Article Text

Abstract
Introduction Adolescents and young adults (AYAs) with type 1 diabetes (T1D) are at risk of suboptimal glycemic control and high acute care utilization. Little is known about the optimal age to transfer people with T1D to adult care, or time gap between completing pediatric care and beginning adult endocrinology care.
Research design and methods This retrospective, longitudinal study examined the transition of AYAs with T1D who received endocrinology care within Duke University Health System. We used linear multivariable or Poisson regression modeling to assess the association of (1) sociodemographic and clinical factors associated with gap in care and age at transfer among AYAs and (2) the impact of gap in care and age at transfer on subsequent glycemic control and acute care utilization.
Results There were 214 subjects included in the analysis (54.2% female, 72.8% white). The median time to transition and age at transition were 8.0 months and 21.5 years old, respectively. The median gap in care was extended by a factor of 3.39 (95% CI=1.25 to 9.22, p=0.02) for those who did not see a mental health provider pre-transfer. Individuals who did not see a diabetes educator in pediatrics had an increase in mean age at transition of 2.62 years (95% CI=0.93 to 4.32, p<0.01). The post-transfer emergency department visit rate was increased for every month increase in gap in care by a relative factor of 1.07 (95% CI=1.03 to 1.11, p<0.01). For every year increase in age at transition, post-transfer hospitalization rate was associated with a reduction of a relative factor of 0.62 (95% CI=0.45 to 0.85, p<0.01) and emergency department visit rate by 0.58 (95% CI=0.45 to 0.76, p<0.01).
Conclusions Most AYAs with T1D have a prolonged gap in care. When designing interventions to improve health outcomes for AYAs transitioning from pediatric to adult-based care, we should aim to minimize gaps in care.
- Adult
- Diabetes Mellitus, Type 1
- Adolescent Medicine
- Health Services Research
Data availability statement
Data are available upon reasonable request. The data that support the findings of this study are available on request from the corresponding author (DS).
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Though determinants of prolonged care gaps have been studied in other chronic conditions, they have not been studied in type 1 diabetes. The optimal age to transfer to adult care and impact of a prolonged gap in care for individuals with type 1 diabetes are not well understood.
WHAT THIS STUDY ADDS
A longer gap in care in type 1 diabetes is associated with more emergency department visits. Transferring to adult care at an older age is associated with less emergency department visits and diabetes-related hospitalization.
Factors associated with prolonged gap in care include absence of mental health provider visit in pediatrics and absence of hyperlipidemia.
Older age at transfer was associated with absence of a visit with a diabetes educator in pediatrics.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Providers should aim to minimize gaps in care when transitioning people with type 1 diabetes to adult care, which may be accomplished by providing greater engagement with the healthcare system.
Further prospective studies are needed to examine the associations of sociodemographic and clinical factors with gap in care and age at transfer, as well as the role different types of providers play in transitioning people with type 1 diabetes from pediatric to adult care.
Introduction
Transition of care is the planned, purposeful movement of adolescents and young adults (AYAs) with chronic conditions from pediatric to adult-oriented healthcare systems.1 Transfer is the event of changing from pediatric healthcare to adult healthcare.2 For AYAs between the age of 18 and 25 years with type 1 diabetes (T1D), the transition period and transferring to adult care present unique challenges and barriers. AYAs are at risk of suboptimal glycemic control, high acute care utilization, and long-term complications.3–5
The goal of pediatric to adult transition is to provide healthcare that is coordinated, uninterrupted and developmentally appropriate.1 In some countries, the age of transfer is standardized, but in the USA, it varies greatly across institutions and regions. Multiple organizations have released position statements emphasizing the importance of effective transition from pediatric to adult care, but the optimal age to transfer to adult care and impact of a prolonged gap in care are not well understood.6–8 In addition, it is unclear what patient-level factors contribute to the age at transfer and time to transfer from pediatric to adult care for people with T1D.
In light of these evidence gaps, this study had two aims. In aim 1, we sought to understand the sociodemographic and clinical factors associated with timing of pediatric to adult transfer of care among AYAs with T1D. In aim 2, we examined the association of gap in care and age at transfer with glycemic control and acute care utilization. The knowledge gained from this study will guide the development of interventions aimed at improving the transition from pediatric to adult care in people with T1D.
Design and methods
After obtaining approval from the Duke Institutional Review Board, a retrospective chart review was performed to examine the transition of AYAs with T1D who received care in the pediatric and adult endocrinology clinics at the Duke University Health System.
Data source and sample
We identified subjects through the electronic health record (EHR) using the Duke Enterprise Data Unified Content Explorer (DEDUCE) research portal, a web-based clinical research query tool providing access to clinical information at Duke. Our inclusion criteria were (1) International Classification of Diseases, Ninth or Tenth Revision (ICD-9 or ICD-10) diagnosis code for T1D, (2) at least two encounters in a Duke pediatric endocrinology clinic at ≥12 years of age and ≥18 years of age at study end date, and (3) at least one encounter in a Duke adult endocrinology clinic between 2000 and 2019. We excluded participants who took longer than 36 months to transition because we considered this to be a lapse in care.
Filters using the inclusion criteria were sequentially applied to identify the study sample. A data technician from the DEDUCE team assisted in the data extraction to ensure the accuracy of data. The EHR was reviewed to extract data not available in DEDUCE.
Measures
The total period of data collection was from January 1, 2000 through December 31, 2020. Eligibility for study inclusion was assessed between January 1, 2000 and December 31, 2019, with follow-up collected through December 31, 2020. The 1-year period of follow-up captured the acute care utilization of those who transferred at the end of the study period. Timing of transfer variables included: (1) the age at which an AYA had his/her first adult endocrinology clinic appointment; and (2) gap in care defined as time in months from the last pediatric endocrinology clinic visit to the first adult endocrinology clinic visit. Sociodemographic measures included date of birth, gender, race, ethnicity, and last pediatric encounter payor. Medicare is the federal health insurance program for people who are 65 years or older, younger people with disabilities, and people with end-stage renal disease. Medicaid is a state and federal program that provides medical coverage to low-income people. Baseline characteristics also included an ICD-9 or ICD-10 diagnosis code for depression, anxiety, hypertension, hyperlipidemia, or obesity prior to the first adult endocrinology visit. The baseline hemoglobin A1c was the last A1c collected prior to transfer to adult care. A mental health encounter was defined as an outpatient encounter with a psychologist or psychiatrist before transfer to adult endocrinology. Continuous glucose monitor use, insulin pump use, visit with certified diabetes educator, and visit with nutritionist were assessed prior to transfer to adult care. Baseline number of pediatric endocrinology clinic encounters, hospitalization, and emergency department (ED) visits per year were assessed as visits per year during the time from first pediatric endocrinology visit to first adult endocrinology visit. When selecting baseline characteristics, the authors used clinical judgment to select any variables that may impact the timing of transfer.
Outcomes
Timing of transfer variables were the outcomes for aim 1 and the predictors for aim 2. For aim 2, outcomes included acute care utilization during adult care (rates of diabetes-related hospital admissions and ED visits), mean hemoglobin A1c during adult care, and number of endocrinology visits during first year in adult care.
Data analysis
We used SAS statistical software (V.9.4, SAS Institute) to summarize the data and conduct the statistical analysis. Patient characteristics were described using means and SDs, or medians and quartiles for continuous variables and frequencies and percentages for categorical ones. Aim 1 was addressed using multivariable linear regression with timing of transfer to adult-based care variables as the dependent variable (age at transition, and log-transformed months to transition), and patient-level sociodemographic and clinical variables as independent variables. These variables were identified a priori by clinical investigators as potentially related to timing of transfer to adult care. Aim 2 was addressed using multivariable regression modeling. Poisson loglinear modeling was used to model rates of hospitalization and ED visits, normalizing for length of follow-up in adult care. Similar analysis was used for number of endocrinology visits during the first year of adult care. Linear regression modeling was used for log-transformed mean hemoglobin A1c during adult care. Timing of transfer to adult-based care was the main predictor variable, and sociodemographic and clinical variables (diabetes educator, presence of continuous glucose monitor, presence of insulin pump, hypertension, mental health diagnosis, gender, and pre-transfer A1c level) were used as adjustment covariates. All statistical tests were two sided, point estimates from models were reported with nominal 95% CIs, statistical significance was determined at p<0.05, and no adjustment was made for multiple hypothesis testing.
Results
Baseline characteristics
There were 1114 individuals who had two pediatric encounters in our health system at age ≥12 years and were at least 18 years old at the study end date, and 214 subjects who transitioned to adult endocrinology care at Duke within 36 months (figure 1). The population who transitioned (table 1) was 54.2% female (n=116) and 72.8% white (n=155). The mean hemoglobin A1c at the last pediatric encounter was 8.7%±2.1. The median number of months to transition from pediatric to adult endocrine care (gap in care) was 8.0 (Q1–Q3 3.5–15.1). The median age at transfer was 21.5 years old (Q1–Q3 19.9–23.1). There were 14.5% of subjects with a diagnosis of depression and 4.2% with a diagnosis of anxiety.
Baseline characteristics of subjects who transitioned to adult endocrinology clinic
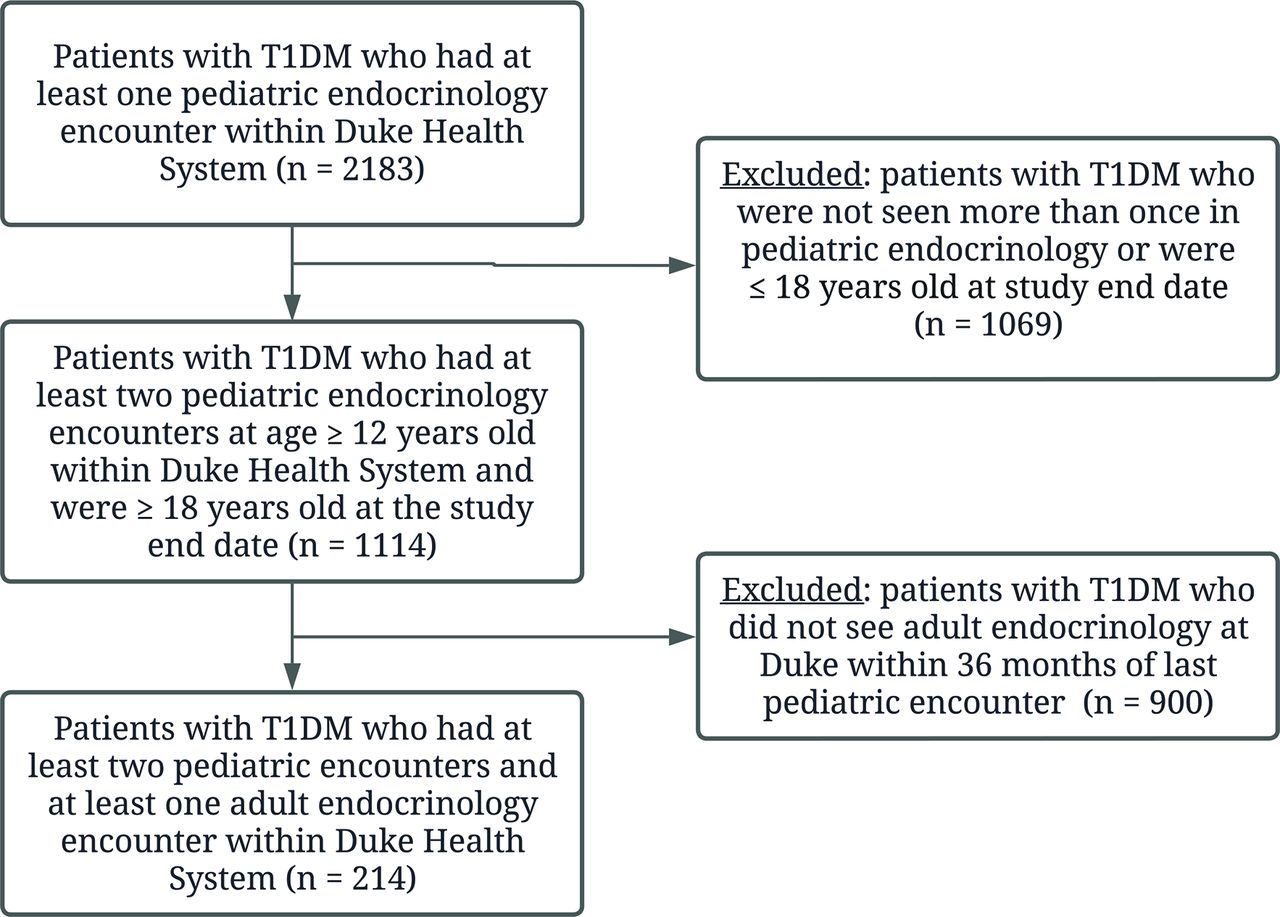
Study flow chart. T1DM, type 1 diabetes mellitus.
For those who did not transition to adult endocrinology at Duke within 36 months (n=900), the baseline characteristics were similar with 47.3% female, 71.5% white, and 91.4% Medicaid. Among the 900 patients who did not transition to adult endocrinology care within 36 months, 104 (11.6%) were seen by adult primary care during follow-up, 396 (44.0%) had at least one adult ED visit or hospital admission during follow-up, and 400 (44.4%) had no adult encounters in the health system during follow-up.
Aim 1: association of baseline characteristics and timing factors
For those who did transition to adult endocrinology, the gap in care and age at transfer were not significantly associated with pre-transfer A1c, pediatric acute care utilization, or pediatric endocrine visits per year (table 2). The duration of the gap in care more than tripled (relative risk 3.39, 95% CI=1.25 to 9.22, p=0.02) for those who did not see a mental health provider pre-transfer and more than doubled (relative risk 2.54, 95% CI=1.08 to 5.97, p=0.03) for those without hyperlipidemia.
Association of selected predictors on time to transition in months
For individuals who did not see a certified diabetes educator in pediatrics, there was an increase in age at transfer of 2.62 years (95% CI=0.93 to 4.32, p<0.01) (table 3). For people with no obesity, there was a decrease in age at transfer of 1.82 years (95% CI=−3.62 to –0.02, p=0.047).
Association of selected predictors on age at transfer in years
Aim 2: association of timing factors with healthcare utilization and hemoglobin A1c in adult care
There was no clinically significant association between timing factors (gap in care in months and age at transition) and number of endocrine clinic visits in the first year of adult care or mean hemoglobin A1c in adult care (figure 2). After adjusting for covariates, the rate of hospitalization was reduced for every year increase in age at transition by a relative factor of 0.62 (95% CI=0.45 to 0.85, p<0.01). In other words, the rate of hospitalization if a patient transferred to adult care at age 22 years was 62% of the hospitalization rate if a patient transferred at age 21 years. The rate of ED visits was reduced for every year increase in age at transfer by a relative factor of 0.58 (95% CI=0.45 to 0.76, p<0.01). The rate of ED visits was increased for every month increase in gap in care by a relative factor of 1.07 (95% CI=1.03 to 1.11, p<0.01).

{kind=link}
{kind=link}
Association of timing factors and outcomes in adult care. ED, emergency department; HbA1c, hemoglobin A1c.
Discussion
It is important to provide developmentally appropriate and uninterrupted healthcare to people with T1D. To design effective interventions that minimize healthcare gaps, we aimed to gain a better understanding of the factors associated with gap in care and age at transfer. Our findings suggest there is often a long gap in care when people with T1D transfer from pediatric to adult endocrinology, with the median time to transfer from pediatric to adult care found to be 8 months. Factors that were associated with an increased gap in care include the absence of a mental health encounter in pediatrics and the absence of hyperlipidemia. The median age at the first adult endocrinology encounter was 21.5 years. The absence of a certified diabetes educator visit in pediatrics was associated with transferring to adult care at an older age. Though there was no association between gap in care in months and age at transfer and hemoglobin A1c in adult care, transferring to adult care at an older age and having a shorter gap in care were associated with lower rates of ED visits. Transferring to adult care at an older age was also associated with a lower rate of hospitalization.
People with chronic conditions frequently experience a lapse in care or prolonged gap in care. Various definitions have been used to define care gaps, and we chose to define gap in care as the time from the last pediatric visit to the first adult visit, similar to the definition used by Wisk et al.9 10 It is unclear if the factors associated with a shorter gap in care (mental health encounter in pediatrics and presence of hyperlipidemia) are related to patient characteristics or the transition process. Those who see a mental health provider may be more proactive in their care, or this may be a marker of greater engagement with the healthcare system. Alternatively, referrals to mental health providers and a diagnosis of hyperlipidemia may be indicators of better quality of healthcare. Our findings suggest that a visit with a mental health professional prior to transfer may be beneficial to patients, and providers should consider a mental health consultation as deemed appropriate. This is consistent with the American Diabetes Association recommendation for universal mental health screening for people with diabetes.11 In a study of people with complex congenital heart defects, individuals with at least one comorbid condition were more likely to transfer successfully.12 Like other studies of chronic conditions, ethnicity and type of healthcare insurance were not found to be associated with gap in care.13 About 87% of the individuals had Medicaid, so the study may not have been able to detect a difference between different insurance types. In countries where there is universal healthcare at all ages, AYAs still experience adverse diabetes-related outcomes around transition.14 Although there are no clear recommendations for the optimal length for the gap in care from pediatric to adult endocrinology, our findings suggest that a longer gap in care is associated with a slightly higher rate of ED visits and is less than the 3 months that is typically needed for ongoing diabetes care. Providers should aim to minimize gaps in care from pediatric to adult-based care for AYAs who are at risk of high acute care utilization and poor outcomes.
Like previous studies, we found that age at transfer was not significantly associated with gap in care or glycemic control. Garvey et al found that those with three or more pediatric diabetes visits in the year before transition were significantly less likely to report a gap >6 months between pediatric and adult care, but our study did not find an association between the number of outpatient pediatric visits and gap in care.15 Our study found that seeing a certified diabetes educator in pediatrics was associated with a decrease in the age at transfer. The clinical significance of this is unclear, but perhaps diabetes educators may potentially play a role in facilitating the transfer to adult care at a younger age. Future studies should evaluate the role that different types of providers have on the transition from pediatric to adult care.
For individuals with chronic conditions, older age at transfer has been associated with improved health service use, clinical outcomes, and patient satisfaction.16 We found that for people with T1D, transitioning at an older age was not significantly associated with hemoglobin A1c but it was associated with a lower rate of hospitalization and ED visits. It has been reported that older people with chronic illnesses have greater self-management skills and transition readiness.17 The data appear to be mixed, however, as Helgeson et al found that individuals with T1D who transferred to adult care at an older age had worse glycemic control.18 In a study of 1299 people who were diagnosed as having T1D as children, remaining in pediatric care until the age of 30 years old did not impact survival.19 This study was conducted in Japan thus its findings may not be applicable to the population in the USA, and it did not include individual factors such as glycemic control and complications. Our study was not powered to evaluate the association with mortality. Overall, this study suggests that continuing pediatric endocrinology care for youth into their early 20s may lead to better outcomes, though the specific age is not clear. Providers should continue to make decisions regarding the transfer from pediatric to adult care on an individual basis.
Differences in how pediatric healthcare is delivered versus adult care may also play a role in the challenges of successful transition. In pediatrics, care is monitored by parents and healthcare providers with integrated support services. Adult care requires patients to take more initiative and seek support services when needed. It is important for providers to consider the developmental maturity of individuals with diabetes when transitioning them to adult care.6 Using registries to monitor the care transition, such as those provided by Got Transition, is a way to monitor transfer and allow the healthcare team to identify people who do not make the transfer within 3 or 4 months. This identification of youth with T1D who are beginning to have extended gaps in care can lead to targeted outreach or coaching to decrease the gap.20 More research is needed to determine the clinical significance of a prolonged gap in care and age at transfer and the role that mental health providers and certified diabetes educators play in the transition process.
This study has a few limitations. The observational design of the study allows us to report associations, but limits conclusions about causality. Healthcare transition is a complex process involving many individual, clinical, and social factors. We cannot exclude the possibility that some of the findings may be false positives. The goals of the analyses were exploratory and therefore we did not control type I error across all the comparisons made. Our study was limited to one health center with a predominantly white population, which may affect generalizability to other health centers and populations. This was a small study of 214 individuals and regression models included ~20 covariates. Although this satisfies the rule of thumb of ≥10 observations per covariate, results may not reproduce in an independent study. Given the retrospective nature of the study and limitations of our EHRs, we were unable to evaluate outcomes for those who did not transition. We evaluated people who transitioned to adult endocrine care in our health system and were unable to collect data on those people who transitioned to adult endocrine care in another health system or were lost to follow-up. Similarly, we were not able to see if people were engaged in mental health services outside of the Duke system. We may have also missed hospitalization and ED visits in other healthcare systems that were not identified through our EHRs. We were unable to collect data on socioeconomic status at the time of transfer, though insurance status may serve as an indicator of socioeconomic status. In addition, given that we evaluated the transition of care over many years, there are changes in the healthcare system, such as mechanisms of delivery and approach towards transition, which we could not account for in our analysis. Despite these limitations, this study meaningfully adds to the dearth of literature on healthcare transition for youth with T1D by shining light on important factors that may be related to successful transition.
Conclusion
This study found that younger age and a longer gap in care when transferring from pediatric to adult care are associated with an increase in acute care utilization. Prospective, multicenter studies are needed to understand the relationship among healthcare gaps, age at transfer, individual and clinical factors. The findings from this study will help guide the development of prospective studies. When designing interventions for AYAs with T1D, we should aim to minimize gaps in care and facilitate a smooth transition to adult care.
Data availability statement
Data are available upon reasonable request. The data that support the findings of this study are available on request from the corresponding author (DS).
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Duke IRB (Pro00105350). No consent was obtained as this was a retrospective study to gather quantitative data. No investigation was planned that would influence patient treatment or outcome.
References
Footnotes
Contributors DS, MJC, AM, and GM conceived the study. DS collected the data. AR and KC analyzed the data. DS drafted and revised the manuscript. All authors reviewed and provided critical comments on all drafts. DS is responsible for the overall content as the guarantor. All authors read and approved the final version of the manuscript.
Funding This study was supported by a grant from the Endocrine Fellows Foundation and National Institutes of Health (T32DK007012). The authors also acknowledge support from the Duke Department of Pediatrics and Duke Division of Endocrinology, Diabetes and Metabolism.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.