases in the future, the percentage of older patients with diabetes in LTCFs will also rise. This will generate numerous challenges to control blood glucose in these settings since older adults admitted will have various levels of functionality, different sets of comorbidities, and distinct life expectancy. Most of the LTCF residents are on insulin alone and/or oral regimens, resulting in increased risk of hypoglycemia.
Optimizing cost-effective approaches to treat older adults with diabetes safely will provide an improved outcome in morbidity and mortality along with decreasing the economic burden. Currently, major diabetes guidelines lack the direction needed to screen and recognize hypoglycemia risks, or the interventions needed to treat acute severe hypoglycemia for older adults in long-term settings. These facilities are expected to develop their own practice procedure to treat hypoglycemia which currently lacks the use of glucagon. This agent might effectively reduce prehospital hypoglycemic complications if encompassed in the transition of care plans of older adults.
Data availability statement
All data relevant to the study are included in the article.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Footnotes
Contributors TI, IAC-R, ALM, and GEU have participated in writing and reviewing the manuscript. EMM has participated in reviewing the manuscript. All authors provided critical feedback and helped shape the research, analysis, and manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests GEU is a member of the BMJ editorial board.
Provenance and peer review Not commissioned; externally peer reviewed.