Article Text

Abstract
Introduction Recurrent hypoglycemia due to postbariatric hypoglycemia (PBH) is a postoperative complication after Roux-en-Y gastric bypass (RYGBP). The historic term is late dumping syndrome or reactive hypoglycemia. The aim of this study was to assess clinically applicable tools, in order to diagnose these patients, for the purpose of preventing hypoglycemic complications.
Research design and methods Ten patients with PBS and nine controls were recruited. Continuous glucose monitoring (CGM) and food intake were registered for 7 days, together with metabolic parameters at baseline.
Results There was a significant difference (p<0.05) in Dumping Syndrome Rating Scale (DSRS) between the groups. There was no difference between p-glucose or HbA1c between the groups, but a highly significant difference in C peptide p<0.01 was observed. Using the Dexcom Studio system, the PBH group had significantly (p<0.05) more time during the day in very low blood sugar (5.9±4.2% vs 1.8%±2.3%) compared with the controls. Counting hyperglycemic and hypoglycemic episodes showed that the quantity of hypoglycemic episodes was significantly higher, p<0.01, in the PBH group compared with controls (16.6±11.0 vs 8.1±8.6 hypoglycemic events). C peptide was positively correlated with the late dumping group, p<0.01 (CI 95% 0.353 to 0.814) and very low blood sugar (<3.2 mmol/L) in all subjects with p<0.01 (CI 95% 0.194 to 0.763).
Conclusions Finding patients with recurrent hypoglycemic episodes after bariatric surgery is important to prevent future health problems. To diagnose recurrent hypoglycemia (PBH) after RYGBP, we used blood sugar analyzing tools that are commonly available in clinical settings. Interestingly, patients with few or no symptoms of PHB still had recurrent hyperglycemic and hypoglycemic events. We recommend an active approach with dumping syndrome questionnaires, assessment of metabolic parameters and CGM with food registration. Assessment of PBH using this method can potentially lead to reduced blood glucose variability due to behavioral changes.
- Obesity
- Reactive Hypoglycemia
- Hypoglycemia
- Bariatric Surgery
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Recurrent hypoglycemia is a postoperative complication after bariatric surgery, also called postbariatric hypoglycemia (PBH).
Many hypoglycemic events are asymptomatic in this group of patients due to hypoglycemic unawareness.
Recurrent hypoglycemic episodes, especially in patients unaware of hypoglycemia, result in negative health consequences.
Early diagnosis and treatment of PBH is important.
WHAT THIS STUDY ADDS
We recommend an active approach with dumping syndrome questionnaires which are helpful to suspect PBH.
We used blood sugar analyzing tools that are commonly available in clinical settings.
Increased C peptide after a standardized breakfast was a good indicator of recurrent hypoglycemia.
A continuous glucose monitoring (CGM) for 7 days combined with a food diary can facilitate patients to change their eating behavior in order to decrease glucose variability and, consequently, the risk of hypoglycemic events.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
We propose simple and clinically applicable methods to diagnose PBH, which may decrease ongoing hypoglycemic events and prevent future hypoglycemic complications.
Introduction
A common surgical treatment for patients living with obesity worldwide is Roux-en-Y gastric bypass (RYGBP).1 2 This method is successful in treating patients with obesity to induce long-term weight loss and also in treating or controlling obesity-related comorbidities. It is often referred to as metabolic surgery due to the postoperative metabolic benefits.1–3 However, RYGBP also causes complications and risks, such as late dumping syndrome (LDS),4 5 also referred to as postbariatric hypoglycemia (PBH).6 The term postbariatric hypoglycemia describes this disease entity better than the historical term late dumping syndrome, or reactive hypoglycemia, which has commonly been used previously. It must be noted that other types of upper gastrointestinal surgery involving altered nutrient delivery, such as gastric banding, gastrectomy and esophageal resection, also can induce this symptomatology along with hypoglycemia, but these patients are less well characterized and the prevalence seems much lower.7
PBH is characterized by hyperglycemia followed by hyperinsulinemia and hypoglycemia, 1–3 hours after meal intake.8 9 The symptoms, usually linked to a high intake of carbohydrates, are often non-specific, such as dizziness, fatigue, and palpitations but can be due to severe hypoglycemia which may also cause syncope and seizures.8 10 Some patients also experience abdominal pain.11 Hypoglycemia after bariatric surgery is usually described as an uncommon problem,12 13 but considering the unspecific symptoms, these estimations seem doubtful. Marsk et al14 used the Swedish National Patient Registry and found an absolute risk of 0.2% to require hospital care due to postprandial hypoglycemia after RYGBP compared with 0.04% in the general population. Furthermore, it has been shown that most hypoglycemic events are asymptomatic in this group of patients,5 15–17 thus supporting the apprehension that PBH is a much more frequent complication than previously described. Abrahamsson et al5 examined 15 patients, randomly selected after RYGBP with CGM (continuous glucose meter). They found that hypoglycemia (<3.3 mmol/L) occurred during 2.9% of the day (42 min/24 hours). Most hypoglycemic episodes (around 80%) were asymptomatic. A control group with obesity had no hypoglycemic episodes at all. These findings suggest that a considerable number of patients with recurrent hypoglycemia are underdiagnosed. In patients living with diabetes, recurrent hypoglycemic episodes, especially in patients unaware of hypoglycemia, increased risk of dementia, cardiovascular disease and poor quality of life18–22 are consequential. Hypoglycemia is defined by the American Diabetes Association as all episodes of an abnormally low plasma glucose concentration that exposes an individual to potential harm.23 A newer definition of clinically significant hypoglycemia is a blood glucose level ≤3.0 mmol/L.24 With regard to the issue of harm, it is not only the nadir glucose concentration that is dangerous but also the frequency and the duration of hypoglycemic events. Frequent hypoglycemic events interfere with daily living and lead to defective glucose counter-regulation and hypoglycemia unawareness. Since patients with PBH seem to have both recurrent hypoglycemia and hypoglycemic unwareness, early diagnosis and treatment are important.
The pathophysiology of PBH is not fully understood. RYGBP is performed on subjects living with obesity in order to induce weight loss. The standardized length of the Roux limb connected to a small bastric pouch in our institution is 100cm, and the bileopancreatic limb is 70cm.1 2 Therefore, a considerable amount of undigested food reaches the small intestine too fast. Postprandial hyperglycemia is believed to trigger excessive secretion of glucagon-like peptide-1 (GLP-1) and gastric inhibitory polypeptide,25 which in turn increases the insulin secretion, leading to hypoglycemia.26 27 Dietary modification, for example, by carbohydrate restriction, and especially decreased sugar, is recognized as the initial treatment of PBH.10 28–31 Eating with a regular meal pattern with 6–8 meals per day is also considered as favorable to keep the blood sugar level stable.31 Other suggested therapeutic options are different pharmacological treatments (such as acarbose, GLP-1 analogs and somatostatine) as well as some surgical procedures,10 but all of them have limited efficacy toward the number of hypoglycemic events.
It is important that the patients comply with the dietary recommendations to avoid health issues related to PBH and also to prevent nutritional deficiencies. However, the compliance to the dietary recommendations is inadequate after RYGBP.32–34 The definition of PBH and the tools to actually diagnose this condition are poor.7 13 35 36 Symptoms of recurrent hypoglycemia together with validated questionnaires and measured recurrent blood sugar levels below 3.9 mmol/L have been suggested as diagnostic tools in a recently published consensus on dumping syndrome.37 Continuous glucose monitoring (CGM) assessment has proven useful as diagnostic tool for hypoglycemia38 and for PBH in previous studies.5 38 39 In those studies, complicated and sophisticated calculation tools were used to define the glycemic variability, tools that usually are unavailable in a clinical setting.
Since many patients are unaware of hypoglycemia, our hypothesis is that recurrent hyperglycemia followed by hypoglycemia is present also among patients without awareness of postbariatric hypoglycemic symptoms. Therefore, in this study we compared patients with severe symptoms of PBH with those showing none or mild symptoms using CGM. All subjects kept a food diary during the study and commonly used metabolic parameters were measured. The aim of this study was to assess differences between these two postbariatric groups using clinically available tools to find patients with PBH, which could also prevent future hypoglycemic complications.
Research design and methods
Patients
The patients were consecutively recruited, and data collection was conducted between December 2015 and February 2017 (closing date for inclusion) at the Obesity Center at Capio St Goran’s Hospital in Stockholm, Sweden. All patients underwent a RYGBP with standard procedure in terms of technique.1 2 The inclusion criteria were 12–24 months post-RYGBP, weight stability, as well as absence of diabetes and other blood sugar affecting conditions (such as impaired glucose tolerance) or medications. All patients at this center undergo a dietary counseling program after bariatric surgery and also attend follow-up visits on a regular basis until 10 years after surgery. The patients’ dietary recommendations were to be consistent with the reference values from the Nordic Nutrition Recommendations 2012.40
All patients in the study were recruited during their follow-up visits after RYGBP at our bariatric center. They were asked specific questions addressing hypoglycemic symptoms during their postoperative visits, which indicated if LDS could be suspected or not, using questions based on Sigstad’s scoring system.41 The questions asked were about recurrent fatigue, desire to lie down or sit down, dizziness, sweating, palpitation, weakness, pre-syncope/syncope and other questions that could indicate rapidly occurring hypoglycemia.35 41 In accordance with Sigstad’s scoring system, a diagnostic threshold of at least seven points indicated a suspicion of dumping syndrome, but a clinical decision was applied if a patient had suspected PBH or not.
The Dumping Syndrome Rating Scale (DSRS) was then used to reinforce the clinical suspicion of late dumping after RYGBP.36 According to Laurenius et al, the scale should be used to arouse suspicion of dumping syndrome. Lower scores indicate early dumping syndrome and higher scores might indicate more severe symptoms of dumping syndrome, and also a possibility of existing recurrent hypoglycemic events. Although this score quantifies symptoms, its discriminatory value for early versus postbariatric hypoglycemia has not been fully assessed.37
Furthermore, no cut-off was defined regarding high or low scores. Nineteen patients participated and all completed the study. Ten patients had PBH and nine were controls. Patients’ characteristics are presented in table 1. All patients with suspected PBH received special and specific dietary counseling within 6 months prior to the study with the advice to reduce their carbohydrate (and especially the sugar) intake according to the guidelines.37 They were advised to have a maximum of 30 g of carbohydrates per meal, with preferably low glycemic index. A snack should contain no more than 15 g, and carbohydrates with high glycemic index should be avoided. These patients were also instructed to include healthy fats in their meals (15 g per meal and 5 g per snack), as well as to avoid liquids with their meals. A more regular meal pattern with 6–8 meals per day is also considered as favorable to keep the blood sugar level stable.31
Patients’ characteristics with respect to postbariatric hypoglycemia and controls
Biochemical measurements
The patients came to the center after overnight fasting and had a standard breakfast at the center. The subjects ingested bread, butter and cheese containing 75 g carbohydrates, 8 g fat and 12 g proteins, thus mirroring the carbohydrate amount in an OGTT (oral glucose tolerance test).37 42 No glycemic index was available for the bread, but it was a wholemeal bread. The subjects were instructed to eat in the same manner as they usually do. Before eating breakfast, weight and length were obtained (table 1). Blood samples were collected 15 min after breakfast to analyze glucose, HbA1c, GLP-1, insulin and C peptide. C peptide is secreted by the islet β cells and has a common precursor proinsulin with insulin. It is widely used to detect β cell function since the degradation rate is much slower than that of insulin.43
The samples for the GLP-1 analysis were frozen at −70°C and then analyzed at Uppsala University Hospital (ELISA; Mercodia). The other blood samples were analyzed at the local laboratory of Capio St Goran’s Hospital, which is certified by the Swedish government authority (Swedac).
Continuous glucose meter
All subjects wore a blinded continuous blood glucose monitor (CGM) Dexcom G4 for 7 days. The CGM was blinded to avoid food intake bias. The CGM device was inserted by the study nurse, according to the instructions from the manufacturer, after the biochemical assessment was finished. The subjects calibrated the CGM device two times per day by capillary glucose samples (Freestyle, Precision Neo, Abbott). The patients were instructed to live as normally as possible during the study.
Blood glucose range of ≥3.9 to <8.9 mmol/L was considered as normal.3 23 44 To date, no definitive guidance regarding cut-off values for plasma glucose has been established, but some clinicians consider plasma glucose concentrations <2.8 mmol/L to be indicative of PBH, whereas others regard levels <3.3 mmol/L diagnostic of hypoglycemia.10 Analyses of the CGM results were made using the Dexcom Studio SW10214: 12.0.5.15 Dexcom, which also had predefined cut-off values of blood glucose levels. This system is available in most diabetes units, commonly used for analyzing CGM curves in patients with diabetes. Analyzing instruments used in other studies of PBH are not commonly available and not in clinical use.5 39
Hypoglycemia was defined as blood glucose ≤3.8 mmol/L and very low blood sugar level (severe hypoglycemia) as blood glucose of 2.2–3.1 mmol/L. The CGM could not measure a blood sugar level below 2.2 mmol/L. Hyperglycemia was defined as blood glucose ≥9.0 mmol/L.
Food diary
During the CGM measurement, all patients were instructed to eat normally and record a detailed food diary. The amounts of food and drink intake were estimated, measured or weighed. The data from the food diaries were recorded in Dietist Net (V.1.0, food database of the National Food Agency of Sweden version 2016-02-17). At least 15 min between meals was required to count them as separate meals, and one meal was at least 100 kcal. Sugar was defined as the sum of monosaccharides and disaccharides.45
Detailed data from the food diaries have previously been reported.34 All patients with PBH also had very specific dietary recommendations 6 months before the study, as described above.
Statistics
SPSS (V.25) was used for all statistical analyses. In spite of the relatively small study population, data were normally distributed. Therefore, independent t-test was used in comparing the means of the groups. Due to the small sample size, data were also recalculated using Mann-Whitney U non-parametric test without different results. The statistical tests were two-sided, and p≤0.05 was considered as statistically significant. Correlation tests were also performed using Pearson’s bivariate two-tailed test.
Results
Patient’s characteristics
After signing an informed consent, 20 patients participated in this 7-day-long clinical observational study. One of the patients was excluded due to elevated HbA1c and CGM curves indicating type 2 diabetes had reoccurred (figure 1). Two patients had type 2 diabetes in remission, which was defined by HbA1c level <48 mmol/mol for at least 1 year without any active glucose-lowering pharmacotherapy.46 Ten patients were selected to the PBH group and nine as controls.

Female patient (born on 1968) who was diagnosed with postbariatric hypoglycemia and developed type 2 diabetes. (A) Representative continuous glucose monitoring (CGM) curves from 2015. HbA1c level was 41 mmol/mol and the patient was diagnosed with postbariatric hypoglycemia. (B) Representative CGM curves from 2017. HbA1c level was 56 mmol/mol and the patient was diagnosed with type 2 diabetes.
Baseline characteristics are presented in table 1. Only one male was included in the PBH group and two in the control group. The gender distribution in the study population reflects the gender distribution of patients undergoing bariatric surgery where approximately 70%–80% are female.1 2 Both groups were examined for an average of 18 months (range 14–20 months) after their gastric bypass surgery. There was a significant difference in the body mass index (BMI) between the groups; the PBH group had an average BMI of 29.5 (±3.4) and the control group 26.4 (±2.4) kg/m2. In the PBH group, two patients had type 2 diabetes preoperatively, but went into remission postoperatively (HbA1c levels 36 and 34 and fasting glucose at 4.5 and 5.1, respectively). There was a significant difference regarding psychiatric comorbidity. Four patients in the PBH group had ongoing psychiatric diagnoses with medical treatment, but none in the control group. Two had depression, one had attention deficit hyperactivity disorder (ADHD) and one had both depression and ADHD. The psychiatric psychopathology was diagnosed and treatment was initiated by different psychiatric clinics prior to entering the obesity treatment program at our center. Medication used by some of the subjects with psychiatric diagnoses was considered stable before their obesity treatment started, and thus not affecting weight or glucose variability.
Regarding the outcomes of DSRS, a significant difference between the groups was found as expected. The PBH group had significantly higher total scores than the control group (an average of 59.2±18.5 vs 34.4±12.6).
Metabolic parameters
There was no significant difference in mean fasting blood sugar levels between the groups, which was 8.1+2.9 mmol/L in the PHB group and 9.1+2.4 in the control group (table 2). No significant difference in insulin secretion was detected, but the spread was large. Likewise, no significant difference was found in HbA1c levels between the groups. However, a significant difference in C peptide (p<0.01) and GLP-1 (p<0.05) between the groups was observed.
Metabolic parameters measured at baseline, 15 min after a standardized meal with approximately 75 g carbohydrates before the start of the CGM
Since C peptide was the best metabolic parameter to suspect patients living with PBH, correlation analyses were also performed. These showed that C peptide is positively correlated with the PBH group regarding high DSRS scores, p<0.01 (CI 95% 0.353 to 0.814). There was also a positive correlation between C peptide with low blood sugar at night (<3.9 mmol/L), p<0.05 (CI 95% 0.194 to 0.763), as well as with counting hypoglycemic events, p<0.05 (CI 95% 0.05 to 0.847) in all subjects. Furthermore, there was also a strong significance between C peptide and very low blood sugar during the 24-hour analysis (<3.2 mmol/L) in all subjects with p<0.001 (CI 95% 0.194 to 0.763).
Food diaries
There was no significant difference in mean daily energy intake between the groups (table 1), and both groups showed a higher frequency of meals (seven to nine meals) per day than the recommended minimum number of meals, that is, six meals per day.
The PBH showed a larger energy percent (E%) from added sugars (14.6%) than the control group (11.4%), but the difference was not statistically significant (p=0.327). Using dietary recommendation according to the Nordic Nutrition Recommendations, both groups exceeded the maximum energy percent from sugars, which is 10%.40 Data from our food registration have been presented in detail in a previous publication.34
Glucose homeostasis measured by CGM
Daytime versus night-time analysis
To assess the variability in blood sugar, we defined different blood sugar intervals and percentage of time in each interval using the preset options of the analyzing program, the Dexcom Studio system (table 3). The measurements were divided into daytime measurements (at 06–22) and night-time (at 22–06). Normal blood sugar was defined as 3.9–8.9 mmol/L, high as ≥9 mmol/L and low as ≤3.8 mmol/L. During the day, the PBH group had significantly (p<0.05) higher blood sugar (9.7%±9.3% vs 2.6%±3.0%) than the control group. At night, patients with PBH also had significantly (p<0.05) shorter time with normal blood sugar (66.9%±9.2% vs 80.7%±16.0%) compared with controls. So, the PBH group spent approximately 68 min more time with high blood sugar during the day, and 66 min less with normal blood sugar levels during the night, compared with controls.
CGM analysis using automatic Dexcom Studio
24-hour total analysis
The analyses of blood sugar categories during 24 hours were divided into more subcategories by the Dexcom Studio system. Normal blood sugar remained 3.9–8.9 mmol/L but was differentiated into normally high blood sugar (5.6–8.9 mmol/L) and normally low blood sugar (3.9–5.5 mmol/L). High blood sugar was defined as 9–22.3 mmol/L. Low blood sugar was split up into low (3.2–3.8 mmol/L) and very low (2.2–3.1 mmol/L). The limitation regarding the measurement using the Dexcom G4 was 2.2–22.3 mmol/L. There were no significant differences in normal high, high or low blood sugar between the groups. However, the PBH group spent significantly (p<0.05) more time during the day in normal low blood sugar (47.0%±9.9% vs 57.6%±9.8%) and very low blood sugar (5.9%±4.2% vs 1.8%±2.3%) compared with the controls. Thus, the PBH group spent approximately 59 min more time with blood sugar below 3.2 mmol/L during 24 hours than controls.
Manual counting of hyperglycemic and hypoglycemic events
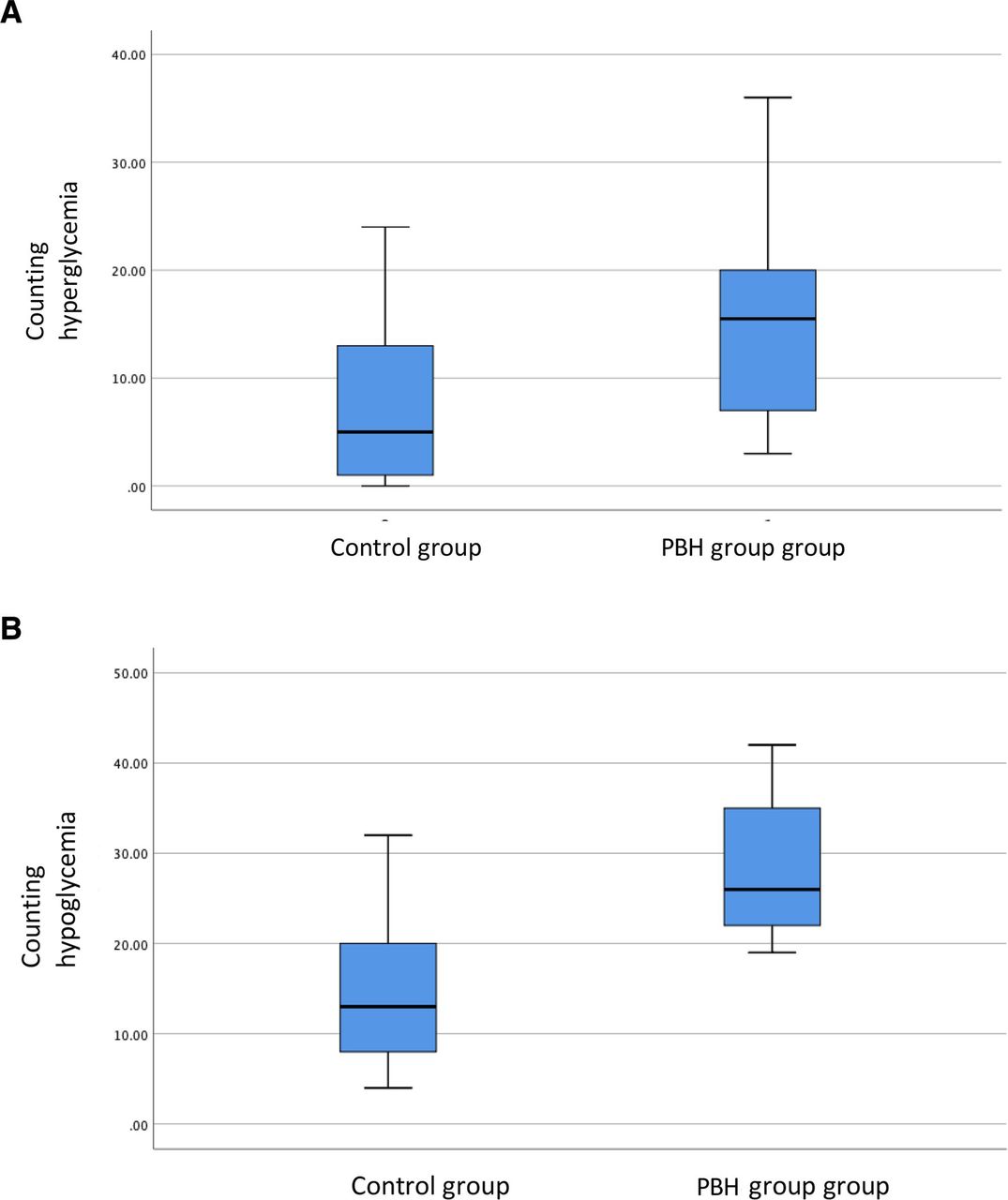
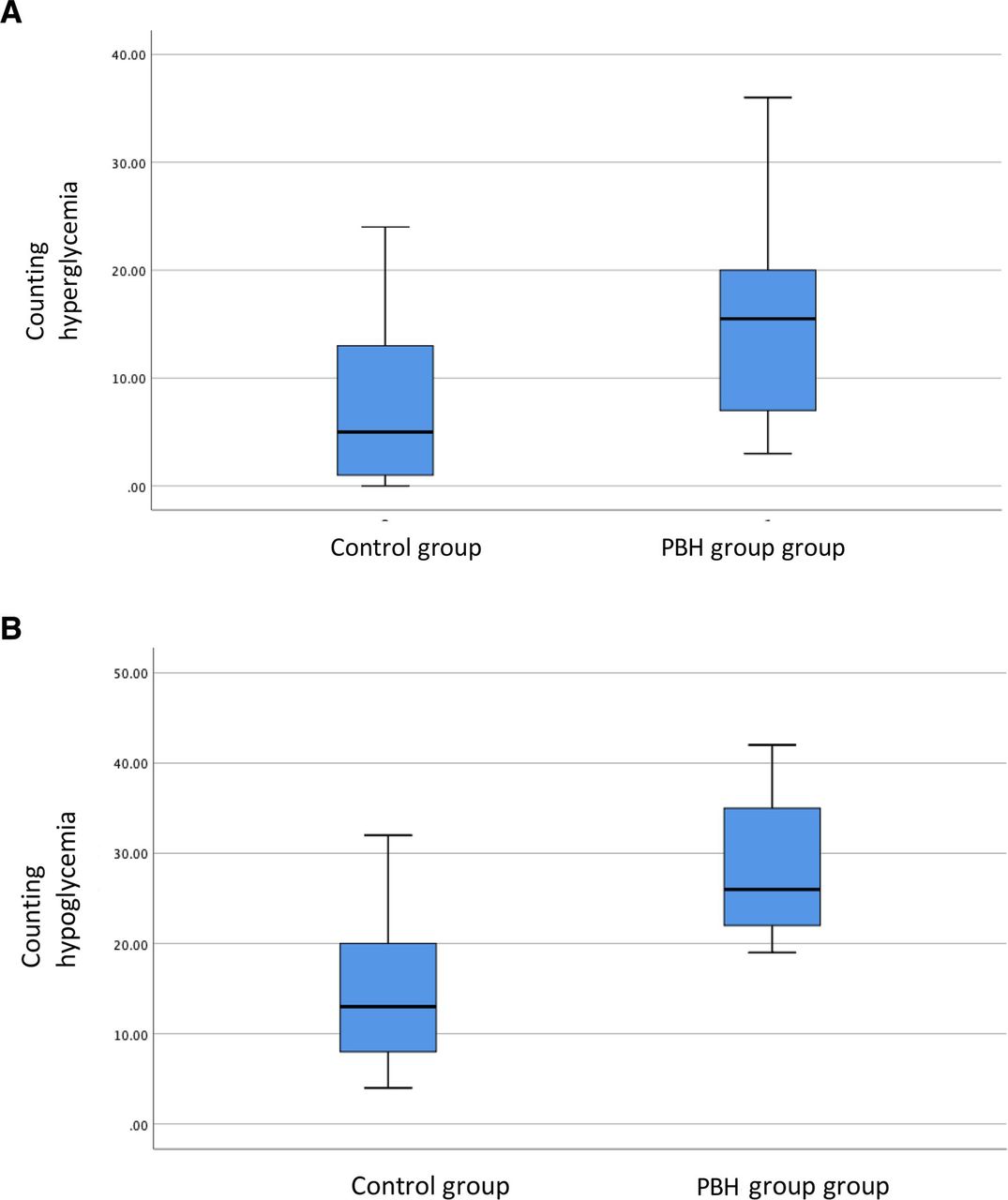
The variability of blood sugar was analyzed by a manual count of events when the blood sugar exceeded 8.9 or was below 3.9 mmol/L (table 3). When a blood sugar level was above or below the cut-off limits for longer time (persistent hyperglycemia or hypoglycemia), it was still counted as one event. The number of hyperglycemic events was higher but did not reach statistical significance (p=0.073) in the PBH group compared with controls (28.7±8.8 vs 14.5±9.0) (figure 2). By contrast, the number of hypoglycemic events was significantly more, p<0.01, comparing the PHB group to controls (16.6±11.0 vs 8.1±8.6 hypoglycemic events).
{kind=link}
{kind=link}
Counting frequencies of hypoglycemia (glucose <3.9 mmol/L) and hyperglycemia (glucose >8.9 mmol/L). Means, first and third quartiles, minimum and maximum values are shown. The number of hyperglycemic events was borderline significantly (p=0.073) higher in the postbariatric hypoglycemia (PBH) group compared with controls (28.7±8.8 vs 14.5±9.0) (A). By contrast, the number of hypoglycemic events was more common, p<0.01, comparing the PBH group to controls (16.6±11.0 vs 8.1±8.6 hypoglycemic events) (B).
Discussion
The major purpose of this study was assessing clinically applicable diagnostic and therapeutic tools for PBH after RYGBP. We showed that patients with symptomatic PBH had an increased number of hypoglycemic events compared with controls without PHB, which was expected. However, in this study, we used blood sugar analyzing tools that are commonly available in a clinical setting and not only at research units. Interestingly, patients with few or no symptoms of PBH still had recurrent hyperglycemic and hypoglycemic events on a daily basis, which is uncommon among people who have not undergone RYGBP. The hypoglycemic events in this study were, in addition, also correlated to an increased level of C peptide which, consequently, is suggested as a diagnostic tool.
Recurrent rapid change of blood sugar levels with hyperglycemic and hypoglycemic events is a well-known problem after RYGBP surgery and usually occurs within 2 years after surgery. The exaggerated hormonal response to hyperglycemia that occurs when food, and especially carbohydrates, are rapidly absorbed in the small intestine has been presented as a feasible cause of the consequential hypoglycemia.9 10 37 Most likely, the hormonal response (mainly by insulin and incretines) is overcompensated over time resulting in PBH. In gastric sleeve surgery, the pylorus part of the ventricle is retained, so the food is not distributed to the small intestine as fast as after RYGBP surgery. Although hypoglycemia may occur even after gastric sleeve surgery, it is not as common.12 Many patients are not aware that the symptoms they experience, for example craving for sugar, are actually hypoglycemic events.35 We asked our patients questions based on Sigstad’s scoring system and also used a validated questionnaire, DSRS, to confirm the clinical findings36 of dumping syndrome. These questionnaires are not validated for finding patients with recurrent hypoglycemia, so-called LDS or PBH. Our hypothesis that higher scores could also indicate PBH was then validated by CGM assessments as well as metabolic parameters. According to recently published guidelines,37 dumping syndrome questionnaires can be used in finding patients with dumping syndrome. We compared the PBH group with an asymptomatic control group regarding dietary assessment, continuous blood sugar measurement and metabolic parameters.
We published data on dietary intake in a previous article.34 Interestingly, both groups followed current guidelines regarding the number of meals per day (5–6) and energy distribution. However, intake of fast carbohydrates was higher in both groups. According to Nordic nutritional recommendations, 10% of food intake should be from monosaccharides and disaccharides (sugar). The intake was 14.5% in the PBH group and 11.4% in the control group. Fiber intake was also lower in both groups compared with the recommended. Both groups underwent dietary counseling, but as already mentioned, the PBH group were recommended to also reduce their carbohydrate intake more than controls.
Food choices, amount of food and a regularity in meal patterns are challenges for many people with obesity. Patients living with psychiatric illness often present a greater challenge to comply with dietary advice, especially having ADHD and depression that four of our patients had. Emotional eating, impulsivity and increase intake of sugary food choices are some examples which are relevant since dietary measures are important in treating PBH after bariatric surgery.1 In our study, 40% of the subjects in the late dumping group also had psychiatric comorbidity, unlike the controls where no one had psychiatric illness.
C peptide was the best metabolic parameter to suspect recurrent hypoglycemic events after the test meal, unlike HbA1c, insulin, and glucose in this study. Thus, HbA1c can be an important marker to distinguish type 2 diabetes from PBH, which otherwise can be a clinical challenge (figure 2). Although many patients with type 2 diabetes achieve remission after bariatric surgery, they also have an increased risk of PBH postoperatively.39 47 Glucose variability also seems to be exaggerated after gastric bypass surgery.39
GLP-1 was also significantly elevated in the PBH group compared with the controls, but generally, GLP-1 is only analyzed in research units, not in ordinary clinical settings. Therefore, C peptide, which is a common metabolic parameter, could be of clinical help in detecting and diagnosing PBH.
All units with access to CGM, usually diabetes units, also have access to the analysis software that is automatically used to analyze CGM curves in diabetes. We used Dexcom Studio, which is a common analyzing program for diabetes, to evaluate the CGM curves in this study. Patients with PBH had higher blood sugar during the day (p>0.05) and that the time within normal blood sugar range at night was shorter in the PBH group (p<0.05) compared with the controls. Percentage of time remaining within a certain blood sugar range showed that the PBH group had significantly more time with very low (2.2–3.1 mmol/L) blood sugar compared with the controls (p<0.01). They were approximately spending 59 min more than controls with blood sugar levels below 3.1 mmol/L during 24 hours. These hypoglycemic events were not perceived by patients, which is consistent with a previous study.5 Patients with recurrent hypoglycemia after bariatric surgery often lack awareness and do not understand that different unspecific symptoms originate from recurrent hypoglycemia.5 37 We know from previous studies on patients with diabetes that recurrent hypoglycemia can cause increased all-cause mortality, dementia, traffic accidents and also quality of life impairment.18 19 21 48–50 Unawareness of hypoglycemia is also feared among patients with diabetes due to the increased risk of neuroglycopenic symptoms, syncope and, in the long run, also increased risk of cardiovascular disease.20 22 48 In contrast, healthy patients without diabetes show a very low amount of hypoglycemic events.51 Long-term effects of these recurrent hypoglycemic events among patients after bariatric surgery are however not investigated, and due to the unawareness of hypoglycemia as well as indistinct symptoms, recurrent hypoglycemia and postbariatric hypoglycemia may be not considered and treated.
The CGM curves often show recurrent rapid oscillations after food ingestion in PHB with a rapid rise above 8.9 mmol/L, and then consequently a rapid blood sugar drop below 3.9 mmol/L. We therefore analyzed the curves manually and defined a hyperglycemic episode as a rapid blood sugar increase above 8.9 mmol/L and a hypoglycemic episode as a blood sugar drop below 3.9 mmol/L. Irrespectively of the duration, the hyperglycemia or hypoglycemia was counted only as one. With this method, the PBH group showed highly significantly more hypoglycemic events (p<0.01) but no significant difference was seen in hyperglycemic events (p=0.07) compared with controls. This method has not been validated, but can be helpful in suspecting the PBH diagnosis. The percentage of the day with very low blood sugar (≤3.1 mmol/L) and also the manually counted hypoglycemic events were correlated to increased C peptide (p<0.01). However, no correlation was found with hyperglycemia, thus suggesting C peptide primarily to be a clinical tool to assess recurrent hypoglycemia.
The strengths of the study were that the patient selection was based on postbariatric follow-up visits at a bariatric center, with a representative patient population, and with a long clinical experience of late complications after bariatric surgery. Patients were questioned with an unbiased approach, and the clinical suspicion of the presence of PBH or not was verified using a validated questionnaire. Our assessment included 7 days of CGM together with dietary registration so the patient would acquire a better understanding of the food’s impact on blood sugar levels.
A weakness of this study was a potential selection bias of the study population due to uncertainties of how reliable the validated questionnaire was in finding a control group. No cut-off limits of scores were available, so the definition of PBH and non-PBH was a combination of a clinical suspicion confirmed by the scoring of this validated questionnaire. On the other hand, this approach mirrors a clinical reality and we could show a highly significant difference in questionnaire scores between the PBH group and control group, thus confirming the group division. Furthermore, it has been previously shown that many patients after gastric bypass surgery have no or poor awareness of their recurrent hypoglycemic events.15 37 Many patients mainly experience fatigue, sweating, depressed mood and weight gain as the only symptoms of PBH. So, bringing these symptoms upfront can be helpful for them in understanding the origin of the symptomatology.
Another weakness of this study was the under-reporting of the energy intake in the food diaries in both groups, as well as the inaccuracy and variability in self-reported food diaries when food intake is estimated. Under-reporting of energy intake has been shown previously using self-assessed data from food diaries after bariatric surgery.52 In our study, the under-reporting was similar in both groups, which still makes intergroup analysis possible.
Further weakness in the study is using the analytical method of CGM curves, Dexcom Studio. This program was developed to analyze CGM curves in patients living with diabetes. It has not, to our knowledge, been used previously in analyzing blood sugar levels in patients living with PBH. However, this analysis approach is commonly used and validated in patients with diabetes. Counting the number of hyperglycemic and hypoglycemic events for 7 days to assess blood sugar oscillations has not been used before which can also be seen as a weakness. There was a clear correlation between C peptide and the number of counted hypoglycemic events nevertheless. The correlation between C peptide and very low blood sugar (below 3.2 mmol/L) in our study also reinforces the value of C peptide as a diagnostic tool for PBH in clinical everyday life. However, most patients after gastric bypass surgery seem to have blood sugar fluctuations in contrast to healthy obese subjects.39 47 Our study included only a small number of patients, which per se is also a limit, and makes the possibilities for conclusions limited.
Conclusions
Diagnosing patients with recurrent hypoglycemic episodes after bariatric surgery is important to prevent future health problems and late complications. We are proposing simple and clinically applicable methods to diagnose PBH in this study. We show that a questionnaire, Dumping Syndrome Rating Scale, combined with questions using the Sigstad’s dumping index was helpful to detect patients with PBH. Elevated C peptide after a standardized breakfast was also a useful diagnostic tool for recurrent hypoglycemic events. Using a CGM for 7 days combined with a food diary can facilitate patients with PBH to change their food choices, and other behaviors, in order to decrease the glucose variability and the risk of hypoglycemic events.
Since many patients experience non-specific and vague symptoms of hypoglycemia, an active approach with dumping syndrome questionnaires, assessment of metabolic parameters and CGM together with food registration is recommended.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the Swedish Ethical Review Authority, Stockholm (number 2015/1687-31/2). Participants gave informed consent to participate in the study before taking part.
References
Footnotes
Contributors JUH has contributed to patient recruitment, scientific design of the study, as well as implementation and execution of the study. She has also contributed to data management, data analysis and is the head writer of the manuscript. C-EL has contributed to patient recruitment, data management and writing of the manuscript. JUH is responsible for the overall content as the guarantor. MK has contributed to the scientific design of the study, as well as implementation and execution of the study. She has also contributed to data management, data analysis and writing of the manuscript.
Funding This study was supported by unrestricted grants from Nordic Infucare AB and Capio Forskningsfonder.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.