Article Text

Abstract
Introduction Higher concentrations of serum 25-hydroxyvitamin D (25(OH)D) and lower concentrations of parathyroid hormone (PTH) are associated with lower insulin resistance and incident diabetes in non-Hispanic White and Hispanic Americans. Results are mixed in other populations, with no observational studies in a large multiethnic cohort. The association of serum 25(OH)D with diabetes may vary by adiposity level.
Research design and methods Among 5611 participants in the Multi-Ethnic Study of Atherosclerosis without diabetes at baseline, cross-sectional associations of serum 25(OH)D with homeostasis model assessment of insulin resistance (HOMA-IR) and HOMA-β were examined using linear regressions. The association of 25(OH)D with incident diabetes over 9 years was examined using Cox proportional hazard regression.
Results Black Americans had the highest proportion of individuals with 25(OH)D<20 ng/mL (61%) and White Americans had the least (17%). Serum 25(OH)D was inversely associated with HOMA-IR in fully adjusted models (−0.34% difference in HOMA-IR per ng/mL higher 25(OH)D, p<0.0001). Longitudinally, a 1 ng/mL higher serum 25(OH)D was associated with 2% lower risk of incident diabetes (HR 0.982, CI 0.974 to 0.991), and a 1 pg/mL higher serum PTH was associated with 1% higher risk of incident diabetes (HR 1.007, CI 1.004 to 1.010), both prior to adjustment for waist circumference. After adjusting for waist circumference, a 1 ng/mL higher 25(OH)D was associated with 1% lower risk of incident diabetes (HR 0.991, CI 0.983 to 1.000). The magnitude of association of serum 25(OH)D with incident diabetes was largest at lower waist circumference (p for interaction=0.025). There was no heterogeneity by race/ethnicity (p=0.317).
Conclusions Serum 25(OH)D is inversely associated with insulin resistance and incident diabetes in a diverse cohort, including non-Hispanic White, Black, Hispanic and Chinese Americans. Future research should explore mechanisms for the interaction between serum 25(OH)D and adiposity in this relationship.
- Vitamin D
- Diabetes Mellitus, Type 2
- Insulin Resistance
- Adiposity
Data availability statement
Data may be obtained from a third party and are not publicly available. Data from MESA Examinations 1-5 are available on the NIH-NHLBI Biologic Specimen and Data Repository Information Coordinating Center (BioLINCC)
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic
Previous work has illuminated an inverse association of serum 25(OH)D with incident diabetes in white populations, but results in other populations are mixed.
What this study adds
The inverse association of serum 25(OH)D with incident diabetes does not vary by race/ethnicity.
The inverse association of serum 25(OH)D with incident diabetes does vary by adiposity level.
Parathyroid hormone predicts incident diabetes.
How this study might affect research, practice or policy
More research is needed to elucidate mechanisms for the interaction between adiposity and serum 25(OH)D in the association with incident diabetes.
Introduction
Vitamin D is a fat-soluble vitamin important for bone, glycemic, and overall health.1 Low serum 25-hydroxyvitamin D (25(OH)D) concentration causes an elevation in parathyroid hormone (PTH).1 The Endocrine Society Vitamin D guidelines set vitamin D deficiency as a serum 25(OH)D concentration of ≤20 ng/mL (51 nmol/L), insufficiency 21–29 ng/mL (52–71 nmol/L), and sufficiency is ≥30 ng/mL (≥72 nmol/L).2 These cut points are controversial and have been determined mostly from samples of European descent. There is evidence that vitamin D binding protein genotypes, which have different prevalence rates in different racial/ethnic groups, may affect vitamin D metabolism3 and cut points for deficiency, insufficiency and sufficiency. PTH reaches its nadir at a lower serum 25(OH)D concentration in Black Americans than it does in White Americans.4 In addition to variance in serum 25(OH)D by ancestry, serum 25(OH)D varies with adiposity. Greater fat mass is associated with lower serum 25(OH)D.5
Higher serum 25(OH)D levels are achieved by exposing skin to ultraviolet B radiation and/or consuming vitamin D in fatty fish, dairy, red meat, fortified foods, mushrooms, and other lesser sources.1 Vitamin D and PTH are well known for their role in bone metabolism, but 25(OH)D and PTH status is also associated with type 2 diabetes mellitus (T2DM) and related outcomes (fasting plasma glucose, hemoglobin A1c, insulin resistance, etc).6–8 Data from cross-sectional and longitudinal cohort studies consistently show these associations in White populations,6 9 but randomized controlled vitamin D supplementation trial data are mixed.
A 2007 review calculated a non-statistically significant odds ratio (OR) for incident T2DM of 0.54 (95% CI 0.23 to 1.27) comparing the highest to lowest serum 25(OH)D concentration.6 When the OR was recalculated excluding data from non-Hispanic Black people, there was a statistically significant correlation between T2DM prevalence and serum 25(OH)D concentration (OR 0.36, 95% CI 0.16 to 0.80).6 The differences in vitamin D homeostasis by racial group discussed above are one possible explanation for these results. There may also be heterogeneity by adiposity in the association of serum 25(OH)D with incident diabetes. The D2d trial of vitamin D supplementation in people with pre-diabetes found a significant reduction in incident diabetes among participants with body mass index (BMI) <30, but not among those with BMI ≥30.10
Because the association of vitamin D or PTH with diabetes may differ by racial/ethnic group9 11 12 and/or adiposity,10 as it does in other disease states,13 we analyzed the association of 25(OH)D and PTH with homeostasis model assessment of insulin resistance (HOMA-IR), HOMA-β cell function (HOMA-β) and diabetes incidence in a multiethnic cohort and tested for heterogeneity by race/ethnicity and adiposity.
Research design and methods
Participants
The Multi-Ethnic Study of Atherosclerosis (MESA) has been previously described.14 Briefly, it is a prospective cohort study evaluating characteristics of subclinical cardiovascular disease (CVD) and the risk factors that predict progression to clinically overt atherosclerotic cardiovascular disease (ASCVD). The baseline examination was conducted between 2000 and 2002. We used diabetes incidence data from examination 2 (2002–2004) through examination 5 (2010–2012). Participants included 6814 individuals with White, Black, Hispanic, or Chinese race/ethnicity aged 45–84 years, without known ASCVD. Participants without diabetes at baseline (fasting glucose <126 mg/dL, no self-reported physician diagnosis of diabetes, and no use of diabetes medication) were included (n=5931). Participants with missing values in independent variables or covariates (PTH, annualized total 25(OH)D, education, occupation, smoking, physical activity, alcohol use, systolic blood pressure, waist circumference) were excluded for a final sample of 5611. An institutional review board for each institution participating in MESA approved the study. All participants gave written informed consent.
Baseline assessments
Standardized questionnaires were used to measure demographic variables, smoking status, physical activity, medical history, alcohol use, and medication use. Trained research staff measured height, weight, waist circumference, and blood pressure. BMI was calculated from height and weight (kg/m2). Blood pressure was measured three times with the participant seated. The average of the second and third measurements was used. Blood was collected between 07:30 and 10:30 am after a 12-hour fast. Estimated glomerular filtration rate (eGFR) was calculated from serum creatinine and cystatin C using the CKD-EPI equation.15 Vitamin D metabolites were measured from frozen serum via immunoaffinity extraction and high-performance liquid chromatography tandem mass spectrometry (HPLC-MS).16 Total 25(OH)D was calculated as the sum of 25(OH)D2 and 25(OH)D3, then annualized as described elsewhere.17 The inter-assay coefficients of variation were 8.5% for 25(OH)D3 at 24.8 ng/mL and 11.8% for 25(OH)D2 at 7.0 ng/mL. We used cut-off points published in the Endocrine Society Clinical Practice Guidelines2 to divide participants into clinically relevant vitamin D status groups. Participants with undetectable 25(OH)D2 (<0.06 ng/mL, 17.6% of the sample) were coded as having 0 ng/mL 25(OH)D2.
PTH was measured from frozen serum via Beckman-Coulter DxI automated 2-site immunoassay (Beckman-Coulter, Brea, California, USA).3 Low and high inter-assay coefficients of variation were 6.1% and 3.4%, respectively.18
Serum insulin was measured with the Linco Human Insulin Specific RIA Kit (Linco Research, St. Charles, Missouri, USA). Serum glucose was measured by rate reflectance spectrophotometry with thin film adaptation of the glucose oxidase method via the Vitros analyzer (Johnson & Johnson Clinical Diagnostics, Rochester, New York, USA). HOMA-IR was calculated from fasting insulin and glucose (insulin (μU/L) × glucose (nmol/L)/22.5). HOMA-β was calculated with the equation 360 × fasting insulin (μU/mL)/(fasting glucose (mg/dL) − 63).19
Determination of incident diabetes
Diabetes was defined as fasting glucose ≥126 mg/dL,20 self-reported physician diagnosis of diabetes, or use of diabetes medication. Time of incident diabetes was defined as the midpoint between the last examination free of diabetes and the first examination where diabetes was detected.21 22 We censored participants who did not develop diabetes at their last examination.
Statistical analysis
Our conceptual model is shown in online supplemental figure 1. Descriptive statistics were used to report baseline characteristics by vitamin D sufficiency groups. Linear regression models were used to examine the cross-sectional associations of HOMA-IR and HOMA-β with total annualized 25(OH)D and PTH. The natural logarithm of HOMA-IR and HOMA-β were used in the analyses due to skewness.
Supplemental material
Cox models for incident diabetes were fit using PTH and total annualized 25(OH)D at baseline as exposures. Both unadjusted and adjusted models (covariates: age, sex, study site, race/ethnicity, education, occupation, eGFR, systolic blood pressure, smoking, physical activity, alcohol use, BMI, and waist circumference at baseline) were fit. BMI or waist circumference were added last in separate models. Only waist circumference models are presented here, as waist circumference is the better measure of adiposity,23 and BMI models were similar. Interaction terms between baseline covariates (continuous: age, BMI, and waist circumference; and categorical: sex, race/ethnicity and glucose <100 (normoglycemia) vs ≥100 mg/dL (pre-diabetes)) and PTH and total annualized 25(OH)D were also tested to evaluate heterogeneity. For models with significant interaction terms, the nature of the interaction was visualized by plotting the linear predictor (Xβ) in the hazard function for quartiles of waist circumference across the values of PTH and 25(OH)D (non-parallel lines indicate the interaction effect). Statistical significance of analyses was defined as p<0.05 and p<0.10 for interactions.24 Analyses were performed using SAS V.9.4 (SAS Institute).
Results
Baseline characteristics of the participants (n=5611) are shown in table 1. Serum total annualized 25(OH)D varied by race/ethnicity, with the highest percentage of the sample with vitamin D deficiency in black populations and the lowest in Chinese American populations.
Baseline characteristics of MESA participants without diabetes by serum 25 hydroxyvitamin D categories
In cross-sectional analyses (table 2), annualized total serum 25(OH)D was inversely associated with log-HOMA-IR in unadjusted and adjusted models (all p<0.0001). PTH was positively associated with log-HOMA-IR in unadjusted models only (p<0.001, table 2). There was no association between log-HOMA-β and 25(OH)D in fully adjusted models. In unadjusted models, total annualized 25(OH)D was inversely associated with log-HOMA-β, while PTH was positively associated with log-HOMA-β (p<0.05, table 2). Similar results were found when serum 25(OH)D was analyzed categorically (online supplemental table 1).
Supplemental material
The association of annualized 25 hydroxyvitamin D and parathyroid hormone with incident diabetes (n=5611)
In longitudinal analyses (table 2), median follow-up time was 9.08 years. A 1 ng/mL higher total annualized 25(OH)D was associated with a 2% lower risk of incident diabetes after adjustments for demographic factors, kidney function, systolic blood pressure, physical activity, alcohol consumption, and smoking (model 1, p<0.0001). Additional adjustment for waist circumference (model 2) attenuated the findings; total annualized 25(OH)D was associated with a 1% lower risk of incident diabetes per 1 ng/mL higher serum concentration (model 2: HR 0.99, CI 0.98 to 1.00, p=0.056, table 2). A 1 pg/mL higher PTH was associated with 0.7% higher incident diabetes risk in models adjusted for demographic factors, kidney function, systolic blood pressure, physical activity and smoking (HR 1.007, CI 1.004 to 1.010, p<0.0001, table 2). The association between PTH and incident diabetes was also attenuated in the waist circumference model (HR 1.003, 95% CI 1.000 to 1.006, p=0.0948).
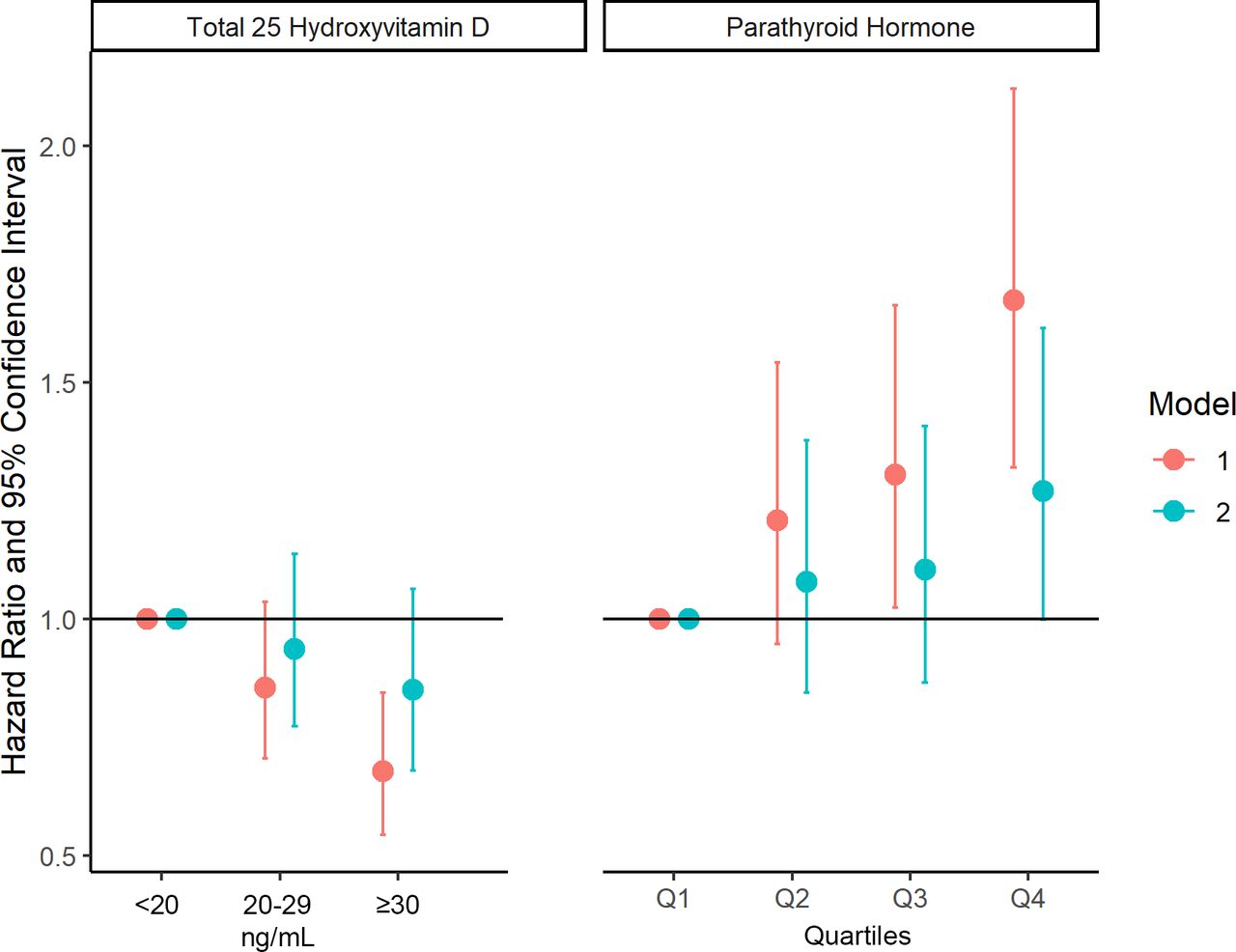
Similar trends in the relationship between incident diabetes and 25(OH)D or PTH were seen when analyzed categorically (online supplemental table 2 and figure 1). Those with 25(OH)D≥30 ng/mL had a lower risk of incident diabetes than those with 25(OH)D<20 ng/mL) after adjustment for demographic factors, kidney function, systolic blood pressure, physical activity, alcohol consumption, and smoking (OR 0.68, 95% CI 0.54 to 0.84). This relationship was no longer significant after adjustment for waist circumference. People in the highest quartile of PTH had higher risk of incident diabetes than those in the lowest quartile after adjustment for demographic factors, kidney function, systolic blood pressure, physical activity, alcohol consumption, and smoking (OR 1.67, 95% CI 1.32 to 2.12), but there was no significant association after adjustment for waist circumference.

The categorical associations of total annualized 25 hydroxyvitamin D and parathyroid hormone with incident diabetes (n=5611).
Interaction terms between waist circumference (continuous) and total annualized 25(OH)D and PTH were significant (p=0.025 and p=0.001, respectively, online supplemental table 3). Figure 2 and online supplemental figure 2 demonstrate the nature of the interaction between 25(OH)D and waist circumference or BMI by plotting the linear predictor (Xβ) in the hazard function. At lower values of waist circumference, there is a greater inverse association of 25(OH)D with incident diabetes (steeper negative slope), as compared with higher waist circumference values (flatter slope). For the interaction between PTH and BMI or waist circumference (figure 2 and online supplemental figure 2), at lower waist circumference there is a greater association between PTH and incident diabetes (steeper slope) compared with higher waist circumference levels (flatter slope). The interaction term for race/ethnicity was not statistically significant and the estimates were similar (online supplemental tables 3 and 4).
Supplemental material

{kind=link}
{kind=link}
The interaction between 25 hydroxyvitamin D or parathyroid hormone and waist circumference as evidenced by different slopes (Xβ) in the hazard model describing incident diabetes. The three lines represent the slope of 25 hydroxyvitamin D (x-axis) predicting Xβ in the hazard model (y-axis) such that one line was plotted for the cut point of the first quartile of waist circumference (87.4 cm), a second line for the cut point of the second quartile of waist circumference (96.2 cm), and a third line for the cut point of the third quartile of waist circumference (105 cm). WC, waist circumference (cm).
Discussion
In this multiethnic analysis, serum 25(OH)D and insulin resistance were inversely associated. Annualized 25(OH)D was inversely associated with incident diabetes, while PTH was positively associated with incident diabetes, with differences by adiposity, but not race/ethnicity. Participants with lower waist circumference had a greater magnitude of the association of 25(OH)D and PTH with incident diabetes. This has important implications for the interpretation of previous studies which found no association and enrolled a majority of individuals with high adiposity.10 12 25 26
The association of 25-hydroxyvitamin D and PTH with homeostasis model of insulin resistance and β-cell function
The hypothesized association of 25(OH)D with HOMA-IR and HOMA-β was demonstrated, with annualized total 25(OH)D levels being inversely associated with HOMA-IR. Similar to current findings, an analysis of National Health and Nutrition Examination Survey (NHANES) III showed an inverse association between serum 25(OH)D and log HOMA-IR, and no association of serum 25(OH)D with log HOMA-β.11 Other studies have found an association between serum 25(OH)D and insulin resistance.7 27–30 Kayaniyil et al27 examined the association between serum 25(OH)D and HOMA-IR in 712 Canadians and found higher serum 25(OH)D was associated with lower HOMA-IR (p=0.007) when adjusting for BMI, PTH, physical activity, supplement use, age, sex, season, and ethnicity. They also found a weaker association between 25(OH)D and insulin resistance among those with higher BMI. In the current study, there was no association between PTH and HOMA-IR and HOMA-β in adjusted models similar to results obtained by Zhao et al in their analysis of NHANES data.29
25-Hydroxyvitamin D and incident diabetes
Vitamin D deficiency is associated with lower beta cell function and higher insulin resistance, the hallmarks of T2DM. Because β cells and peripheral insulin-sensitive tissues need vitamin D to function properly,31 we hypothesized that those with lower serum 25(OH)D concentrations would have higher incidence of T2DM. We showed that serum total annualized 25(OH)D is inversely associated with incident diabetes risk. The findings are consistent with other longitudinal cohort studies; higher serum 25(OH)D is associated with lower risk of developing diabetes.28 32 33 A meta-analysis of 21 prospective studies (n=76 220) calculated a summary risk ratio (RR) of 0.62 (95% CI 0.54 to 0.70) of incident T2DM risk comparing highest to lowest category of serum 25(OH)D concentration.33 This is similar to the magnitude of association we measured in our analysis of incident diabetes risk by serum 25(OH)D categories prior to the adjustment for waist circumference. Limits of the studies included in the meta-analysis were lack of diversity of participants (mostly non-Hispanic White populations) and heterogeneity in the T2DM classification methods and vitamin D assay methods.33 Our analysis differs from the majority of those included in this meta-analysis because of our diverse sample, gold standard method of 25(OH)D measurement, and biological ascertainment of diabetes with fasting glucose. The current study is further differentiated by adjusting for waist circumference and performing interaction analyses by waist circumference. Only 6 of the 21 studies in the meta-analysis adjusted for BMI, and those studies yielded a numerically lower magnitude of association than six studies that did not adjust for BMI (RR 0.66, CI 0.56 to 0.77 vs RR 0.54, CI 0.47 to 0.61, p for interaction 0.06).33
Trials of vitamin D supplementation and incident diabetes have been completed.10 26 28 Double-blinded trials specifically designed to measure incident diabetes that were of sufficient duration to measure this outcome, and gave an adequate dose of vitamin D have been completed and did not show reduction in diabetes risk.10 26 Both of these trials enrolled people with pre-diabetes without consideration for vitamin D status. Mean serum 25(OH)D at baseline was 24 and 28 ng/mL, which is close to vitamin D sufficiency by the strictest definition. This was done because it is unethical to have a placebo group of people with known vitamin D deficiency, leaving them untreated. Ethics also dictated that researchers must allow outside-of-study vitamin D consumption from foods and supplements. Partaking in outside sources of vitamin D is a major confounder, which was not measured or used as an adjustment. These studies are also limited by the majority of their sample having high adiposity, which we have demonstrated weakens the association between 25(OH)D and incident diabetes. Despite these limitations, meta-analyses of these and similar studies show vitamin D supplementation at doses higher than 1000 IU/day reduced risk of new-onset diabetes in people with pre-diabetes, especially among those with BMI<30 kg/m2.34 35
PTH and incident diabetes
To the authors’ knowledge, only two other studies have assessed the relationship between PTH and incident diabetes.9 36 Reis et al found a positive association of PTH with incident diabetes only among White participants of the ARIC study, even after adjustment for BMI and 25(OH)D.9 There was no association among Black participants, before or after adjustment for BMI. In a study of Hong Kong Chinese people, Sing et al found no association between PTH and incident diabetes.36 These results differ from the current results, which revealed a positive association between PTH and incident diabetes independent of racial/ethnic group (Black, White, Hispanic, or Chinese American) before adjustment for waist circumference.
Incident diabetes interactions: adiposity
There is a triangle of associations between adiposity, T2DM, and serum 25(OH)D. Higher adiposity is associated with higher incidence of T2DM,37 higher serum 25(OH)D is associated with lower incidence of T2DM,6 and higher adiposity is associated with lower serum 25(OH)D.38 Suggested mechanisms for these associations include chronic inflammation, β cell dysfunction, and dilution of 25(OH)D stores. Increasing adiposity leads to insulin resistance and β cell failure brought on by chronic inflammation in some people, culminating in T2DM.39 Similarly, low serum 25(OH)D inhibits proper β cell function and insulin sensitivity in rats and cultured cells.6 In humans with high adiposity, fat-soluble vitamin D dissolves into adipocytes, with greater fat mass leading to greater dilution of stores and lower blood concentration.5 Others have theorized that vitamin D is ‘sequestered’ in adipose tissue, implying that once the vitamin enters adipose tissue it does not exit the tissue easily. The evidence does not support this theory, as 25(OH)D in adipose tissue declines after the cessation of supplementation and helps maintain elevated serum levels of 25(OH)D for months.40 More research is needed to settle the dilution versus sequestration debate.
The magnitude of association between adiposity and T2DM is larger than the association between serum 25(OH)D and T2DM.37 41 It is possible that in people with high adiposity, any T2DM-risk-lowering effect of high serum 25(OH)D is overwhelmed by the effect of high adiposity on risk for T2DM. This would explain our results. We found an interaction between waist circumference and 25(OH)D and PTH in relation to incident diabetes. Those with higher waist circumference saw less reduction in diabetes risk with higher serum 25(OH)D or lower PTH concentrations.
In the two vitamin D supplementation trials mentioned above, both controlled for BMI in their Cox proportional hazards models.10 26 The D2d research group presented HRs for T2DM stratified by BMI status (≥ or <30 kg/m2). Intervention participants with a BMI <30 had a lower risk of developing T2DM compared with controls with a BMI <30 (HR 0.71, CI 0.53 to 0.95). In intervention and control participants with a BMI ≥30, the HR was not significantly different from 1 (HR 0.97, CI 0.80 to 1.17).10 This is congruent with the results of the current study. In people with lower waist circumference, the effect of 25(OH)D on incident T2DM risk was greater than in people with higher waist circumference. More research is needed to elucidate mechanisms for this interaction.
Race/ethnicity
Previous studies have found an interaction between serum 25(OH)D and race/ethnicity in relation to incident T2DM.11 12 32 Reis et al found reduced risk of diabetes with higher serum 25(OH)D among 8120 White people, but not among 2102 Black people (p for interaction 0.004).32 This is congruent with results from a nationally representative cross-sectional study, NHANES III, where a correlation was observed between serum 25(OH)D and diabetes prevalence, but only among non-Hispanic White and Hispanic populations, not among non-Hispanic Black populations.11 Our results differ—we did not uncover an interaction by race/ethnic group—possibly because our sample size is smaller than the aforementioned studies. Another reason for the lack of an interaction is that despite Black Americans having lower serum 25(OH)D concentrations than White Americans, Black Americans have similar levels of bioactive 25(OH)D.42
Mechanisms
Mechanisms for the possible effect of 25(OH)D on T2DM incidence have not been concretely elucidated. One of the prevailing theories is 1,25(OH)2D modifies pancreatic islet cell physiology and the expression and function of the insulin receptor.31 Pancreatic islet cells express 1-alpha-hydroxylase, the enzyme that converts the inactive 25(OH)D to the active 1,25(OH)2D. Active 1,25(OH)2D from local and other endogenous sources bind to the vitamin D receptors that islet cells also express.6 One of the effects of 1,25(OH)2D binding to its receptor is a change in the expression of over 200 genes with a vitamin D response element.1 One notable gene with this element is the insulin receptor, which may help explain the association between 25(OH)D and insulin resistance. 1,25(OH)2D also affects islet cell physiology indirectly through its known effect on extracellular calcium concentration and the flux of calcium across cellular membranes.6 This is a very important function of 1,25(OH)2D, as both insulin secretion and the insulin-mediated activities that follow insulin binding its receptor are calcium-dependent processes.6 A hallmark of T2DM risk and progression is systemic inflammation.43 In vitro and animal studies suggest 25(OH)D has anti-inflammatory effects,6 43 which may slow the progression of T2DM. Human data on the relationship between 25(OH)D, inflammation, and T2DM are limited, and what data are available have generated conflicting findings.28 43 More research is needed to explain the interaction between waist circumference and 25(OH)D in incident diabetes.
Strengths and limitations
Strengths of the current analyses include a large, diverse sample of White Americans, Black Americans, Hispanic Americans, and Chinese Americans, all in appreciable proportions. The sample was socioeconomically diverse. Another strength is that vitamin D was measured via HPLC-MS, which is the gold standard for this measurement. The covariates were collected using standardized questionnaires and diabetes was ascertained using fasting glucose, diabetes medications, and self-reported physician diagnosis of diabetes. In addition, the current study assessed various aspects of glucose dysregulation, including insulin-based indices and glycemic status. Despite these strengths, the analyses must be viewed in light of some limitations. Despite its diversity, our sample is not representative of the US population unlike previous studies in NHANES.11 12 The analyses did not include an assessment of ancestry or genetics, which may better characterize participants than racial/ethnic group. The analyses did not include assessment of vitamin D binding protein, which precludes the assessment of bioavailable vitamin D. Additionally, the ascertainment of diabetes did not include hemoglobin A1c or oral glucose tolerance testing. Finally, these results are observational in nature and no conclusions about causation can be made; however, Mendelian randomization studies done in white and Asian populations suggest that the serum-25(OH)D-associated single nucleotide polymorphism (SNP) in the DHCR7-rs12785878 locale is causally associated with risk of diabetes.44 More research is needed on this and other serum-25(OH)D-associated SNPs.
Conclusion
Serum 25(OH)D is inversely associated with insulin resistance and incident diabetes in a diverse cohort including non-Hispanic White, Hispanic, Black, and Chinese Americans. Waist circumference modified the results with a greater magnitude of effect at lower waist circumference, consistent with a recent clinical trial, suggesting that further work to understand the interactions between vitamin D, adiposity, and glycemia are paramount.
Data availability statement
Data may be obtained from a third party and are not publicly available. Data from MESA Examinations 1-5 are available on the NIH-NHLBI Biologic Specimen and Data Repository Information Coordinating Center (BioLINCC)
Ethics statements
Patient consent for publication
Ethics approval
This was an analysis of anonymized data, so no IRB approval was necessary. Exempted this study. Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors AW drafted the manuscript. Statistical analyses were performed by SZ, GB, and DK. All authors were involved in the design of the project. All authors contributed to the critical revision of the manuscript and approved the final version. The guarantor of this work is JJJ.
Funding The MESA study was supported by contracts HHSN268201500003I, through N01-HC-95169 from the National Heart, Lung, and Blood Institute and by grants UL1-TR-000040 and UL1-TR-001079 from The National Center for Research Resources. Funding for 25-hydroxyvitamin D measurements was provided by R01HL096875 from the NIH (to IHdB and BK). The analyses and preparation of the manuscript was supported by NIDDK (K23DK117041, JJJ) of the NIH and The Robert Wood Johnson Foundation Harold Amos Medical Faculty Development Program (ID# 76236, JJJ) and NCATS (UL1TR002733, GB).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.