Article Text

Abstract
Introduction To assess disparities in retesting for glycated hemoglobin (HbA1c) and systolic blood pressure (SBP) among people with diabetes mellitus (DM) and hypertension (HTN), respectively, we analyzed medical records from a lesbian, gay, bisexual, transgender, queer-specialized federally qualified health center with multiple sites in Chicago.
Research design and methods We identified people with DM seen in 2018 and 2019 then assessed if individuals had HbA1c retested the following year (2019 and 2020). We repeated this using SBP for people with HTN. Rates of retesting were compared across gender, sexual orientation, and race and ethnicity and across the 2 years for each categorization with adjustment for socioeconomic indicators.
Results Retesting rates declined from 2019 to 2020 for both HbA1c and SBP overall and across all groups. Cisgender women and transgender men with DM (vs cisgender men) and straight people (vs gay men) had significantly lower odds of HbA1c retesting for both years. There was evidence of widening of HbA1c retesting disparities in 2020 between gay men and other orientations. Cisgender women, straight people, and black people (vs white) with HTN had significantly lower odds of SBP retesting for both years. There was evidence of narrowing in the retesting gap between black and white people with HTN, but this was due to disproportionate increase in no retesting in white people rather than a decline in no retesting among black people with HTN.
Conclusions Disparities in DM and HTN care according to gender, race, ethnicity, and sexual orientation persisted during the pandemic with significant widening according to sexual orientation.
- Glycated Hemoglobin A
- Hypertension
- Gender Identity
- Healthcare Disparities
Data availability statement
Data may be obtained from a third party and are not publicly available. Data are not made open access since it came from electronic health records. Requests for data access can be sent to Howard Brown Health.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Lockdowns due to the COVID-19 pandemic have led to interruptions in delivery of care for people with chronic diseases like diabetes and hypertension. Studies have documented disparities in service utilization but mostly according to binary gender and race and ethnicity; investigation of other social categories is important to help health equity efforts.
WHAT THIS STUDY ADDS
There were disparities in assessments for and achievement of treatment targets for diabetes and hypertension according to race and ethnicity and multicategory gender and sexual orientation. We observed widening of prepandemic disparities in not getting an HbA1c test according to sexual orientation.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
We provide evidence of disparities across multiple axes of identity including based on expansive gender categories and sexual orientation which stresses the need to collect these variables and examine disparities along these categories. More research to examine mechanisms behind these observed disparities is needed to inform tailored approaches to outreach and care.
Introduction
Lockdowns during the COVID-19 pandemic disrupted provision of health services. To reduce COVID-19 exposure, health facilities switched to telehealth consults or applied decision algorithms that resulted in lower in-person visits.1–3 There are some services, however, that necessitate in-person visits, such as measuring glycated hemoglobin (HbA1c) for diabetes mellitus (DM) and systolic blood pressure (SBP) for hypertension (HTN).4 Without regular assessments, tailoring management (eg, stepping up antihypertensive treatment or referral to diabetes case managers) becomes difficult and increases risk for downstream morbidities (eg, renal failure, myocardial infarction). Several studies have demonstrated that lockdowns led to declines in in-person assessments.5 6 These declines in chronic disease management, however, have not impacted all populations equally. Disparities have been found by sex, race, and age.7 8 For example, a study found steeper decline in HbA1c testing volume among female versus male patients and older versus younger patients with diabetes.7
To our knowledge, no studies have assessed how the pandemic affected care of sexual and gender minority individuals with chronic diseases. There are very few prepandemic quantitative studies on DM and HTN care outcomes in lesbian, gay, bisexual, transgender, queer (LGBTQ+) populations. Additionally, most studies used national surveys rather than health system-specific sources.9 10 While national surveys offer representativeness, these sources are limited in terms of doing longitudinal outcomes and can be difficult to use for assessing healthcare utilization. Health system records capture actual care received, could be easier to contextualize, and thus be used for localized interventions, although lose some generalizability.11 12
Before pandemic, LGBTQ+ individuals already faced barriers to accessing regular care due to stigma and discrimination.13–15 Combined with social marginalization, LGBTQ+ populations are likely to be disproportionately affected by the pandemic.13 Many LGBTQ+ have health conditions (eg, heart disease, asthma, HTN) that put them at higher risk of severe COVID-19 which could affect willingness to seek in-person care.16 Lockdowns may have made access to the few health facilities that provide affirming and inclusive care more difficult.13 17 Sexual minority individuals had worse declines in mental health outcomes compared with heterosexual individuals during the early phase of the pandemic.18 Before pandemic, the LGBTQ+ rates of poverty, unemployment and being uninsured were already higher compared with the non-LGBT rates.19 20 These may have worsened due to disproportional job loss in certain industries with high rates of LGBTQ+ employment such as food services, hospitality, and retail.19 21 All these factors affected health seeking and ability to access care.
We aimed to address this knowledge gap by assessing disparities in care for DM and HTN in an LGBTQ+-focused federally qualified health center (FQHC) with multiple sites in Chicago. While the center specializes in LGBTQ+ population, it caters to all regardless of sexual orientation and gender identity (SOGI), including cisgender heterosexual individuals. As an FQHC, it also serves a high number of low-income and/or uninsured individuals. We hypothesize that rate of retesting for HbA1c and SBP differentially declined according to SOGI from 2019 to 2020, leading to widening of disparities between majority and minority groups. We think disparities still occurred due to societal factors outside the influence of an inclusive health system that disproportionately affected healthcare utilization by LGBTQ+ populations.18 19 21 Uncovering these disparities is important to ensure proper action can be taken at all levels, including primary care. Addressing uncovered disparities in DM and HTN care will also contribute to reducing the risk of cardiovascular disease in LGBTQ+ populations.22
Methods
Overview and data source
In this retrospective observational study, we analyzed data from Howard Brown Health, an FQHC specializing in providing primary care to LGBTQ+ populations with several sites in Chicago. Our main outcome is retesting for HbA1c (for people with DM) and SBP (for people with HTN) in 2019 and 2020. As this was an analysis of electronic health records (EHR) data, requirement for informed consent was waived. Analysis was done on deidentified data with measures in place to ensure data security.
Study population
We identified people with DM and HTN from the EHR using a mix of diagnosis codes, laboratory tests, and medication use. People were classified as having DM if they had at least one International Classification of Diseases (ICD) code for DM (ICD-9: 250.x; ICD-10: E10.x, E11.x, E13.x) and had either an HbA1c ≥6.5% or were on an antidiabetic medication. People with HTN were those who had at least two HTN diagnosis codes (ICD-9: 405, 401; ICD-10: I10, I15) within a 2-year period. For components that were met on separate dates, we use the earlier date as the diagnosis date. All individuals who met the criteria were included. This approach was based on a previously published approach on case identification with EHR data.23
As a facility that has systematically collected SOGI data in their medical records for decades, variables on SOGI and race and ethnicity were derived from structured fields embedded in the patient intake forms and the EHR.
Outcome assessment
To calculate retesting rate per year, we first identified individuals who were diagnosed with DM (new or returning) and had at least one HbA1c test the year before the observation year. After this, we assessed if these individuals received at least one HbA1c test during the observation year. For example, for 2019 retesting of HbA1c, we assessed if individuals with DM who were tested for HbA1c (either as part of diagnosis or routine testing) in 2018 received any HbA1c test in 2019. A similar process was done for retesting in 2020 with people with DM and at least one HbA1c in 2019. The same process was applied to calculate SBP retesting for 2019 and 2020 in people with HTN. Those who received a test were further classified based on the achievement of treatment targets (HbA1c ≤9% for DM and SBP <140 mm Hg for HTN). While guidelines for DM and HTN recommend more frequent testing and visits (two to four HbA1c tests for DM and visits every 2 weeks to 6 months for HTN), we used lower requirements since we were more interested in changes in utilization rather than quality of care.24 25
Statistical analysis
To assess for widening of disparities, we used multinomial regression models with an addition of an interaction term between time (2019 or 2020) and a social category (race and ethnicity, gender, sexual orientation). All models were adjusted for age, housing status, poverty status, and insurance status. Due to issues of collinearity, the race and ethnicity model adjusted for gender but not sexual orientation, the gender model adjusted only for race and ethnicity but not sexual orientation, and finally the sexual orientation model adjusted only for race and ethnicity but not gender. For gender in the main analysis, we used an organization-defined four-category variable (cisgender man, cisgender woman, transgender man, transgender woman) based on responses to gender, sex assigned at birth, and use of hormone medications. As a sensitivity analysis, we created a five-category variable with an additional variable for non-binary and genderqueer individuals.
Subgroups with the largest subgroup size were selected as reference categories to produce statistically stable estimates and since it allows more direct comparisons to assess disparities. The largest group often aligned with the historically privileged groups that are least affected by specific systems of oppression driving disparities. For example, cisgender man was the reference category since they were least affected by sexism against women and transphobia.
All analyses were run in R V.4.1/RStudio.26 27 Missing data on covariates (eg, poverty status) were due to missing or ‘refuse to answer’ responses to questions during the patient intake processes. Missing data were addressed using missForest.28
Results
Study population and overall trends
Four groups (2019 DM: 839; 2020 DM: 1060; 2019 HTN: 2891; 2020 HTN: 3749) with similar sociodemographic characteristics were included in the analysis. All groups had an average age of around 50 years. About a third were black and 16%–23% were Hispanic. The majority had permanent housing (~80%) and were insured (~85%). The most common orientations were gay (35%–45%) and straight (30%–40%); around 10%–15% were transgender (table 1). While volume of testing (without consideration of prior testing) in 2019 was stable across months, a drastic decline was observed in 2020 corresponding to the lockdown (figure 1).
Sociodemographic characteristics of eligible people with diabetes and hypertension, Howard Brown Health (2019–2020)

Trends in (A) glycated hemoglobin (HbA1c) testing and (B) systolic blood pressure measurements in Howard Brown Health, 2019–2020. Testing here includes any test regardless of testing in the prior year. For example, people who were newly diagnosed in 2020 were included in the tests done in 2020.
People with diabetes
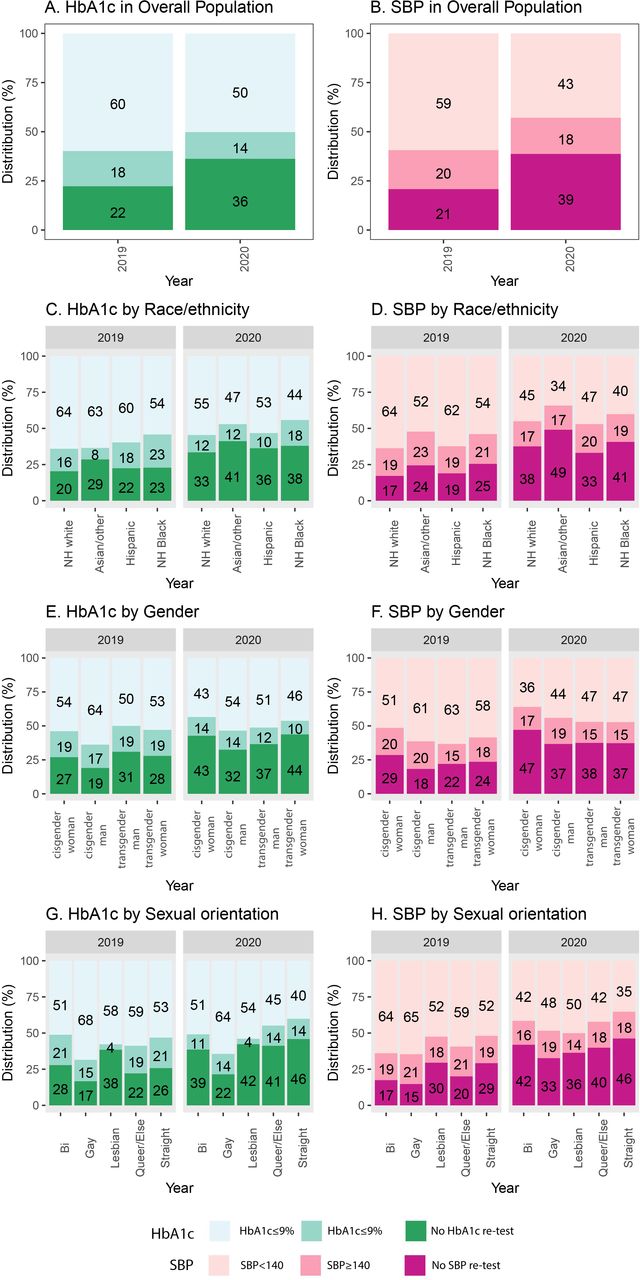
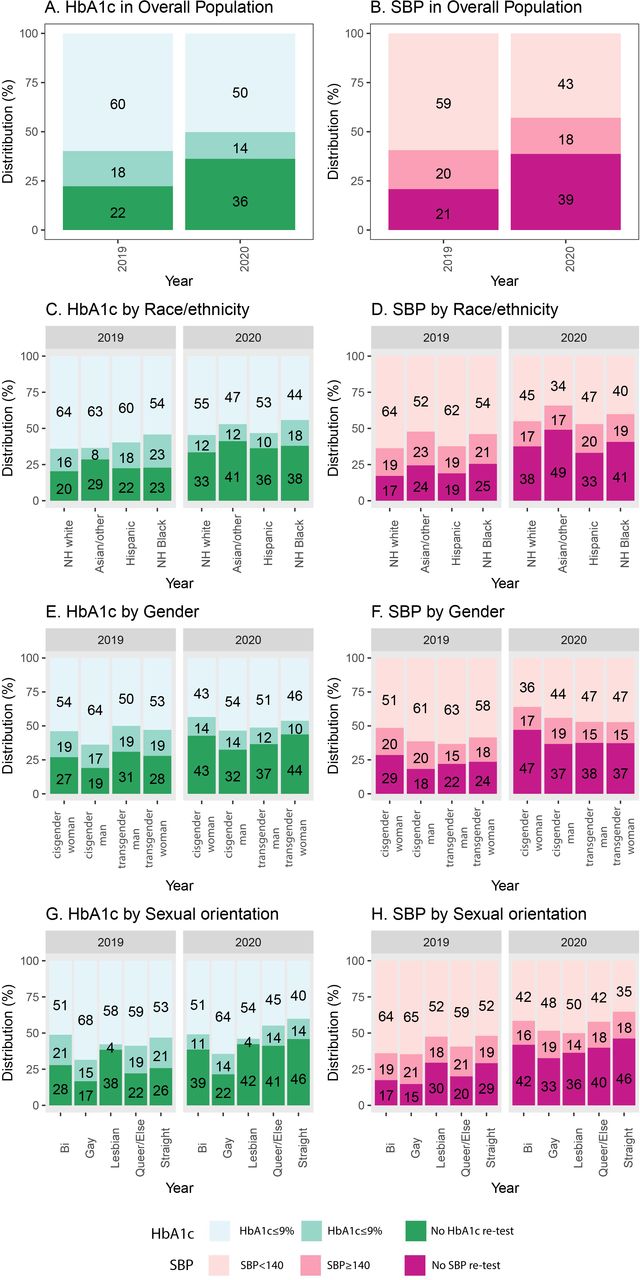
In 2019, 22% did not get retested, 18% got retested, but had HbA1c >9%, and 60% got retested and had HbA1c ≤9%. By 2020, there was a 14-point increase in proportion of not getting retested and a 10-point decline in proportion of having HbA1c ≤9% (figure 2). In unadjusted models, the odds of not retesting HbA1c was significantly higher in 2020 than 2019 (OR 1.94, 95% CI 1.57 to 2.40, p<0.001), but odds of not achieving the HbA1c target was constant (OR 0.90, 95% CI 0.70 to 1.17, p=0.45). This pattern remained even after confounder adjustment (table 2).
Adjusted odds of getting retesting and achieving HbA1c target in people with diabetes mellitus according to different sociodemographic categories
{kind=link}
{kind=link}
Unadjusted rates of the glycated hemoglobin (HbA1c) and systolic blood pressure (SBP) retesting, Howard Brown Health, 2019–2020. Other race and ethnicity include Native American, Pacific Islander, multiracial, declined, and unknown. See table 1 for group sizes for each categorization. NH, non-Hispanic.
Finally, rates of not getting an HbA1c retest (vs achieving the HbA1c target) were similar across race and ethnicity groups for both years. However, black people with DM had significantly higher unadjusted odds of having HbA1c >9% (vs achieving HbA1c ≤9%) than non-Hispanic (NH) white people with DM. These differences, however, disappeared on multivariable adjustment for age, social categories, and socioeconomic status indicators and no evidence of widening of disparities in 2020 was detected (table 2).
People with HTN
The retesting rate for SBP was 79% in 2019 and 61% in 2020. The rates of having SBP <140 mm Hg were 59% and 43% for 2019 and 2020, respectively. Odds of not getting SBP remeasured (OR 2.57, 95% CI 2.29 to 2.90, p<0.001) and failing to achieve the SBP target (<140 mm Hg) (OR 1.28, 95% CI 1.12 to 1.46, p<0.001) increased in 2020 and remained even after multivariable adjustment (table 3).
Adjusted odds of getting retesting and achieving systolic blood pressure target in people with hypertension according to different sociodemographic categories
Initial models showed that cisgender women were significantly less likely to get their SBP retested compared with cisgender men. These models also showed no differences in unadjusted rates of SBP ≥140 mm Hg across gender categories. After multivariable adjustment, cisgender women still had increased odds of not getting retested (OR 1.71, 95% CI 1.35 to 2.16, p<0.001) with no widening of the disparity in 2020 (table 3). On sensitivity analysis, cisgender women still had higher odds of not getting retested while non-binary people had similar odds compared with cisgender men.
Initial unadjusted models related to sexual orientation showed bisexual, gay, and queer/else people with HTN were significantly more likely to get retested (ie, less likely to not have a retest) than straight individuals with no differences in odds of not achieving SBP <140 mm Hg across categories. The difference in odds of no retesting persisted even after multivariable adjustment (OR for no retesting vs straight: bisexual: 0.99, 95% CI 0.987 to 0.997, p=0.001; OR gay: 0.49, 95% CI 0.32 to 0.75, p<0.001; OR queer: 0.57, 95% CI 0.42 to 0.77, p<0.001). The adjusted model did not show evidence of widening in disparities (table 3).
In initial models, we found that NH black and Asian/other people with HTN had significantly higher odds of not getting SBP retested and not achieving HTN <140 mm Hg compared with NH white people with DM. The difference between black compared with white people remained for not getting tested (OR 1.26, 95% CI 1.01 to 1.58, p=0.040), but not for failing to achieve the SBP target (OR 1.17, 95% CI 0.93 to 1.46, p=0.18). The difference in Asian/other group disappeared after adjustment. Finally, the interaction term between year and black race for no SBP retest was significant (β=−0.36, 95% CI −0.62 to −0.08, p=0.01), suggesting that while odds of not getting SBP retested increased from 2019 to 2020, the magnitude of increase in 2020 for black people with HTN was lower than white people with HTN (table 3). To better illustrate this, we can see that the unadjusted rates of not getting retested increased from 17% to 38% among white people but only from 25% to 41% for black people. Using the model, the adjusted change from 2019 to 2020 for white people was higher at a 23.5% increase (95% CI 19.7 to 27.4) compared with the increase in black people at 16.0% (95% CI 11.9 to 20.1).
Discussion
Key findings
In this analysis of data from LGBTQ+-focused FQHCs in Chicago, we found that receipt of testing services to monitor control of DM and HTN generally declined during 2020, with widening of disparities according to select sexual orientation categories (ie, worse decline in straight, lesbian, bisexual, and queer/else compared with gay people with DM). While there were prepandemic disparities in retesting according to race and ethnicity and according to gender, these did not widen during the pandemic. Indeed, the gap narrowed between black and white people with HTN in terms of retesting. However, this was due to the disproportionate increase in people without SBP retesting among white individuals (unadjusted rates: 17%–38%) rather than an increase in black people with HTN getting SBP retesting (unadjusted rates: 25%–41%) (table 3). Our findings were robust even after adjusting for insurance and socioeconomic indicators.
Several studies examined the changes in DM or HTN care outcomes during the early phases of the pandemic. Like our findings, many observed worse markers of care (eg, getting HbA1c tests, HbA1c levels) in 2020 compared with 2019. However, not all studies observed (or even investigated) widening disparities according to gender or race and ethnicity.5–8 29–32 For example, one study used National Health and Nutrition Examination Survey data to demonstrate decline in achievement of blood pressure targets in the 2017–2020 period versus 2009–2012 among women and black adults.31 Another study observed larger declines in HbA1c testing among females with DM (vs males) but this was associated with higher rebound in testing after lockdown.7 While we did not directly model rebound testing, we indirectly captured it through measuring outcomes at an annual scale. This allowed for people to do catch-up testing after lockdown. The rebound, together with our permissive outcome definition, could help explain why we did not observe widening disparities in several groups. This also stresses the need to do outreach for groups that continued to lag despite allowing for catch-up via the rebound. Community outreach has been shown to address inequities in COVID-19 vaccinations and this model could be extended to chronic disease care.33 Outreach and engagement may also help uncover underlying reasons for the lag and help inform best approaches to promote health visits.34
Our work builds on the prior research by including sexual orientation and expansive gender identity and investigating widening of disparities across multiple axes. In addition, since DM and HTN are important drivers of risk of cardiovascular disease in LGBTQ+ populations, identifying these gaps in care produced by the pandemic would be important in larger efforts to achieve better cardiovascular health in this population.22 35
Drivers of disparities in chronic disease management
Our work stresses the need to include a variety of axes of marginalization, including sexual orientation and expansive gender identity categories, when conducting investigations of disparities. Socioecological theory points to the need for recognizing in the role of different axes of identity in assessing disparities.36 Most disparities research, however, has focused on race and ethnicity and binary gender, partially due to the ready availability of data on these variables and theories to interpret findings. However, these are not the only forms of oppression that drive disparities. Homophobia, monosexism, and transphobia are also important. These systems can act directly (eg, implicit bias, exclusionary policies) or indirectly (eg, affect socioeconomic status and thus access to insurance and care) to affect health outcomes and healthcare utilization.22 35
Our findings demonstrated the differential impacts on subgroups among people with DM and HTN. These differences are driven by differences in needs and experiences according to SOGI and race and ethnicity and as such a one-size-fits-all approach would be inappropriate to solve care disparities. Tailored population approaches would be important to address the disparities we uncovered.37 38 Tailoring requires considering how different populations interact with the health system. Organizations could consider the types of routine care certain groups usually get and how it could be integrated with chronic disease management. HIV or mental healthcare integration efforts can serve as models.39 40 They could also consider social risks that affect care utilization (eg, housing or transport issues) and provide solutions to address these (eg, social services referral, remote care).41–43 These efforts should be done with community engagement and should also ensure that changes within the health system to address issues like bias or cultural competency are made.44
Limitations
Our use of data from a single health system in Chicago limits generalizability. Replication in other contexts is needed. We were also unable to fully examine some categories (eg, Pacific Islander) due to small samples. In addition, recent work calls for applying intersectionality in disparities research,45 46 unfortunately we were unable to examine intersectional subgroups (eg, Hispanic transwomen) due to small group sizes.
We are also unable to examine mechanisms underlying the observed disparities. For example, as health systems pivoted to telehealth settings, remote measurements of SBP and HbA1c (through at-home equipment or partner laboratory services) became more available. We are unable to account for this out-of-system measurements in our analysis and it is possible that the disparity we captured may be explained by increased utilization of these services by some groups. Finally, we are unable to confirm how disproportionate impact of lockdowns on behavior of different groups (eg, mobility or out-of-home activities) translated to healthcare utilization.47 Future research on mechanisms is needed to help inform interventions.
Conclusion
Disparities in DM and HTN care according to gender, race and ethnicity, and sexual orientation persisted and might have widened during the pandemic. More work is needed as to how SOGI affects care utilization. Despite limitations to generalizability, this study was made possible because SOGI was integrated into routine data in the EHR. More widespread inclusion of SOGI in EHR is necessary to facilitate future work.
Data availability statement
Data may be obtained from a third party and are not publicly available. Data are not made open access since it came from electronic health records. Requests for data access can be sent to Howard Brown Health.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the Institutional Review Boards of Howard Brown Health (E-075) and Northwestern University (STU00214102).
References
Footnotes
Contributors All authors reviewed and approved the article before submission. ASR: conceptualization, methodology, formal analysis, data curation, writing–original draft, gaurantor. MP: data curation, writing–review and editing. AD: visualization, writing–review and editing. MJF: methodology, review and editing. LKR: data curation, resources, writing–review and editing, funding acquisition. LBB: conceptualization, methodology, resources, writing–review and editing, funding acquisition.
Funding ASR received funding support from the American Heart Association Predoctoral Fellowship Program (825793). The data pull was funded through NIAID P30 AI117943 (PI: D’Aquila). Publication was supported by the Northwestern University Open Access Fund. The fund had no role in the design, analysis, and writing of this paper. The paper is solely the responsibility of the authors and does not necessarily represent the official views of the fund.
Competing interests MP, AD, and LKR are currently employed at Howard Brown Health.
Provenance and peer review Not commissioned; externally peer reviewed.