Article Text

Abstract
Introduction Evaluate the prevalence of, and factors associated with, diabetes in people with severe mental illness (SMI) attending the Collaborative Centre for Cardiometabolic Health in Psychosis (ccCHiP) tertiary referral clinics.
Research design and methods Adult patients attending an initial ccCHiP clinic consultation (2014–2019) were studied. Diabetes was defined by an hemoglobin A1c of ≥6.5%, fasting blood glucose of ≥7.0 mmol/L, or a self-reported diagnosis of diabetes and prescription of antihyperglycemic medication.
Results Over 5 years, 1402 individuals attended a baseline consultation. Mean age of 43.9±12.8 years, 63.1% male and 63.5% had a diagnosis of schizophrenia. Prevalence of diabetes was 23.0% (n=322); an additional 19.5% fulfilled criteria for pre-diabetes. Of those with diabetes, 15.8% were newly diagnosed. Of those with pre-existing diabetes, 84.5% were receiving treatment with antihyperglycemic medication. Over 94% of individuals with diabetes had dyslipidemia; half were current smokers; and 46.4% reported sedentary behavior. On multivariate analysis, diabetes was associated with older age, Aboriginal, Indian or Middle Eastern maternal ethnicity, elevated waist-to-height ratio, family history of diabetes and use of antipsychotic medication.
Conclusion Prevalence of diabetes mellitus in this multiethnic cohort with SMI is significantly higher than the Australian population. Targeted interventions via an assertive integrated approach are required to optimize cardiometabolic health in this population.
- diabetes mellitus, type 2
- diagnosis
- mental disorders
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Internationally, the risk of diabetes in people with severe mental illness (SMI) has been reported to exceed threefold that of the general population. While diabetes is undoubtedly a common comorbidity for Australians living with SMI, an accurate estimate of the prevalence of diabetes in Australians with SMI is yet to be firmly established.
WHAT THIS STUDY ADDS
Prevalence of diabetes mellitus in this multiethnic cohort of people with SMI is significantly higher than the background Australian population, especially in younger people. New diabetes was detected in 15.8% of the cohort.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Our finding of new diabetes in a multidisciplinary clinic setting provides support for more comprehensive screening in this high-risk population. Moreover, it raises the need for early intervention with a focus on younger people and in the subgroup of people with pre-diabetes as a preventative measure in reducing the risk of diabetes in this vulnerable population.
Introduction
Diabetes remains one of the most common chronic health conditions1 and is associated with high levels of morbidity and premature mortality.2 3 The Australian Bureau of Statistics 2017–2018 National Health Survey estimated the prevalence of self-reported diabetes in the general Australian population to be 4.9%4 5; a further 3.1% of the Australian population has been estimated to have pre-diabetes.6
People with severe mental illness (SMI) are known to be at increased risk of diabetes.7 8 Those with SMI face significant medical and psychosocial challenges, and these undoubtedly contribute to an increased risk of diabetes. Chronic treatment with antipsychotic and other psychotropic medications is frequently associated with significant weight gain. Overweight and obesity are associated with increased insulin resistance and increased risk of dysglycemia. People with SMI face financial constraints that significantly restrict dietary choices. In addition, many people with SMI struggle to maintain adequate levels of physical activity with a significant proportion of this cohort leading sedentary lives.
Research has shown that individuals with SMI have excess mortality compared with the general population due to the development of premature chronic physical and medical conditions.8 There are reports that people with schizophrenia or bipolar disorder and diabetes have a higher mortality rate than those with no diabetes9 and those with SMI only.10 In a small Australian study, the combination of schizophrenia and diabetes increased the mortality rate by sixfold compared with that seen in people with neither condition.11 A large Danish registry-based study reported that the cumulative risk of death was 15.0% at 7 years post diagnosis of diabetes for the cohort of people <50 years of age with both SMI and diabetes.12 Similarly, in a British register-based study, Vinogradova et al found that 23.1% of people with SMI and diabetes died within 5 years of follow-up.9
Despite this knowledge, the screening and diagnosis of diabetes in this population remains poor due to limited access to care, fragmentation of care delivery and patient-related factors. It has been estimated that 70% of people prescribed second-generation antipsychotic pharmacotherapy remain unscreened for diabetes.13 Those with schizophrenia have a greater risk of acquiring acute and macrovascular complications14 of diabetes and an estimated 74% greater risk of requiring a hospital admission for hypoglycemia/hyperglycemia compared with those without schizophrenia.15
Internationally, the prevalence of diabetes in people with SMI has been reported to be two to three times higher than that in the general population without SMI.16 However, rigorous studies examining prevalence of diabetes in the setting of SMI in Australia are scarce. The self-reported prevalence of diabetes in the 2010 Australian Survey of High Impact Psychosis was 20%.17 Previous studies conducted within a number of Australian mental health services determined the combined prevalence of impaired fasting glucose and diabetes (diagnosed on the basis of elevated fasting glucose) in the SMI population to be >30%.18 19
A more comprehensive understanding of the diabetes burden in the Australian SMI population is clearly required. The primary aim of our study was to determine the prevalence of diabetes in this high-risk population using more comprehensive screening criteria for detecting diabetes and compare this to the general Australian population. The secondary aim was to investigate the factors associated with the diabetes status in these patients. This knowledge will help to facilitate more appropriate allocation of resources and thus provide an opportunity to improve early treatment and the holistic management of people with SMI.
Methods
Study setting
The study population included adults (aged 18–65 years) with SMI who attended a baseline visit to the Collaborative Centre for Cardiometabolic Health in Psychosis (ccCHiP) clinics between May 2014 and December 2019. The ccCHiP clinics are located within the Sydney Local Health District New South Wales, Australia, which services a catchment area of approximately 700 000 residents. ccCHiP provides a multidisciplinary, consultative service for patients with SMI, and referrals are received from local community mental health centers and local general practitioners. The service runs on an integrative health model with input from a psychiatrist, endocrinologist, cardiologist, dietitian, exercise physiologist, sleep clinician, nurse and oral health team.20 It is a one-stop shop where all clinicians are seen by the patient in a single session.
Diagnostic criteria used to classify diabetes mellitus and pre-diabetes in the ccCHiP clinic
For the purpose of this study, a hierarchical approach (table 1) was used to determine type 2 diabetes status (patients with type 1 diabetes are not seen in the clinic). If an individual presented with a hemoglobin A1c (HbA1c) level of ≥6.5%, this was deemed to be consistent with diabetes and coded accordingly. In the event that an HbA1c was unavailable (or the HbA1c was <6.5% at the time of their visit), a self-report of a diagnosis of diabetes, treatment with insulin or other antihyperglycemic medications and/or elevated fasting blood glucose measurements were used to identify individuals with diabetes. We excluded people who did not have a pre-existing diagnosis of diabetes and were using metformin for an off-label indication. Overall prevalence of diabetes was determined by the addition of the six diagnostic subgroups incorporated in table 1. Within the cohort of clinic patients not identified as having diabetes, further review of HbA1c and fasting blood glucose results allowed for the identification of individuals with pre-diabetes. Individuals with an HbA1c of 6.0%–6.4% (Australian Diabetes Society criteria)21 and/or a fasting blood glucose level between 5.6 mmol/L and 6.9 mmol/L (ADA criteria)22 were classified as having pre-diabetes.
Categories used to determine diabetes status in the ccCHiP cohort
Data collection
Demographic data (age, gender, ethnicity and marital status) and clinical data (International Classification of Diseases, 10th Revision (ICD-10) psychiatric diagnosis, medication use, personal history of diabetes, family history of diabetes, smoking status, alcohol consumption, physical activity level, body mass index (BMI), waist:height ratio (WtoHt), blood pressure, fasting blood glucose, HbA1c, total cholesterol, triglyceride, high-density lipoprotein (HDL) cholesterol, low-density (LDL) lipoprotein cholesterol and estimated glomerular filtration rate (eGFR) are routinely collected for patients who attend the ccCHiP clinic.
Ethnicity was classified as low-risk category for diabetes when the father’s or mother’s country of birth was from a Mediterranean or Caucasian origin; high-risk category when African–American, Pacific Islander, Middle Eastern, Asian/Southeast Asian, Aboriginal/Torres Strait Islander, Indian subcontinent or other high-risk origin. BMI was defined as ‘normal’ if (18.0–<25.0 kg/m2 and low-risk ethnicity or 16.0–<23.0 kg/m2 and high-risk ethnicity), overweight (25.0–<30.0 kg/m2 and low-risk ethnicity or 23.0–<27.5 kg/m2 and high-risk ethnicity) and obese (≥30 kg/m2 and low-risk ethnicity or ≥27.5 and high-risk ethnicity).
WtoHt was categorized as elevated if an individual’s WtoHt was >0.52 and low-risk ethnicity, or >0.50 and high-risk ethnicity. Abdominal circumference was categorized as normal if an individual’s waist was <94.0 cm for men and low-risk ethnicity, or <90.0 cm for men and high-risk ethnicity, or <80.0 cm for women; and ‘abnormal’ if ≥94.0 cm for men and low-risk ethnicity, or ≥90.0 cm for men and high-risk ethnicity or ≥80.0 cm for women. Dyslipidemia was defined by the presence of one or more of the following findings: (1) prescription of cholesterol-lowering medication, (2) total cholesterol of ≥4.2 mmol/L, (3) HDL cholesterol of <1.04 mmol/L (for men) and <1.29 mmol/L for women, (4) LDL cholesterol of ≥2.59 mmol/L and (5) triglycerides of ≥1.7 mmol/L. Consumption of alcohol was categorized as ‘high risk’ (≥7 standard drinks/week for men and ≥5 standard drinks/week for women) and ‘low risk’ (<7 standard drinks/week for men and <5 standard drinks/week for women). Treatment with antipsychotic medication was categorized as (1) clozapine (±another antipsychotic medication), (2) olanzapine (±another antipsychotic medication), (3) non-clozapine/non-olanzapine antipsychotic medication and (4) no antipsychotic medication.
Statistical analysis
Data were analyzed using SAS V.9.1.4 statistical software program.23 Descriptive statistics are presented as count and percentage for discrete variables and as mean and SD for continuous variables. Prevalence of diabetes and the prevalence of pre-diabetes are both reported with their corresponding 95% CIs. The Pearson’s χ2 test was used to assess for differences in the distribution of categorical variables. Logistic regression analyses were carried out to explore the association between risk factors and diabetes status. In this approach, potential risk factors against diabetes status were analyzed in a backward selection procedure. Variables with p values of < 0.10 in the univariate association were entered into the multivariate model with a p value of <0.05 being the criterion for removal of variables. ORs (with 95% CIs) for each risk factor are reported. Statistical tests were two-tailed with the significance level set at 0.05.
Results
Characteristics of ccCHiP clinic participants
Between May 2014 and December 2019, 1402 patients with SMI were seen for a baseline visit at a ccCHiP clinic. The mean age of the ccCHiP cohort was 43.9±12.8 years; 63.1% were male; 79.0% were overweight or obese; and 50.0% were current tobacco smokers (table 2). White/Caucasian (64.0%) and Asian/Southeast Asian (17.0%) were the most frequently cited ethnicities within the clinic population. The most common psychiatric diagnosis among ccCHiP clinic attendees was schizophrenia (63.5% of the clinic cohort). For those individuals not reporting a diagnosis of schizophrenia, the primary psychiatric diagnosis was attributed to schizoaffective disorder (in 9.6% of cases), bipolar disorder (12.2% of cases), depression (4.0% of cases) and other psychosis (7.4%). Of the clinic cohort, 3.3% had another ICD-10 diagnosis recorded as their primary psychiatric illness. Table 2 demonstrates that there is a difference across various psychiatric diagnosis with the diabetes and no diabetes groups (p<0.001).
Baseline characteristics of ccCHiP clinic population by diabetes status
Diabetes and pre-diabetes prevalence
Overall, the prevalence of diabetes within the ccCHiP clinic population was found to be 23.0% (95% CI 20.8% to 25.2%) (table 2). The prevalence of diabetes was similar for men (24.0%, 95% CI 21.2% to 26.8%) and women (21.2%, 95% CI 17.7% to 24.8%). A further 19.5% (95% CI 17.4% to 21.5%) of our cohort were classified as having evidence of pre-diabetes (on the basis of an HbA1c in the 6.0%–6.4% range and/or a fasting blood glucose in the 5.6–6.9 mmol/L range). Pre-diabetes was identified in a slightly higher proportion in men than in women (21.0%, 95% CI 18.4% to 23.7% (male) vs 16.8%, 95% CI 13.6% to 20.0% (female)). Within the female cohort, 8.2% (95% CI 5.5% to 10.9%) of individuals reported a history of gestational diabetes. Of those with a history of gestational diabetes, one-third had developed diabetes mellitus by the time of their first visit to the ccCHiP clinic.
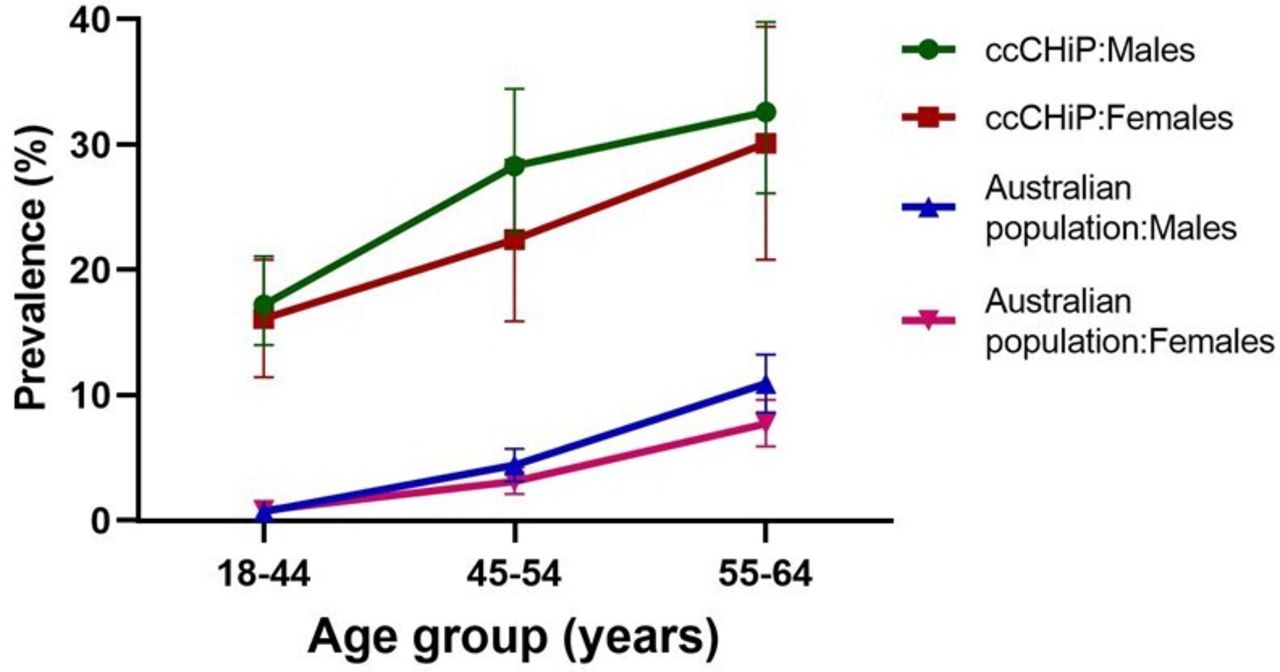
Figure 1 highlights the prevalence of diabetes mellitus (stratified by age group and sex) for the ccCHiP clinic population. These data are presented in comparison to the background, general Australian population.4 5 As can be seen, the prevalence of diabetes within the ccCHiP clinic population is substantially higher than the Australian General population across each of the 18–44, 45–54 and 55–64 years of age categories.
{kind=link}
Prevalence of diabetes (stratified by age group and sex) for the ccCHiP population and the background, Australian general population. ccCHiP, Collaborative Centre for Cardiometabolic Health in Psychosis.
Diabetes treatment and level of glycaemic control
Of the 322 individuals classified as having diabetes according to our diagnostic criteria, 51 (15.8%) were newly diagnosed with diabetes at the time of their first ccCHiP clinic visit. Of the 271 individuals with pre-existing diabetes at the time of first ccCHiP clinic visit, 229 (84.5%) were receiving treatment with diabetic pharmacotherapy. Within the cohort of patients holding valid prescriptions for diabetic pharmacotherapy, the three most prescribed agents were metformin (216/229, 94.3%), gliclazide (or other sulfonylurea) (44/229, 19.2%) and insulin (36/229, 15.7%) (table 3). The most prescribed treatment regimen was metformin monotherapy (n=145, 63.3%). Of those with a pre-existing diagnosis of diabetes and on metformin monotherapy, 36.4% were not at the recommended HbA1c target (<7.0%) at the time of their ccCHiP visit. Approximately 37.0% were prescribed dual antihyperglycemic therapy. Sodium-glucose co-transporter-2 (SGLT2) inhibitors and glucagon-like peptide-1 (GLP-1) receptor agonists were the least frequently used pharmaceutical agents. Table 3 illustrates the distribution of diabetic pharmacotherapy use at the time of the initial ccCHiP clinic visit.
Diabetic pharmacotherapy use among those individuals holding at least one valid prescription for an antihyperglycemic agent at the time of initial ccCHiP clinic visit (n=229)
Ninety per cent of individuals (n=289 of the diabetes cohort) with a diagnosis of diabetes had a recent HbA1c measurement available at the time of their first clinic visit. The median HbA1c for those with a diagnosis of diabetes was 6.8% (range 4.3%–16.2%). Forty-five per cent (n=131) had an HbA1c of ≥7.0%, and 28.0% (n=82) had an HbA1c of ≥8.0%.
Diabetes and antipsychotic therapy
Thirty-five per cent of people with diabetes were receiving treatment with clozapine±other antipsychotic medication, 11.0% olanzapine±other antipsychotic medication, 47.2% were receiving treatment with non-clozapine/non-olanzapine antipsychotic medication, and 6.5% were not prescribed any antipsychotic medication.
Factors associated with diabetes in the ccCHiP population
Univariate logistic analysis revealed that age, WtoHt, father’s ethnicity, mother’s ethnicity, family history of diabetes, psychiatric diagnosis, consumption of alcohol, physical activity and antipsychotic treatment with clozapine±other antipsychotic medication or olanzapine±other antipsychotic medication were statistically significantly associated with diabetes (table 4). We did not find a significant association between gender and diabetes or smoking status and diabetes.
Logistic regression models of factors associated with diabetes in people with severe mental illness attending a multidisciplinary service
Multivariate logistic analysis found that older age was significantly associated with diabetes. Those with an elevated WtoHt had significantly higher odds of diabetes (OR 4.5, 95% CI 2.2 to 9.2) relative to those with a normal WtoHt. People with a family history of diabetes had twofold higher odds of diabetes (OR 2.0, 95% CI 1.5 to 2.8). Those with Aboriginal/Torres Strait Islander and Indian subcontinent maternal ethnic backgrounds had greater than threefold increased odds of diabetes relative to the Caucasian/Mediterranean ethnic group. Finally, the odds of diabetes in those treated with clozapine±other antipsychotic medication (OR 1.7, 95% CI 1.2 to 2.4) were almost twofold higher than in those treated with non-clozapine/non-olanzapine antipsychotic therapy. Treatment with olanzapine±other antipsychotic medication was associated with half the odds (OR 0.5, 95% CI 0.3 to 0.8) of having diabetes than those treated with non-clozapine/non-olanzapine antipsychotic therapy.
Discussion
Throughout the world, the prevalence of diabetes mellitus continues to increase with predictions that the 2045 worldwide prevalence will reach 783 million.24 Within the cohort of people with SMI, most antipsychotic pharmacotherapy contributes to weight gain and insulin resistance. International studies have found that the prevalence of diabetes is two to three times higher in those with SMI than that observed in the general population.16 In the Australian setting, we have confirmed a significantly higher prevalence of diabetes in the SMI population than that seen in the general Australian population. In the category aged 18–44 years, diabetes prevalence in the ccCHiP population is 16.7% (>10 times higher than the age-matched, general Australian population). In the 45–54 years of age category, diabetes prevalence in the ccCHiP population is 25.9% (>6 times higher than the age-matched, general Australian population) and in the 55–64 years of age category, diabetes prevalence in the ccCHiP population is 31.7% (>3 times higher than the age-matched, general Australian population).
Within the ccCHiP cohort alone, we found that diabetes was significantly associated with older age; elevated WtoHt; presence of a family history of diabetes; maternal ethnic background being Aboriginal/Torres Strait Islander, Indian or Middle Eastern compared with Caucasian/Mediterranean, and being on clozapine or olanzapine±other antipsychotic medication compared with not using any antipsychotic medication. Comparable risk factors are prevalent in high-risk psychosis groups globally, reinforcing the notion that the diabesity ‘pandemic’ is even more accentuated in those with SMI.
In this study, treatment with olanzapine±other antipsychotic medication was associated with lower odds of having diabetes than those on other antipsychotic medication only. This unexpected finding was in contrast to the increased odds of diabetes observed in those on treatment with clozapine±other antipsychotic medication. One possible explanation for the discordance between olanzapine and clozapine may be driven by prescriber behavior. We observe that many prescribers in our local area are acutely aware of the orexigenic and diabetogenic effects of olanzapine and are therefore more proactive in the metabolic management of patients commenced on treatment with olanzapine. This certainly needs to be explored in future research in similar cohorts.
A significant concern for the ccCHiP service is a relatively high prevalence of undiagnosed diabetes at the time of first clinic visit. From the literature, it is estimated that up to 70% of cases with diabetes in people with SMI are undiagnosed.25 In our clinic population, over 15% of those with diabetes mellitus were newly diagnosed at the time of their first visit. Over 40% of those newly diagnosed with diabetes at the time of their first visit were aged less than 45 years.
These data support a more proactive screening approach in the young adult SMI population. It is now well recognized that early detection and assertive treatment of diabetes can be very useful in achieving better long-term outcomes.26 The high rate of undiagnosed diabetes provides a strong argument for more intensive screening for diabetes within the SMI population. It appears that screening for diabetes should start at least two decades earlier for those with SMI. Such screening also provides an opportunity to identify those who have impaired glucose tolerance or pre-diabetes. From a pragmatic point of view, screening with fasting glucose and an HbA1c level would appear to be a reasonable strategy to adopt.
Another concern for clinicians at the ccCHiP clinic is that of treatment inertia in the management of diabetes for the target cohort. For those with a pre-existing diagnosis of diabetes, >40% were not at the recommended HbA1c target (<7%) at the time of their ccCHiP visit. On review of pharmacotherapy use, it is apparent that metformin, gliclazide and insulin were the most commonly prescribed antihyperglycemic agents during the study period. In view of high levels of suboptimal glycemic control at the time of a patient’s initial ccCHiP clinic appointment, diabetes treatment intensification appears currently inadequate within the local community who have SMI. In this context, a ccCHiP-like service is well placed to provide diabetes management support to primary care and local community mental healthcare teams. The relative underuse of newer, antihyperglycemic pharmacotherapies (namely, SGLT2 inhibitors and GLP-1 receptor agonists) is most likely explained by the national pharmaceutical benefit scheme prescribing restrictions that were in place for these agents during the study period (2014–2019). Moving forward, there is certainly a role for services like ccCHiP to support an increased uptake of these metabolically favorable treatments in partnership with local general practitioners.
Strengths and limitations
Our study is notable for a number of strengths. The ccCHiP clinic has provided clinical services to >1400 individuals with SMI over the past 5 years, and thus this study captured data from a substantial number of individuals with SMI who reside in the Sydney Local Health District.
This study provides the first systematically collected data on cases of schizophrenia in our catchment area. The question of representativeness arises. Given the currently accepted point prevalence rate for the schizophrenias (0.28%), the catchment population size serviced (700 000) and the known number and diagnoses of persons in public psychiatric care (2200; ~65% schizophrenia spectrum), and given public clinics are the predominant setting for the treatment of SMI, we estimate that about three-quarters of suitable patients are referred to ccCHiP. There is no significant difference (age and gender) between our cohort of people with SMI and the Australian SMI population not referred to the ccCHiP Clinical Service.27 Further, referral criteria are not based on anthropometric or pathology criteria, but rather a mandate that all new patients with psychosis are assessed within a year and then between 12 and 24 months in periodic follow-up. This suggests that the ccCHiP cohort is representative of those that are managed in public psychiatric settings.
The use of a hierarchical approach to diabetes identification incorporating both HbA1c and fasting glucose data, in addition to self-report and review of pharmacotherapy, is another strength. Previous Australian studies have primarily relied on fasting glucose measurements to estimate diabetes/pre-diabetes prevalence, and in some studies, simply a self-report. Evidently, these previous studies may have resulted in a less accurate estimation than the more comprehensive approach employed in this study. It is also important to note that the ccCHiP service prospectively collects clinical data at each patient visit to the clinic, and thus missing data are kept to a minimum. In addition, the comprehensive data collected by the ccCHiP service has allowed insights into pharmacotherapy use within the cohort of patients with co-morbid SMI and diabetes. In turn this provided an opportunity to quantify the degree of diabetes treatment inertia currently faced by this high-risk population.
It is also important to recognize the study’s limitations. Data presented are collected from a secondary referral service and thus may be subject to a referral bias. Nevertheless, our criteria used for referring individuals to ccCHiP clinics accommodated all people with a diagnosis of ‘psychosis’ which is reasonably representative of those in the Central Sydney public mental health population, as described previously. Referrals are accepted from all local healthcare providers; however, the majority of referrals are received from local community mental health services and a minority are received from within-area general practitioners. Individuals with SMI managed in the private health sector are relatively under-represented. We also acknowledge that the criteria used to identify individuals with diabetes within the ccCHiP clinic population, while more comprehensive than those used in previous Australian studies, are imperfect. Ideally, to confirm a new diagnosis of diabetes, one would normally request a second confirmatory fasting blood test. This is usually performed by the patient’s GP, and the ccCHiP clinic does not have direct access to the results of confirmatory testing that may have been performed by general practitioners.
Conclusion
Overall, the prevalence of diabetes within the SMI population in metropolitan Sydney is significantly higher than that of the age-matched, general Australian population. Two areas of significant concern are the relatively high rates of undiagnosed diabetes in the clinic population (especially considering the elevated rates of early onset) and an apparent treatment inertia in those with an established diagnosis of diabetes. Implementation of targeted interventions via an integrated care approach may help these high-risk individuals improve their diabetes management and their cardiometabolic health.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
Collection and analysis of Collaborative Centre for Cardiometabolic Health in Psychosis data were approved under REGIS 2021/ETH00456 (previously HREC/16/CRGH/101) through the Sydney Local Health Area District ethics committee. A waiver for informed consent was obtained as the study was performed on deidentified, routinely collected clinical data and carried minimal risk to participants.
Acknowledgments
The study was performed using data collected from patients attending the
Collaborative Centre for Cardiometabolic Health in Psychosis
(ccCHiP) clinics using a bespoke clinical informatics system. The authors thank the staff at the ccCHiP clinics for their assistance with data collection.
References
Footnotes
Contributors TL, RC and TM have made substantial contributions to the conception and design of the article or study, or acquisition of data. PS performed the statistical analysis and coordinated the interpretation of data with TM. TM, PS and TL were involved in the drafting of the article or revising it critically for important intellectual content. TL accepted full responsibility for the work and/or the conduct of the study, had access to the data, and controlled the decision to publish as the guarantor. All authors provided comments on drafts of the manuscript.
Funding The activities of the ccCHiP clinics are supported by the Sydney Local Health District.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.