Article Text

Abstract
Introduction New glucose-monitoring technologies have different cost–benefit profiles compared with traditional finger-prick tests, resulting in a preference-sensitive situation for patients. This study aimed to assess the relative value adults with diabetes assign to device attributes in two countries.
Research design and methods Adults with type 1 or 2 diabetes from the Netherlands (n=226) and Poland (n=261) completed an online discrete choice experiment. Respondents choose between hypothetical glucose monitors described using seven attributes: precision, effort to check, number of finger pricks required, risk of skin irritation, information provided, alarm function and out-of-pocket costs. Panel mixed logit models were used to determine attribute relative importance and to calculate expected uptake rates and willingness to pay (WTP).
Results The most important attribute for both countries was monthly out-of-pocket costs. Polish respondents were more likely than Dutch respondents to choose a glucose-monitoring device over a standard finger prick and had higher WTP for a device. Dutch respondents had higher WTP for device improvements in an effort to check and reduce the number of finger pricks a device requires.
Conclusion Costs are the primary concern of patients in both countries when choosing a glucose monitor and would likely hamper real-world uptake. The costs-benefit profiles of such devices should be critically reviewed.
- patient-centered care
- blood glucose self-monitoring
- economics
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Previous research identified factors that patients with diabetes find important when choosing a glucose monitor for self-management of their diabetes. These studies did not assess the relative importance of these factors or were only conducted in samples of type 1 diabetes mellitus (T1DM), limiting how these findings can be applied.
WHAT THIS STUDY ADDS
This study identified out-of-pocket costs as the most important factor for both patients with T1DM and type 2 diabetes mellitus in two countries and quantified that these costs are 5–50 times more important than any other factor.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Regulators and policy makers can incorporate this patient preference information into decision making to develop diabetes care management strategies that are not only cost-efficient but also based on patient values.
Introduction
Diabetes is a chronic disease characterized by the body’s inability to maintain healthy levels of blood glucose, which is associated with long-term health problems including an increased risk of mortality with an estimated global prevalence of 10.5% in 2021.1–3 Diabetes care is centered around the cornerstone of metabolic control, specifically keeping glucose levels as close to normal as possible through medication, a careful diet, physical activity and self-monitoring of blood glucose (SMBG).4 5 SMBG has traditionally been done using the finger-prick test and is associated with improvements in glycemic control.6 While highly accurate,7 this technique represents a large burden to patients, which can result in non-compliance to medical treatment advice.8–10 Studies examining the adherence of patients to SMBG regimens report adherence rates ranging from 88% in Australia11 to as low as 44% in Sweden,12 26% in the USA13 and 20% in Hungary.14 These low adherence rates are related to barriers to the practice of SMBG including low socioeconomic status (SES), fear of testing and fingertip pain, distressing emotions and thoughts, frustration about ‘poor’ blood glucose reading, lack of awareness of hypoglycemia and hyperglycemia, lack of social support and difficulty in interpreting SMBG results.15
Recent technological developments have resulted in commercially available medical devices which can (semi-)continuously monitor blood glucose levels (or proxies thereof).16 17 These devices are often less invasive, quicker and easier to use, and can give more detailed daily blood glucose-level information by showing trends over time compared with SMBG with finger pricking.18–20 However, these devices vary in regard to functionality and features including (but not limited to) differences in accuracy, size, battery requirements, range of transmitter, calibration requirements, scanning procedures and longevity (replacement time). Further, these devices are often not reimbursed through insurance plans and can have high out-of-pocket costs for the patient.21 The differences in function, features and costs have resulted in a situation where personal preferences may guide the choice of device used for SMBG.
Despite growing interest in patient preference assessment, limited research has been done quantifying patient preferences for glucose monitors. Hannah et al found that for patients with type 1 diabetes (T1DM), the most important factors for choosing a continuous glucose monitor (CGM) were method of data retrieval, longer sensor wear time with more adhesive durability, and personalized alerts and alarms.22 Engler et al found that the reasons related to stopping CGM usage for patients with T1DM were poor accuracy due to lag times, insurance reimbursement or cost, comfort and false alarms.18 They also found that for patients with T1DM without CGM experience cost, having a device attached to the body and expectations of discomfort in wearing were primary reasons for not using a CGM for SMBG.18 Both studies highlight the preference-sensitive nature of these devices; however, neither included patients with type 2 diabetes mellitus (T2DM), a growing population of patients who may need to monitor their blood glucose.19 20 23 Further, only Hannah et al22 used a method of relative valuation to show how important these attributes were in regard to each other but did not include a cost attribute, which is a major concern for many patients. There is thus a gap in knowledge regarding the relative valuation information that regulatory authorities and decision makers use to guide policies for medical treatments.24 This study aimed to fill that gap by quantitatively assessing the factors that patients with T1DM and T2DM consider important when choosing a glucose-monitoring device for SMBG and identify willingness to pay (WTP) and expected device uptake rates.
Materials and methods
Subjects
Participants were recruited from the Netherlands and Poland through a professional panel provider (SurveyEngine). These countries were chosen as costs were expected to play an important role in deciding between devices, and these two countries had partial and no reimbursement of glucose monitors for SMBG at the time of data collection (respectively). To be eligible to complete the survey, patients had to have a self-reported diagnosis of T1DM or T2DM, reside in the Netherlands or Poland, be over 18 years of age, be able to read and understand Dutch or Polish, and have access to a computer.
Discrete choice experiment (DCE)
A DCE was used to quantify patient preferences.25 26 DCEs are based on random utility theory, which assumes that the utility or value of a healthcare alternative can be derived through the compound valuation of the different attributes and attribute levels used to describe the treatment alternative.27–29 In a DCE, respondents are presented with choice tasks in which they chose their preferred option from two or more alternative treatment profiles. These alternative profiles describe treatments using a set of characteristics (called attributes) with varying levels, representing realistic values of these attributes.30 31 Patients choose the alternative which represents the highest personal utility based on the personal value they attach to the different levels of attributes used to describe the alternative. After a patient completes the DCE, attribute estimates can be generated using econometric models and the relative importance of the included attributes can be inferred from these estimates.32–34
Attributes and levels
The attributes and levels used in this DCE were developed according to best practices using a stepwise, qualitative approach from April 2019 to October 2019.35 36 This approach started with a scoping literature review of articles describing aspects relevant to patients in using glucose-monitoring devices. The results of this review were used to create an interview guide (see online supplemental material) which was used in semistructured interviews with patients with T1DM and T2DM from the Netherlands (n=9), clinical diabetes experts (n=5), patient organization representatives (n=2) and pharmaceutical industry representatives involved in glucose-monitoring device development (n=4), as well as a focus group with patients with T1DM and T2DM in Poland (n=10). This process generated a list of 12 potentially relevant attributes which was reviewed and reduced by the research team to ensure relevance according to the interviewees, non-redundancy and operationality to a final list of 7 attributes for use in the DCE. The levels used to describe the attributes were developed based on the literature review and interviews and were chosen to be realistic and reflect the most common types of commercially available glucose monitors, including CGMs and flash glucose monitors (FGMs).37–40 One attribute (‘out-of-pocket costs’) was standardized between the two countries using purchasing power parity weights to ensure that the relative value of the levels was similar, given the differences in wealth between the two countries.41 The final list of attributes and levels used in the DCE can be found in table 1.
Supplemental material
Supplemental material
Attributes and levels for the discrete choice experiment
Experimental design
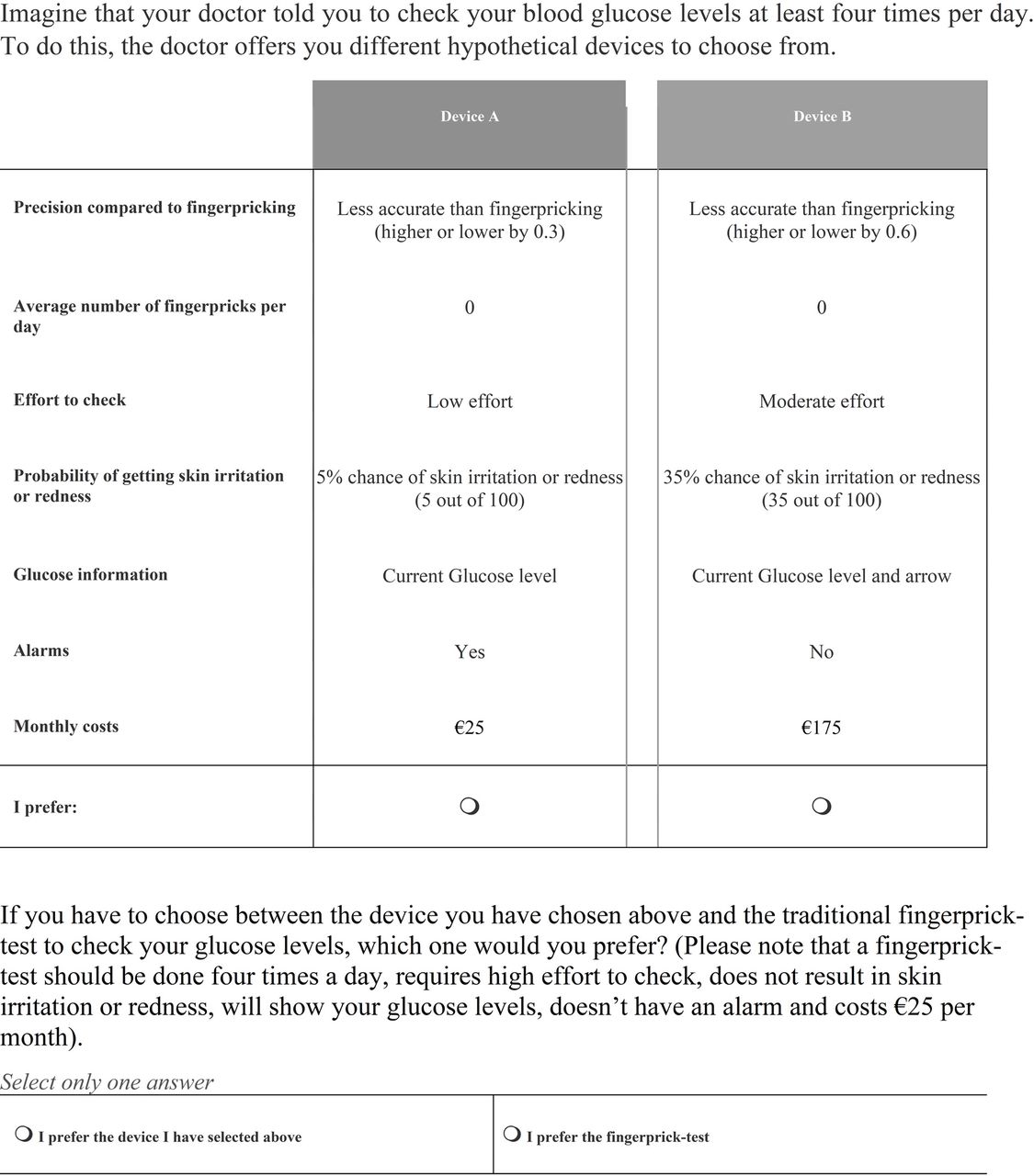
The DCE was developed using an efficient design (Bayesian D-efficient design42 43) generated in NGene V.1.0 software. This allows for participants to complete a minimal amount of choice tasks (3 blocks of n=12 choice tasks each) while maximizing the amount of information each task generates. Available literature, interviews, and researcher knowledge were used to generate the initial design. The design was updated after a pilot of n=99 Dutch participants. In each choice task, patients were instructed to imagine that their doctor told them to check their blood glucose levels at least four times per day and gave them options of devices to choose from to do this. The choice tasks were presented using a dual response ‘best–best’ set-up where participants first chose between two hypothetical glucose monitors (device A or device B) and then they chose between that choice and a standard finger-prick test for their care (see figure 1).44 45 This method mimics realistic choice scenarios while also ensuring data quality. The finger-prick test was always described as requiring four finger pricks per day, a high amount of effort to check blood glucose, no skin irritation or redness associated with a device on skin, showing glucose level only at time of measurement, no alarm and with out-of-pocket costs of €25 (or 55zl) per month. Participants were given two ‘warm-up’ DCE choice tasks before the main exercise started to ensure comprehension.
{kind=link}
Example discrete choice experiment choice task.
Questionnaire
Prior to completing the DCE, the participants were given information describing glucose monitoring as a part of diabetes self-management, including the impact of uncontrolled blood glucose on health outcomes and a description of the attributes used in the DCE. Participants were asked to answer sociodemographic questions and disease-related questions including diabetes type, years since diagnosis, use of medication and questions related to their current diabetes self-care regimen. Two brief measures assessing subjective numeracy (the Shortened Subjective Numeracy Scale-3)46 and health literacy (Brief Health Literacy Screener (Chew Items))47 were included in the survey. The final survey was pretested in think-aloud interviews with n=6 patients with diabetes from the Netherlands. The outcomes of this pretest were used to reword the survey for understandability.
Analysis
Data quality
Respondents were required to answer all questions, and only surveys that included all necessary questions for the final analysis were included. Completed responses were checked for flatlining (only choosing device A or device B) and speeding (respondents completing the survey faster than 70% of the mean response time based on log data) as data quality checks. Differences in sample demographics were assessed using χ2 tests or t-tests where applicable. A significance of p<0.05 was used for all analyses.
Preferences
Data from the DCE was analyzed by combining the two questions from each choice task as a single observation (device A vs device B vs the finger-prick test). Preference estimates in each country were assessed independently using a panel mixed-effects logit regression to account for heterogeneity of preferences within patient populations.32 Effects-coding was used for all variables except for cost, which was assumed to be linear.48 Effects-coding allows for a calculation of the reference category coefficient, which can be used for comparison to other attributes and a clear interpretation of a constant term (reflecting the utility of a status-quo finger-prick test).48 Robust outcomes were generated by applying 1000 Halton draws.49 The analysis was conducted in Stata V.14.34 The optimal model was identified based on log likelihood. Attributes with significant SD for at least one level were included as random effects in the final model. The following value functions were used for the final analyses (Equations 1–3):
 (1)
(1)
 (2)
(2)
 (3)
(3)
In these equations, the value of an alternative for individual i is calculated based on the coefficients reflecting the relative importance of each attribute or attribute level (β1–β10). β11 is an alternative specific constant reflecting the individual’s preference for the fixed alternative of the finger-prick test over device B. β0 is a constant term which identifies the respondent’s preferences for device A over device B, reflecting a left–right bias in case participants had a tendency to favor the left option. All attributes and attribute levels were included as random parameters, with a normal distribution to identify heterogeneity in the preferences for those attributes.
The mixed logit model preference estimates were used to calculate the attribute relative importance score (RIS).50 The RIS reflects how important one attribute is compared with another. These were calculated by identifying the attribute with the greatest absolute difference between highest and lowest valued levels and using this as a reference (RIS=1). The RIS for each attribute was then calculated as the quotient of the absolute difference of the most and least valued levels of that attribute and the reference value. This results in a normalized scale for comparison.
WTP estimates and uptake rates
Individual attribute coefficient estimates were extracted from the mixed-effects models to calculate individual WTP estimates and expected uptake rates. WTP estimates were generated by calculating the utility difference between attribute levels and dividing this by the negative linear cost coefficient resulting in the estimated amount that each participant would be willing to pay for the change in attribute level. Very small cost coefficients for some participants led to extreme WTP outliers so the median and IQR are reported rather than the mean. Differences in median WTP estimates were assessed using Mood’s test for equality of medians.51
Expected uptake rate estimates were calculated using the individual attribute coefficient estimates. Three device profiles represent potential glucose-monitoring devices were used to calculate uptake rates compared with a standard finger-prick test. The first profile represented the most desired device according to the outcomes of the mixed logit model: high precision, zero finger pricks per day, low effort to check, low chance of skin irritation, €25 per month out-of-pocket costs, glucose information with a daily trendline, and an alarm. The second profile was similar to a generic FGM: moderate precision, zero finger pricks, moderate effort, moderate chance of skin irritation, €100 per month out-of-pocket costs, glucose information with an arrow indicating glucose direction, and no alarm. The last profile used the generic FGM profile but changed the monthly out-of-pocket costs to €25. The uptake estimate was calculated at the individual level by taking the proportion of the individuals’ (i) total utility, which was accountable to a device (V) in a scenario containing both this device and a finger-prick alternative (W) using the following equation:
 (4)
(4)
The mean of these expected uptake rate estimates was interpreted as the expected population uptake rate.
Results
In total, n=521 respondents completed the surveys. Of those, n=487 responses were included in the final analysis after n=34 (6.5%) respondents were excluded following a check of data quality. Participant demographic information can be found in table 2. Compared with the Polish sample, the Dutch sample was significantly older (51.6 years vs 39.4 years), had lived with diabetes for more years, were less educated, had lower levels of health numeracy, and were less likely to monitor their blood glucose than the Polish sample. No other significant differences were found between the samples.
Respondent characteristics (N=487)
Preferences for glucose monitors
All attributes were found to be significant for patients in at least one of the countries. Significant heterogeneity of preferences was found for all attributes except for type of glucose information. High costs were associated with a lower likelihood of choosing a device. Increased precision was preferred over lower precision, and decreased number of finger pricks and chance of skin irritation were consistently favored over increases in these attributes. Samples from both countries favored a device with an alarm over one without an alarm. Improving a device’s effort to check from moderate to low and improving glucose information to show more than only current levels were only important for the Dutch respondents. Both samples preferred glucose-monitoring devices over a finger-prick test. The complete results of the mixed logit model can be found in table 3.
Attribute-level estimates for the panel mixed logit model
Regarding the RIS of the attributes, costs were found to be the most important factor when choosing a device by a factor of 5, compared with the next most important attribute, and a factor of approximately 50, compared with the least important attribute (online supplemental figure 2). For the Dutch sample, after costs, the most important attributes were number of finger pricks, followed by precision and chance of skin irritation, all of which were comparably valued. For the Polish population, after costs, precision of device was the second most important attribute followed by chance of skin irritation. These were also comparably valued. Polish patients were not as averse to additional finger pricks as Dutch respondents and found this approximately half as important as Dutch respondents. However, Polish respondents valued switching to a device from a finger-prick test more than Dutch respondents. Having an alarm and improving glucose information were both relatively unimportant in a device. Only the Dutch sample viewed improved effort to check and the type of glucose information as important when deciding on a device.
Supplemental material
WTP for a glucose monitor and expected uptake rates
WTP results can be found in table 4. It was estimated that Polish patients would pay significantly more to switch from a standard finger prick to a device than Dutch patients (€65.01 vs €27.74 per month). The median WTP for improvements in glucose monitors ranged from €2.58 (for the Dutch respondents to improve glucose information) to €33.64 (for the Polish respondents to increase precision from low to high). Significant differences were found between the two countries with Dutch respondents having higher WTP for device improvements in precision from low to medium, improving effort to check, and improving glucose information. Dutch patients were also willing to pay significantly more for a reduction in the number of finger pricks per day in conjunction with a device compared with Poland (€32.71 vs €13.35).
Median WTP estimates and average uptake rates compared with traditional finger prick
These differences were also reflected in the expected uptake rates for devices. Polish patients were significantly more likely to choose a device over finger prick (table 4) compared with Dutch patients. These differences were most pronounced in patients aged 18–50, patients with T2DM, and current finger prick-only users.
Discussion
To the best of our knowledge, this was the first study to investigate the relative importance of different attributes describing glucose-monitoring technologies which involved cost as an attribute. As expected, cost was found to be the most important factor for patients when deciding on glucose monitors in both the Netherlands and Poland. Increased device precision, reduction in skin irritation, and required number of finger pricks per day were the next most important attributes when choosing between glucose monitors.
The findings from this study replicate some of the findings of earlier studies,18 22 but the current study enables us to show that costs were at least more than five times more important for patients when choosing a glucose monitor than any other attribute. As costs are the primary consideration for patients when deciding to use a glucose-monitoring device or a standard finger prick, it may not be a question of WTP, but the ability to pay that is determining glucose monitor choice.18 52–54 This is unfortunate as the improvements in diabetes outcomes, patient quality of life, and healthcare expenditures in connection with using these devices are increasingly documented.17 54–60
Beyond costs, the relative importance of the other attributes differed to some degree between the two countries. Specifically, Dutch respondents valued reducing the number of daily finger pricks to zero more than twice as much as Polish respondents. The acceptance of additional finger pricks to verify blood glucose levels may reflect the greater importance that Polish respondents assigned to precision as these finger pricks are the most accurate reading and can be used for calibration of devices or verification of device glucose information. For both populations, precision was mainly significant when the device was described as having higher levels of imprecision. Lower levels of imprecision were not important for choosing a device, indicating that there is an acceptable amount of device imprecision. This was also reported by patients during the qualitative phase.
These preference differences resulted in different in WTP for glucose devices and expected uptake rates for the two countries. Both samples reflected an overall desire to move away from finger-prick tests for SMBG, although this was more pronounced in the Polish population compared with the Dutch population. Patients were consistently willing to pay for device improvements that resulted in devices that more closely represented FGMs or CGMs regarding functionality.
While we found type of information to be relatively less important based on the model outcomes, this conflicts with the findings from the qualitative phase of this study. During the interviews, stakeholders from every area including the patients indicated that only having the current glucose level was insufficient for proper glucose management. In the preference study outcomes, improvements in this area were not nearly as important for choosing a device as the interviews would have led us to believe. In addition to this, industry interviewees and patients reported that connectivity to devices which the patients normally carried around (eg, smartphone and smartwatch) was a desirable feature as it reduces effort to check and the stigma of checking blood glucose levels. The preference outcomes indicated that while the Dutch patients significantly preferred a device with low burden, the added benefit of accessing this information on a smartphone or watch instead of a dedicated device was relatively limited compared with other features or costs. This indicates that connectivity is something that is a want but not a must in a device. Exceptions to this may be in specific instances, such as parents who want to be able to monitor a child’s glucose level at a distance.61 62
Our case study focused on two countries, the Netherlands and Poland, which are examples of ‘Western’ and ‘Eastern’ European countries with partial and no reimbursement for glucose-monitoring devices supporting the transferability of these findings to other countries with out-of-pocket costs for SMBG. At the time of designing the study, the reimbursement for CGMs was limited in the Netherlands with FGMs not fully reimbursed.21 The reimbursement policy of Dutch insurance companies changed while the study was being conducted to allow patients with T1DM, patients with T2DM with intense insulin regimens, and patients with T2DM who are pregnant or trying to become pregnant to be eligible for FGMs through their health insurance. CGMs and FGMs were not reimbursed in Poland at the time that the study was conducted, and to the best of our knowledge are still not reimbursed.63 64 Respondent awareness of the change in reimbursement in the Netherlands may have resulted in lower WTP estimates. It would be interesting to study how improved access to these devices for some patients has changed preferences in Dutch patient populations and if the removal of cost as an attribute impacts their preferences compared with Poland without a change in reimbursement. The removal of cost as a barrier would likely have a large impact on patient preferences and expected uptake rates of these devices with a greater focus on how the device fits into the patient’s lifestyle as reflected in the study by Hannah et al.22
The strengths of this study include the extensive qualitative phase used to identify the relevant attributes for use in the DCE. This process was more extensive than what is commonly done to generate attributes in preference studies. Interviewees were internationally diverse with a broad range of backgrounds and contributed to the identification of a set of attributes relevant to a broad sample of patients. Another strength of this study is the multicountry sampling, which allows for a better understanding of the transferability of these findings to diabetes patient populations in other countries. This study did have some limitations. First, the study used data that relied on self-reports of diabetes diagnosis and no quotas based on SES were imposed. This limited exploring subgroup analyses of SES group preferences which may be relevant as SES has previously been associated with adherence to SMBG. Second, patients were recruited through an online panel only and not through clinical partners or patient organizations due to COVID-19-related restrictions on all non-vital research. This resulted in a sample of respondents that had generally higher levels of education and were younger than we would expect from the general diabetes population.65–68 The results of a more representative sample may produce different relative preference outcomes as we found differences in expected uptake rates based on age stratifications.
Conclusion
While patients value many aspects of glucose monitors, out-of-pocket costs are the primary concern of patients when deciding on devices to self-monitor blood glucose. Even when different welfare levels between the two countries were accounted for, differences in estimated WTP were found between the countries. This study shows that uptake of modern glucose-monitoring devices is dependent on out-of-pocket costs. In light of these clear preferences to switch from glucose measurement by finger pricks to more modern equipment, a critical review of the costs and benefits of such devices is needed to see if removing the cost barrier is justified by the potential improvements in blood glucose monitoring.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was reviewed by the medical research ethics committee of the UMC Utrecht in 2019 and found to present limited risk to participants according to the Medical Research Involving Human Subjects Act 1998 (Wet Medisch-Wetenschappelijk Onderzoek met Mensen). Thus, the study was thus waived from full medical ethical review and was approved to be conducted (reference number WAG/mb/19/045208). The study was conducted according to the principles of the Declaration of Helsinki. All participants were informed about the study through written materials and provided written informed consent prior to participating in the study.
Acknowledgments
The authors of this article acknowledge the following people for their contributions to the study: the patients for participating and sharing their valuable insights on the interviews and survey, Angela de Rooij and Anna Sliwinska for their insights into patient values and experiences in the Netherlands and Poland, Maria van Dijk-Okla for her help in translating and reviewing the Polish survey, and the PREFER consortium for their advice and guidance throughout the study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors IPS, CLW, JV, MPMHR-vM, RCV, EWdB-G and GAdW were responsible for the initial development, set-up and design of the study. IPS and CLW were responsible for the qualitative aspects of the study as well as quantitative data collection under the direct supervision of GAdW, JV, EWdB-G, and MPMHR-vM. The primary analysis was conducted by IPS with assistance from JV and CGMG-O. All authors reviewed the final manuscript and contributed to the revisions. IPS is the guarantor for this articla and accepts full responsibility for the work and/or the conduct of the study, had access to the data, and controlled the decision to publish.
Funding This study formed part of the Patient Preferences in Benefit-Risk Assessments during the Drug Life Cycle (PREFER) project. The PREFER project has received funding from the Innovative Medicines Initiative 2 Joint Undertaking (grant agreement number 115966). This joint undertaking receives support from the European Union’s Horizon 2020 research and innovation programme and the European Federation of Pharmaceutical Industries and Associations.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.