Article Text

Abstract
Introduction To present longitudinal data from the Real-world Observational Study on Patient Outcomes in Diabetes (RESPOND) in Japan.
Research design and methods In this multicenter, prospective, observational cohort study, patients with type 2 diabetes mellitus (T2DM) newly initiated on monotherapy were followed up for 2 years. Primary outcomes included changes in treatment pattern over time, target hemoglobin A1c (HbA1c) attainment and treatment satisfaction per Oral Hypoglycaemic Agent Questionnaire (OHA-Q).
Results Among 1474 enrolled patients (male, 62.1%; mean age, 59.7 years; HbA1c, 8.08%), the oral antidiabetic drug (OAD) monotherapy prescription rate decreased to 47.2% and that of 2 and ≥3 OADs increased to 14.8% and 5.4% at 24 months, respectively. Switch/add-on OAD was associated with higher HbA1c and body mass index (BMI), baseline OAD being non-dipeptidyl peptidase-4 inhibitor (DPP-4i)/non-sodium glucose cotransporter-2 inhibitor (SGLT2i), diabetes complications, no comorbidities and consulting a diabetes specialist. The mean (SD) HbA1c (%) was 6.73 (0.85) at 24 months. Higher HbA1c, diabetes complications, cardiovascular disease, being employed, no hypertension and younger treating physician were associated with ≥2 OAD classes prescription or target HbA1c non-attainment at 24 months. OHA-Q subscale scores were significantly higher in patients achieving (vs not achieving) target HbA1c and in those continuing monotherapy (vs combination therapy). Baseline age (<65 years), sex (female), HbA1c, alcohol use, use of non–DPP-4i OADs or non-T2DM drugs, diabetes complications and cardiovascular disease had a significant negative impact, while EuroQol five-dimensional five-level and Summary of Diabetes Self-Care Activities-specific diet scores, BMI and unemployment had a significant positive impact on OHA-Q scores at 24 months.
Conclusions Primary outcomes show real-world treatment patterns and glycemic control over 2 years in patients with T2DM newly initiated on OAD monotherapy in Japan. Key factors associated with durability of initial monotherapy, target achievement or treatment satisfaction included baseline HbA1c, comorbidity and initial OAD choice.
- diabetes mellitus, type 2
- dipeptidyl peptidase 4
- metformin
- observational study
Data availability statement
Data are available on reasonable request. Data are available on reasonable request. The data sharing policy of Merck & Co., Inc., Kenilworth, New Jersey, USA, including restrictions, is available online (http://engagezone.msd.com/ds_documentation.php). Requests for access to the study data can be submitted through the EngageZone site or via email to dataaccess@merck.com.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Treatment recommendations for first-line therapies in patients with type 2 diabetes mellitus (T2DM) differ between the Japanese and Western guidelines.
The Japanese guidelines recommend individualized therapy, with no preference for treatment class.
The Western guidelines generally recommend metformin as initial therapy, taking into consideration any contraindications such as high cardiovascular risk and comorbidities, patient-centered treatment factors such as body weight and management needs.
WHAT THIS STUDY ADDS
Most patients with T2DM continued oral antidiabetic drug (OAD) monotherapy, and the use of injectables was uncommon within 2 years of initiating OAD.
Overall, more than one-third of patients who remained on treatment attained the individualized target HbA1c throughout the study period. The percentage of patients achieving the target HbA1c at 24 months reduced with an increase in the number of add-on OADs.
Besides patient characteristics such as HbA1c, comorbidity and background cardiovascular risk, the initial OAD choice may significantly impact the likelihood of treatment adjustment and patient satisfaction.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The study results highlighted the significance of initial drug choice as a part of key consideration associated with the outcomes and treatment satisfaction in T2DM management.
Further investigations for patient-centric focus on other related clinical activities not addressed in the present study are warranted.
Introduction
The global prevalence of diabetes is projected to reach 783 million by 2045 from the 537 million of 2021.1 In Japanese adults aged 20–79 years, the prevalence of diabetes was 11.8%, and 0.25 million deaths were attributed to diabetes.1 Type 2 diabetes mellitus (T2DM) is characterized by a lower insulin secretory function and lower probability of obesity-associated insulin resistance in the Japanese versus other ethnic populations.2 3
According to the American Diabetes Association (ADA) guidelines, first-line therapy should be selected based on comorbidities, patient-centered treatment factors and management needs and generally includes metformin, unless contraindicated, along with comprehensive lifestyle modifications.4 The European Association for the Study of Diabetes (EASD)/European Society of Cardiology (ESC) guidelines also recommend metformin as first-line therapy in overweight patients with T2DM at moderate cardiovascular (CV) risk and without CV disease (CVD).5 Although the Japanese Clinical Practice Guideline (CPG) 2019 recommends individualized therapy and no particular treatment class as the preferred initial therapy in patients with T2DM,6 dipeptidyl peptidase-4 inhibitors (DPP-4i) have been increasingly prescribed as first-line therapy in Japan. A preference for DPP-4i over metformin for initial therapy in Japan could partly be explained by the delayed approval of high-dose metformin (2250 mg) due to a potential risk of lactic acidosis and unavailability of extended-release formulation of metformin.7
To date, limited information is available regarding the durability of initial T2DM monotherapy and subsequent changes in pharmacotherapy in Japan. Further real-world studies are needed to evaluate the experience of patients with T2DM treated with oral antidiabetic drugs (OADs), given the increase in the number of newer OADs and complexity of treatment regimens. The Real-world Observational Study on Patient Outcomes in Diabetes (RESPOND) is a multicenter, prospective, observational cohort study designed to generate high-quality, comprehensive, real-world data for treatment-naïve patients with T2DM newly initiated on an OAD.8 The study design for RESPOND; baseline data, including the OAD distribution by treatment class prescribed as initial monotherapy by specialists and non-specialists; and differences in diabetes self-care activities, adherence to self-care recommendations and education on nutrition and foot care among patients treated by specialists and non-specialists were published previously.8 Here, we present the 2-year longitudinal phase data from RESPOND, including changes in treatment patterns over time, the target hemoglobin A1c (HbA1c) attainment rate and treatment satisfaction in patients with T2DM in a real-world setting in Japan.
Materials and methods
Study design
RESPOND (Japan Pharmaceutical Information Center identifier, JapicCTI-163306) was conducted from June 2016 to November 2019 in patients with T2DM who newly initiated OAD monotherapy at 174 sites in Japan. The detailed inclusion and exclusion criteria have been described previously.8 Two-year follow-up data from the enrolment date were captured via electronic case report forms. Patient medical records and patient/physician survey information were used as data sources. Treatment patterns were recorded in the medication log/records over the study period.8
Physician participants
Diabetologists and endocrinologists (considered diabetes specialists) and general practitioners, family medicine physicians, primary care physicians and cardiologists (considered non–diabetes specialists) who were routinely involved in the management of patients with T2DM were targeted for recruitment.
Outcomes
Primary outcomes included treatment patterns changes over time for T2DM treatment classes (switch or addition of new classes) and the proportion of patients initiating OADs as monotherapy achieving their individualized glycemic target set by physicians at baseline during the 2-year follow-up.
Other outcomes included time to first treatment adjustment (switch/add-on therapy) by baseline OAD, proportion of patients initiating OADs as monotherapy achieving HbA1c <7.0% and subscale scores for treatment convenience, somatic symptoms and treatment satisfaction at the end of the 2-year follow-up using the Oral Hypoglycaemic Agent Questionnaire (OHA-Q).9 In the analysis of first treatment adjustment, switch was defined as the initiation of another monotherapy on or after the discontinuation of baseline OAD monotherapy. Add-on therapy was defined as initiating combination therapy without discontinuing baseline OAD monotherapy. The occurrence of treatment adjustment and HbA1c target attainment during the 2-year follow-up were stratified by baseline patient characteristics or treatment regimen at each time point. A multivariate regression analysis for each outcome was performed to identify the baseline patient characteristics associated with time to first treatment adjustment, history of treatment change or missing individualized HbA1c target set by physicians at baseline and the OHA-Q subscale scores at the end of the 2-year follow-up.
Statistical analysis
Sample size estimation has been described previously.8 Missing data were not imputed. In descriptive analyses, continuous variables are summarised as mean (SD) or median (IQR) and categorical variables as number and proportion of the total study population and by predefined subgroups, where appropriate. Median (IQR) time to first treatment adjustment by baseline OAD was estimated using the Kaplan-Meier method.
Baseline patient characteristics associated with first treatment adjustment were evaluated using a Cox regression analysis and those associated with the history of treatment adjustment or HbA1c greater than or equal to the target value at 2 years were evaluated using a multivariate logistic regression analysis. In the multivariate analyses, explanatory variables were selected considering their importance in glycemic control; categorical variables included age, sex, family history of diabetes, current smoking status, drinking habit, educational background, family living together, current employment status, baseline OAD, diabetic complications, CVD, dyslipidemia, hypertension, comorbidities, non-T2DM drugs, consulting physician and place of visit; continuous variables included EuroQol five-dimensional five-level (EQ-5D-5L) utility score, Summary of Diabetes Self-Care Activities (SDSCA) general diet subscale, SDSCA specific diet subscale, SDSCA exercise subscale, HbA1c, body mass index (BMI), physician’s age and number of visits/month of patients with T2DM.8 10 11 Baseline patient characteristics, which either positively or negatively impacted the OHA-Q subscale scores at 2 years, were evaluated using multivariate linear regression analysis with the same set of explanatory variables. Statistical significance was defined as p<0.05.
Results
Patient disposition
Of the 1521 patients registered, 1506 were enrolled. Subsequently, 1496 patients were eligible, of whom 22 withdrew consent and 1474 were included in the analysis (online supplemental figure S1).
Supplemental material

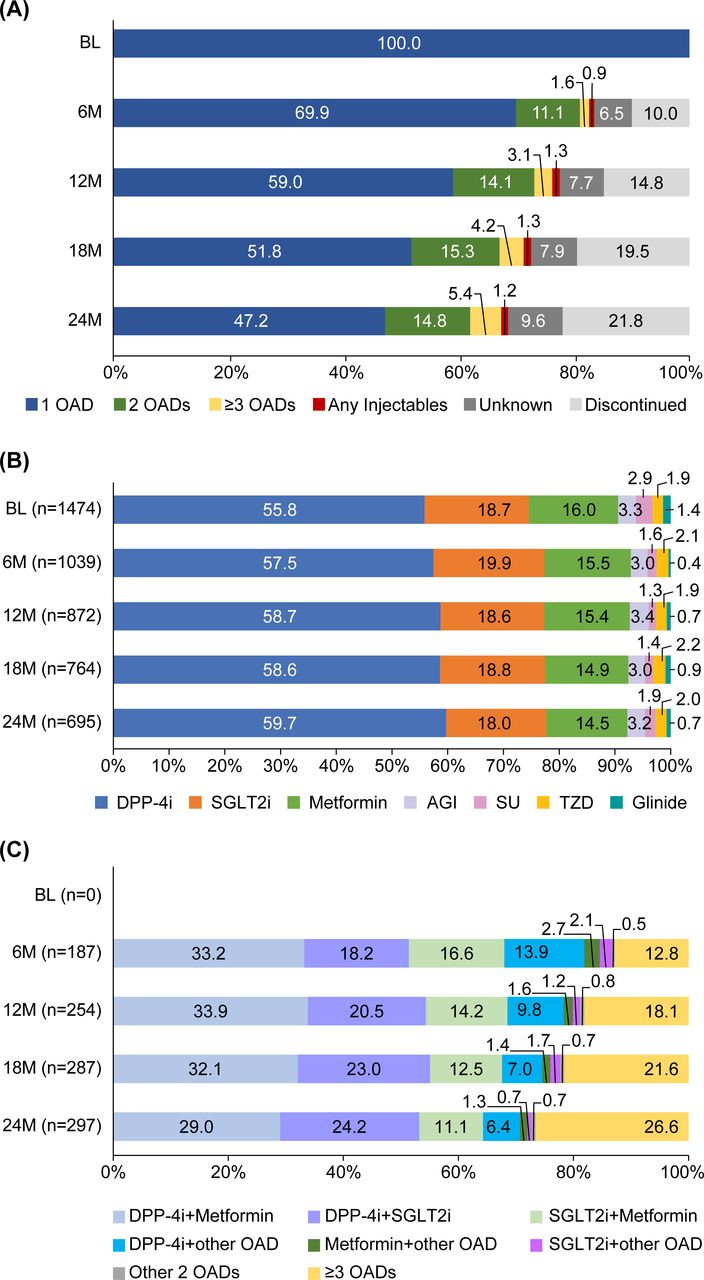
Distribution of treatment regimens over time. (A) Type of drug treatment at each time point (full analysis set). (B) OAD monotherapy class among patients receiving OAD monotherapy at each time point. (C) OAD combination therapy type among patients receiving OAD combination therapy at each time point. AGI, alpha glucosidase inhibitor; BL, baseline; DPP-4i, dipeptidyl peptidase-4 inhibitor; M, month; OAD, oral antidiabetic drug; SGLT2i, sodium-glucose cotransporter-2 inhibitor; SU, sulfonylurea; TZD, thiazolidinedione. n presented on the Y-axis refers to the number of patients with prescribing information available at the respective time point; proportions were calculated from the full analysis set; unknown group refers to patients who were lost to follow-up or had prescribing information unavailable during follow-up.
Patient characteristics
Of the 1474 patients included in the analysis, 62.1% (n=915) were male, 42.5% (n=626) had a family history of T2DM and 90.3% (n=1331) were visiting clinics; 43.0% (n=634), 20.7% (n=305), 6.0% (n=88) and 2.6% (n=38) were consulting a diabetes specialist, cardiologist, nephrologist and geriatrician, respectively. At baseline, the mean (SD) age was 59.7 (13.3) years; diabetes duration, 0.86 (1.87) years; HbA1c, 8.08% (1.83%); and individualized target HbA1c, 6.51% (0.52%). Most patients did not have diabetes complications (n=1279), CVD (n=1383) or other comorbidities (n=1006; online supplemental table S1).
Distribution of treatment regimens
Treatment pattern
In the overall analysis population, the OAD monotherapy prescription rate decreased to 47.2% at 24 months from baseline (n=1474; figure 1A). However, the proportion of patients prescribed a combination of 2 and ≥3 OADs increased to 14.8% and 5.4%, respectively, at 24 months. The proportion of patients prescribed injectable antidiabetic therapies remained <2.0% throughout the study period, and those discontinuing treatment was 21.8% at 24 months.
Oral monotherapy
Among patients with available prescription record, DPP-4i was the most commonly prescribed OAD monotherapy in 55.8% and 59.7% of patients at baseline and those who were on monotherapy at 24 months, respectively (figure 1B). The proportion of patients on monotherapy who were prescribed sodium/glucose cotransporter-2 inhibitors (SGLT2i), metformin and other OAD classes remained relatively stable from baseline to 24 months (SGLT2i, 18.7% vs 18.0%; metformin, 16.0% vs 14.5%; alpha glucosidase inhibitors, 3.3% vs 3.2%; sulfonylureas (SU), 2.9% vs 1.9%; thiazolidinediones, 1.9% vs 2.0%; glinides, 1.4% vs 0.7%, respectively).
Oral combination therapy
The most commonly prescribed (range) 2-drug combinations throughout the study period were DPP-4i+metformin (29.0%–33.9%), DPP-4i+SGLT2 i (18.2%–24.2%) and SGLT2i+metformin (11.1%–16.6%) (figure 1C).
Distribution of OADs
The percentage of patients prescribed metformin, DPP-4i and SGLT2i as monotherapy decreased steadily from 6 months to 24 months, which was associated with a corresponding increase in the proportion of patients prescribed these OADs as add-on therapy (online supplemental figure S2). At 24 months, >50.0% of patients with available prescription record continued the baseline metformin, DPP-4i or SGLT2i as monotherapy. The percentage of patients who switched OAD increased at 24 months versus 6 months for all 3OAD classes: metformin (8.4% vs 2.9%), DPP-4i (3.4% vs 1.1%) and SGLT2i (4.2% vs 3.8%).

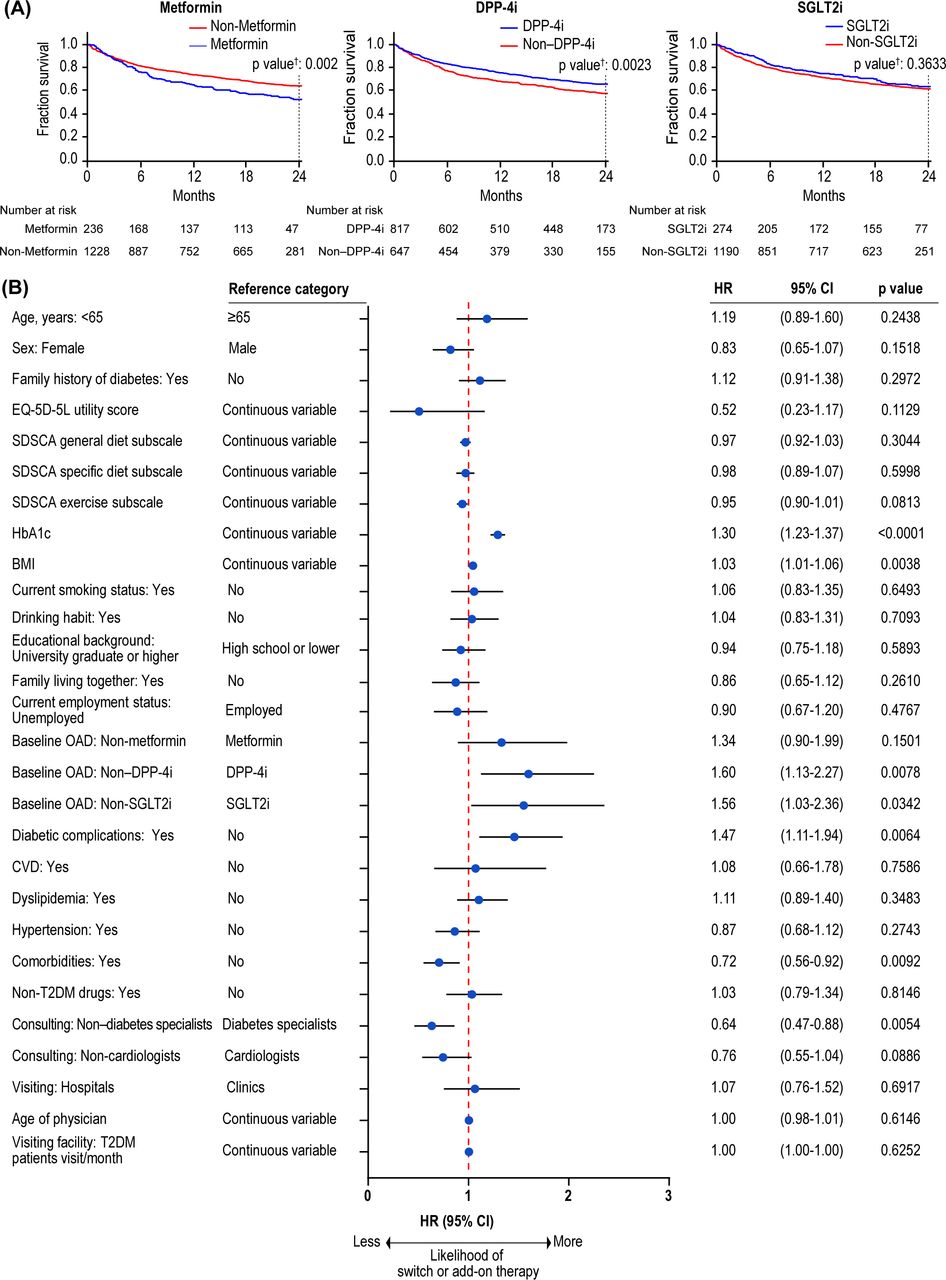
Time to first treatment adjustment. (A) Kaplan-Meier curve by baseline OADs. (B) Cox regression analysis by baseline variables. As for continuous variables, HR is for a 1-unit increase in the value. †Calculated using the log-rank (Mantel-Cox) test. BMI, body mass index; CVD, cardiovascular disease; DPP-4i, dipeptidyl peptidase-4 inhibitor; EQ-5D-5L, EuroQol five-dimensional five-level; HbA1c, hemoglobin A1c; OAD, oral antidiabetic drug; SDSCA, Summary of Diabetes Self-Care Activities; SGLT2i, sodium-glucose cotransporter-2 inhibitors; T2DM, type 2 diabetes mellitus. Most common comorbidities were liver disease, CVD, atrial fibrillation, chronic kidney disease and peptic ulcer disease, excluding those categorized as diabetes complications, CVD, dyslipidemia and hypertension. Employed included full-time and part-time employees, and unemployed included students, homemakers and retired employees.
Durability of initial OAD treatment
Overall, 725 patients (49.2% of the analysis population) discontinued the initial OAD during the follow-up period. The median (IQR) duration of the initial OAD (days) was 204 (61.5–440.0), including the period after the initiation of combination therapy with additional OAD(s). The duration of baseline SGLT2i, DPP-4i and metformin was 260 (107.0–687.0), 226 (91.0–448.5) and 112 (42.0–335.5), respectively, and that for other OAD classes was 121.5 (33.0–384.0).
Time to first treatment adjustment by baseline variables
The estimated probability of continuing initial OAD monotherapy without any treatment adjustment at 24 months was 52.7%, 66.1% and 64.1% in patients receiving metformin, DPP-4i or SGLT2i, respectively, versus 64.3%, 58.0% and 62.1% in patients receiving non-metformin, non–DPP-4i or non-SGLT2i, respectively, at baseline (figure 2A). A Cox regression for time to treatment adjustment revealed that patients with higher HbA1c and BMI, prescribed non–DPP-4i/non-SGLT2i OAD, with diabetes complications, without other comorbidities and consulting a diabetes specialist were at a greater risk of switching/add-on therapy (figure 2B). Online supplemental table S1 summarises the number and proportion of patients who underwent treatment switch or add-on therapy by baseline patient characteristics.
Individualized target HbA1c attainment rate by baseline characteristics
Among patients with available laboratory data, the proportion of patients achieving the target HbA1c at 24 months was significantly impacted by age and hypertension. A higher proportion of patients aged ≥66 versus ≥54 to <66 versus <54 years (41.3% vs 33.1% vs 31.4%; p=0.0113; online supplemental table S2) achieved the target HbA1c at 24 months. Similarly, a higher proportion of those with (vs without) hypertension achieved the target HbA1c at 12 months (41.8% vs 32.6%; p=0.0012), 18 months (41.9% vs 31.1%; p=0.0002) and 24 months (39.1% vs 31.9%; p=0.0151). At 12 months, a higher proportion of patients consulting (vs not consulting) a diabetes specialist (41.9% vs 34.0%; p=0.0054) and not consulting (vs consulting) a cardiologist (39.6% vs 29.4%; p=0.0033) achieved the target HbA1c.
Glycemic control by treatment regimen
Overall, the mean (SD) HbA1c (%) at 24 months was 6.73 (0.85) (online supplemental table S3). Among patients with available data on glycemic outcome, a similar proportion of patients achieved the individualized target HbA1c throughout the study period (6 months, 35.8%; 24 months, 35.7%). The percentage of patients achieving the target HbA1c at 24 months reduced with an increase in the number of OADs (1 OAD, 35.1%; 2 OADs, 33.6%; ≥3 OADs, 31.6%). Patients treated with OAD monotherapy had similar mean (SD) HbA1c (%) at 6 months (6.68 (0.86)) and 24 months (6.64 (0.73)); 36.9% and 35.1% of patients achieved the target HbA1c at 6 and 24 months, respectively. In patients treated with 2 OADs, the mean (SD) HbA1c (%) was 7.20 (1.09) and 6.85 (0.78) at 6 and 24 months, respectively; 27.0% and 33.6% of patients achieved the target HbA1c, respectively. Among patients receiving 2-drug combinations, 35/86 (40.7%), 21/71 (29.6%) and 10/33 (30.3%) treated with DPP-4i+metformin, DPP-4i+SGLT2 i and SGLT2i+metformin, respectively, achieved the target HbA1c at 24 months (online supplemental table S3). The mean (SD) HbA1c (%) in patients receiving ≥3 OADs at 6 and 24 months was 7.51 (1.29) and 7.13 (1.09), with 29.2% and 31.6% of patients achieving the target HbA1c, respectively. One-half of patients who received SGLT2i+another OAD achieved the target HbA1c at 24 months compared with one-quarter of patients at 6 months. A higher percentage of patients who received injectables and unknown therapies achieved the target HbA1c at 6 and 24 months than those who received metformin, DPP-4i or SGLT2i.
Achievement of HbA1c <7.0% by baseline characteristics
The mean (SD) HbA1c (%) at baseline was 8.08 (1.83), and 70.3% of patients achieved HbA1c <7.0% at 6 months, which was sustained until 24 months (online supplemental table S4). A higher proportion of patients aged ≥66 versus ≥54 to <66 versus <54 years (77.3% vs 72.1% vs 59.9%; p=0.0001), female versus male patients (77.2% vs 65.9%; p=0.0001), baseline HbA1c <7.0% versus ≥7.0% to <8.2% versus ≥8.2% (90.1% vs 67.8% vs 53.4%; p=0.0001), with versus without hypertension (75.5% vs 65.0%; p=0.0002) and treated versus not treated by a cardiologist (76.1% vs 69.0%; p=0.0411) achieved HbA1c <7.0% at 24 months.
Predictors of requiring treatment intensification
A multivariate logistic regression analysis to identify the explanatory variables associated with a history of receiving ≥2 OAD classes or missing the individualized HbA1c target at 24 months showed that patients with higher baseline HbA1c, with diabetes complications or CVD, employed, without hypertension or being treated by a younger physician were likely to require treatment intensification (figure 3). The baseline OAD class was not significantly associated with the likelihood of requiring treatment intensification.

{kind=link}
{kind=link}
{kind=link}
Multivariate logistic regression for history of treatment adjustment during the follow-up period or HbA1c exceeding the individualized target at 24 months. As for continuous variables, OR is for a 1-unit increase in the value. BMI, body mass index; CVD, cardiovascular disease; DPP-4i, dipeptidyl peptidase-4 inhibitor; EQ-5D-5L, EuroQol five-dimensional five-level; HbA1c, hemoglobin A1c; OAD, oral antidiabetic drug; SDSCA, Summary of Diabetes Self-Care Activities; SGLT2i, sodium-glucose cotransporter-2 inhibitor; T2DM, type 2 diabetes mellitus. Most common comorbidities were liver disease, CVD, atrial fibrillation, chronic kidney disease and peptic ulcer disease, excluding those categorized as diabetes complications, CVD, dyslipidemia and hypertension. Employed included full-time and part-time employees, and unemployed included students, homemakers and retired employees.
Treatment satisfaction
OHA-Q subscale scores were significantly higher in patients achieving (vs not achieving) the target HbA1c and in those continuing monotherapy (vs combination therapy) over the study period (table 1). Multivariate regression analysis revealed that baseline patient characteristics such as age (<65 years), sex (female), HbA1c, alcohol use, use of non–DPP-4i OADs or non-T2DM drugs, diabetes complications and CVD had a significant negative impact, while EQ-5D-5L and SDSCA specific diet scores, BMI and unemployment had a significant positive impact on at least one of the OHA-Q subscale scores at 24 months (table 2).
Treatment satisfaction scores
Multivariate logistic regression for treatment satisfaction scores at 24 months
Discussion
To the best of our knowledge, RESPOND is one of the largest prospective, non-interventional studies that enrolled treatment-naïve patients with T2DM newly initiated on OAD monotherapy in a real-world setting in Japan. This study provides new insights that may help improve the outcomes of initial T2DM pharmacotherapy. Because multiple factors impact the choice of initial OAD, the present study addresses key hypotheses about the association between patient characteristics and treatment trajectory.
The use of OAD monotherapy reduced over the study period, with a corresponding increase in that of a combination of ≥2 OADs. These findings are concordant with the Japanese CPG that recommends initiating treatment with a single drug at a low dose and subsequently increasing the dose, adding another drug with a different mechanism of action or adding/switching to insulin therapy if adequate glycemic control is not achieved.6
DPP-4i is reportedly more effective in Asian patients than in patients from other ethnic groups as per a systematic review/meta-analysis of randomized studies of DPP-4i in T2DM.12 Furthermore, DPP-4i treatment demonstrated a low risk of hypoglycemia, weight neutrality and preservation of residual pancreatic function in a multicenter, prospective, randomized, open-label study directly comparing the efficacy and safety of DPP-4i and SU in elderly patients with T2DM in Japan, suggesting that DPP-4i is a potentially beneficial OAD class for use in elderly patients with T2DM.13 Moreover, diabetes prevalence is expected to further increase during the next decade primarily due to a rapidly aging population.14 Taken together, the neutral effect on body weight and favorable efficacy/safety profile, particularly in a rapidly increasing proportion of elderly patients who are generally at a higher risk of hypoglycemia and/or sarcopenia, could be the reason for DPP-4i being the most commonly prescribed OAD class in Japan.15–17 DPP-4i was also reported as the most preferred first-line OAD class by approximately 70.0% of diabetes specialists and non-specialists in a web-based online survey conducted across eight selected regions in Japan (n=491).10
SGLT2i was the second most commonly prescribed OAD as monotherapy in this study. Although the specific reasons for prescription of SGLT2i in this study were not captured, SGLT2i reportedly promotes weight loss and reduces blood pressure.18 SGLT2i is the recommended first-line treatment by ADA and EASD/ESC in patients at an increased risk of heart failure and those at a high risk of atherosclerotic CVD and chronic kidney disease (CKD).4 5 As this study included treatment-naïve patients who were newly initiated on monotherapy and majority of the patients had normal kidney function or mild-to-moderate CKD, the association between SGLT2i use and renal dysfunction was not evaluated. SGLT2i have demonstrated greater effectiveness in patients with T2DM with moderate-to-advanced CKD in real-world studies.19–22
Although metformin is the recommended first-line OAD in many countries,4 5 23 it was the third most prescribed first-line OAD class in our study. The inclusion of a boxed warning for an increased risk of lactic acidosis with a high dose and in the elderly (aged >75 years) with metformin in March 2012 in Japan7 could be one of the reasons for the less frequent metformin prescriptions in this study. The mean (SD) dose of metformin at the end of its monotherapy was 861.4 (388.1) mg/day. A total of 14/101 (13.9%) patients were prescribed metformin at a dose >1000 mg/day. The reason(s) for the discontinuation of monotherapy without reaching the maximum daily dose of metformin is unclear because this study did not capture the reason for treatment change; lack of efficacy is most likely a predominant reason for switch or add-on.24 In addition, a lingering concern for potential risk of lactic acidosis with higher metformin dose might be one of the reasons to discontinue monotherapy before reaching the maximum dose.7
In this study, OAD monotherapy was maintained in approximately 50.0% of patients who remained on treatment for 2 years. The persistence of initial monotherapy with DPP-4i or SGLT2i was longer than that with metformin. A lower persistence rate with metformin could be a result of poor tolerance to metformin-associated gastrointestinal symptoms, as observed in a previous study.25 DPP-4i and SGLT2i were also widely prescribed as part of 2-drug and 3-drug regimens in this study. This could be because both DPP-4i and SGLT2i are well tolerated, have a low risk of hypoglycemia (unless combined with an SU or insulin) and may be combined with other antidiabetic therapies to enhance HbA1c-lowering efficacy.18 23 25 26
In our study, 21.6% and 13.8% of patients in the overall analysis population received an add-on or switched therapy as a second-line treatment, respectively, likely intending to achieve an improved glycemic control (online supplemental table S1). Safety concerns associated with the initial OAD could be other potential reasons. The Cox regression analysis revealed a greater likelihood of switch/add-on therapy in patients consulting diabetes specialists in our study, which could be associated with lower prevalence of clinical inertia for treatment intensification among diabetes specialists as suggested in Southeast Asian studies.27 28 Another reason could be a potentially greater compliance of diabetes specialists (vs non–diabetes specialists) to current treatment guidelines. Although several studies have reported an association between non–diabetes specialists and clinical inertia for initiating insulin therapy in patients with inadequate glycemic control on OADs,29 to our knowledge, none have analyzed the association between treatment intensification using add-on OADs, and therefore, this warrants further investigation. Moreover, clinical inertia may be concerning in patients consulting non–diabetes specialists.
An analysis of a Japanese diabetes specialists’ patient registry indicated that baseline HbA1c ≥8.0% was associated with a higher likelihood of add-on therapy to the initial OAD monotherapy (biguanide/DPP-4i),30 potentially due to poor glycemic control. In our study, patients consulting diabetes specialists (vs non–diabetes specialists, online supplemental table S2) had a higher baseline HbA1c (8.35% vs 7.88%), suggesting a greater risk of developing diabetes complications, thereby likely requiring more frequent treatment changes to achieve the target glycemic goals, as observed. In case of diabetes complications, a need for treatment intensification could lead to switch/add-on therapy, particularly in patients consulting diabetes specialists.
The Japan Diabetes Society recommends a glycemic goal of HbA1c <7.0% for the prevention of diabetes complications.6 In our study, baseline HbA1c significantly impacted the achievement of the glycemic goal, with a higher proportion of patients with baseline HbA1c <7.0% versus ≥7.0% maintaining the glycemic control at 2 years (online supplemental table S4). Similarly, patients with baseline HbA1c <7.0% (vs ≥7.0%) were five times more likely to achieve the glycemic goal in a claims-based Japanese study.27 The Japanese CPG also recommends that HbA1c goals are individualized based on patient characteristics, patient preferences and the risk of treatment-related adverse effects such as hypoglycemia and weight gain. In our study, the mean individualized HbA1c target and attainment rate (6.5% and 35.7%%–37.4%, respectively; online supplemental table S3) in overall analysis population were close to those (6.8% and 39.1%, respectively) reported in a survey conducted in Europe and the USA in which 62.5% of patients were prescribed metformin as monotherapy or as part of combination therapy.31 An increase in the number of OADs coincided with a lower proportion of patients achieving the target HbA1c (online supplemental table S3), consistent with the findings of the International Diabetes Management Practice Study that identified the use of fewer OADs as a predictor of achieving HbA1c targets.32 Consultation with a diabetes specialist was not a predictor of requiring prescription of ≥2 OADs during the follow-up period or missing the glycemic target at 24 months, although it was significantly associated with time to first treatment changes. This suggests that diabetes specialists likely treated patients with a longer duration of diabetes, more complications or other difficulties to manage diabetes and, thus, might have needed to try multiple treatment options over a long term to achieve glycemic control.
In patients with T2DM, treatment satisfaction is a key determinant for maintaining patient commitment and confidence in their treatment and self-care.33 Patient satisfaction with treatment is linked to improved adherence,34 which should be significantly associated with improved glycemic control.35 Thus, treatment satisfaction being an important consideration for treatment selection, a greater understanding of this parameter can help physicians make an optimal choice among a plethora of OAD options. OHA-Q, an instrument specifically designed to evaluate treatment satisfaction in patients with T2DM receiving OADs, has the ability to distinguish between OADs and has good psychometric attributes.36 In our study, all the subscales of OHA-Q were generally higher among patients who achieved the target HbA1c and continued monotherapy versus those who received combination therapy. Furthermore, at least one of the OHA-Q subscale scores was negatively impacted by baseline age (<65 years), sex (female), HbA1c, alcohol use, use of non–DPP-4i OADs or non-T2DM drugs, diabetes complications and CVD, and positively impacted by EQ-5D-5L and SDSCA specific diet scores, BMI and unemployment. A previous Japanese randomized controlled study, PREFERENCE 4, reported the highest treatment satisfaction scores for DPP-4i among all OAD classes, which is in line with the negative impact of non–DPP-4i on treatment convenience and somatic symptom subscale scores identified in our study, over a longer duration and in a larger study population.33
This was a non-interventional nationwide study in the usual care setting in Japan and enabled the generation of robust real-world evidence around the treatment patterns of treatment-naïve patients with T2DM initiating OAD monotherapy. The prospective study design ensured that there was no recall bias, and selection bias was reduced because of broad inclusion criteria. However, the study limitations include unavailability of data for all study variables and outcomes for all patients, potential impact of unmeasured confounders and short duration of diabetes, increased probability of inflation of type 1 errors due to multiple statistical testing in the exploratory subgroup comparison, lack of information on medication adherence at the patient level, lack of reason(s) for treatment changes and limited length of follow-up and possibility of survival bias because patient-level data could not be fully collected in 31.5% of enrolled patients.
Most of the two-thirds of enrolled patients in real-world settings whose data were available at 2 years remained on OAD monotherapy, and the use of injectables was uncommon within 2 years of initiating OAD. Approximately 50% of patients who continued baseline OAD over 2 years continued receiving it as monotherapy. This finding implies that initial OAD selection was generally successful in achieving HbA1c <7.0% based on the patient characteristics at baseline, although there is scope for improvement in the individualized target attainment. In general, initial OAD treatment was proactively adjusted to aim for individualized care, especially among patients with comorbidities. Furthermore, the choice of initial OAD was identified as a key independent determinant associated with treatment adjustment during the follow-up period and patient satisfaction at 24 months. Further investigations for patient-centric focus on some other clinical activities in T2DM management, including glucose monitoring, shared decision-making and multidisciplinary team–based diabetes care, not addressed in the present study are warranted.
Data availability statement
Data are available on reasonable request. Data are available on reasonable request. The data sharing policy of Merck & Co., Inc., Kenilworth, New Jersey, USA, including restrictions, is available online (http://engagezone.msd.com/ds_documentation.php). Requests for access to the study data can be submitted through the EngageZone site or via email to dataaccess@merck.com.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Toukeikai Kitamachi Clinic ethical review board (approval number, MSD04820). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We thank the investigators and patients who participated in RESPOND. Medical writing support was provided by Deepali Garg, MBBS, PGDHA, of Cactus Life Sciences (part of Cactus Communications) and funded by MSD K.K., Tokyo, Japan.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
AT and KT are joint first authors.
Contributors AT contributed to the data analysis and manuscript writing. KT contributed to the study design and conduct, data collection and analysis and manuscript writing. JE, HO, HW, IS and TK contributed to the manuscript writing. ST contributed to the study design and manuscript writing. AT and KT are guarantors and accept full responsibility for the work.
Funding This study was funded by MSD K.K., Tokyo, Japan.
Competing interests AT, KT, JE and ST are employees of MSD K.K., a subsidiary of Merck & Co., Inc., Kenilworth, NJ, USA, and may own stock and/or hold stock options in the company. HO has received personal fees from MSD during the conduct of the study. HW has received grants and personal fees from MSD during the conduct of the study. His relevant financial activities outside the submitted work are grants and personal fees from Astellas, Daiichi Sankyo, Eli Lilly, Mitsubishi Tanabe, Nippon Boehringer Ingelheim, Novartis, Novo Nordisk, Ono, Sanofi, Sanwa Kagaku, Sumitomo Dainippon and Takeda; grants from Johnson & Johnson, Teijin, Yakult, Kissei, Kowa, Kyowa Hakko Kirin, Pfizer and Taisho Toyama and personal fees from Fujifilm, Terumo and AstraZeneca. IS has received personal fees from MSD during the conduct of the study. His relevant financial activities outside the submitted work are grants and personal fees from Kowa, Novo Nordisk and Takeda; grants from Kobayashi, Daiichi Sankyo, Kyowa Kirin, Mitsubishi Tanabe, Mochida, Rohto, Sanofi, Sumitomo Dainippon and Teijin; and personal fees from Ono, Taisho and Eli Lilly. TK has received honoraria (e.g., lecture fees) from MSD K.K., Takeda Pharmaceutical Co., Ltd., Mitsubishi Tanabe Pharma Corporation, Astellas Pharma Inc., Teijin Pharma Ltd., Ono Pharmaceutical Co., Ltd., AstraZeneca K.K., Sumitomo Dainippon Pharma Co., Ltd., Sanofi K.K., Eli Lilly Japan K.K., Nippon Boehringer Ingelheim Co., Ltd., Novo Nordisk Pharma Ltd., Novartis Pharma K.K., Daiichi Sankyo Co., Ltd., FUJIFILM Toyama Chemical Co., Ltd., Kowa Co., Ltd. and Kyowa Kirin Co., Ltd.; received research grants from Nippon Boehringer Ingelheim Co., Ltd., Eli Lilly Japan K.K., Kyowa Kirin Co., Ltd., MSD K.K., Daiichi Sankyo Co., Ltd., Novo Nordisk Pharma Ltd., Sanofi K.K., Takeda Pharmaceutical Co., Ltd., Astellas Pharma Inc., Ono Pharmaceutical Co., Ltd., Mitsubishi Tanabe Pharma Corporation and Sumitomo Dainippon Pharma Co., Ltd.; received consulting fees from Abbott Japan LLC, Medtronic Japan Co., Ltd. and Novo Nordisk Pharma Ltd. and endowed departments by commercial entities (Asahi Mutual Life Insurance Company).
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.