Article Text

Abstract
Introduction Imeglimin is a novel anti-hyperglycemic drug that improves both insulin resistance and insulin secretion. The effects of imeglimin on glycemic control were confirmed in phase III clinical trials, but little is known about its effectiveness in daily clinical practice settings, especially compared with metformin. Therefore, we aim to clarify the efficacy of imeglimin in patients with type 2 diabetes (T2D) being treated with a dipeptidyl peptidase-4 (DPP-4) inhibitor plus low-dose metformin.
Research design and methods This is a multicenter, randomized, prospective, open-label, parallel-group trial. Seventy participants with T2D treated with a DPP-4 inhibitor plus metformin (500–1000 mg/day) for more than 12 weeks and a glycated hemoglobin (HbA1c) level of 52–85 mmol/mol (7.0%–9.9%) will be randomized to receive add-on imeglimin 1000 mg two times per day or metformin dose escalation for 24 weeks. Biochemical analyses and physical assessments will be performed at baseline and at the end of the study, and adverse events will be recorded. The primary endpoint is the change in HbA1c after 24 weeks. The secondary endpoints comprise the changes in blood pressure, pulse rate, body weight, abdominal circumference, and other laboratory parameters; the relationship between improvements of biological parameters including glycemic control and patient background characteristics; and side effects.
Results This study will reveal new insights into the incorporation of imeglimin into the diabetes treatment strategy.
Conclusions This will be the first randomized controlled trial to compare the efficacy of adding imeglimin versus metformin dose escalation on glycemic control in patients with T2D.
Trial registration number jRCT1011220005.
- Metformin
- Dipeptidyl Peptidase 4
- Diabetes Mellitus, Type 2
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic
Imeglimin is a novel oral antidiabetic drug that improves both insulin secretion and insulin resistance.
A phase III trial revealed an additional anti-hyperglycemic action on other oral antidiabetic agents.
What this study adds
It is under whether imeglimin administration provides a better effect than metformin dose escalation following pretreatment with a dipeptidyl peptidase-4 inhibitor plus metformin.
The study will be conducted in a real-world setting at six medical centers, and this study design will include broad eligibility criteria.
How this study might affect research, practice or policy
The results of this study will reveal new insights into the incorporation of imeglimin into the diabetes treatment strategy.
Introduction
Both progressive impairment of insulin secretion and worsening insulin resistance have been described as features of diabetes.1–3 Conversely, one of the goals in the management of diabetes is reducing mortality by preventing macrovascular and microvascular complications.4 To achieve this, comprehensive management of metabolic conditions including obesity, hyperglycemia, dyslipidemia, and hypertension is required.5 6 Therefore, treatment strategies that improve both insulin secretion and insulin resistance without causing undesirable effects are required.
Metformin has long been an essential medical agent for type 2 diabetes (T2D)7 8 because of its safety and efficacy, especially concerning mortality and cardiovascular events.9 10 Recently, glucagon-like peptide-1 (GLP-1) receptor agonists and sodium glucose cotransporter 2 (SGLT2) inhibitors were demonstrated to potently reduce the risk of cardiovascular events in several cardiovascular outcomes trials11; however, it is noteworthy that most participants in such trials received metformin as the baseline treatment.11 Meanwhile, dipeptidyl peptidase-4 (DPP-4) inhibitors, which increase endogenous incretin levels and exert hypoglycemic effects in a glucose level-dependent manner, are widely used in Japan based on their safety pharmacological actions and potent effect on glycemic control in the Asian population.12 A recent investigation revealed that both metformin and DPP-4 inhibitors are frequently prescribed as oral antidiabetic drugs in Japan.13 However, treatment strategies to achieve better glycemic management in patients taking these two medications have not been elucidated.
Recently, imeglimin, a first-in-class anti-hyperglycemic agent that improves both insulin secretion and insulin resistance received its first approval for use in T2D in Japan. It has a similar structure as metformin14; however, the risk of lactic acidosis is lower than metformin.15 Imeglimin improves both insulin resistance and insulin secretion via multiple molecular mechanisms, namely, inhibition of complex I and correction of deficient complex III activity followed by reducing reactive oxygen species levels, incrementally increasing ATP generation in beta-cells, and increasing nicotinamide phosphoribosyl transferase and NAD+ levels.14 16 17 The effects of imeglimin on glycemic control were confirmed in several phase III trials,18–20 but little is known about its efficacy in standard clinical practice settings. In addition, it is unclear whether imeglimin administration is superior to a doubling of the metformin dose with respect to glycemic control in patients who were treated with combination therapy of a DPP-4 inhibitor plus metformin. In this multicenter, randomized, prospective, open-labeled parallel-group trial, we aim to verify the efficacy of imeglimin compared with metformin dose escalation in patients with T2D who were treated with a combination of DPP-4 inhibitor plus low-dose metformin.
Research design and methods
Study design
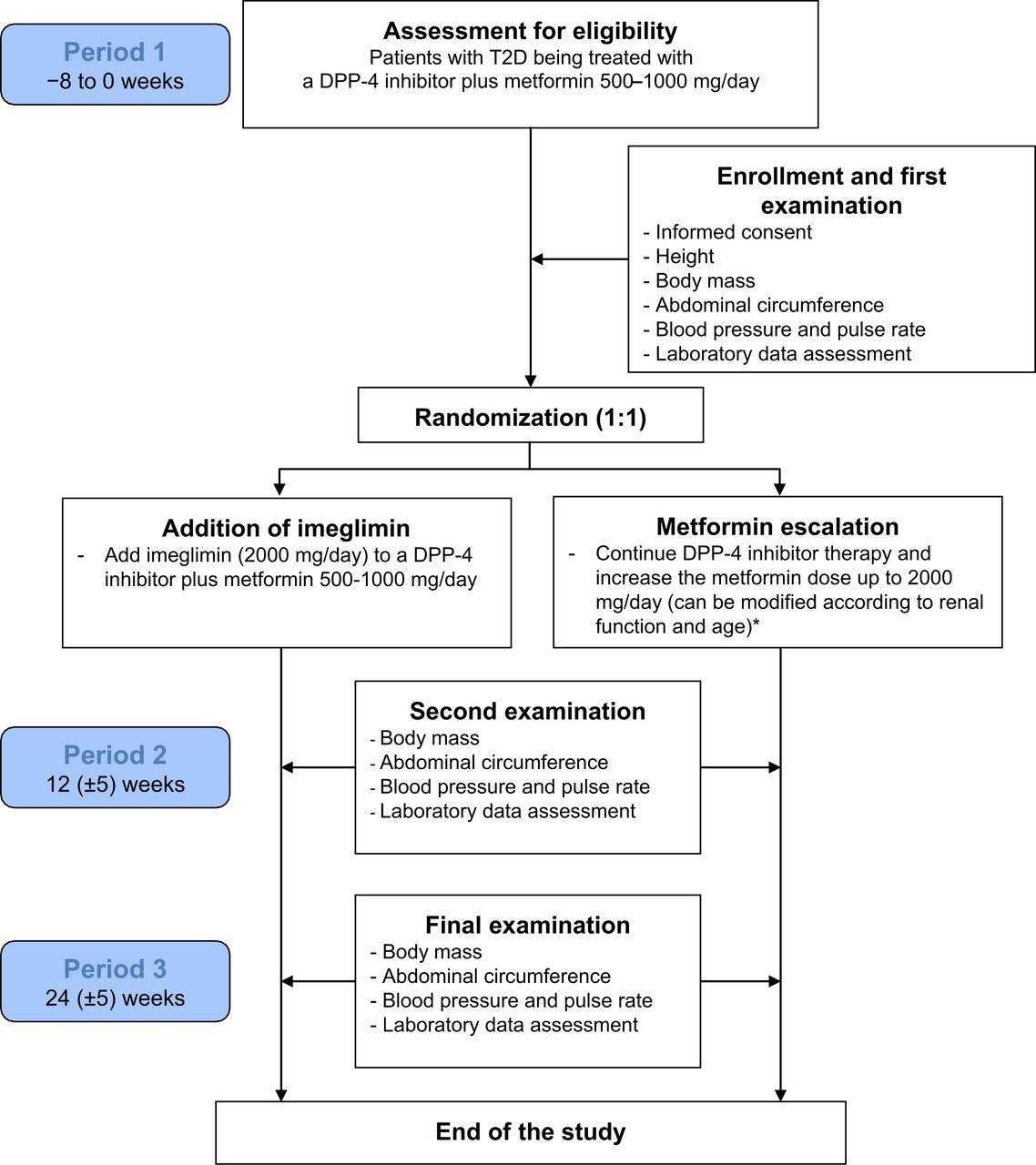
The MEGMI study is a multicenter, open-label prospective, randomized, parallel-group comparison study aiming to demonstrate the superiority of imeglimin over metformin dose escalation in patients with T2D who previously treated with the combination of a DPP-4 inhibitor plus low-dose metformin. After enrolment with written informed consent, the participants will undergo physical examination including clinic blood pressure, pulse rate, body weight, and abdominal circumference, and will provide urine and serum samples, including measurements of lactate acid and vitamin B12 levels, to obtain baseline data. As shown in figure 1, serum and urine metabolic parameters, physical examination will be repeatedly measured at each study visit. During period 1 (−8 to 0 weeks), all participants will be randomly assigned at a 1:1 ratio to receive add-on imeglimin or metformin dose escalation up to 2000 mg/day according to the baseline characteristics such as age, body mass index, and glycated hemoglobin (HbA1c) level.21 Web-based automated system that is independent of the participating sites (NorthNet; https://www.crmic-huhp.jp/northnet/edc/) will be used for randomization and allocation of the participants, as described previously.21 The glycemic target for each patient will be determined based on the recommendations of the Japan Diabetes Society (JDS).22

{kind=link}
Patient recruitment scheme. Participants will be randomly assigned to add-on imeglimin 2000 mg/day or metformin dose escalation to 1000–2000 mg/day (doubling of the current metformin dose; *restricted to 1500 mg/day in patients with eGFR=45–60 mL/min/1.73 m2 and/or those ≥75 years old; in case of a starting dose of 1000 mg/day, the dose will be increased to 1500 mg/day at least for 4 weeks followed by 2000 mg/day if tolerable). All participants will undergo physical and biochemical examinations at baseline and at the end of the study. DPP-4, dipeptidyl peptidase-4 inhibitor; eGFR, estimated glomerular filtration rate; T2D, type 2 diabetes.
Inclusion and exclusion criteria
Boxes 1 and 2 show the inclusion and exclusion criteria. Briefly, Japanese adult (20–89 years) patients with T2D who have been treated with the combination of a DPP-4 inhibitor plus metformin 500–1000 mg/day for at least 12 weeks before enrolment, although with HbA1c levels of 52–85 mmol/mol (7.0%–9.9%) will be enrolled (box 1).
Inclusion criteria
Japanese patients with T2D
Age of 20–89 years
HbA1c=52–85 mmol/mol (7.0%–9.9%)
Treatment with a DPP-4 inhibitor plus metformin (500–1000 mg/day) for at least 12 weeks before enrolment
DPP-4, dipeptidyl peptidase-4; HbA1c, glycated hemoglobin; T2D, type 2 diabetes.
Exclusion criteria
Allergy to imeglimin
Unsuitable for metformin dose escalation
Unstable diabetic retinopathy
Current severe liver dysfunction or nephropathy (eGFR <45 mL/min/1.73 m2)
Pregnancy
Severe ketosis
Diabetic coma or pre-coma
Severe infection, trauma, and/or recent or planned surgery
Low drug compliance rate
Inability to consume an appropriate diet
Incompatibility with the trial for other reasons as determined by the physician
eGFR, estimated glomerular filtration rate.
As summarized in box 2, patients who will not be suitable for adding imeglimin or metformin will be excluded, such as severe renal dysfunction (estimated glomerular filtration rate (eGFR) <45 mL/min/1.73 m2), severe infection and planned surgery.
Study arm and treatment strategy
In the imeglimin arm, imeglimin will be initiated at 1000 mg two times per day, and no dose adjustment will be performed during the study period because only a dose of 2000 mg/day is approved in Japan. In the metformin escalation arm, patients will undergo metformin dose escalation (eg, increased from 500 to 1000 mg/day or from 750 to 1500 mg/day). In patients who were treated with metformin at 1000 mg/day, the dose will be increased to 1500 mg/day for at least 4 weeks followed by 2000 mg/day to minimize the risk of gastrointestinal disorders. The maximum dose of metformin will be restricted to 1500 mg/day in patients with mild renal dysfunction (eGFR=45–60 mL/min/1.73 m2) and/or in older patients (≥75 years old) based on both the recommendation on safe use of metformin from the JDS and the package insert of metformin. In patients with gastrointestinal disorders, metformin therapy can be temporarily interrupted and/or adjusted. The treatments including diet and exercise regimens will be supervised for 24 weeks at the appropriate medical care center during the study. To avoid hypoglycemia, anti-hyperglycemic agents which cause hypoglycemia such as sulphonylureas, glinides, and insulin can be adjusted according to the recommendations of the JDS.22 The doses of other anti-hyperglycemic drugs as well as concomitant treatments will not be adjusted during the study period. If appropriate glycemic control is not achieved and/or worsening occurs despite suitable lifestyle interventions, dose adjustment or the addition of anti-hyperglycemic drugs will be considered.
Sample selection
Written informed consent from all eligible participants will be obtained from the physicians in the research team. The eligibility criteria are described above. The Research Committee has approved the written material, consisting of a participant information leaflet and consent documentation. The participants will be able to ask questions regarding the trial freely, and there will be an opportunity to withdraw their consent at any time during the study period. Similar to our previous trial,21 patients will be withdrawn from the trial for any of the reasons summarized in box 3. Participant enrolment will occur between 11 May 2022 and 31 December 2024 at six medical centers and clinics located in Sapporo, Japan.
Withdrawal criteria
Withdrawal of consent
Decision of the physician based on the patient’s condition
Discontinuation of the study
Decision of the physician for any other reason
Primary and secondary endpoints
The primary endpoint of the study is the change in HbA1c from baseline to week 24. The secondary endpoints are as follows: (1) the mean changes in physical examination findings such as body weight, abdominal circumference, blood pressure and pulse rate; (2) the mean changes in laboratory parameters indicative of glucose and lipid metabolism and liver and renal function; (3) the relationship between improvements of metabolic parameters including HbA1c and patient background; and (4) side effects. The changes of these primary and secondary endpoints will be compared between the imeglimin and metformin escalation groups. The frequency of hypoglycemia (symptomatic hypoglycemic events or blood glucose levels less than 70 mg/dL) will be recorded. A time-course sheet for each study visit will be prepared to minimize the risk of participant withdrawal as described previously.21
Sample size calculation
The sample size was calculated based on the assumption that imeglimin 2000 mg/day addition to a DPP-4 inhibitor will improve HbA1c levels by at least 0.92±0.87% as demonstrated in a phase III trial.19 Conversely, doubling of the metformin dose will reduce HbA1c levels by 0.40±0.47% based on our previous randomized controlled trial.23 It was determined that 30 patients per arm is needed to achieve a power of at least 80% for detecting the superiority of imeglimin over metformin dose escalation. Based on an assumption that five patients (15%) will withdraw from each arm, the target sample size was set at 35 individuals per group. The significance level will be set at 0.05 and two-sided tests will be performed. To ensure that sufficient participants of various background are enrolled, the study will be conducted at six medical centers in Sapporo city.
Data analysis
Analysis of data for the primary and secondary endpoints will be principally performed using the full analysis set as described previously.21 This analysis will exclude the data from the patients who do not meet the inclusion criteria, those with insufficient primary endpoint data, or those who appreciably deviated from the study protocol. Differences between the two study arms will be analyzed using the Welch t-test or Mann-Whitney U test for continuous variables, and the χ2 test or Fisher’s exact test for categorical variables. The factors correlated with any improvements in glycemic control or other variables in metabolic factors will be explored using analysis of covariance and multivariate analysis. The data will be analyzed using JMP Pro (SAS Institute), BellCurve for Excel (Social Survey Research Information, Japan), and GraphPad Prism (GraphPad Software, San Diego, California, USA).
Ethics approval
The MEGMI study was registered with the Japan Registry of Clinical Trials (jRCT1011220005) before enrolment. The study will be carried out in accordance with the principles of the Declaration of Helsinki and its amendments.
Data protection and management
The researchers will perform data management such as cleaning, coding, storage, and security throughout the study. The participants will be able to know the outcomes of this trial, and all data related to this study will be kept at Hokkaido University for 5 years. Detailed information regarding the trial will be published in jRCT databases (https://jrct.niph.go.jp/latest-detail/jRCT1011220005). Similar to our previous trials, a monitor who is independent of the investigators will perform monitoring for the first participant at each of the study sites. In addition, fifth participant at Hokkaido University Hospital will be monitored.21 Adverse events and other information, including modifications to the trial, will be disclosed publicly in line with the provisions of the Clinical Trials Act in Japan.
Availability of data and materials
The data generated during this trial will be available on reasonable request.
Discussion
To date, no studies have directly compared the efficacy of imeglimin with respect to glycemic control with other anti-hyperglycemic agents in patients with T2D in a real-world setting. Imeglimin is a first-in-class oral anti-hyperglycemic drug that targets mitochondrial bioenergetics. Mitochondrial dysfunction is reported to be an underlying T2D pathogenesis resulting in both beta-cell dysfunction24 25 and insulin resistance.24 26 Considering that progressive beta-cell dysfunction and loss are common features of diabetic islets1 27 and that insulin resistance occurs under diabetic conditions regardless of obesity,28 targeting both insulin resistance and beta-cell dysfunction via interventions targeting mitochondria represents a promising treatment strategy.
The effects of imeglimin on glycemic control were demonstrated in the TIMES phase III randomized controlled trials conducted in Japan.18–20 Briefly, imeglimin monotherapy for 24 weeks significantly lowered HbA1c levels by 0.87% versus placebo, and its efficacy as add-on therapy was also confirmed. However, such efficacy has not been confirmed in real-world settings. Additionally, the effects of add-on imeglimin therapy on HbA1c differed according to the baseline therapy in the TIMES2 trial (from 0.12% with GLP-1 receptor agonists to 0.92% with DPP-4 inhibitors).19 Therefore, the efficacy of imeglimin should be confirmed in patents taking more complicated antidiabetes therapies. Recent Japanese cohort data obtained from an administrative claims database also illustrated that the most frequently administrated antidiabetic agents were DPP-4 inhibitors followed by metformin, and the initial dose of metformin was 500 mg or less in 72.9% of metformin-naïve patients.29 In this situation, it would be plausible to consider two treatment options for patients in whom appropriate glycemic control is not achieved even with the combination of a DPP-4 inhibitor plus metformin, namely, the addition of a suitable antidiabetic agent and metformin escalation up to the effective dose.
Metformin administration is known to be related to vitamin B12 deficiency and lactic acid accumulation, which can lead to lactic acidosis in some cases.30 Both of these adverse events are believed to be uncommon for imeglimin treatment. In the TIMES2 trial, the incidence of gastrointestinal disorders related to imeglimin treatment was higher in patients being treated with metformin than in those receiving other anti-hyperglycemic drugs.19 In addition, metformin dose escalation can also lead to gastrointestinal complaints. Considering that both treatment regimens in this trial can induce bowel symptoms, resulting in dehydration and/or renal dysfunction, careful monitoring is required. Therefore, we will investigate relevant serum markers and symptoms in the safety analysis. This information will also be useful for safe use of the sue in daily practice. Owing to the broad inclusion criteria, extremely old patients can be recruited into this trial. Although the benefits or risks of metformin in extremely old patients with diabetes have not been verified,31 such patients are more likely to become ill. There is a certain risk of withdrawal based on physicians’ decisions in both arms for these reasons. However, our research team consists of well-trained diabetologists, and we will attempt to enroll patients without frailty under the aforementioned inclusion and exclusion criteria.
In conclusion, the present study will be the first randomized controlled trial to investigate the efficacy of add-on imeglimin compared with metformin dose escalation concerning glycemic control in patients with T2D who were treated with a DPP-4 inhibitor plus low-dose metformin in a real-world clinical setting. The results are expected to reveal new insights into the use of imeglimin in treatment strategies for patients with T2D.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The institutional review board of Hokkaido University reviewed and approved the study protocol (approved no. 021-008), and written consent will be obtained from all participants. The study has been registered in the Japan Registry of Clinical Trials under the identifier jRCT1011220005. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We thank the participants in the study.
References
Footnotes
Contributors HN and HM designed the original study protocol. AN, AM, HK and KYC modified the study design. HN wrote the manuscript, and all other named authors contributed to its revision. All authors will contribute to participant enrolment. KYC will collect and analyze the data. HN will take responsibility for the integrity of the data and the accuracy of the data analysis, and this author is the guarantor of this work. All named authors meet the International Committee of Medical Journal Editors criteria for the authorship of this article. They take responsibility for the integrity of the work as a whole and give their approval for this version of the manuscript to be published.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests AN has obtained research support from Taisho Pharmaceutical Co., Ltd., Kissei Pharmaceutical Co., Ltd., Nippon Boehringer Ingelheim Co., and Mitsubishi Tanabe Pharma. KYC has obtained speaking fees from Eli Lilly Japan K.K. HM has received honoraria for lectures from Astellas Pharma Inc., Sumitomo Pharma Co., Ltd., Eli Lilly Japan K.K., Mitsubishi Tanabe Pharma Co., MSD K.K., Novo Nordisk Pharma Ltd., Sanofi, Nippon Boehringer Ingelheim Co., Kowa Pharmaceutical Co., Ltd., and Ono Pharmaceutical Co., Ltd.; and has received research funding from Novo Nordisk Pharma, Astellas Pharma Inc., Sumitomo Pharma Co., Ltd., Daiichi Sankyo Co., Mitsubishi Tanabe Pharma Co., Kowa Pharmaceutical Co., Ltd., Abbott Japan Co., Taisho Pharmaceutical Co., Ltd., Nippon Boehringer Ingelheim Co., LifeScan Japan Inc., and Ono Pharmaceutical Co., Ltd. TA has obtained research grants from Ono Pharmaceutical Co., Ltd., Pfizer Inc., Astellas Pharma Inc., Chugai Pharmaceutical Co., Ltd., Takeda Pharmaceutical Co., Ltd., Daiichi Sankyo Co. Ltd., Mitsubishi Tanabe Pharma Co., Otsuka Pharmaceutical Co., Ltd., Teijin Pharma Ltd., and Alexion Inc.; speaking fees from Kyowa Kirin Co., Ltd., Mitsubishi Tanabe Pharma Co., Eli Lilly Japan K.K., Chugai Pharmaceutical Co., Ltd., Novartis Pharma K.K., Astellas Pharma Inc., Eli Lilly Japan K.K., Takeda Pharmaceutical Co., Ltd., Eisai Co. Ltd., Pfizer Inc., AbbVie Inc., Bristol-Myers Squibb Co., Daiichi Sankyo Co., Ltd., UCB Japan Co. Ltd., and Taiho Pharmaceutical Co., Ltd.; and fees for consultancies from Novartis Pharma K.K., AstraZeneca plc., Ono Pharmaceutical Co. Ltd., Medical & Biological Laboratories Co., Ltd., AbbVie Inc., Nippon Boehringer Ingelheim Co., Ltd., and Pfizer Inc.
Provenance and peer review Not commissioned; externally peer reviewed.