Article Text

Abstract
Introduction The aims of this cross-sectional study were to (1) describe habitual physical activity and adherence to WHO recommendations, and (2) investigate the association of comorbidity, obesity, stress, and health-related quality of life (HRQoL) with moderate to vigorous physical activity (MVPA) among individuals with diabetes.
Research design and methods This study included 6856 participants with diabetes from the Danish National Health Survey from 2017. The primary outcome measure was weekly MVPA. Exposures included self-reported number of conditions, body mass index (BMI), perceived stress, and HRQoL. Mean difference in MVPA across exposures was estimated by multiple linear regression analyses.
Results Forty per cent of individuals with diabetes were not adherent to WHO recommendations for physical activity. Individuals with diabetes had higher BMI, more comorbidities, higher perceived stress, and lower HRQoL. Individuals with three or more comorbidities were significantly associated with lower weekly MVPA (−0.48 hours/week, 95% CI −0.88 to −0.07) compared with individuals with no comorbidity. Furthermore, overweight or obese (class I–III) individuals engaged in significantly less weekly MVPA (obese class III vs normal weight: −1.98 hours/week, 95% CI −2.49 to −1.47). Higher perceived stress was significantly associated with lower weekly MVPA (−1.76 hours/week, 95% CI −2.18 to −1.34) versus low perceived stress. Finally, having low physical and mental HRQoL was associated with lower weekly MVPA (−0.93 hours/week, 95% CI −1.19 to −0.66 and −0.39 hours/week, 95% CI −0.71 to −0.08 respectively vs moderate or high HRQoL).
Conclusions We found that 40% of individuals with diabetes do not engage regularly in adequate physical activity. Comorbidities, higher BMI, higher perceived stress, and lower HRQoL were associated with less engagement in physical activity. This study suggests that subgroups of individuals with diabetes are at higher risk of physical inactivity.
- Physical Activity
- Comorbidity
- Obesity
- Diabetes Mellitus, Type 2
Data availability statement
Data are available upon reasonable request. All data used in the current study were derived from the DNHS. Data are available through application to the National Institute of Public Health, University of Southern Denmark.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
No previous large-scale study has provided a detailed description of habitual physical activity among individuals with diabetes and associated factors.
WHAT THIS STUDY ADDS
Forty per cent of individuals with diabetes do not engage regularly in adequate physical activity.
Having comorbidities, higher body mass index, higher perceived stress, and lower health-related quality of life is significantly associated with lower moderate to vigorous physical activity among individuals with diabetes.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Subgroups of individuals with diabetes are at higher risk of physical inactivity and might need additional support or tailored interventions to increase their physical activity level.
Introduction
Physical inactivity alone is estimated to cause 7% of the burden of type 2 diabetes.1 On the other hand, engaging in regular physical activity is a cornerstone of diabetes management to prevent long-term diabetes complications, declines in quality of life and premature mortality.2 3 According to the WHO and the American Diabetes Association,4 5 adults living with diabetes are recommended to do at least 150–300 min of moderate-intensity or 75–150 min of vigorous-intensity (or an equivalent combination) aerobic physical activity weekly.4 5 Living with diabetes can be very stressful and significantly affect the individual’s quality of life.6 7 Individuals with diabetes may worry about existing and future complications and comorbidities, as well as feeling guilty and ashamed of not adhering to lifestyle recommendations, for example, in terms of body mass index (BMI) and physical activity.8 Meeting the WHO recommendations of regular physical activity is a major challenge among individuals with diabetes,9 but some studies report that about 40%–45% of individuals with diabetes do adhere to the recommendations10 11 and their treatment should thus not necessarily revolve around increasing physical activity. Morbidity, obesity, stress, and lower health-related quality of life (HRQoL) are associated with decreased habitual physical activity in the general population.12–15 Given that individuals with diabetes are at high risk of suffering from all these factors,6 16 17 it is likely that physical activity among individuals with diabetes is also associated with these factors. Availability of such information would be an important resource when designing and promoting a physical activity intervention taking individual characteristics, needs and preferences into account, and thereby spending the resources on those in most need. However, no previous large-scale studies have provided a detailed description of habitual physical activity among individuals with diabetes and associated factors.
Therefore, the aims of this study were to (1) describe habitual physical activity and adherence to WHO recommendations, and (2) investigate the association of comorbidity, obesity, stress, and HRQoL with moderate to vigorous physical activity (MVPA) among individuals with diabetes based on data from a large nationwide Danish survey.
Research design and methods
Reporting of this cross-sectional study followed the ‘Strengthening the Reporting of Observational Studies in Epidemiology’ checklist.18
Setting and data sources
We used data from the cross-sectional nationwide Danish National Health Survey (DNHS) from 2017. The overall aim of the DNHS is to monitor the status and trends in physical and mental health in the adult Danish population (≥16 years). A detailed description of the DNHS design is available on the DNHS web page (https://www.danskernessundhed.dk/).19 20 In 2017, a total of 312 349 individuals were randomly drawn from the population using the Danish Civil Health Registration System and invited via a secure electronic mail service (Digital Post) or regular postal service to participate in the survey. The questionnaire was fully or partially completed (sex, age, and at least one other question answered) by 183 372 respondents (58.7%).20
Participants
The present study included participants with ‘Diabetes’ and ‘No known diabetes’. Following the categorization of diabetes from DNHS, respondents were defined as ‘Having diabetes’ if they had answered ‘I have diabetes now’ or ‘I have had diabetes’ and ‘I suffer from sequela due to the diabetes’. The question on diabetes did not distinguish between types of diabetes; therefore, the respondents covered the whole spectrum of diabetes. Out of 183 372 respondents, 10 216 individuals reported to have diabetes. Respondents with complete data on outcome, exposure, and confounder variables were considered eligible for the present study.
Outcome variables
The outcomes of interest were self-reported MVPA (hours/week), adherence to WHO recommendations of physical activity and sedentary behavior, and total sedentary behavior (hours/day). MVPA was assessed with the question: ‘During a regular week, how much time do you spend on moderate and vigorous physical activities, where you can feel your pulse and your breathing increase (eg, walking, cycling as transport or recreational activity, hard gardening, running or exercise sports)? Indicate only activities lasting at least 10 min’. Respondents replied in hours and minutes.
Adherence to WHO recommendations was assessed with the question regarding MVPA and the question: ‘How much time of the above-mentioned physical activities do you spend in a regular week on vigorous physical activities? These are activities where your pulse is substantially increased, you sweat, and which cause you to be out of breath and to find it hard to talk (eg, swimming, running, cycling at high speed, strength training or ball games)’. Adherence to WHO recommendations was dichotomized to ‘Following WHO recommendations’ or ‘Not following WHO recommendations’. Respondents were categorized as ‘Following WHO recommendations’ if they reported at least 150 min/week of moderate intensity, at least 75 min/week of vigorous intensity, or an equivalent combination.4
In addition, self-reported MVPA was categorized into four levels of habitual physical activity in accordance with the WHO recommendations: (1) inactive: 0 hour/week; (2) inadequate: participants do not meet recommendations (150–300 min/week of moderate intensity or 75–150 min/week of vigorous intensity); (3) adequate: participants meet recommendations, but not more than 300 min/week of moderate intensity or 150 min/week of vigorous intensity; and (4) optimal: participants with more than 300 min/week of moderate intensity or 150 min/week of vigorous intensity.
Total sedentary behavior was assessed with the question: ‘On a typical weekday/workday, how much time do you spend on sitting down in each of the following situations? Please consider your total sitting time and distribute it in each of the following categories’. Respondents reported minutes and hours spent on (1) transport (eg, in car, bus or train; not cycling); (2) work/school/education (eg, sitting by the desk or at meeting); (3) leisure time: by screen (eg, television, computer, tablet, smartphone); (4) leisure time: other (eg, meals, reading, social gatherings). All questions regarding MVPA and sedentary behavior have been validated.21 Motivation for being more physically active was assessed with the question: ‘Do you want to be more physically active?’.
Exposures
Comorbidity
Self-reported information on selected long-term conditions (excluding diabetes) and sequela were used to assess comorbidity. Respondents reported whether they had or have had selected long-term conditions, and whether they were suffering from sequelae due to the specific long-term condition. The definition of comorbidity was based on diagnoses organized in 10 groups of different body systems according to Willadsen et al.22 In this study, there were only seven groups due to lack of information on conditions in all body systems, and since diabetes was the only endocrine condition in the survey, it was excluded from the comorbidity variable. The seven groups were: (1) lung, (2) musculoskeletal, (3) mental, (4) cancer, (5) neurological, (6) cardiovascular, and (7) sensory organs.
The variable was categorized as a count variable, counting the numbers of comorbidities from zero to three or more from different body systems including diabetes. Suffering from several long-term conditions within the same body system, for example, hypertension and myocardial infarction, would still only count as one comorbidity.
Individuals with mental comorbidities engage less regularly in physical activity compared with individuals with only somatic comorbidities.23 24 Therefore, a variable differentiating between comorbidities with and without a mental health condition was created.
Obesity
Self-reported data on height and weight were used to calculate BMI (kg/m2). BMI was categorized into five groups: underweight/normal weight (BMI <25.0), overweight (BMI ≥25.0 to <30.0), obese class I (BMI ≥30.0 to <35.0), obese class II (BMI ≥35.0 to <40.0), and obese class III (BMI ≥40), as defined by the WHO.25
Stress
Self-reported psychological stress was assessed using the Danish version of Cohen’s 10-item Perceived Stress Scale (PSS).26 27 PSS was categorized into three as follows: (1) low perceived stress (scores ranging from 0 to 13), (2) moderate perceived stress (scores ranging from 14 to 26), and (3) high perceived stress (scores ranging from 27 to 40).27
Health-related quality of life
Self-reported HRQoL (physical and mental health) was assessed using the 12-item Short-Form Health Survey and was categorized into a physical and mental scale.28 29 A physical score of 50 or less was categorized as ‘Low physical HRQoL’, and a mental score of 42 or less was categorized as ‘Low mental HRQoL’.30
Covariates
The following covariates are suggested to be potential independent risk factors of the four exposures (comorbidity, obesity, stress, and HRQoL) and the outcome (physical activity): age, sex, ethnicity, marital status, educational level, alcohol consumption, smoking, and diet. Directed acyclic graphs31 of the assumed causal relations between exposures and outcome of the primary analysis are available in online supplemental file 1. Marital status was dichotomized into ‘Married or living with partner’ or ‘Living alone’. Educational level was assessed using the respondents’ highest level of education and categorized into three: (1) primary and lower secondary education, (2) upper secondary or vocational, and (3) higher education. Ethnicity was categorized into three groups: Danish, other Western, and non-Western background. Smoking was categorized into (1) smoker, (2) ex-smoker, (3) never smoked. Alcohol consumption was measured by the number of drinks of beer, wine and spirits consumed in a typical week and categorized in accordance with the national recommendations from the Danish Health Authority: (1) no alcohol (0 drink), (2) below low risk (men >0 and <14 drinks, women >0 and <7 drinks), (3) above low risk (men ≥14 and ≤21 drinks, women ≥7 and ≤14 drinks), (4) high risk (men >21 drinks, women >14 drinks). Eating habits were measured using the diet score dividing the respondents into three health levels based on their diet: (1) healthy diet, (2) medium healthy diet, and (3) unhealthy diet.32
Supplemental material
Statistical analyses
A statistical analysis plan was developed (online supplemental file 2) and openly available (https://osf.io/25u4g/) prior to commencing the analyses. Cross-tabulations were conducted to describe habitual physical activity among individuals with diabetes and individuals with no known diabetes and to display potential subgroup differences.
Supplemental material
Descriptive statistics are presented as numbers and percentages or means and SDs or medians and IQR. Four multiple linear regression analyses were conducted to investigate the associations between the exposures (comorbidity, obesity, stress, and HRQoL) and the outcome MVPA. Results of the multiple linear regression analyses are presented as mean differences with 95% CIs across levels of exposures with no comorbidity, underweight or normal weight, low perceived stress, and moderate to high HRQoL as reference categories.
To explore the associations between the same four exposures and adherence to WHO recommendations of physical activity, four multiple logistic regression analyses were performed. Results of the logistic regression analyses are presented as prevalence ORs with 95% CI. Furthermore, four multiple linear regression analyses were performed with total sedentary behavior as outcome.
All models are reported crude and adjusted for age, sex, ethnicity, marital status, educational level, alcohol consumption, smoking, and diet. Furthermore, the four exposures were potential independent risk factors in the individual model; therefore, the variables were included as confounders in the individual model (online supplemental file 1). Post hoc analyses of comorbidities and MVPA excluding adjustment of BMI were performed to investigate the size of difference in MVPA between numbers of comorbidities allowing for adiposity levels to be different across comorbidities, because obesity is a strong determinant of a wide range of morbidities. In addition, cross-tabulations were conducted describing proportions and characteristics of participants with diabetes who were not following WHO recommendations of physical activity and their motivation for being more physically active. Statistically, weights provided by the DNHS were included in all models to account for non-response by certain population groups. The weights were computed by Statistics Denmark and account for differences such as age, sex, educational level, income, socioeconomic group, municipality of residence, marital status, ethnic background, healthcare utilization and research protection.33 All statistical analyses were conducted in STATA/BE V.17.0 using an α level of 0.05, two sided.
Results
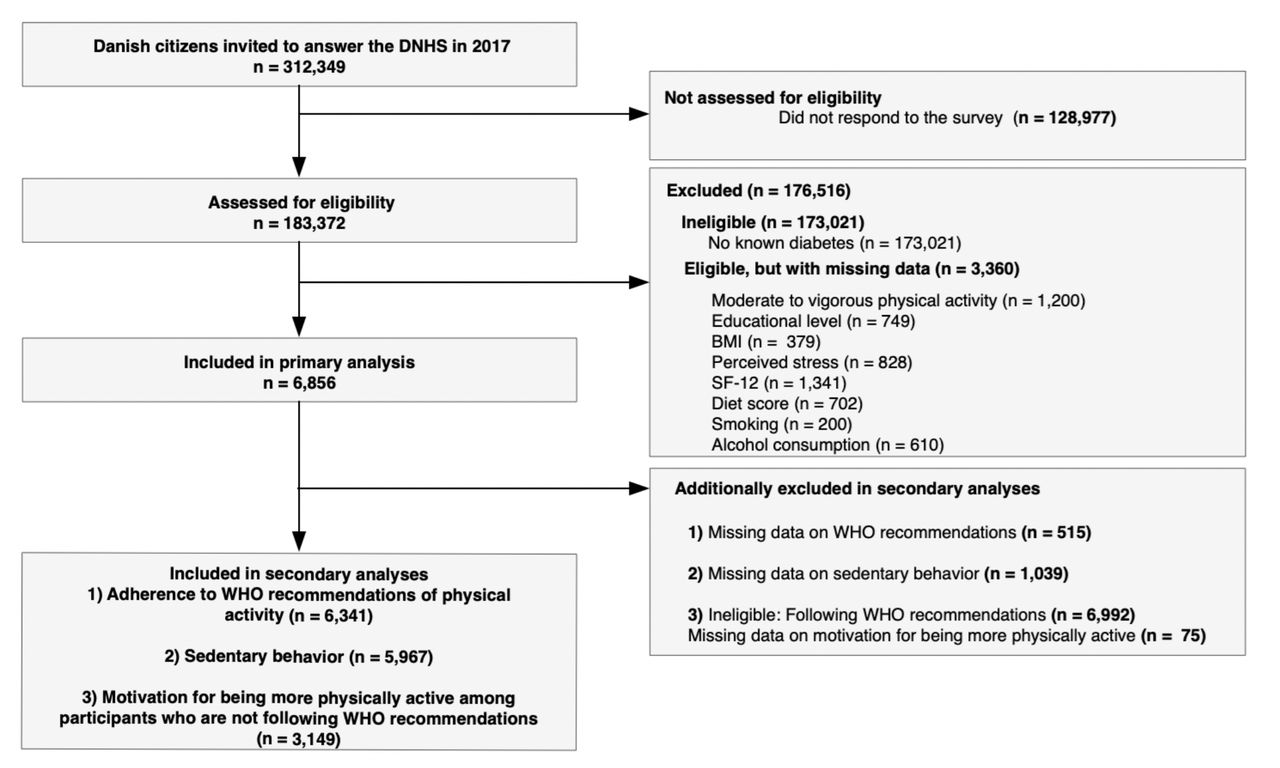
Out of 183 372 responses, 10 216 participants reported they had diabetes. Of these, 6856 participants had complete data on outcome, exposures, and covariates in the primary analysis (figure 1).
{kind=link}
Flow chart of all included participants in the primary analysis and the three secondary analyses from the Danish National Health Survey (DNHS) 2017. BMI, body mass index; SF-12, 12-item Short-Form Health Survey.
Participant characteristics
Characteristics of participants with diabetes with and without complete data and participants with no known diabetes are presented in table 1. Due to differences in age and sex between diabetes status, direct standardization was performed on participants with no known diabetes based on the age and sex distribution among participants with diabetes. Only 60% of those with diabetes met the WHO recommendations compared with 70% of those without diabetes. Participants with diabetes had higher BMI, more comorbidities, higher perceived stress, and lower HRQoL.
Characteristics of participants with diabetes with and without complete responses and no known diabetes
Participant characteristics by level of habitual physical activity
Characteristics of participants with diabetes stratified by level of habitual physical activity according to WHO Guidelines of Physical Activity and Sedentary Behavior are presented in table 2. Out of 6341 participants, 2530 (38.8%) had optimal amount of habitual physical activity and 955 (16.4%) were inactive. Inactive participants had lower levels of education and more unhealthy eating habits, higher prevalence of obesity class II and III, higher prevalence of three or more comorbidities, higher perceived stress, and lower HRQoL.
Characteristics of participants with diabetes stratified by level of habitual physical activity
Associations of MVPA and comorbidities
Table 3 represents the results from the primary analysis regarding associations between exposures and MVPA (hours/week) in participants with diabetes. Having diabetes with three or more comorbidities including mental health conditions had significantly lower weekly MVPA after adjustments (−0.48 hours/week, 95% CI −0.88 to −0.07) compared with individuals with no comorbidity, whereas three or more comorbidities excluding mental health conditions were non-significant after adjustments (−0.54 hours/week, 95% CI −0.76 to 0.04) compared with no comorbidity. Post hoc analyses showed significant lower weekly MVPA among individuals with two comorbidities and three or more comorbidities including mental health conditions without adjustment of BMI (−0.58 hours/week, 95% CI −0.98 to −0.18 and −0.85 hours/week, 95% CI −1.25 to −0.45) compared with individuals with no comorbidity. The analyses excluding mental health conditions showed also significant results without adjustment of BMI (−0.51 hours/week, 95% CI −0.89 to −0.12 and −0.72 hours/week, 95% CI −1.12 to −0.32).
Linear regressions on the associations of determinants with MVPA in participants with diabetesTherefore, the aims of this
Associations of MVPA and obesity
Overweight or obese (class I–III) individuals engaged in significantly less MVPA after adjustments (overweight: −0.61 hours/week, 95% CI −0.94 to −0.29; obese class I: −1.08 hours/week, 95% CI −1.43 to −0.74; obese class II: −1.43 hours/week, 95% CI −1.85 to −1.01; obese class III: −1.98 hours/week, 95% CI −2.49 to −1.47) compared with underweight and normal weight individuals.
Associations of MVPA and perceived stress
Moderate and high perceived stress were significantly associated with lower weekly MVPA after adjustments (−0.59 hours/week, 95% CI −0.83 to −0.34 and −1.76 hours/week, 95% CI −2.18 to −1.34) compared with low perceived stress.
Associations of MVPA and HRQoL
At last, low physical and mental HRQoL were associated with lower weekly MVPA after adjustments (−0.93 hours/week, 95% CI −1.19 to −0.66 and −0.39 hours/week, 95% CI −0.71 to −0.08) compared with moderate or high HRQoL. The pattern of association of comorbidity, obesity, and stress with MVPA appeared consistent with an inverse graded relationship.
Adherence to WHO recommendations
The estimated associations of the logistic regression models between exposures and adherence to WHO recommendations appeared similar to the linear models (online supplemental file 3).
Supplemental material
Associations of sedentary behavior and determinants
Results of sedentary behavior showed significant associations between obese class II and III and higher weekly sedentary behavior compared with normal weight individuals with diabetes (for more details see online supplemental file 4).
Supplemental material
Motivation for being more physically active
Table 4 shows the distribution and characteristics of participants with diabetes who are not following WHO recommendations of physical activity and their motivation for being more physically active. Younger participants were more motivated for being more physically active. In addition, the proportion of motivated participants was highest among obese class II and III compared with obese class I, overweight, and underweight/normal. Distribution and characteristics of participants with diabetes who are following the WHO recommendations of physical activity and their motivation for being more physically active are available in online supplemental file 5.
Supplemental material
Distribution of insufficiently physically active participants and their motivation for being more physically active
Discussion
We found that 40% of individuals with diabetes from this nationwide population were not adherent to WHO recommendations for physical activity as measured by self-report. Inactive individuals with diabetes were less educated, had more unhealthy eating and smoking habits, higher BMI, more comorbidities, higher perceived stress, and lower HRQoL. The primary analysis showed that higher BMI, higher perceived stress, lower HRQoL, and having two comorbidities and three or more comorbidities were associated with lower weekly MVPA. However, when comorbidities only included somatic conditions, the association was only significant when participants had three or more comorbidities. Obesity, high perceived stress, and low physical HRQoL were the most remarkable determinants of low physical activity with mean differences of at least 1 hour of lower weekly MVPA compared with references. Post hoc analyses showed significant lower weekly MVPA among individuals with two comorbidities and three or more comorbidities.
Among individuals with diabetes who did not meet the WHO recommendations, 60% were motivated for being more physically active, with higher motivation among young, middle-aged and obese individuals.
The prevalence of adherence to the WHO recommendations found in this study is inconsistent with two previous cross-sectional studies outside Denmark. A study by Martinez-Harvell et al11 from 2020 found that 53.5% of 25 980 participants with diabetes from the USA did not meet the recommendations of physical activity (150 min/week of MVPA, or 75 min/week of vigorous intensity at least three times/week). A Scottish study by Salman et al34 from 2019 found that 65.9% of 1259 participants did not meet the recommended levels of physical activity (150 min/week moderate or 75 min/week vigorous physical activity or equivalent combination). The inconsistency might be explained by differences in how physical activity was quantified and the populations included. Our study included a large population with diabetes from all regions of Denmark, which increases the generalizability to the whole country thereby extending previous findings. Even though our results are inconsistent with previous studies, our results still indicate that physical activity interventions targeting individuals with diabetes are needed.
We found that individuals with higher perceived stress, lower HRQoL and comorbidities including mental health conditions are less likely to engage in regular physical activity. These findings support previous studies showing an association between mental health conditions, distress, and physical activity among individuals with diabetes.35 36 Individuals suffering from mental health conditions or distress may experience challenges concerning self-care in managing the diabetes condition compared with individuals with only somatic conditions. We also found that higher BMI and lower HRQoL were associated with lower MVPA, which support the results from other studies.11 34 37 Individuals with poor HRQoL and elevated BMI may suffer from discomfort, fatigue, shame and fear of exercise as barriers to engage in regular physical activity.38–40
No other studies have described and investigated the characteristics and correlates of physical activity among individuals with diabetes who are completely inactive corresponding to 0 hour of weekly MVPA. Results showed that inactive individuals with diabetes had lower levels of education, which indicates that social inequality in engagement in physical activity is present among individuals with diabetes. Social inequality is highly associated with prevalence and complications of type 2 diabetes.41 42 This includes a 10% higher risk of developing severe diabetes-related complications, and 26% higher risk of premature mortality among individuals with lower levels of education.43 With a large sociodemographic and geographic represented population, the results of the present study highlight the nationwide challenges of social inequality among individuals with diabetes and their ability to engage in regular physical activity.
Clinical implications
Based on our results, healthcare providers may need more targeted approaches to reach those in most need of physical activity interventions to increase the reach and motivation as well as the success of the interventions. Tailored interventions that are adapted to individuals with lower levels of education, higher BMI, more comorbidities, higher perceived stressed, and lower HRQoL might be needed to help improve diabetes self-management and physical activity level among all individuals with diabetes and thereby help prevent the development of other chronic conditions, diabetes-related complications and premature mortality. It seems important to develop or adapt current diabetes management and physical interventions to increase reach and motivation on an individual level among insufficiently active individuals to increase the health of the population and prevent the development of other chronic conditions. In our study, most individuals with diabetes who were not sufficiently active were motivated to increase their physical activity level (60%), which suggests that other factors prevent them from increasing their physical activity level. Previous studies have found that mental health, lack of time and energy, working schedule, economic circumstances, and social support are reasons for not being more physically active.38 44–46 These reasons are also important to consider when designing and promoting a physical activity intervention.
Strengths and limitations
The present study is based on a relatively large nationwide sample, which strengthens the generalizability of the results. The sample of participants with self-reported diabetes was 5.6%, which is slightly higher than the prevalence of diabetes in a recently published study in Denmark that found an overall prevalence of 0.5% of type 1 diabetes and 4.4% of type 2 diabetes in 2016.47 Another strength of this study is the data on perceived stress, HRQoL and weekly MVPA, which were provided with validated questionnaires.21 26 28 Furthermore, this study applied statistically weights provided by the DNHS to account for non-response and ensure a nationally representative analysis.33
The results of this study should be interpreted with the following limitations in mind. It was not possible to distinguish between type 1 and type 2 diabetes among participants, which would have been preferable due to etiological differences. Since type 2 diabetes accounts for 85%–95% of diabetes cases in high-income countries,48 the findings of this study will primarily be applicable to this patient group. In addition, information regarding diabetes complications and duration of the diabetes disease was not available, and the sample answering could potentially be skewed. Data were collected through self-reported questionnaires, which introduces information bias, including social desirability bias regarding lifestyle questions, such as diet, alcohol, smoking, and physical activity. Individuals with certain negative health conditions and behaviors are more likely to refrain from responding to health surveys.49 Thus, the absolute prevalence of diabetes might be underestimated, and the presented characteristics might not be representative for all subgroups of individuals with diabetes, while the estimated levels of MVPA might be overestimated due to desirability bias. Despite the use of statistical weights to reduce the possible impact of non-response bias on the estimates, citizens living alone, or with non-Western background or at younger age were not highly represented in the study population affecting the generalizability of the findings.
The comorbidity variable created in this study does not include all the conditions, and not all conditions affect the individual’s ability to be physically active. Questions regarding weekly MVPA are reported to provide an acceptable but weak estimate of participants’ level of physical activity, which questions the absolute distribution of adherence to WHO recommendations of physical activity.21 In addition, results might be different if assessment of MVPA was following the WHO recommendations from 2020, where physical activity of less than 10 min bouts has been removed.4 Finally, the cross-sectional study design is a limitation, as reverse causation, uncontrolled confounding, and information bias cannot be ruled out. A prospective study design and/or objective measurement tools are suggested for further research to support the findings of this study.
Conclusion
In this nationwide survey, we found that having comorbidities, higher BMI, higher perceived stress, and lower HRQoL were significantly associated with lower MVPA. Suffering from obesity, high perceived stress, and low physical HRQoL were the most remarkable determinants of low MVPA. Furthermore, we found that 40% of individuals with diabetes do not engage regularly in adequate physical activity, and 60% of those who do not meet the WHO recommendations for physical activity are motivated for being more physically active.
Our study suggests that subgroups of individuals with diabetes are at risk of physical inactivity and might need additional support or tailored interventions to increase their physical activity level.
Data availability statement
Data are available upon reasonable request. All data used in the current study were derived from the DNHS. Data are available through application to the National Institute of Public Health, University of Southern Denmark.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Danish Data Protection Agency through the University of Southern Denmark (journal number: 11.397). Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors All authors contributed to formulation of the study question and design. PLK and AG supervised the statistical analyses, and SRM conducted the statistical analyses. All authors contributed to the interpretation of the study results. SRM wrote the first draft of the manuscript. STS reviewed and commented on all drafts of the manuscript. All authors contributed to the critical revision and final manuscript. All authors read and approved the final manuscript. SRM is the guarantor and takes responsibility for the conduct and the overall content of the article.
Funding SRM is funded by a program grant from Region Zealand (Exercise First), a research grant from Næstved-Slagelse-Ringsted Hospitals’ Research Fund (A986), a research grant from the Health Science Research Fund of Region Zealand (A1136), and a research grant from Steno Diabetes Center Sjælland. STS is currently funded by a program grant from Region Zealand (Exercise First) and two grants from the European Union’s Horizon 2020 research and innovation program: one from the European Research Council (MOBILIZE, grant agreement number: 801790) and the other from ESCAPE (grant agreement number: 945377). AG is funded by the European Research Council (SCREENS, grant agreement number: 716657), the Novo Nordisk Foundation (grant number: NNF20SH0062965), and TrygFonden (grant numbers: 130081 and 115606). MR-L is funded by TrygFonden. The Danish National Health Survey was funded by the Capital Region, Region Zealand, the South Denmark Region, the Central Denmark Region, the North Denmark Region, Ministry of Health and the National Institute of Public Health, University of Southern Denmark.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.