Article Text

Abstract
Introduction Leucocyte telomere length (LTL) is linked to accelerate aging and premature mortality. In this research, we aimed to explore the relations between biochemical and anthropometry markers and LTL in Asian Indian women with abnormal fasting glycemia (impaired fasting glucose).
Research design and methods In this study, 797 pre-diabetic women (obese, 492; non-obese, 305) were recruited. Demographic and clinical profiles, anthropometry, and fasting blood glucose were evaluated. LTL was quantified by a quantitative PCR. LTL was expressed as the relative telomere length or telomere repeat:single copy gene (T:S) ratio. The subjects were separated into quartiles according to the LTL.
Results The average LTL was significantly decreased with increasing age. The average LTL was significantly shorter in obese women with abnormal fasting glycemia (p<0.05). R-squared (R2) statistic for multivariable linear model after adjusted for age, family income, education and hypertension showed that LTL was inversely correlated with body mass index (BMI), waist and hip circumference, waist-hip and waist-to-height ratio, truncal skinfolds (subscapular, and subscapular/triceps ratio, central and total skinfolds), fat mass (kg) and % body fat. The relationship between obesity measures and LTL (using the LTL quartile 1 as reference) identified central skinfolds (R2=0.92, p<0.0001), Σ4SF (R2=0.90, p<0.0001), BMI (R2=0.93, p<0.0001) and % body fat (R2=0.91, p<0.0001) as independent predictors of LTL.
Conclusions Besides age, obesity and subcutaneous adiposity (predominantly truncal) are major contributors to telomere shortening in Asian Indian women with abnormal fasting glycemia (impaired fasting glucose).
- aging
- obesity
- Asian Indians
- pre-diabetic state
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Leucocyte telomere length (LTL) is linked with aging and associated diseases, such as obesity, type 2 diabetes, and cardiovascular disease.
WHAT THIS STUDY ADDS
This is the first study to investigate the relationship of LTL in women with abnormal fasting glycemia (impaired fasting glucose). Specifically, relationship of LTL with subcutaneous adiposity, particularly truncal adiposity, is being reported in women for the first time.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
In women with abnormal fasting glycemia, obesity and truncal obesity should be targets of lifestyle and drug management for inducing salutary effects on LTL.
Introduction
Abnormal fasting glycemia (impaired fasting glucose) and type 2 diabetes (T2D) are increasing in developing countries.1 South Asians develop diabetes a decade before and at a lower body mass index (BMI) than white population, have prominent abdominal obesity, and accelerated conversion from abnormal fasting glycemia to diabetes.2 Importantly, India has one of the maximum number of people with abnormal fasting glycemia and diabetes.3 Our previous studies have shown increasing obesity and diabetes in Asian Indian women.4 Diabetes can have serious health implications that affect life expectancy. The UK Diabetes Study stated a 5-year decrease of life expectancy for men aged 45–50 years at the time of diagnosis of diabetes when compared with the common population.5 Data from the Emerging Risk Factor Collaboration likewise showed that life years lost were significantly larger when diabetes is present at earlier ages.6
Telomerase is an important enzyme that maintains leucocyte telomere length (LTL) and cellular replicate potential. LTL naturally shortens with each cell phase, and cells with critically short telomere undergo replicative senescence and apoptosis, which promote organismal aging and age-related diseases. LTL shortening is accelerated by oxidative stress, inflammation, and cell production.7 Hornsby et al8 have reported that telomere shortening resulting from the absence of telomerase activity may be a factor in determining some age-related properties of organs in humans. Given that telomerase, the enzyme responsible for maintaining telomere lengths is not expressed at levels sufficient to prevent telomere shortening in most of our cells, and telomeres progressively erode with advancing age.9 Short LTL in peripheral blood mononuclear cells is linked with aging and its related diseases, such as obesity, T2DM, and cardiovascular disease.10
A systematic review and meta-analysis included 63 original studies (n, 119 439) showing a negative correlation between obesity and telomere length.11 The selected studies showed weak to moderate statistical significance, and there was heterogeneity. For this reason, the causal relationship of obesity and telomere length remains controversial. German administrative claims data (n, 2 900 065) showed that T2D is inter-related to lower life expectancy regardless of an individual’s socioeconomic status for individuals in Lower Saxony, Germany.12 Another review on LTL in different metabolic categories indicated that LTL was negatively related to 2-hour postprandial blood glucose and the relationship with increasing fasting plasma glucose may be non-linear.13 It was possible that these data along with reports of the possibility of modifying LTL can improve the understanding of present-day epidemiological trends in incidence and mortality of T2DM. There are no published data regarding pre-diabetes and shortening of lifespan in Asian Indians.
There have been few intervention trials to assess LTL. Lifestyle and dietary interventions were conducted in 217 elderly Italian subjects stratified according to Mediterranean diet score (MDS) (low adherence (MDS ≤3), medium adherence (MDS 4–5), and high adherence (MDS ≥6) groups). These authors have shown that the high adherence group showed following compared with other two groups showed longer LTL and higher telomerase activity. These results support benefits of Mediterranean diet in promoting health span.14
There is paucity of data regarding leukocyte telomerase activity and LTL in individuals with abnormal fasting glycemia. It is important to note that effects of pistachio intake on LTL have been shown in only one previous study, in which limited number of Spanish subjects (n, 49) having abnormal fasting glycemia were recruited.15 Although these findings suggested that shorter LTL might be associated with increased risk of abnormal fasting glycemia, their significance was limited by small sample size, cross-sectional observation, and short follow-up period. Further, association between LTL, abnormal fasting glycemia, and obesity in Asian Indians has not been researched.
To better highlight this knowledge gap, we proposed to investigate the relationship of LTL in abnormal fasting glycemia with obesity in community dwelling Asian Indian women residing in New Delhi, North India. We have selected women for this study since we have been previously researching various non-communicable diseases, including abnormal fasting glycemia, in this group.16 17
Research design and methods
Subject recruitment
We carried out a cross-sectional population-based study from July 2015 to December 2020. One thousand three hundred and sixty-one women were randomly selected from North India (aged 20–60 years) and were residing in the area for more than 6 months. Among this group, 797 women were categorized as having impaired fasting glucose (plasma glucose concentrations between 100 and 125 mg/dL) (obese, 492; non-obese, 305). Study subjects were randomly designated to have approximate representation from each income group (higher ~10%, middle ~65%–70%, and lower ~15%–20%) from 41 residential sites in Delhi. Subjects were excluded if any of the following criteria applied: (1) T2D or use of oral antidiabetic drugs; (2) alcohol, tobacco, or drug abuse; (3) any medication which could affect insulin sensitivity; (4) those with pregnancy; (5) severe end-organ damage or chronic diseases; (6) malignancy and other endocrine disorders; (7) significant liver, kidney, thyroid, or other endocrine diseases.
Demographic characteristics and clinical profile
Demographic characteristics, clinical profiles, medical history (personal and family), socioeconomic features, skin exposure, and duration of sunlight exposure were determined with the use of prevalidated questionnaire. Skin exposure was measured as percentage of body surface area (face/hands, face/hands and arms, and face/hands and legs) exposed to sunlight. The duration of sun exposure (minutes/day) was measured in the following manner: <5 min, 5–15 min, 15–30 min, and >30 min. Blood pressure was recorded by a standard mercury sphygmomanometer, over the right arm in sitting position.
Anthropometric measurements
BMI, circumferences (waist circumference (WC) and hip circumference (HC)) and skinfold thickness at four sites (biceps, triceps, suprailiac and subscapular) were recorded.17 Waist-hip ratio (WHR) and waist-to-height ratio (W-htR) were calculated. Sum of all skinfolds (Σ4SF, total skinfolds), ratios of subscapular and triceps skinfolds (SS/TR ratio), central skinfolds (sum of subscapular and suprailiac), and peripheral skinfolds (sum of biceps and triceps) were also calculated. Percentage body fat and fat mass (kg) were calculated using sum of 4 skinfolds with Durnin and Womersley method.18 19
Biochemical analysis
Venous blood sample was collected into vacutainer tubes containing plain and EDTA vials. The fasting blood sample was processed into different aliquots (including whole blood and blood clot) within 2 hours into 1.0 mL FluidX tubes (FluidX, Cheshire, UK) and frozen at −80°C freezer (Thermo Fisher Scientific, Waltham, Massachusetts, USA). Fasting blood glucose (FBG) levels were analyzed as previously described.17 Estimation of FBG and LTL was done on the same blood sample.
DNA isolation and quantification
DNA was separated from peripheral blood mononuclear cells using the QIAamp DNA extraction kit (Qiagen, Hilden, Germany) and stored at −20°C for the future experiments.20 After DNA isolation, the DNA samples were quantified and diluted to 50 ng/µL. The concentration and quality of DNA were both measured by using a nanodrop (Nanodrop Technologies, Wilmington, North Carolina, USA), and samples included for analysis all had an optical density ratio A260/A280 >1.8.
Measurement of leucocyte telomere length
LTL was analyzed with a quantitative PCR (qPCR)-based technique that compares telomere repeat sequence copy number (T) with a reference single copy-gene copy number (S) as previously described.21 22 The telomere length for each sample was estimated using the telomere to single copy gene ratio (T/S ratio) with the calculation of ∆Ct [Ct(telomere)/Ct(single gene)]. T/S ratio for each sample (x) was normalized to the mean T/S ratio of the reference sample [2−(∆Ctx−∆Ctr)=2−∆∆Ct], which was used for the standard curve, both as a reference sample and as a validation sample. The measurement consists of determining the relative ratio (T/S ratio) of nanogram of telomere (T) to nanogram of albumin (single-copy gene, S) in experimental samples using a standard curve. The T/S ratio is proportional to the average telomere length. All qPCR assays were performed using filtered pipette tips to prevent amplification of contaminants. Reactions were set up on ice to prevent DNA polymerase activity, non-specific amplification and to minimize potential primer dimerization. All analyses were done blinded to cross -sectional status of the individual.
The coefficient of variations (CVs) of the interplate T/S were 11.6% and 12.2% for the long and short telomere QC samples, respectively. Interplate and intraplate CVs of calibrator DNA samples were 10.2% and 8.3%, respectively. Mean ratio of long to short telomere QC samples in our assays was 3.9 with 4.5% CV. All samples in our study were assayed in triplicate, and the results were consistent. Less than 12% of samples had a T/S CV more than 10%.
Definitions
Overweight and obesity were defined as BMI 23–24.9 kg/m2 and >25 kg/m2, respectively.23 Abnormal blood pressure was ≥130/85 mmHg. Abnormal fasting glycemia was defined as FBG levels >100 and 125.9 mg/dL. LTLs were categorized in quartiles, 0–25th percentile (1st quartile; LTL ratio <0.83), 26th–50th percentile (2nd quartile, LTL ratio 0.84–0.87), 51st–75th percentile (3rd quartile, LTL ratio 0.88–0.93), and 76th–100th percentile (4th quartile, LTL ratio 0.94–0.98). Because several values of LTL were gathered around cut-off values of quintiles, slightly changed numbers of subjects were separated in each quintile.
Statistical analysis
Complete data was entered in an Excel worksheet (Microsoft, Redmond, Washington, USA). The distribution of demographic, clinical profiles, socioeconomic, medical history (personal and family), behavioral characteristics, sun and skin exposure and biochemical investigations were confirmed for estimated normality. Mean, SD and number (%) was used to summarize the variables. Relationships between LTL and various indices of body composition were identified by Pearson correlation analyses. Body fat percentage and fat mass (kg) were also calculated.
Bivariate relationships of LTL (Pearson correlation and Spearman’s r) with obesity measures variables were examined first. Associations with LTL were estimated using partial correlations that adjusted by age, family income, education, and hypertension.
Associations of categorical variables were assessed by χ2/Fisher’s exact test. The continuous variables were compared between obesity by independent t-test/Wilcoxon rank-sum test, as appropriate. The comparisons of clinical, biochemical, anthropometry and body composition profiles among different LTL quartiles were performed by means of analysis of variance and Kruskal-Wallis test, as appropriate, and further trend was seen by non-parametric trend test. Univariate and multivariable linear regression analyses were used to find independent effect of obesity measures on LTL after adjusting for confounders. Complete analyses were performed using Stata 14 (Stata, College Station, Texas, USA). For all above, p value of <0.05 was considered as statistically significant.
Results
Clinical and biochemical profiles
Educational status, employment status, family income, personal history of hypertension, family history of heart disease, skin exposure (face and hands) to sun were significantly higher in obese subjects with abnormal fasting glycemia as compared with those with non-obese with abnormal fasting glycemia (online supplemental tables 1 and 2).
Supplemental material
The mean±SD for age was 42.02±11.4 years. Mean age, systolic and diastolic blood pressure, weight, BMI, circumferences, and ratios thereof (WC, HC, W-HR, W-htR), skinfold thickness and ratios thereof (biceps, triceps, subscapular, suprailiac, Σ4SF, subscapular/triceps ratio, central and peripheral) and FBG levels were significantly increased in obese subjects with abnormal fasting glycemia as compared with those with non-obese with abnormal fasting glycemia.
Leucocyte telomere length
LTL was significantly decreased in older subjects as compared with younger subjects (online supplemental figure 1). Mean values of LTL were significantly decreased in obese subjects with compared with those with non-obese and overweight (online supplemental figure 2). After stratifying the sample according to LTL quartiles, we observed age, systolic and diastolic blood pressure, weight, BMI, circumferences, and their ratios (WC, HC, W-HR, W-htR), skinfolds (biceps, triceps, subscapular, suprailiac, Σ4SF, subscapular/triceps ratio, and peripheral and central skinfolds; see table 1), % body fat, body fat mass (kg) and FBG levels were significantly increased in first quartile as compared with other quartiles.
Supplemental material
Supplemental material
Demographic and clinical profiles, body composition, and biochemical investigations of the subjects according to quartile of LTL
Partial correlations
We observed a significant partial correlation of LTL with subscapular/triceps ratio (r=−0.4371, p=0.00001), central skinfolds (r=−0.8375, p=0.0001), Σ4SF (r=−0.8560, p=0.00001), FBG (r=−0.1234, p=0.00001), BMI (r=−0.8783, p=0.00001), % body fat (r=−0.8986, p=0.00001), and W-htR (r=−0.1672, p=0.0001), adjusted by age (figure 1).

Partial correlations between leucocyte telomere length (LTL) and skinfold thickness. (A) Subscapular/triceps ratio (r=−0.4371; p=0.0001), (B) central skinfolds (r=−0.8375; p=0.0001), and (C) total skinfolds (r=−0.8560; p=0.0001); (D) waist-height ratio; (E) body mass index; and (F) % body fat adjusted by age.
Univariate and multivariable linear regression analyses to identify factors associated with LTL
The univariate and multivariable regression analyses showed that LTL was inversely correlated with BMI, WC, HC, W-HR, W-htR, subscapular, Σ4SF, subscapular/triceps ratio, and central skinfolds. Further, R2 statistic for multivariable linear model after adjusted for age, family income, education, and hypertension LTL was significantly related to BMI (R2=0.79), WC (R2=0.83), HC (R2=0.78), W-HR (R2=0.43), W-htR (R2=0.72), subscapular skinfolds (R2=0.66), central skinfolds (R2=0.73), Σ4SF (R2=0.75), and % body fat (R2=0.75) (table 2).
Regression analysis showing effect of obesity measures on leucocyte telomere length
Relationship between obesity measures and LTL according to LTL quartiles
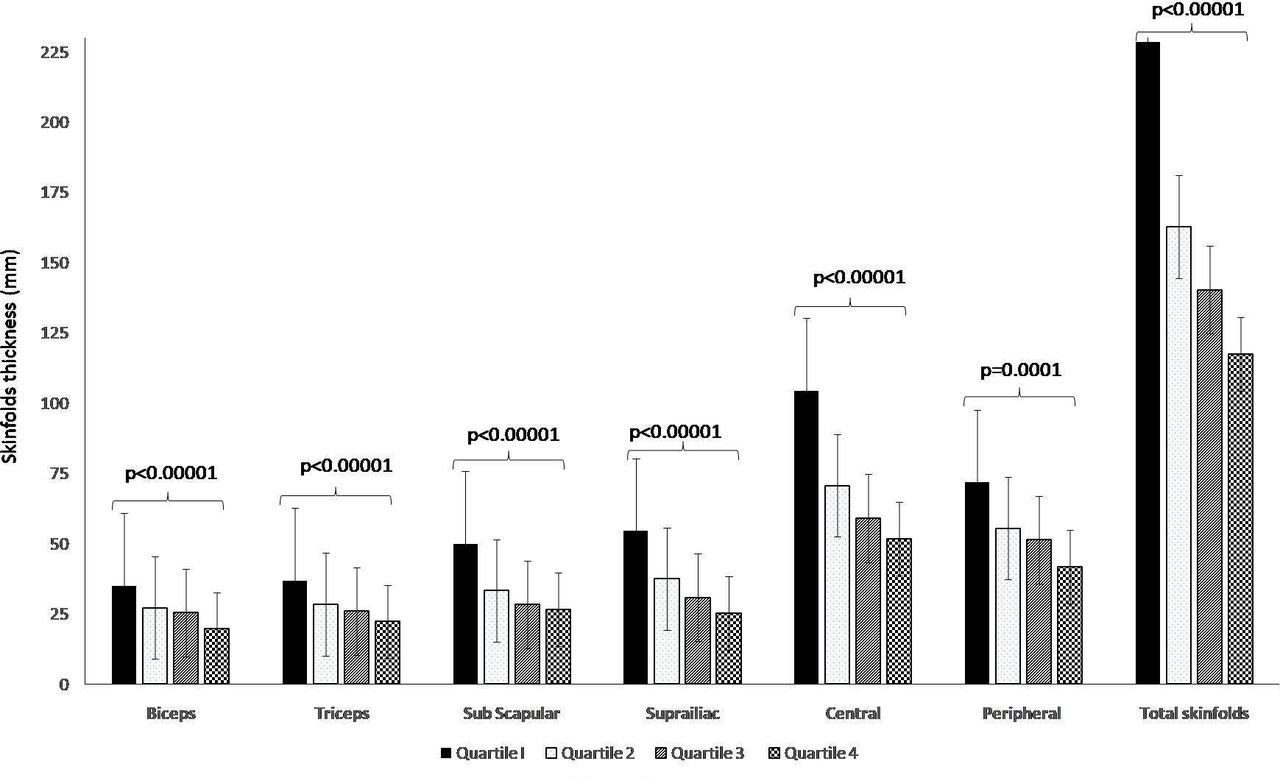
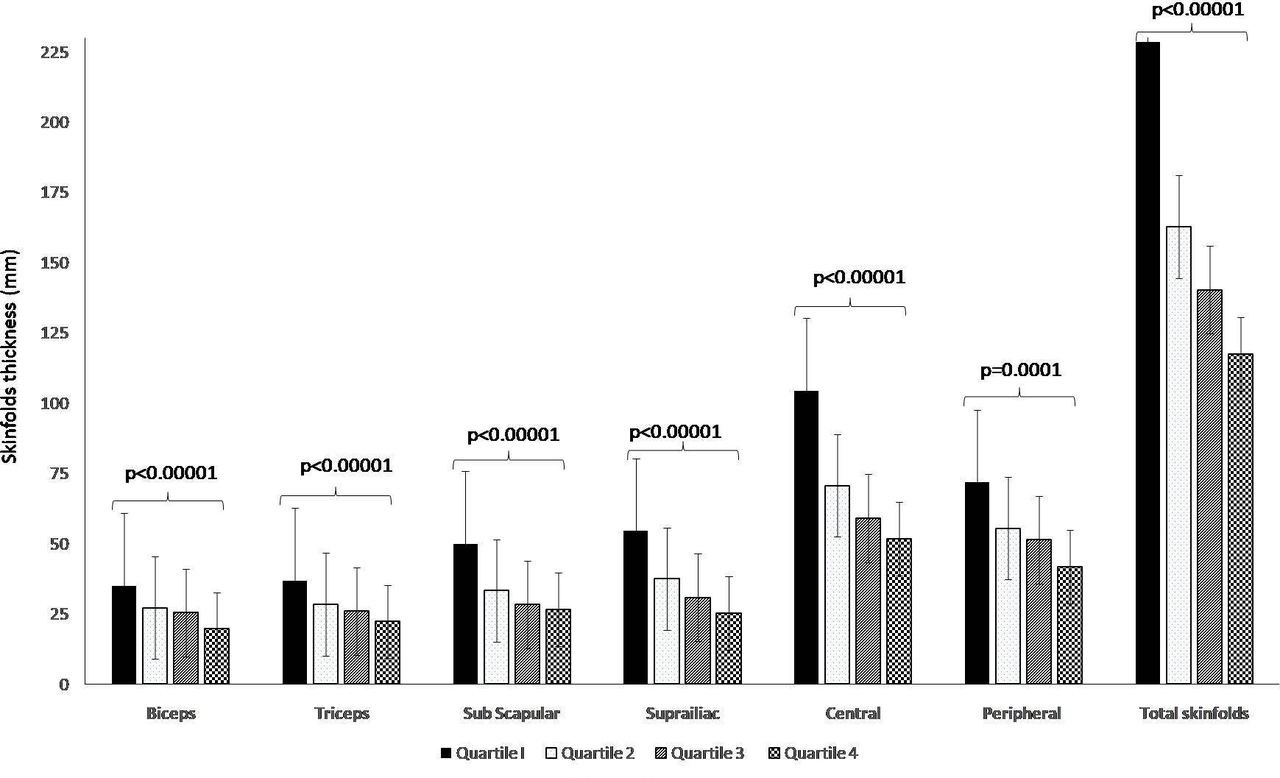
The association of measures of obesity and LTL revealed a significant negative correlation by multivariable linear regression analyses adjusted for age, family income, education, and hypertension, using the quartile 1 as reference. Multivariable linear regression analysis identified central skinfolds (R2=0.92, p<0.0001), Σ4SF (R2=0.90, p<0.0001), BMI (R2=0.93, p<0.0001), and % body fat (R2=0.91, p<0.0001) are independent predictors of LTL (figure 2, table 3).
{kind=link}
{kind=link}
Distribution of skinfolds’ thickness according to quartiles of leucocyte telomere length.
Univariate and multivariable linear regression analyses to identify independent predictors of leucocyte telomere length (LTL) according to LTL quartiles
Conclusions
This is the first study to investigate the relationship of LTL in women with abnormal fasting glycemia. Specifically, relationship of LTL with subcutaneous adiposity, particularly truncal adiposity is being reported for the first time.
The association between obesity and telomere physiology has been investigated previously. Previously, some research studies have shown significant negative relationship between adiposity measures and LTL24 25 while others did not.26 27 Associations of LTL with generalized and abdominal obesity, as well as weight changes was researched in China (n,2912 healthy Chinese women aged 40–70 years).28 Interestingly, like our study, Chinese study was done exclusively in women. This study showed that women who maintained their weight within ±5% since age 50, or reduced their weight, had a longer mean of current telomere length than women who gained weight since age 50.28 A study in white women (n, 1122 aged 18–76 years) in UK showed that the telomere of obese women were 240 bp shorter than those of lean women.29 In a meta-analysis (87 observational studies including data from 1 46 114 subjects), Gielen et al30 showed a significant inverse relationship between BMI and LTL particularly in younger population without any gender differences. These associations were predominantly for the white pooled population.30
Asian Indians have thicker subcutaneous adipose tissue than white Caucasians,31 which is an important correlate of insulin resistance.32 Only a few studies have shown relationship of multiple measures of obesity with LTL. Cui et al28 showed inverse association between LTL and weight, WC, HC, BMI, and W-htR, but not with W-HR or height in Chinese women. In non-Hispanic whites (Fels Longitudinal Study, 309 subjects aged 8–80 years, 52% women), WC, HC, total body fat, and visceral adipose tissue volume were inversely associated with telomere length at borderline significance.33 In the current study, both abdominal and truncal adiposity (as measured by skinfolds and circumferences) are related to LTL, the association of latter with LTL has not been investigated before.
Relationship between hyperglycemia and telomere has been researched more often. Human observational case–control study from a community-based white population (432 T2DM and 424 controls) has shown decreased log (e) transformed mean leucocyte telomere repeat copy number to single gene copy number was significantly associated with T2D.34 Recent study from north India (n, 1354 individuals: 682 cases of T2D and 672 healthy controls), genotyped for 12 variants from seven telomere maintenance genes showed significant association of five variants with T2D.35 Zhou et al36 recruited 556 Chinese subjects (T2D, n, 159), abnormal fasting glycemia (n, 197), and normal glucose tolerance (n, 200)) and suggested that shorter LTL was associated with higher glycated hemoglobin (HbA1c), fasting plasma glucose, postprandial glucose, and lower glucose-stimulated insulin release. Interestingly these authors showed LTL shortening existed in individuals with pre-diabetes, and LTL was shortest in diabetes. Patients with diabetes with better glycemic control (HbA1c <7 %) had longer LTL. Further, these authors also investigated relationship of LTL with diet consumed by the subjects. They reported that legumes, nuts, fish, and seaweeds were protective factors for LTL shortening, and sweetened carbonated beverage was a risk factor for LTL shortening.36 This was the only study, apart from present study, where individuals with abnormal fasting glycemia (impaired fasting glucose) were investigated in context of LTL. An intervention study of pistachio intake in individuals with abnormal fasting glycemia has been briefly stated previously. This randomized clinical trial on 49 men and women (aged between 25 and 65 years, BMI ≤35 kg/m2) with abnormal fasting glycemia showed that chronic pistachio consumption reduced oxidative damage to DNA and increased the gene expression of some telomere-associated genes.15 36
Due to practical difficulties in conducting 2-hour post oral glucose tolerance test in community setting, we have only done FBG. We acknowledge the absence of 2-hour blood glucose value as a limitation while interpreting our data, since it has been shown that LTL may be more related to impaired glucose tolerance than impaired fasting glucose as shown in 115 adult Caucasian individuals residing in Ukraine.37 However, these important observations need to be replicated in other populations, including Asian Indians.
Further, we also acknowledge that our study is also focused on women alone. It is important to note that we have been doing research in women for last several years; hence, our present study is also focused on women. Our data should not be generalized since there might be gender differences in LTL. A systematic review and meta-analyses from 36 cohorts (36 230 participants) showed that, on the average, females had longer telomeres than males. Further, there was no association of variations by other factors such as age group and cell type. Importantly, the association between gender and LTL vary by measurement methods such as the Southern blot method, but not for the real-time PCR or the Flow-FISH (fluorescent in situ hybridization) method.38 It also has been reported that longer LTL in women than men could be due to a slower rate of telomere attrition in women.39 Further, longer telomeres might be a cause of improved fitness in women, manifest in longer lifespans, and lower risk for cardiovascular disease and cancers.40 Further data are needed in Asian Indian men for assessing any differences in LTL from women.
Other limitations of the study are as follows. The study targeted of people of one ethnic origin and a single geographical region, which prevents generalization to the entire population and race. Second, since it was a cross-sectional study, hence sequential correlation could not be verified. Finally, longitudinal and intervention studies are necessary to study interplay between LTL and pre-diabetes.
Having stated that, the following are positive points about our study. First subjects with pre-diabetes have been less examined in the context of LTL. Indian studies on LTL include those on Yoga and meditation (impact of), obstructive sleep apnea, human malignancies, T2D, obesity, and hypertension, and not on pre-diabetes. Second, no investigator has specifically focused on women with pre-diabetes. Finally, association of LTL with skinfolds thickness (hence subcutaneous and truncal adiposity) in individuals with pre-diabetes has been shown in a few studies, for example: (1) in Asian children from Singapore,41 (2) in Caucasian 8-year-old children,42 and (3) in Mexican population43 and correlation with body fat in only one study in Australian rural dwelling subjects with pre-diabetes and diabetes.44
Overall, our report clearly shows that presence of obesity and truncal obesity may accelerate aging in Asian Indian women with abnormal fasting glycemia.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was sanctioned by the Institutional Ethics Committee from Fortis C-DOC, Center of Excellence for Diabetes, Metabolic Diseases and Endocrinology, Chirag Enclave, New Delhi, India (ID No: 0001/2017). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The co-operation of the subjects who took part in the study is greatly appreciated.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Collaborators Metabolic Research.
Contributors AM conceived the study and contributed to the discussion and reviewed the manuscript. SPB conducted the study, performed laboratory investigations, and wrote the manuscript. RMP and ADU analyzed and interpreted the data. AM is the guarantor for this manuscript.
Funding This research was supported from the Department of Science and Technology, Ministry of Science and Technology, Government of India (File No: SSD/WS/098/2010).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.