Article Text

Abstract
Introduction We tested whether normal-weight obesity might be associated with weight trajectories, body composition and metabolic traits.
Research design and methods Body size trajectory since birth, body composition at age 20 years and metabolic traits were compared cross-sectionally among normal-weight Japanese women with low (<25.0%, n=67), normal (25.0–34.9%, n=160) and high (≥35.0 %, n=24) percentage body fat. Multivariate logistic regression analyses were used to identify most important determinants of normal-weight obesity (high percentage body fat).
Results Fasting glucose averaged <84 mg/dL, homeostasis model assessment-insulin resistance <1.4 and triglyceride <70 mg/dL and did not differ among three groups. However, waist and trunk/leg fat ratio were higher, and weight-adjusted skeletal muscle mass was lower in normal-weight obesity. Serum and LDL cholesterol, apolipoprotein B (ApoB) and high-sensitivity C reactive protein were higher, and apolipoprotein A1 was lower in normal-weight obesity compared with the other two groups, whereas HDL cholesterol did not differ. Weight gain from birth to age 12 years was higher in normal-weight obesity. In multivariate logistic regression analyses, weight gain until 12 years (OR: 1.17,95% CI 1.02 to 1.34, p=0.02), ApoB (OR: 1.15, 95% CI 1.06 to 1.24, p<0.001) and weight-adjusted skeletal muscle mass (OR: 0.22, 95% CI 0.10 to 0.49, p<0.001) were associated with normal-weight obesity independently of trunk/leg fat ratio, high-sensitivity C reactive protein and apolipoprotein A1.
Conclusions Normal-weight obesity may be associated with early childhood growth, lower skeletal muscle mass and higher serum ApoB in young Japanese women through mechanisms unrelated to abdominal adiposity, inflammation and insulin resistance.
- Muscle, Skeletal
- Obesity
- Preventive Medicine
- Growth
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Normal-weight obesity has been shown to be associated with high triglyceride and low high-density lipoprotein cholesterol. However, studies evaluating associations with apolipoproteins and growth during childhood are limited.
WHAT THIS STUDY ADDS
Normal-weight obesity was associated with weight gain from birth until 12 years, lower skeletal muscle mass and higher serum apolipoprotein B in young Japanese women.
Theses associations were independent of trunk/leg fat ratio, insulin resistance and high-sensitivity C reactive protein.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Normal-weight obesity may be associated with early childhood growth and increased cardiometabolic risk through mechanisms unrelated to abdominal adiposity, insulin resistance and inflammation in young Japanese women. Our study highlights rapid childhood growth as a risk factor for normal-weight obesity, which is associated with cardiometabolic morbidity and mortality.
Introduction
It is well known that subjects with normal weight (defined as a body mass index (BMI) of 18.5–24.9 kg/m2) have a lower risk for cardiometabolic diseases and all-cause mortality compared with overweight and obese subjects.1 2 As BMI does not differentiate fat-free mass from adipose tissue, an individual with normal weight may have low, appropriate or excess fat. Normal-weight obesity is characterized by the presence of high body fat despite having a normal BMI and is associated with cardiometabolic morbidity and mortality.3 Epidemiological and experimental data indicate that nutritional or environmental stressors during early development can induce long-term adaptations that increase risk of diabetes and cardiovascular disease.4 Altered body composition characterized by increased fat mass and reduced muscle mass is a common phenotype.5 In addition, current evidence suggests that growth and body weight trajectories in infancy and childhood are useful indicators of later obesity and type 2 diabetes.6 As far as we know, however, studies are missing in people with normal-weight obesity.
Most of triglycerides and cholesterol in the circulation are carried in very low-density lipoprotein (VLDL) and low-density lipoprotein (LDL) particles, respectively, both of which contain one molecule of apolipoprotein B (ApoB). ApoB is a single index that quantitates the atherogenic risk due to the ApoB-containing lipoprotein particles.7 Although triglycerides and LDL cholesterol are both risk factors of cardiovascular disease, a study indicates that the clinical benefit of lowering triglyceride and LDL cholesterol levels may be proportional to the absolute change in ApoB.8 Although many studies reported associations of normal-weight obesity with cardiometabolic abnormalities including high triglyceride and LDL cholesterol,3 studies are limited on the association with ApoB.9 10 Age, sex and race/ethnicities may be related to normal-weight obesity.3 We, therefore, studied whether normal-weight obesity may be associated with body weight trajectories since birth to childhood, current body composition, dietary intake and a broad range of cardiometabolic risks including ApoB in young Japanese women in the present study.
Subjects and methods
We reanalyzed cross-sectionally 251 normal weight (BMI: 18.5–24.9 kg/m2) women, whose age and BMI averaged 20.6 years and 20.6 kg/m2, respectively, among 307 young Japanese women whose details were reported previously,11 from which 56 underweight (BMI <18.5 kg/m2) and overweight (BMI: 25.0–29.9 kg/m2) women were excluded. They were students of Department of Food Sciences and Nutrition, Mukogawa Women’s University and were recruited as volunteers. Among 251 women, 181 and 166 women provided data on weight trajectory and dietary intake, respectively. Women with clinically diagnosed acute or chronic inflammatory diseases, endocrine, cardiovascular, hepatic, renal diseases, hormonal contraception, unusual dietary habits were excluded from the study. This research followed the tenets of the Declaration of Helsinki.
Weight at birth, and height and weight at age 12 and 15 years were obtained either through maternal health check notes or child health notebook records (issued by each municipal office).
After a 12-hours overnight fast, participants underwent blood sampling, measurement of anthropometric indices, blood pressure and body composition as previously described.10–14 Blood pressure was measured using an automated sphygmomanometer (BP-203RV II, Colin, Tokyo, Japan) after participants were seated at least for 5 min. Plasma glucose, serum insulin, triglycerides, cholesterol, high-density lipoprotein (HDL) cholesterol, free fatty acid, aspartate aminotransferase (AST), alanine aminotransferase (ALT), γ-glutamyl transpeptidase (GGT), HbA1c and high-sensitivity C reactive protein (hsCRP) were measured as previously reported.10–14 LDL cholesterol was calculated using the Friedewald’s formula. Adipose tissue-insulin resistance index (AT-IR) and homeostasis model assessment-insulin resistance (HOMA-IR) were calculated as previously reported.14 15
Whole-body dual-energy X-ray absorptiometry (DXA) (Hologic QDR-2000 software version 7.20D, Waltham, Massachusetts, USA) was used to measure lean tissue mass, fat mass and bone mineral mass for arms, legs (lower body), trunk and the total body.12 General adiposity was assessed using BMI, percentage body fat (%BF) and fat mass index (FMI), the last of which was calculated as body fat mass in kg divided by height in meter squared. Waist circumference, percentage trunk fat and the ratio of trunk to leg fat16 were considered as markers of abdominal fat accumulation. Muscle characteristics were evaluated by relative appendicular skeletal muscle mass (ASM) as percentage of body mass (%ASM) and absolute ASM index (ASM/height2 in kg/m2). %ASM is suggested to be a better predictor of insulin resistance and diabetes risk than ASM or ASM index.17
There are no clearly established cut points of %BF for normal-weight obesity. A study employing DXA showed that %BF for a BMI of 18.5 and 25.0 kg/m2 corresponded to 25.0% and 35.0%, respectively, in Japanese women aged 20–39 years.18 Similar results were obtained in our analyses in the entire 307 young Japanese women (data not shown). Accordingly, high %BF, that is, normal-weight obesity, was defined by ≥35.0% (n=24, 9.6%). Because a substantial number of normal-weight women (n=67, 26.7%) had %BF <25.0%, they were considered as having low %BF and used as an internal reference. A %BF of 25.0–34.9% was defined as normal (n=160, 63.7%).
Dietary intake of the previous month was assessed using the self-administered diet history questionnaire.19 This has been widely used throughout Japan, and its validity with respect to commonly studied nutrition factors has been confirmed.
Data were presented as mean±SD unless otherwise stated. Due to deviation from normal distribution, hsCRP were logarithmically transformed for analyses. Differences among three groups were analyzed by analysis of variance and then Bonferroni’s multiple comparison procedure. Stepwise multivariate logistic regression analyses were used to identify most important determinants of normal-weight obesity. Independent variables included were variables that showed significant difference among three groups. A two-tailed p<0.05 was considered statistically significant. All calculations were performed with SPSS system V.23.0 (SPSS Inc).
Results
Of 251 normal-weight Japanese women, nobody had metabolic syndrome, and 239 women had none of metabolic syndrome components. There were 11 women who had a single component and a single woman with normal-weight obesity who had two components.
Although BMI and waist increased in a stepwise fashion from the low to high %BF, women with normal-weight obesity had a mean BMI of 22.4 kg/m2, waist 78.6 cm and ALT 13 U/L (tables 1 and 2). Fasting glucose averaged <84 mg/dL, HbA1c <5.3% and triglyceride <70 mg/dL and did not differ among three groups (table 2).
Weight trajectories since birth and current body composition in young, normal-weight Japanese women with low, normal and high percentage body fat
Cardiometabolic risk factors in young, normal-weight Japanese women with low, normal and high percentage body fat
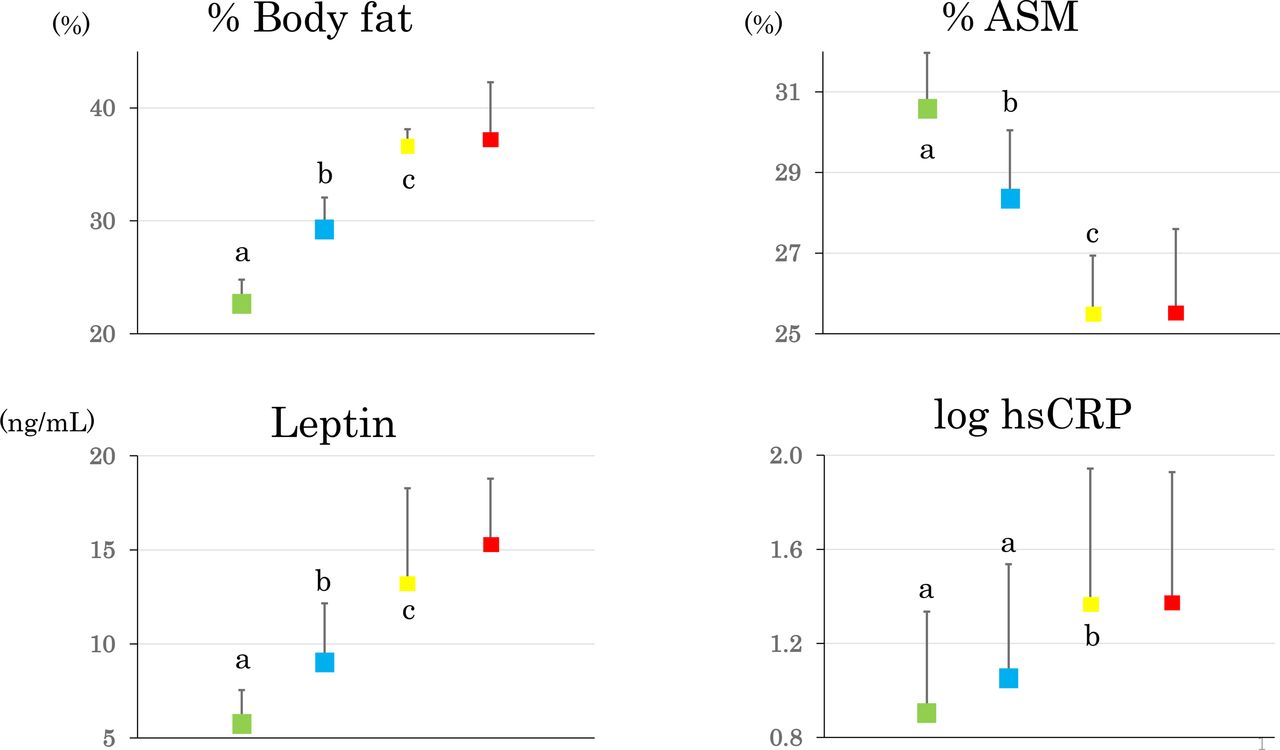
There was no difference in birth weight (table 1). However, weight at 12, 15 and 20 years was higher in normal and high compared with low %BF group. Therefore, weight gain until 12 years was higher in women with normal and high compared with low %BF. There were no or modest differences in height. Percentage trunk fat, trunk/leg fat ratio and fat mass index increased and %ASM decreased in a stepwise fashion from the low through the high %BF although there was no difference in ASM index (table 1 and figure 1).

Percentage body fat (% body fat), weight-adjusted appendicular skeletal muscle mass (% ASM), serum leptin and high-sensitivity C reactive protein (logarithmically transformed, log hsCRP) in young, normal-weight Japanese women with the low (green squares, n=67), normal (blue squares, n=160) and high percentage body fat (yellow squares, n=24), the last of which represent normal-weight obesity. Red squares are results of 14 overweight women.11 Mean±SD means not sharing common letter are significantly different with each other at p<0.05 or less by Bonferroni’s multiple comparison procedure. #P<0.05 versus normal-weight obesity. hsCRP, high-sensitivity C reactive protein.
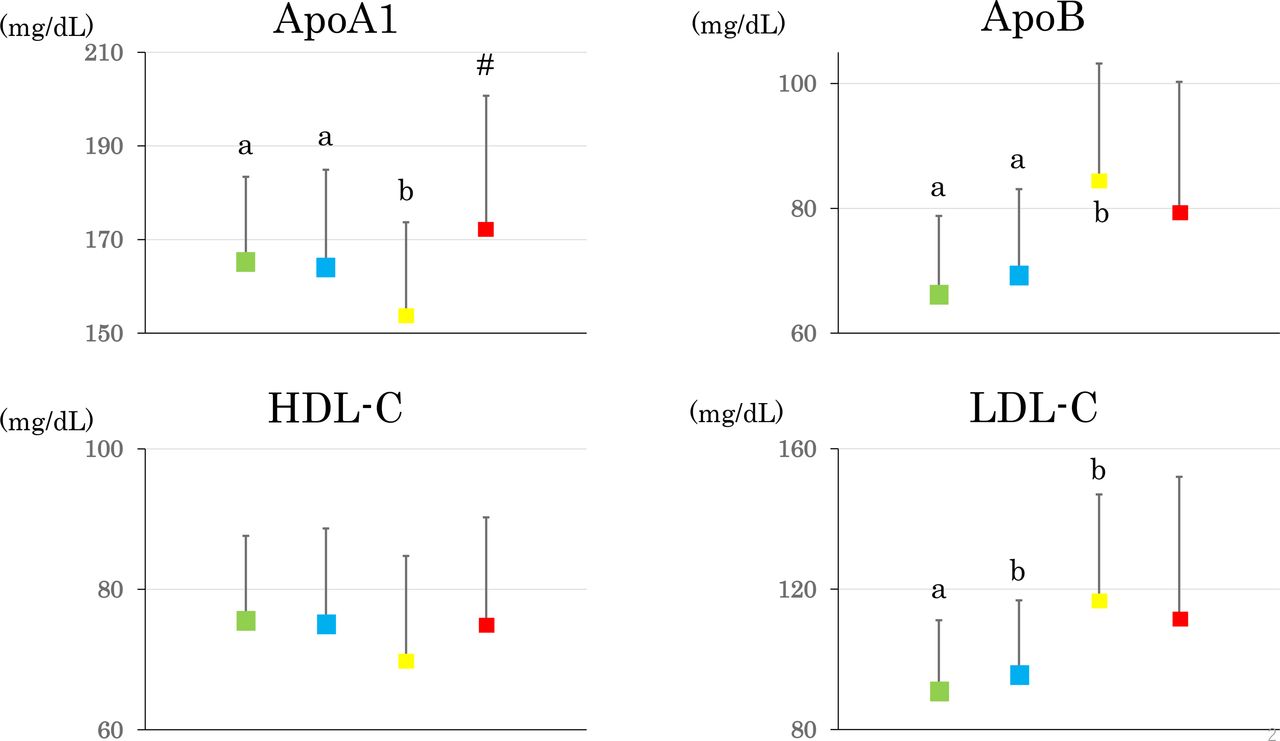
Despite remarkable differences in trunk/leg fat ratio, %BF and %ASM, there was no difference in HOMA-IR, AT-IR and adiponectin (table 2). Serum and LDL cholesterol, ApoB and hsCRP were higher and ApoA1 was lower in normal-weight obesity compared with the other two groups whereas HDL cholesterol did not differ (figures 1 and 2).

{kind=link}
{kind=link}
Serum apolipoprotein A1 and B (ApoA1 and ApoB, respectively), high-density and low-density lipoprotein cholesterol (HDL-C and LDL-C, respectively) in young, normal-weight Japanese women with the low (green squares, n=67), normal (blue squares, n=160) and high percentage body fat (yellow squares, n=24), the last of which represent normal-weight obesity. Red squares are results of 14 overweight women.11 Mean±SD means not sharing common letter are significantly different with each other at p<0.05 or less by Bonferroni’s multiple comparison procedure. #P<0.05 versus normal-weight obesity.
There was no difference in daily energy intake and macronutrients among normal-weight women with low, normal and high %BF (online supplemental table 1).
Supplemental material
It is noteworthy that normal-weight obese women were comparable to overweight women whose BMI averaged 26.6 kg/m211 in % BF, %ASM, serum leptin, log hsCRP, ApoB and LDL cholesterol (figures 1 and 2). ApoA1 concentrations were lower in normal-weight obese compared with overweight women (figure 2). Similarly, normal-weight women with low %BF were comparable with underweight women whose BMI averaged 17.5 kg/m211 in % BF (22.9 v. 21.5 %) and %ASM (30.6 v. 30.8 %).
In multivariate logistic regression analyses (table 3), weight gain until 12 years, ApoB and %ASM were associated with normal-weight obesity independently of trunk/leg fat ratio, ApoA1 and hsCRP.
Multivariable logistic regression analyses for normal-weight obesity
When Asian-specific cut-offs of BMI definitions for normal weight (18.5–22.9 kg/m2) was applied (online supplemental table 2), only 13 women (5.6 %) had high %BF among 232 normal-weight women. However, results were similar to those in tables 1 and 2: higher weight gain from birth to age 12 years, waist, % trunk ratio, serum and LDL cholesterol, ApoB and hsCRP and lower %ASM in women with high %BF.
Discussion
The current study confirmed associations of normal-weight obesity with abdominal fat accumulation and low muscle mass as previously reviewed3 and demonstrated that normal-weight obesity was associated with early childhood growth and higher serum ApoB in young, normal-weight Japanese women. These associations were independent of trunk/leg fat ratio, sophisticated measures of abdominal fat accumulation and hsCRP, a marker of chronic systemic low-grade inflammation. It is noteworthy that fasting insulin, HOMA-IR and AT-IR did not differ among three groups of women despite remarkable differences in %BF, trunk/leg fat ratio and percentage trunk fat, the last of which has been shown to be associated with increased risk of cardiovascular disease in postmenopausal women with normal BMI.20 In addition, waist and ALT averaged 78.6 cm and 13 U/L, respectively, in women with normal-weight obesity, suggesting a minimum abdominal and hepatic fat accumulation, respectively.
Multiple studies showed associations of normal-weight obesity with dyslipidemia including high triglyceride and LDL cholesterol and low HDL cholesterol in adolescents and adults.3 21 However, we found only two studies on the association with ApoB.9 10 Swedish middle-aged people with normal-weight obesity had higher waist and ApoB compared with the normal weight leanness group, whereas ApoA1 did not differ.9 The second study showed associations of ApoB with %BF and HOMA-IR in young India subjects with normal-weight obesity.10 In the present study, ApoB not ApoA1 showed associations with normal-weight obesity independent of abdominal adiposity and insulin resistance although ApoA1 was lower in normal weight obese compared with overweight women.
Fat storage increase in response to positive energy balance and/or disturbances in pathways of lipolysis in adipose tissue.22 A reduced catecholamine-induced lipolysis may contribute to the development and maintenance of increased adipose tissue stores. A number of studies suggest that there is lipolytic resistance to catecholamines in subcutaneous adipose tissue in obese subjects.22 Skogsberg et al studied the effects of ApoB-containing lipoproteins on catecholamine-induced lipolysis in adipocytes from subcutaneous fat cells of obese men, fat pads from mice with plasma lipoproteins containing high or intermediate levels of ApoB100 or no ApoB100, primary cultured adipocytes and 3T3-L1 cells.23 They showed that the binding of ApoB in LDL particles to LDL receptors on cell membrane of adipocytes inhibits intracellular noradrenaline-induced lipolysis in adipocytes. We speculate that because daily energy intake did not differ among three groups of women, decreased lipolysis associated with higher ApoB may be related to higher %BF in normal-weight Japanese women in the present study. We found associations of ApoB not only with %BF and FMI but with leptin, adiponectin (inversely) and hence leptin/adiponectin ratio, the last of which represents a marker of compromised adipocyte function,24 in non-obese young female university students and their middle-aged parents (paper in preparation).
Elevated ApoB may be a component of the metabolic syndrome,25 and higher ApoB in VLDL and LDL particles have been reported to occur in the early phase of insulin resistant women with abdominal obesity who had normal fasting glucose and triglyceride levels.26 A recent Mendelian randomization study showed that genetically higher body fat percentage had a causal effect on ApoB.27 Higher serum ApoB was explained by increased synthesis of ApoB and large VLDI by the liver and impaired lipolysis of VLDL and increased residence time in the circulation, both of which resulted from increased visceral adipose tissue and insulin resistance.27 However, association between ApoB and normal-weight obesity in young women was independent of abdominal fat accumulation and insulin resistance.
Nutritional or environmental stressors during fetal life and infancy may be associated with increased fat mass and reduced muscle mass in later life,5 a phenotype seen in women with normal-weight obesity in the present study. However, birth weight was not associated with normal-weight obesity in Japanese women. Instead, early childhood growth (weight gain since birth to age 12 years) was associated with normal-weight obesity in the present study. This may be in line with the study by Zhang et al,28 who found strong associations between the metabolic markers measured at 11.5 years of age and three growth measures (ages 3–12 months, ages 12 months-6.5 years and ages 6.5–11.5 years), with the largest magnitudes being observed during the latest age period (ages 6.5–11.5 years). To the best of our knowledge, the current study may be the first to demonstrate an association of childhood growth with normal-weight obesity.
The accurate and reliable measures of general and central fat accumulation by DXA are the strength of the present study. There are several limitations of this study including the cross-sectional design, relatively small sample size and a single measurement of biochemical variables. The notion that ApoB inhibits intracellular noradrenaline-induced lipolysis in adipocytes is presently supported by a single publication only.23 However, multiple studies reported the relation of elevated ApoB to white adipose tissue dysfunction.29–33 The study population included only female university students. However, this also might be considered as a strength since it eliminates potential confounding factors.12 For example, more than 90% of grade 1 students are 18 years old. This may decrease the interference of age and environmental factors, including smoking, alcohol, educational and socioeconomic status. Furthermore, in almost all students, almost all school expenses were covered by parents, suggesting that socioeconomic status appears to be less heterogeneous among parents who fed participants of the present study. We did not assess family history of obesity and current exercise habits. However, participants had 9367±1971 steps/day (mean±SD of 77 participants, who used a pedometer for 14 days, and the mean steps a day were calculated for each participant), although they were not engaged in any regular sport activity. We did not measure sex hormones. Statistical power and sample size were not calculated. As participants were young Japanese women, the results may not be generalized to other gender, age populations, races or ethnicities.
In conclusion, normal-weight obesity may be associated with early childhood growth, lower skeletal muscle mass and higher serum ApoB in young Japanese women through mechanisms unrelated to abdominal adiposity, insulin resistance and inflammation. Our study highlights rapid childhood growth as a risk factor for normal-weight obesity, which is associated with cardiometabolic morbidity and mortality. Prospective follow-up studies are needed to see if these phenotypes predict clinical outcomes (ie, development of diabetes or cardiovascular disease).
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the Ethics Committees of Mukogawa Women’s University (No. 07-28 on 19/02/2008). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We would like to thank all participants for their dedicated and conscientious collaboration.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors SM-I, AH, MH and AT-K collected data and prepared figures. MT, KK, MK and BW analyzed data and prepared tables. TK wrote the manuscript, and KF reviewed and edited it. All authors approved the final version of the manuscript to be published. TK supervised the study, had full access to all thedata in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.