Article Text

Abstract
Metformin is considered as first-line treatment for type 2 diabetes and an effective treatment for polycystic ovary syndrome (PCOS). However, evidence regarding its safety in pregnancy is limited. We conducted a systematic review and meta-analysis of major congenital malformations (MCMs) risk after first-trimester exposure to metformin in women with PCOS and pregestational diabetes mellitus (PGDM). Randomized controlled trials (RCTs) and observational cohort studies with a control group investigating risk of MCM after first-trimester pregnancy exposure to metformin were searched until December 2021. ORs and 95% CIs were calculated separately according to indications and study type using Mantel-Haenszel method; outcome data were combined using random-effects model. Eleven studies (two RCTs; nine observational cohorts) met the inclusion criteria: four included pregnant women with PCOS, four included those with PGDM and three evaluated both indications separately and were considered in both indication groups. In PCOS group, there were two RCTs (57 exposed, 52 control infants) and five observational studies (472 exposed, 1892 control infants); point estimates for MCM rates in RCTs and observational studies were OR 0.93 (95% CI 0.09 to 9.21) (I2=0%; Q test=0.31; p value=0.58) and OR 1.35 (95% CI 0.37 to 4.90) (I2=65%; Q test=9.43; p value=0.05), respectively. In PGDM group, all seven studies were observational (1122 exposed, 1851 control infants); the point estimate for MCM rates was OR 1.05 (95% CI 0.50 to 2.18) (I2=59%; Q test=16.34; p value=0.01). Metformin use in first-trimester pregnancy in women with PCOS or PGDM do not meaningfully increase the MCM risk overall. However, further studies are needed to characterize residual safety concerns.
- Metformin
- Pregnancy
- Polycystic Ovary Syndrome
- Type 2 Diabetes
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Metformin belongs to the biguanide class of glucose-lowering medications, and the mechanism of its antihyperglycemic effect is mainly by suppressing hepatic glucose production1–4; it is generally weight neutral with chronic use and does not increase the hypoglycemia risk.5 Metformin features as the most widely used and current first-line pharmacological treatment for type 2 diabetes mellitus (T2DM) in the general population worldwide.3 6 Furthermore, metformin is considered as an alternative to insulin therapy for gestational diabetes mellitus (GDM).7–11 It is increasingly being used in the GDM indication as it has been shown to be a safe and effective alternative to insulin with respect to pregnancy outcomes12 13; it controls glycemia and prevents adverse maternal and neonatal outcomes associated with hyperglycemia; and notably, insulin resistance can be dealt more effectively with metformin.10 14–16 Metformin is also commonly used for polycystic ovary syndrome (PCOS) associated infertility, a condition affecting 4%–20% of women of reproductive age worldwide.17 However, evidence on safety and effectiveness to achieve glycemic targets in the treatment of pregestational diabetes mellitus (PGDM) in early pregnancy is still limited.18 19
Metformin freely crosses the placental barrier12 20; this has caused concerns regarding metformin exposure during the first trimester of pregnancy and its effect on embryological and fetal development.12 21 There is no signal of any major teratogenic effect of metformin neither in animal studies22 23 nor in few available studies in humans24–26 as available data show no association with congenital malformations after exposure in the first trimester.27 28 A meta-analysis performed in 2014 did not detect an increase in risk of major malformations after metformin use in pregnant women with PCOS.25 The authors also aimed to analyze the risk of major congenital malformations (MCMs) after maternal metformin intake for T2DM; however, due to the insufficient number of studies, it was not feasible. Of interest, several studies investigating the pregnancy outcomes after metformin use during early pregnancy were published after this meta-analysis, which may allow for a meta-analytic synthesis.29–35
To better characterize the safety of metformin after its use in the first trimester of pregnancy, this study aims to systematically assess whether first-trimester exposure to metformin is associated with an increased risk of MCM using a meta-analytic approach.
Methods
Search strategy
Searches were conducted by two qualified librarians (CJ and BMW) from the Universities of Lausanne and Bern and the study authors in Medline (Ovid), Embase.com, Cochrane Central Register of Controlled Trials, ClinicalTrials.gov, WHO ICTRP, Web of Science Core Collection and Google Scholar from inception to 10 December 2021. The full search strategies for all databases are available in online supplemental table 1. A manual search including backward and forward citation tracking was held through the reference list of the included studies to identify other potentially eligible studies. The reporting of this systematic review was prepared in compliance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses.36 Findings were reported in adherence with the Meta-Analysis of Observational Studies in Epidemiology guidelines.37 There were no date limitations.
Supplemental material
Eligibility criteria
Studies were selected when they met the following criteria: randomized controlled studies (RCTs) and observational cohort studies with a control group (no teratogenic treatment or no treatment or insulin) investigating MCM after maternal use of metformin in early pregnancy (ie, from 2 to 10 weeks after the last menstrual period). Only studies with first trimester exposure were considered. Case–control studies, case reports and series, animal studies, editorials and reviews were excluded. Only published studies in English were included.
Outcome measures
The main outcome of interest for this meta-analysis were MCM overall. If the malformations reported by the studies were not classified, study authors classified them using the Malformation Coding Guides of European Surveillance of Congenital Anomalies (EUROCAT)38 39 as major and minor for exclusion. JRC-EUROCAT Central Registry was consulted in cases of any disagreement among the authors regarding the classification. The secondary outcome of interest was the subgroup of cardiovascular malformations (eg, transposition of the great arteries and truncus arteriosus).
Study selection, data extraction and assessment of the risk of bias
Two reviewers (NA and UW) independently reviewed the studies using the Rayyan software (https://www.rayyan.ai) in a two-step process. First, the extracted articles were reviewed and selected by title and abstract. The first step selected papers were reviewed and selected by full paper read. We extracted the data using a standardized data extraction form in Excel as follows: main study author(s) and publication year, country, period and design of study, patients, metformin exposure and control group, number and demographics of participants (age and body mass index), total number of live births and MCM in metformin-exposed and control group. Any disagreement was discussed and resolved by consultation with another author (AP and YCK). For observational studies, we aimed to extract adjusted ORs; however, an adjusted result was reported for one study only.
For randomized studies, the risk of bias of each included study was assessed using the criteria of the Cochrane Collaboration.40 These include random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data and selective outcome reporting. The risk of bias was judged on each criterion as ‘low’, ‘high’ or ‘unclear’. Incomplete outcome data were judged as having low risk of bias when numbers and reasons of dropouts were balanced (ie, in the absence of a significant difference) between arms. Two reviewers assessed the risk of bias of each study independently and resolved disagreements by discussion to reach consensus. For prospective observational studies, the Newcastle-Ottawa scale for quality assessment of the study methodologies was used.41 The reviewers were not blinded to the author names, institutions, results or journals of the publications.
Statistical analysis
The included studies were analyzed separately based on the indications, that is, PCOS and PGDM; in addition, within the PCOS indication group, the analysis were done separately per design of studies (RCTs and observational studies). ORs and 95% CIs were calculated using Mantel-Haenszel method, and outcome data were combined using a random-effects model. For observational studies, we aimed to combine adjusted ORs. However, we found only one study that reported the adjusted OR, and this was similar to the no-adjusted one. All the other studies reported the absolute number of participants with the event in each group. Therefore, we decided to combine the latter data. Heterogeneity was assessed using the Q and I2 statistic and by visual inspection of the forest plots. An I2 value between 25% and 50% was considered as low heterogeneity, between 50% and 75% moderate and >75% high heterogeneity.42 Statistical analyses were conducted in STATA (StataCorp). The confidence of evidence generated by studies was assessed via the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach (www.gradeworkinggroup.org). For PCOS we assessed GRADE in only RCTs.
Consent and ethics committee
Consent and ethics committee approval was not needed since this study is a systematic review and meta-analysis of the available data.
Results
The selection process of studies fulfilling the inclusion criteria for the meta-analysis is shown in online supplemental figure 1. Out of 3783 records initially identified by database and trial register searching, a total of 11 studies were eventually included in the review and meta-analysis: two RCTs43 44 and nine observational studies.29 31 35 45–50 The details of included studies and characteristics of the studies participants are presented in tables 1 and 2. Quality assessments of the included studies conducted separately based on the study design are presented in online supplemental figure 2 and table 2. Observational studies obtained a quality score from 5 to 8 out of 9, and the overall risk of bias of the included RCTs was low. Out of the 11 included studies, four included only pregnant women with PCOS, four others only pregnant women with PGDM and three evaluated both indications separately, and we used these three studies in both indication groups accordingly. Regarding the certainty of evidence, the results of GRADE assessment, done separately per studies on PCOS and PGDM indications, showed overall low and very low certainty, respectively (online supplemental table 3). Due to the low number of reported malformations, the analysis of the secondary outcome of interest (ie, subgroups of cardiovascular malformations) was not feasible. Also, as the number of included studies was less than 10 in each set of analysis, we could not use funnel plot to assess publication bias and small study effect.51
Characteristics of included studies
Characteristics of the studies participants
Studies on pregnant women with PCOS
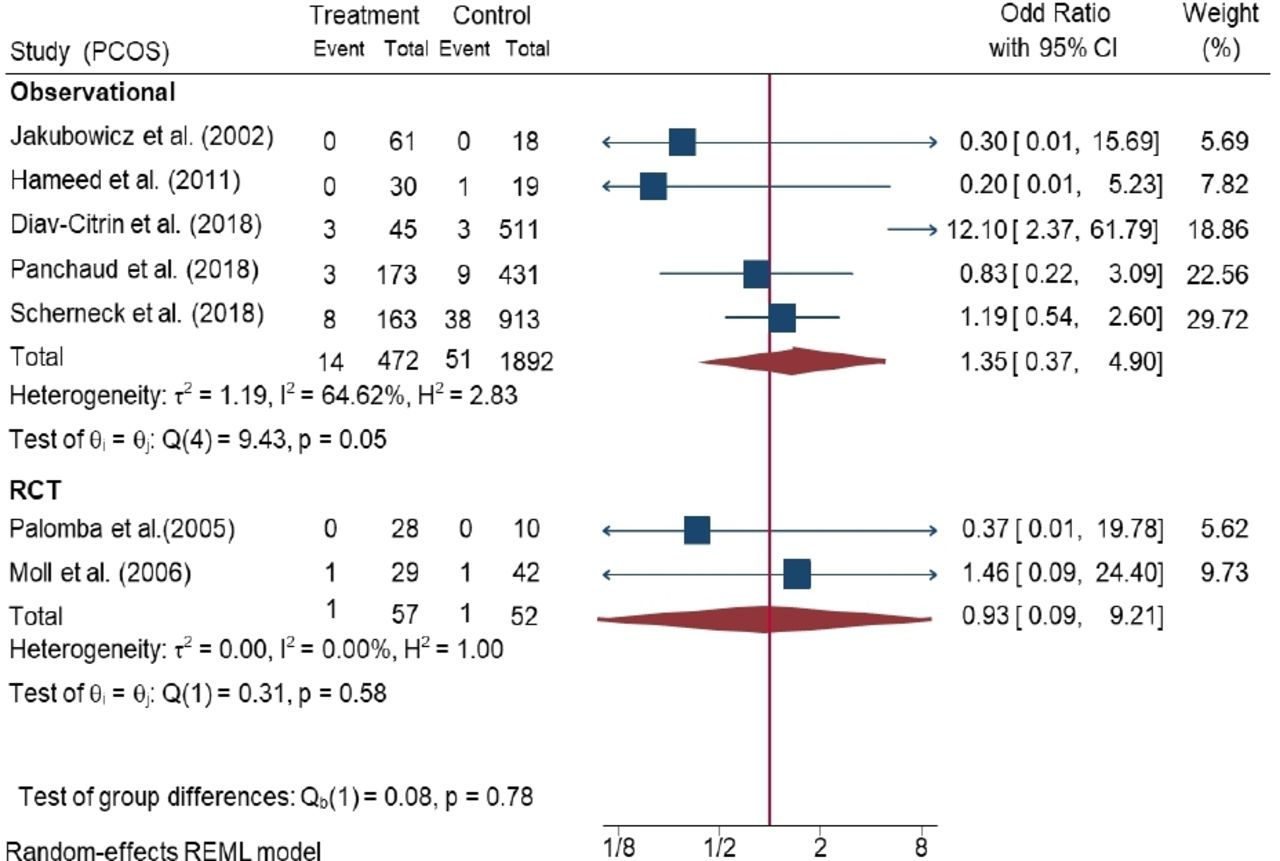
Meta-analysis of overall MCM rates in metformin-exposed women with PCOS is presented in figure 1. Out of the seven studies with PCOS indication, there were two RCTs (with a total of 57 exposed and 52 control infants) and five observational studies (with a total of 472 exposed and 1892 control infants). The point estimate for the rates of MCM in RCTs and observational studies were OR 0.93 (95% CI 0.09 to 9.21) with I2 of 0% (Q test=0.31; p value=0.58) and OR 1.35 (95% CI 0.37 to 4.90), with I2 of 65% (Q test=9.43; p value=0.05), respectively.
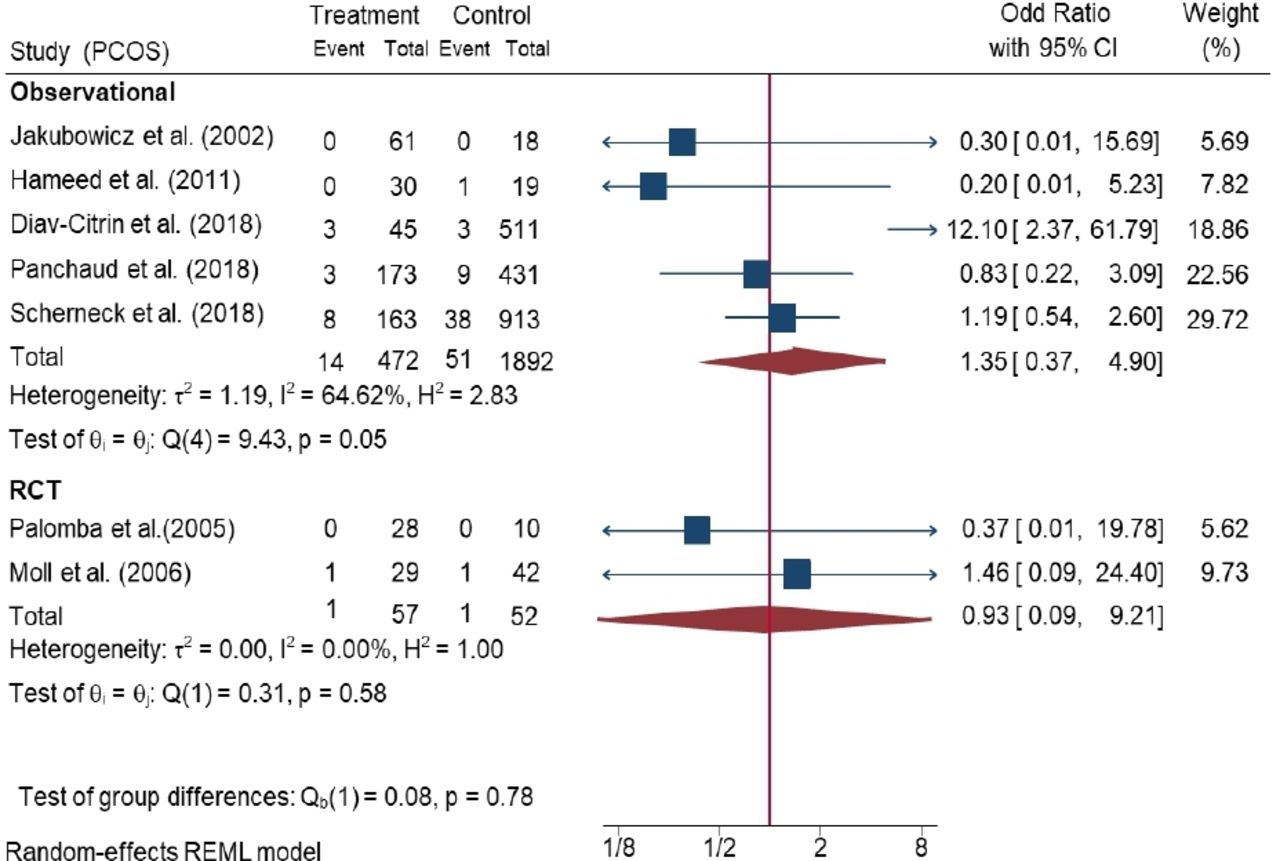
Meta-analysis of overall major congenital malformation (MCM) rates in metformin-exposed women with polycystic ovary syndrome (PCOS).
Studies on pregnant women with PGDM
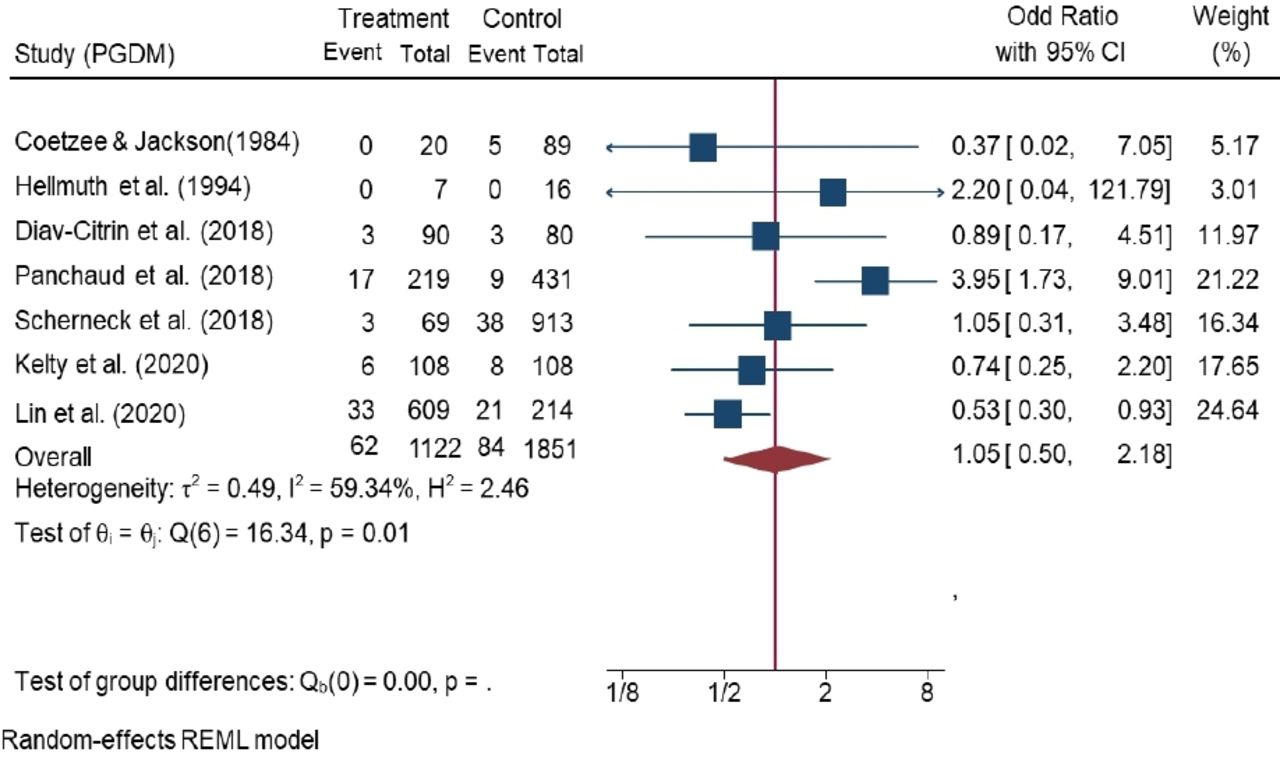
Meta-analysis of overall MCM rates in metformin-exposed women with PGDM is presented in figure 2. Seven observational studies with a total of 1122 exposed and 1851 control infants were pooled. The point estimate for the rates of MCM was OR 1.05 (95% CI 0.50 to 2.18) with I2 of 59% (Q test=16.34; p value=0.01).
{kind=link}
{kind=link}
Meta-analysis of overall major congenital malformation (MCM) rates in metformin-exposed women with pregestational diabetes mellitus (PGDM).
Discussion
Based on the 11 included studies, metformin use during first trimester of pregnancy for PCOS and PGDM does not seem to significantly increase the risk of MCM. However, currently, more specific safety concerns including limited increased risks of specific congenital malformations such as cardiovascular birth defects cannot be ruled out because of a lack of data.
A previous systematic review and meta-analysis of nine controlled studies on women with PCOS showed that the rate of major birth defects in the metformin exposed group was not statistically increased compared with the disease-matched control group. This study involved 351 pregnancies in women exposed to metformin in utero and 178 pregnancies in women not exposed to metformin in utero and the OR of major birth defects was 0.86 (95% CI 0.18 to 4.08).25 Due to small total sample size, this study failed to perform a meta-analysis on few studies reporting information on birth defect rate in PGDM women exposed to metformin during the first trimester of pregnancy. Another systematic review and meta-analysis of eight studies observed similar results with respect to major malformations. The OR for major malformations (including all studies with disease-matched controls) was 0.50 (95% CI 0.15 to 1.60).24 This study also separated the analysis based on the PCOS and PGDM indications and reported the OR for PCOS as 0.33 (95% CI 0.07 to 1.56) and for PGDM as 0.85 (95% CI 0.14 to 5.11).
There is a paucity of information on metformin exposure in early pregnancy and the risk of MCM in the literature. Regarding the design of studies, the relevant information are mainly provided by observational studies as pregnant women have been historically excluded from RCTs.52 For PGDM, there is limited number of studies as women are usually switched to insulin as a first choice treatment as soon as pregnancy is diagnosed because insulin does not cross the placenta.53 For PCOS, metformin is likely to be discontinued as soon as a diagnosis of pregnancy is confirmed,54 which is often done very early on in patients with this condition, and associated to a limited exposure to metformin in the first trimester, and thus patients with PCOS are most often not eligible for safety studies. This may explain the wide CI of OR for RCTs in our study, which is due to the very small number of events per arm over a small number of total sample size (ranging from 10 to 28 participants per arm). In addition, the studies on PCOS mainly focus on the ovulation and pregnancy rate and do not offer follow-up information until birth, which makes them ineligible to assess outcomes such as the risk of malformation. Thus, further larger studies are needed to address the safety of metformin first trimester exposure in pregnancy on longer term pregnancy outcomes such as MCM.
Poorly controlled pregestational diabetes is associated to an increased risk of major malformation ranging from 5% to 10% in live births (ie, baseline risk being 2%–4%).55 The control of PGDM, in itself, is of paramount importance as proper metabolic control maintained throughout the first trimester of pregnancy can significantly reduce the malformation risk.55 56 Such association makes it difficult to disentangle the effect of the underlying disease from the effect of metformin on any observed increased risk in most of the available safety studies without information on the level of control of the disease. This confounding by the underlying diabetes was illustrated in a previous observational study in which, after stratification, the risk of major malformation was 10% in PGDM pregnancies with at least one severity criterion for diabetes (ie, presence of any abnormal glucose test or concomitant use of other oral diabetic drugs or insulin), whereas it was similar in the reference group of patients not exposed to metformin (2.1%) and in those exposed to metformin for indications other than PGDM (1.7%).35
Strengths and limitations
We adopted a rigorous search strategy, and this meta-analysis is the most comprehensive and updated quantitative synthesis of the safety of metformin in terms of MCM after early pregnancy exposure. Since previous most recent meta-analysis, five additional studies were extracted and included for current meta-analysis.29 31 35 49 50 Out of these five studies, three had data on both PCOS and PGDM indications.29 31 35 Furthermore, we provided results of the quality assessments of the included studies separately based on the study design as well as the confidence of evidence generated by RCTs using the GRADE approach, which was not the case in the previous studies. Nonetheless, this meta-analysis is limited by the quality and quantity of included studies coupled with the small sample size and number of events. In addition, due to indication bias, safety assessment of metformin in PCOS and PGDM is complex as the disease itself is associated with an increased congenital malformation risk that makes it difficult to disentangle the effect of the drug from the effect of the disease.57–59
In conclusion, evidence from this meta-analysis suggests that the use of metformin in first trimester of pregnancy in women with PCOS or PGDM do not meaningfully increase the risk of congenital malformations overall. However, further larger studies are needed to characterize more specifically residual safety concerns after metformin exposure in the first trimester.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors AP, YCK and UW conceived the initial research project. CJ and BMW conducted the literature search. NA and UW independently reviewed the studies in a two steps process, extracted and selected articles. The disagreements were discussed and resolved by consulting with other coauthors (AP and YCK). NA performed the statistical analysis supervised by CDG. NA wrote the first draft of the manuscript. All authors critically revised the manuscript and approved the final version.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.