Article Text

Abstract
Introduction To compare the conventional treatment of gestational diabetes mellitus (GDM) with flexible treatment according to the measurement of fetal abdominal circumference (AC) in daily clinical practice.
Research design and methods Two hundred and sixty pregnant women diagnosed with GDM before week 34 were randomly placed in two groups: a control group, treated according to maternal capillary glycemia, and an experimental group, treated according to ultrasound parameters of fetal growth. The glycemic targets in the control group were blood glucose levels when fasting and 1 hour postprandial (<95/140 mg/dL). In the experimental group, glycemic targets depended on the percentile (p) of fetal AC: if AC p <75th, then blood glucose targets when fasting and at 1 hour postprandial were <120/180 mg/dL; and if AC p ≥75th, then the glycemic targets were <80/120 mg/dL. The follow-up of both groups was scheduled according to the GDM protocol of our diabetes and gestation unit.
Results The study was completed by 246 pregnant women, 125 in the control group and 121 in the experimental group. In the experimental group, insulin treatment and neonatal hypoglycemia were significantly lower (p=0.018 and p 0.035, respectively). No differences were observed in large and small infants according to gestational age. However, macrosomic infants were less frequent in the experimental group, although this difference did not reach statistical significance. In terms of gestation complications, the type of delivery and its complications and the rest of the neonatal complications analyzed, no significant differences were observed.
Conclusions The treatment of flexible GDM according to the measurement of fetal AC is safe for the mother and the fetus and almost halves the number of pregnant women who require insulin treatment, without increasing the number of ultrasound checks or medical visits.
- Gestational Diabetes Mellitus
- Insulin
- Birth Weight
- Ultrasonography
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Flexible treatment of gestational diabetes mellitus (GDM) according to fetal abdominal circumference (AC) provides some additional benefit, which is of similar magnitude to that offered by conventional treatment compared with regular obstetric care. However, to achieve this benefit, more demanding follow-up is needed with a greater frequency of ultrasound examinations and insulin treatment.
WHAT THIS STUDY ADDS
Flexible treatment of GDM according to the measurement of fetal AC does not improve neonatal outcomes for large and small newborns in terms of gestational age, but could reduce the number of newborn macrosomia and reduces neonatal hypoglycemia without increasing the number of ultrasound checks and medical visits, and halves insulin treatment.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The flexible treatment of GDM according to the measurement of fetal AC allows for the optimization of resources by directing therapeutic effort towards the pregnancies with the highest risk of fetal overgrowth and relaxing follow-up in the pregnancies at lower risk. This optimization of resources would allow us to apply more up-to-date diagnostic criteria for GDM, with lower glycemic thresholds, since it has been shown that there is no turning point in maternal glycemia at which the perinatal adverse effects of GDM are reduced.
Introduction
Conventional treatment of gestational diabetes mellitus (GDM) aims at the strict control of maternal glycemia, through modifications in lifestyle, diet and exercise, and if glycemic objectives are not achieved, pharmacological treatment with insulin is adopted as the first choice.1 This treatment strategy, adapted from the treatment of pregestational diabetes during pregnancy, has improved perinatal morbidity, reducing the incidence of adverse outcomes, such as macrosomia and shoulder dystocia.2 3 However, it involves intensive monitoring and treatment of all women with GDM, although only about 20% have fetal macrosomia when GDM goes untreated.4
This situation, together with the lack of a tipping point in the relationship between maternal glycemia and adverse pregnancy outcomes, which the Hyperglycemia and Pregnancy Outcome (HAPO) study has confirmed,5 both advocate the use of the fetal growth measurement to identify which fetuses in the womb are at a greater or lower risk of complications.6
The flexible treatment of GDM according to fetal abdominal circumference (AC) relaxes glycemic targets in women whose fetuses are at a low risk of overgrowth and intensifies therapy by using lower glycemic targets for those at a high risk of growth.6 The threshold for discriminating between a low or high risk to fetal growth is set at the 75th percentile (p) of the fetal AC measurement: AC p <75th indicates a low risk and AC p ≥75h suggests a high risk.7 The flexible treatment of GDM according to the measurement of fetal AC is based on the relationship between the pathophysiology of diabetic fetopathy and the clinical evaluation of its effects on the fetus. Fetal hyperinsulinism plays a central role in the development of diabetic fetopathy8 9 and can be determined indirectly by measuring insulin levels in the amniotic fluid (AF), reflecting urinary insulin excretion from the fetus.10 11 Insulin levels in the AF in diabetic pregnancies were positively correlated with increased AC percentiles determined by ultrasound at the time of amniocentesis.7 An AC equal to or greater than the 75th percentile for gestational age identifies all cases of severe hyperinsulinism (>16 μU/mL) related to diabetic fetopathy.7 12
To date, four randomized controlled clinical trials in different populations have used fetal AC measurement to identify fetuses at high and low growth risks and to stratify medical therapy based on this risk: Buchanan et al,13 Kjos et al,14 Schaefer-Graf et al15 and Bonomo et al.16 Overall, compared with conventional therapy, the use of flexible therapy resulted in a reduction in large for gestational age (LGA) infants in more than 50% of cases and a decrease in small for gestational age (SGA) infants in more than 40%, even though no statistical significance was reached.6 The systematic review and meta-analysis carried out by Balsells et al in 2014, which included the two most recent studies at the time, concluded that ultrasound-guided treatment improves perinatal outcomes in terms of abnormal birth weight of a magnitude similar to that offered by conventional treatment when compared with normal obstetric care. However, to achieve this benefit, more demanding follow-up was needed with more frequent ultrasound examinations and insulin treatment.17
Taking into account all of the aforementioned information, together with the fact that fetal AC is a standard component of the basic fetal ultrasound examination, we proposed carrying out the present study with the aim of comparing conventional GDM treatment with flexible treatment based on the measurement of fetal AC in daily clinical practice.
Methods
Study design
A randomized clinical trial with two groups (a control group, treated according to maternal criteria (MC), and an intervention group, treated according to fetal criteria (FC)) was carried out by the Diabetes and Gestation Unit at the Hospital Clínico Universitario Virgen de la Arrixaca (HCUVA), which is part of the Endocrinology and Nutrition Service and the Obstetrics and Gynecology Service.
Once the patients were recruited, they were randomly assigned to either of the study groups: (1) the group using MC for the treatment of GDM, established according to maternal capillary glycemia, or (2) the group using FC for the treatment of GDM, established based on ultrasound parameters of fetal growth. Randomization was performed with a randomized computer-generated number table. The control objectives set for each group were
MC group: fasting capillary glycemia of <95 mg/dL and glycemia at 1 hour postprandial of <140 mg/dL.
FC group:
If AC p was <75: fasting capillary glycemia was <120 mg/dL and glycemia 1 hour postprandial was <180 mg/dL.
If AC p is ≥75: fasting capillary glycemia was <80 mg/dL and glycemia 1 hour postprandial was <120 mg/dL.
All patients were instructed on diet, exercise and performing capillary glycemic self-controls by the diabetes nurse educator. A balanced diet was recommended for adequate weight gain during pregnancy according to prepregnancy body mass index (BMI).18 Complex carbohydrates were advised over simple ones, and their intake was distributed into three meals and three snacks to reduce postprandial glucose fluctuations and overnight fasting. It was recommended to perform mild–moderate intensity aerobic exercise regularly adapted to the physical capacity of the pregnant woman, provided that there was no obstetric contraindication. In general, sessions of 30–60 min duration at least 5 days a week were recommended. Patients had fasting capillary blood glucose self-checks in the mornings and 1 hour after breakfast, lunch and dinner, and wrote them down on a log sheet. Capillary glycemia was performed using the ContourXT blood glucose monitoring system.
All patients were asked for a blood analysis when entering the study, including baseline glycemia and insulinemia, glycosylated hemoglobin and vitamin D. Insulin resistance rate (HOMA-IR, homeostatic model assessment of insulin resistance) was calculated (blood glucose (mg/dL)×insulinemia (μIU/mL)/405).19
The follow-up of the patients was scheduled according to the protocol established for GDM in the diabetes and gestation unit with joint reviews by Endocrinology and Obstetrics every 4–6 weeks from the diagnosis of GDM until week 38. From week 38 the reviews were weekly until the end of delivery. In the FC group, fetal AC percentile assessment to establish glycemic control targets was performed with ultrasound controls from entry into the study and up to week 34. Ultrasound checks were performed using GE Voluson S8 echography. The AC percentiles were obtained by applying the table of Snijders and Nicolaides.20 A more frequent control was adopted if the pregnant woman had poor metabolic control, hypertensive disease due to the pregnancy, intrauterine growth retardation or other similar conditions. Patients were instructed to come to the consultation immediately if glycemic control targets were exceeded on more than three occasions in the same week.
For those patients who did not achieve the glycemic control objectives established for each group in terms of diet and exercise on more than three occasions in the same week, insulin treatment was initiated. For the control of fasting blood glucose, 0.1 UI/kg/day insulin determir was prescribed at night and patients were instructed about self-adjustment in order to achieve fasting blood glucose targets.
For the control of postprandial glycemia, insulin as part was prescribed in the corresponding meal. Treatment began with 2 UI and patients were instructed to self-adjust until postprandial glycemia targets were achieved.
The completion of the pregnancy was scheduled according to the criteria of the Unit established by the Obstetrics and Gynecology Service: If GDM was resolved with diet and exercise then labor was induced at week 41. If insulin-treated GDM led to good metabolic control, induction of labor was during week 38 and if there was poor metabolic control or maternal-fetal complications, induction was at week 37 or earlier if needed. If estimated fetal weight was>4500 g or>4000 g with a history of shoulder dystocia, a cesarean section was scheduled.
During childbirth, patients treated with insulin during pregnancy underwent hourly controls of capillary glycemia and were treated with an intravenous insulin infusion if capillary glycemia>110 mg/dL.
The Endocrinology physicians and the diabetes educator who treated the patients knew the treatment group to which patients were allocated because they needed it to establish glycemic control targets and to indicate insulin treatment when these targets were not met. The obstetricians who performed the ultrasounds, gestational follow-up and delivery care did not know the group to which the patients were assigned. Neither did the midwives, nurses nor the auxiliary nurses who attended the patients during delivery. The pediatric physicians and the nurses and nursing assistants who attended the newborns were also unaware of the group to which the mothers of the newborns were assigned.
Data on gestational complications, delivery data and newborn data were obtained from the clinical reports made by obstetricians, midwives and pediatricians, recorded in the Selene Clinical Station (computerized clinical records).
This study was integrated within the daily clinical practice of our hospital, in which the measurement of newborns is performed by the nursing staff with a tape measure. Also, newborns to mothers with GDM underwent capillary glycemia controls at birth and every 2 hours during the first 6 hours of life and subsequently every 6 to 24 hours, regardless of whether or not the mother was treated with insulin during gestation.
Study population
The study population consisted of pregnant women referred to the diabetes and gestation unit of the HCUVA with a diagnosis of GDM who met the inclusion criteria. The inclusion criteria for the study were (1) diagnosis of GDM in the second or third trimester of gestation, (2) gestational age of <34 weeks, (3) gestation of a single fetus and (4) maternal age of ≥18 years. The diagnosis of GDM was established according to the recommendations of the Spanish Diabetes and Pregnancy Group21 using the two-step strategy and with a 100 g 3-hour oral glucose tolerance test (OGTT), applying the diagnostic criteria of the National Diabetes Data Group (two or more of the four OGTT values above thresholds: baseline ≥105 mg/dL, 1 hour ≥190 mg/dL, 2 hours ≥165 mg/dL and 3 hours ≥145 mg/dL).22 In our setting, GDM screening is performed universally between 24 weeks and 28 weeks of pregnancy or during the first trimester in pregnant women with risk factors. The main risk factors for GDM are maternal age of >35 years, obesity, polycystic ovary syndrome, previous GDM, history of fetal macrosomia and first-degree family history of diabetes mellitus. The O'Sullivan test (50 g of glucose load) is considered positive if the blood glucose at 1 hour is ≥140 mg/dL.
For patient recruitment (February 2017–March 2019) pregnant women who met the inclusion criteria were invited to participate in the study. Patients who agreed to participate signed informed consent after explaining the study protocol in detail.
Study objectives
The objective of this study was to compare the conventional treatment of GDM with a flexible treatment according to the fetal AC measurement in daily clinical practice, and thus without the need to increase the number of medical appointments or ultrasound controls, based on (1) neonatal outcomes in terms of large and small birth weight for gestational age; (2) insulin treatment needs; (3) perinatal complications, such as shoulder dystocia, traumatic injuries, cesarean sections, induced labor, loss of fetal well-being, respiratory distress, hypoglycemia, hypocalcaemia, hyperbilirubinemia and admission to the neonatal intensive care unit (ICU); and (4) gestational complications associated with GDM and its treatment, including hypertensive states of pregnancy, prematurity, maternal weight gain and maternal hypoglycemia.
Statistical analysis
For the calculation of the sample size, it was taken into account that the variance in the weight of the newborn of mothers with GDM is 1.8 kg. To detect a difference of 700 g between the two groups under study with a statistical significance of 0.05 and a power of 0.8, it would be necessary to have 82 patients per group. Assuming a 15% loss, the number would increase to 96 patients per group. It was agreed to recruit 110 patients per group. Finally, 130 patients were recruited per group.
Newborns were classified as LGA and SGA if the birth weight was >90th percentile or <10th percentile, respectively, based on sex-specific growth curves for Carrascosa’s Spanish population.23
Quantitative variables were expressed as means and SD. Qualitative variables were expressed as frequencies and percentages. The analysis of the quantitative variables was carried out using Student’s t-test and the qualitative variables were analyzed using the χ2 test. The results are considered significant for a level of p<0.05.
Statistical analysis was performed using the SPSS V.20.0.
Results
A total of 260 pregnant women were randomized, 130 in each study group. For data analysis, 246 pregnant women were considered, 125 in the MC group and 121 in the FC group, after excluding pregnant women who did not give birth in the HCUVA.
Maternal and fetal characteristics at study entry were not significantly different between the two groups (table 1).
Maternal and fetal characteristics at the start of the study
Maternal data
In the maternal follow-up data (table 2), there were significant differences between the two groups in terms of glycemic control and insulin treatment. Glycemic control was better in the FC group. Excellent glycemic control was achieved in almost 75% of the pregnant women in the FC group, while it did not reach 50% in the MC group. However, poor glycemic control was similar in both groups, around 12%.Insulin treatment was more frequent in the MC group where 24% of pregnant women needed it, while in the FC group, it was only necessary in 12.5%, that is, in half of the cases.
Maternal follow-up data
In relation to maternal hypoglycemia, there were no significant differences between the two groups compared with the total number of patients in the study (table 2), or compared with the number of insulinized patients (16.7% in the MC group vs 26.7% in the FC group) (p=0.524). There were no severe hypoglycemias requiring the intervention of third parties in either of the groups.
Regarding the other maternal follow-up control data such as weight gain during pregnancy, gestational age at which insulin treatment is initiated and maximum insulin doses, there were also no significant differences between the two groups (table 2).
Pregnancy complications
There were no significant differences between the two groups for pregnancy complications reported in this study, either grouped or individually (table 3). The threat of preterm birth was three times more frequent in the MC group, although this did not reach statistical significance.
Gestational complications
Birth data
When we consider gestational age at delivery, initiation and end of delivery (induced deliveries, instrumented deliveries, total and urgent cesarean sections) there were no significant differences between the two groups (table 4). As for the pelvis–fetal disproportion, in close relation to fetal size, it was three times more frequent as a cause of urgent cesarean section in the MC group, although this difference did not reach statistical significance.
Birth and newborn data
There were also no significant differences in the complications of childbirth recorded in this study between the two groups, either grouped or individually (table 4). Although they did not involve significant differences, two shoulder dystocias were recorded in the MC group. There were no cases of maternal death.
Newborn data
There were no significant differences between the two groups in terms of the anthropometric data or in the Apgar newborn test (table 4). There were also no significant differences in the number of LGA and SGA newborns between the two groups. Although statistical significance was not reached, the BMI of LGA newborns was almost one point higher in the MC group. Also, in the MC group, almost 73% of newborn were macrosomic (8 out of 11), although this difference did not reach statistical significance either.
All newborn complications recorded in this study were more frequent in the MC group, but the difference was only statistically significant for newborn hypoglycemia (9 out of 11) (table 4). As for the rest of the complications, it should be noted that 80% of clavicle fractures (four out of five), the two brachial plexus injuries, and 75% of admissions to the neonatal intencive care unit (ICU) (three out of four) were in the MC group. There were no cases of hypocalcaemia, sepsis or neonatal death.
Cross analysis
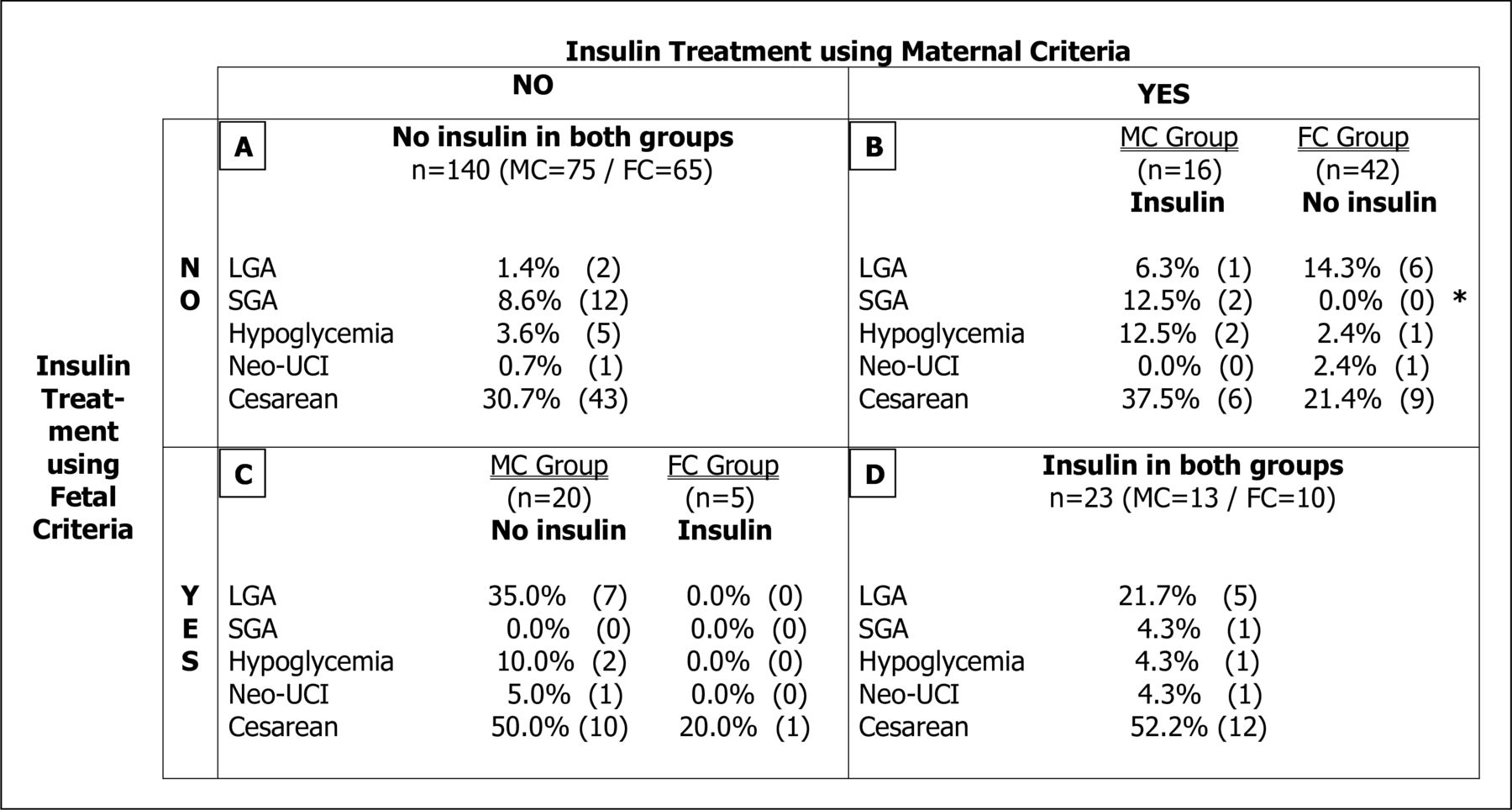
In the cross analysis, each pregnant woman was reassessed using the criteria of the opposite group to that in which she had been originally included, and it was determined whether or not insulin treatment would have been required in that case. Thus, four sets were obtained (figure 1), in which LGA and SGA newborns were analyzed together with newborn hypoglycemia, admission to the neonatal ICU and cesarean sections, conducted in the same way as Schaefer-Graf et al15 in their study.

{kind=link}
Cross analysis. Group A: no insulin in both groups (AC p<75+fasting capillary glycemia/glycemia 1 hour postprandial <95/140 mg/dL and AC p≥75+fasting capillary glycemia/glycemia 1 hour postprandial <80/120 mg/dL). Group B: insulin only in MC group (AC p<75+fasting capillary glycemia/glycemia 1 hour postprandial ≥95/140 but<120/180 mg/dL). Group C: insulin only in FC group (AC p≥75+fasting capillary glycemia/glycemia 1 hour postprandial ≥80/120 but <95/140 mg/dL). Group D: insulin in both groups (AC p≥75+fasting capillary glycemia/glycemia 1 hour postprandial ≥95/140 mg/dL and AC p<75+fasting capillary glycemia/glycemia 1 hour postprandial ≥120/180 mg/dL). *P=0.025. FC, fetal criteria; LGA, MC, maternal criteria; SGA, small for gestational age.
In sets A and D, the pregnant women would have received the same treatment in both cases (64%): in set A, without insulin and in set D, with insulin. In sets B and C, the pregnant women would have received a different treatment in the opposite group. In group B, pregnant women who would be treated with insulin using only the MC, all SGAs were in the MC group (12.5%) (p=0.02) and hypoglycemia was also more frequent in this group (12.5% vs 2.4%) (p=0.120). In the C set, pregnant women who would be treated with insulin only by FC, all the LGA were in the MC group (35%) (p=0.119) and cesarean sections were also more frequent in this group (50% vs 20%) (p=0.226).
Discussion
In this study, the treatment of GDM using FC reduces by almost half (48%) the number of pregnant women who require insulin treatment. Similar studies describe increased insulinization (>50%) in ultrasound-guided treatment groups.15 16 This difference could be due to the fact that these studies present a percentage of pregnant women with AC p of ≥75 at the start of the study (38–45%), greater than in ours (14%). The differences in glycemic control, which was better in the FC group, can be explained mainly by the flexibility in the control targets of the FC group, which allows less strict glycemic targets when there are no ultrasound data of excessive fetal growth. It may also be explained, by the greater involvement of the pregnant women in their metabolic control by associating the glycemic control targets with the ultrasound parameters of fetal growth. On the other hand, the different glycemic targets between the two study groups are not accompanied by differences in insulin doses, in the number of maternal hypoglycemias or in weight gain during pregnancy. In fact, the lack of differences in insulin doses between the groups occurred despite stricter glycemic targets in the FC group, as only 2 of the 15 pregnant women treated with insulin in this group were insulinized due to glycemic criteria (fasting capillary glycemia/1 hour postprandial >120/180 mg/dL).
FC-based GDM treatment does not improve neonatal outcomes for LGA and SGA newborns, but it reduces newborn macrosomia by 60%, although this difference does not reach statistical significance. In similar studies, Kjos et al14 and Schaefer-Graf et al15 did not find differences between LGA and SGA newborns. However, Bonomo et al16 described an increase in macrosomia, LGA and SGA newborns in the conventional treatment group, with statistical significance only for macrosomia and LGA newborns. These significant differences could be attributed to the larger size of the flexible treatment group, twice that of the conventional treatment group and the highest frequency of ultrasound controls in the flexible treatment group (every 2 weeks from the start of the study) compared with the conventional treatment group (only two controls were performed, at baseline and at 34 weeks of gestation), and therefore, the ‘study effect’ bias could be avoided. In the other studies, Kjos et al14 and Schaefer-Graf et al,15 ultrasound checks were performed every 4 weeks in both groups, and in the present study, they were performed every 6 or 8 weeks (although in conventional groups they were not used for management). What is more, in the study by Bonomo et al,16 patients were recruited between 24 weeks and 28 weeks of gestation; while in the studies by Kjos et al14 and Schaefer-Graf et al,15 and also in the present one, patients were recruited up to week 34 of gestation. Therefore, the early diagnosis of the high risk of fetal overgrowth has been able to contribute to the better results of this study, as demonstrated by Rossi et al.24
The significant decrease in newborn hypoglycemia in the group treated using FC could be related to the pathophysiological reasoning on which this therapeutic approach is based: fetal hyperinsulinemia. Fetal hyperinsulinemia is responsible for hypoglycemia in the newborns of mothers with diabetes. According to Weiss et al, ‘biochemical diabetic fetopathy’, defined as hypoglycemia and biochemical dysregulation in the newborn, occurs when in the third trimester insulin levels in the AF were >17 μU/mL.12 Other similar studies have found no significant differences in newborn hypoglycemia, perhaps because their sample size was smaller.14 15 Bonomo et al,16 with a size similar to the present study, described a slight increase in hypoglycemia in the conventional treatment group but without reaching statistical significance, which could be due to the difference in the size of their groups.
Although they do not reach statistical significance, it is worth noting the differences between both groups in other complications closely related to diabetic macrosomia, such as shoulder dystocia, brachial plexus injury and clavicle fracture, which could be explained by the difference in the number of newborns with macrosomia and by the difference in the BMI of LGA newborns. The pathophysiological justification would be the same as for hypoglycemia of the newborn: fetal hyperinsulinemia. In this case the ‘somatic diabetic fetopathy’ or newborn LGA, was found only in pregnancies in which insulin concentrations in the AF were >20 μU/mL.12 Similar studies also found no significant differences in childbirth complications or newborns,14 15 not even Bonomo et al16 (although they only registered admission to the neonatal ICU), despite the differences described in LGA newborns and macrosomia.
Cross-analysis of the data shows that the FC-based treatment strategy redistributes the allocation of insulin therapy in 38.84% of pregnant women (47 out of 121):
It avoids insulin treatment in pregnancies with a low risk of fetal overgrowth despite the fact that the glycemic figures would have indicated it according to the MC strategy in 34.71% of cases (42 out of 121). This approach reduces the number of SGAs and neonatal hypoglycemia. Neonatal hypoglycemia is more frequent in newborn SGA, mainly related to low glycogen stores.25
It applies insulin treatment in pregnancies with a high risk of fetal overgrowth despite the fact that the blood glucose figures would not have indicated it according to the MC strategy in 4.13% of cases (5 out of 121). This approach reduces the number of LGA and cesarean sections.
In the study by Schaefer-Graf et al,15 the redistribution of insulin therapy allocation using the fetal growth-based strategy is similar overall, 34% (31 out of 90), but it avoids insulin treatment in only 20% (18 out of 90) and applies it in 14% (13 out of 90). These differences could be due to the higher percentage of pregnant women with AC p of ≥75 at the start of the study, as already mentioned.
The strengths of our study are that it was carried out under the conditions of our daily clinical practice and that of all the health professionals who attended the pregnant women and newborns, only the endocrinologist and the diabetes educator were aware of the study group to which patients belonged. This was necessary to establish the glycemic control objectives, the degree of compliance with these objectives and the need to initiate insulin treatment. This allows us to apply the results obtained to optimize the management of pregnant women with GDM without increasing the number of ultrasound controls or medical visits, and even to reduce them in pregnancies with a low risk of excessive fetal growth and increase them in pregnancies with a high risk, thus optimizing the therapeutic effort. However, for other health systems in which ultrasound checks are not performed on all pregnant women with GDM, this may be a limitation, since it would imply performing at least one ultrasound scan on all pregnant women with GDM to assess the risk of excessive fetal growth according to the fetal abdominal percentile. However, establishing the risk of fetal overgrowth solely on the basis of maternal capillary glycemia controls appears to be insufficient.
Another limitation of the study that could be attributed to its integration in daily clinical practice is the reliability of hospital records in the collection of clinical data during daily activity. Finally, the low prevalence of some perinatal outcomes does not allow us to know whether there really were differences between the two groups, and multicenter studies with a larger sample size would be necessary to evaluate this.
In this regard, the Cochrane group concluded in its 2019 systematic review of fetal biometry to guide medical management of women with GDM, which included the last three studies prior to ours (Kjos et al,14 Schaefer-Graf et al15 and Bonomo et al16), that more research is needed, ideally larger randomized studies, that can report on short-term and long-term maternal and infant outcomes, including outcomes related to resource use.26
Conclusions
Flexible GDM treatment according to the measurement of fetal AC in daily clinical practice: (1) does not improve neonatal outcomes for LGA and SGA newborns but appears to reduce macrosomia in newborns by almost 60%; (2) reduces insulinization needs in 48% of pregnant women; (3) decreases hypoglycemia by 76% in the newborn, without modifying other perinatal outcomes; and (4) does not modify the complications of pregnancy associated with GDM or its treatment.
Therefore, it can be concluded that flexible GDM treatment according to the measurement of fetal AC by ultrasound is safe for the mother and the fetus and leads to a decrease in the number of pregnant women requiring insulin treatment by almost a half, without increasing the number of ultrasound checks or medical visits.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the research and ethics committee of the Hospital Clínico Universitario Virgen de la Arrixaca (2016-4-7-HCUVA). The participants gave informed consent to participate in the study before taking part.
Acknowledgments
We thank all the mothers who have participated in this study, for their selfless collaboration to advance the treatment of GDM. Also to Mª Dolores González Pina and Vicenta Dólera López, diabetes nurse educators at the Unit of Diabetes and Gestation at the Hospital Clínico Universitario Virgen de la Arrixaca, Guadalupe Ruiz Merino, and statistician at the Instituto Murciano de Investigación Biosanitaria, and José Diego Gutierrez Sánchez, pediatrician-neonatologist at the Hospital Clínico Universitario Virgen de la Arrixaca.
References
Footnotes
Contributors Conceptualization, formal analysis and supervision: MF-L, JEB-C and AMH-M. Patient recruitment: MF-L and JMG-B. Data collection and writing (original draft): MF-L. Investigation: MF-L, JEB-C, JMG-B and AMH-M. Writing (review and editing): all authors. MF-L is responsible for the overall content as the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.